Treatment of Brain Metastasis from Lung Cancer

1
Department of Radiation Oncology, University of Arizona, 1501 N Campbell Ave., Tucson, AZ 85724, USA
2
Department of Radiation Oncology, University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030, USA
*
Author to whom correspondence should be addressed.
Cancers 2010, 2(4), 2100-2137; https://doi.org/10.3390/cancers2042100
Submission received: 9 October 2010
/
Revised: 11 November 2010
/
Accepted: 2 December 2010
/
Published: 15 December 2010
(This article belongs to the Special Issue Organ-Specific Metastasis Formation)
Abstract
:Brain metastases are not only the most common intracranial neoplasm in adults but also very prevalent in patients with lung cancer. Patients have been grouped into different classes based on the presence of prognostic factors such as control of the primary tumor, functional performance status, age, and number of brain metastases. Patients with good prognosis may benefit from more aggressive treatment because of the potential for prolonged survival for some of them. In this review, we will comprehensively discuss the therapeutic options for treating brain metastases, which arise mostly from a lung cancer primary. In particular, we will focus on the patient selection for combined modality treatment of brain metastases, such as surgical resection or stereotactic radiosurgery (SRS) combined with whole brain irradiation; the use of radiosensitizers; and the neurocognitive deficits after whole brain irradiation with or without SRS. The benefit of prophylactic cranial irradiation (PCI) and its potentially associated neuro-toxicity for both small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) are also discussed, along with the combined treatment of intrathoracic primary disease and solitary brain metastasis. The roles of SRS to the surgical bed, fractionated stereotactic radiotherapy, WBRT with an integrated boost to the gross brain metastases, as well as combining WBRT with epidermal growth factor receptor (EGFR) inhibitors, are explored as well.
1. Introduction
Brain metastases are the most common intracranial neoplasm, occurring in 8–10% of cancer patients, and are a significant cause of cancer-related morbidity and mortality worldwide [1,2] The incidence of brain metastases is rising with an annual incidence of approximately 170,000 to 200,000 in the United States [3]. This is caused by a combination of factors including the improved therapeutic efficacy of current cancer treatments, which leads to longer survival, such as the addition of bevacizumab to chemotherapy as the first-line treatment of metastatic non-small cell lung cancer; and failure in a potential systemic therapy sanctuary site, or more frequent brain surveillance for specific cancers that have a predilection for brain metastases; and improvements in modern imaging technology, which lead to the diagnosis of brain metastases at an earlier stage [4,5]. However, such an increase in the incidence of brain metastases in recent years has not been observed in all studies, and may possibly be attributed to under-diagnosis in earlier years [1,6]. The most common origins of brain metastasis include primary cancers of the lung, breast, skin (melanoma), and the GI tract. Among these, primary tumors in the lung are the most common cause of brain metastases, as up to 65% of patients with lung cancer will ultimately develop brain metastases [7].
As the leading cause of cancer mortality, and the most prevalent cancer in men, lung cancer accounted for an estimated 161,840 deaths in the United States with an incidence of 215,020 in 2008. Furthermore, approximately 1.35 million cases were diagnosed worldwide with 1.18 million deaths in 2002 [8]. Therefore, brain metastasis is a very important problem in the overall management of lung cancer. Among the various histologies, small cell lung cancer (SCLC) is the most likely to metastasize to the brain with an 80% probability of brain metastasis after two years from diagnosis [6]. Brain metastases develop in approximately 30% of patients with non-small cell lung cancer (NSCLC) [9]. Among the various histologies of NSCLC, the relative frequency of brain metastases in patients with adenocarcinoma and large cell carcinoma was much higher than that in patients with squamous cell carcinoma [10,11].
Most patients present with significant neurological signs and symptoms that are related to the location and extent of brain involvement. They include both focal neurological changes and general symptoms secondary to increased intracranial pressure [12]. Major clinical presentations are listed in Table 1 [13]. Contrast-enhanced MRI is the preferred imaging study for the diagnosis of brain metastases over non-enhanced MRI or computed tomography (CT) scans in detecting cerebral metastases and in differentiating metastases from other central nervous system (CNS) lesions [14,15]. The recommended pregadolinium studies include T2-weighted and T1-weighted sequences, and the recommended postgadolinium studies include the T1-weighted and fluid-attenuated inversion-recovery (FLAIR) sequences [5]. Thinner axial slices without skips may be necessary to detect the smallest lesions. If the diagnosis is still in doubt, biopsy should be considered. Brain metastases are usually found at the junction of the grey and white matters, with circumscribed margins and large amounts of vasogenic edema relative to the size of the lesion. Furthermore, they usually present as multiple lesions as a result of a lung primary [16].
Without treatment, the median survival of patients is 4–7 weeks [17,18,19]. The treatment can usually be divided into symptomatic and therapeutic strategies. Symptomatic relief is most commonly achieved with corticosteroids to reduce peritumoral edema and anticonvulsants to prevent recurrent seizures. Systemic steroids alone improve neurological function and prolong survival to approximately two months [20]. Whole brain radiotherapy (WBRT), as the primary treatment approach for brain metastases, improves neurological function and prolongs median survival to three to five months [12]. Due to the poor survival outcomes associated with brain metastases, more aggressive treatments for patients have been sought and investigated. In general, the therapeutic approach largely depends on the number and location of metastases, as well as the extent of extra-cranial tumor involvement. In the following sections, prognostic factors that may influence treatment selection and the various treatment approaches will be reviewed.

{kind=link}
| Symptom | Percentage (%) | Sign | Percentage (%) |
|---|---|---|---|
| Headache | 49 | Hemiparesis | 59 |
| Mental problems | 32 | Cognitive deficits | 58 |
| Focal weakness | 30 | Sensory deficits | 21 |
| Ataxia | 21 | Papilledema | 20 |
| Seizures | 18 | Ataxia | 19 |
| Speech problems | 12 | Apraxia | 18 |
2. Prognostic Factors
A retrospective recursive partitioning analysis (RPA) was performed based on three consecutive Radiation Therapy Oncology Group (RTOG) trials, which included approximately 1200 patients with brain metastases [21]. Three prognostic classes (RPA class I, II and III) were found to be associated with the overall survival of patients with brain metastases. This classification scheme is based on age at diagnosis, presence of extracranial disease, Karnofsky performance status (KPS), and the status of the primary cancer. RPA class I includes patients who are younger than 65 years of age, have a KPS score of ≥70, tumor controlled at the primary site, and no extracranial disease. RPA class III patients have a KPS score of less than 70. All other patients are in RPA class II. The median survival times for the RPA classes I-III were 7.1, 4.2, and 2.3 months, respectively. This RPA classification is the most commonly used prognostic system for brain metastases, with further validation in Phase III and major institutional studies for both NSCLC and SCLC [22,23,24,25]. Despite the common adaptation of RPA classification, clinicians are still faced with the dilemma of tailoring treatments to individual patients because factors such as the number or volume of brain metastases were not included in the RPA initially, estimation of systemic disease was not consistently reliable, etc. As newer data came out, a new prognostic index, the graded prognostic assessment (GPA), was generated based on data from five randomized RTOG studies involving brain metastases [26]. Please refer to Table 2 for details of the GPA scoring system. The median survival times according to GPA score were: GPA 0–1, 2.6 months; GPA 1.5–2.5, 3.8 months; GPA 3, 6.9 months; and GPA 3.5–4.0, 11.0 months (p < 0.05). The GPA prognostic index was further validated based on specific diagnosis at the primary site due to the heterogeneous response of brain metastases to various treatment approaches based on histology and the various patterns of systemic disease and response to systemic therapy for different types of primary tumor [27]. For both NSCLC and SCLC, all four prognostic factors remained significant, confirming the prognostic value of the original GPA for lung cancer.
| Score | 0 | 0.5 | 1.0 |
|---|---|---|---|
| Age | >60 | 50–59 | <50 |
| KPS | <70 | 70–80 | 90–100 |
| No. of CNS metastases | >3 | 2–3 | 1 |
| Extracranial metastases | Present | - | None |
Abbreviations: KPS: Karnofsky performance score; CNS: central nervous system; No.: number
3. Symptomatic Management
The management of symptoms from brain metastases has primarily consisted of the usage of corticosteroids (e.g., dexamethasone or methylprednisolone) and anticonvulsants. Corticosteroids are given upon initial diagnosis to relieve the symptoms associated with peritumoral edema in approximately two-thirds of patients because of their ability to reduce the permeability of tumor capillaries [28,29]. In a study by Vecht et al., doses of 8 versus 16 mg/day with tapering schedules over four weeks and doses of 4 versus 16 mg/day with continuation of these doses for 28 days prior to tapering demonstrated similar KPS improvements at seven days (54% to 70%) and 28 days (50% to 81%) in patients treated with WBRT and concurrent ranitidine [30]. However, patients in the 4 mg/day arm experienced a higher rate of drug reinstitution than in patients treated with 8 or 16 mg/day. Furthermore, the greatest KPS improvement was observed in patients in the 16 mg/day arm when this dose was tapered over four weeks. These findings suggest that greater KPS improvement arose from the maximal anti-inflammatory effects of the initial higher doses, while the late toxicity associated with corticosteroids was minimized with gradual tapering. A commonly used dexamethasone regimen in patients with brain metastases is a 10-mg intravenous (IV) bolus, followed by 4 to 6 mg PO every six to eight hours before gradual tapering with caution. However, initial corticosteroid use may be reserved for symptomatic patients owing to the common side effects of dexamethasone, including hyperglycemia, peripheral edema, psychiatric disorder, oropharyngeal candidiasis, Cushing’s syndrome, muscular weakness, and pulmonary embolism [31].
Approximately 15% of patients with brain metastases present with seizures, and seizure is frequently associated with supratentorial lesions. Seizures can be managed with antiseizure medications, but anticonvulsants are generally not given prophylactically. In a prospectively randomized study by Forsyth et al. [32], one hundred patients with newly diagnosed brain tumors were randomized to prophylactic anticonvulsants or no anticonvulsants. After a median follow up of 5.44 months, no difference in the rates of seizures at three months or seizure-free survival were observed, suggesting that antiseizure prophylaxis in brain tumor patients is not necessary.
4. Therapeutic Approaches
4.1. Whole Brain Radiotherapy
The palliative effects of WBRT for brain metastases were appreciated over half a century ago, and are widely accepted to extend the median survival of patients to three to six months, compared to one to two months without treatment [5]. Thus, WBRT continues to be the standard of care for patients with brain metastases, especially metastases from lung cancer. Multiple randomized studies have been conducted since the early 1970s to determine the optimal dose and fractionation of WBRT. Selected studies are summarized below in Table 3.
| Dose/fractionation | n | Median Survival | p value | |
|---|---|---|---|---|
| Borgelt/RTOG [33,34] | ||||
| First study (1971–1973) | 30 Gy/10 | 233 | 21 wk | NS |
| 30 Gy/15 | 217 | 18 wk | ||
| 40 Gy/15 | 233 | 18 wk | ||
| 40 Gy/20 | 227 | 16 wk | ||
| 10 Gy/1* | 26 | 15 wk | ||
| Second study (1973–1976) | ||||
| 20 Gy/5 | 447 | 15 wk | NS | |
| 30 Gy/10 | 228 | 15 wk | ||
| 40 Gy/15 | 227 | 18 wk | ||
| 12 Gy/2* | 33 | 13 wk | ||
| Murray/RTOG 91-04 [35] | 30 Gy/10 | 213 | 4.5 mo | NS |
| 54.4 Gy/34 (bid) | 216 | 4.5 mo | ||
| Haie-Meder/French [36] | 36 Gy/6 split course† | 106 | 5.3 mo | NS |
| 25 Gy/10 | 110 | 4.2 mo | ||
| Priestman/Royal College of Radiology [37] | 30 Gy/10 | 263 | 84 days | 0.04 |
| 12 Gy/2 | 270 | 77 days |
* optional randomization in the 1st and 2nd RTOG study. † 18 Gy/3 split course with another 18 Gy/3 within one month. Abbreviations: WBRT: whole brain radiotherapy; wk: weeks; mo: months; NS: not significant
Over 50% of metastases in these studies were of lung origin. Various dose fractionation schedules were studied with no difference in any clinical outcome (i.e., survival times, symptomatic response rates, duration of symptomatic response). However, the ultrarapid schedules of 10 Gy in one fraction and 12 Gy in two fractions were shown to be associated with shorter remission periods, less time to progression of neurologic symptoms, and lower rate of complete disappearance of neurologic symptoms in the RTOG trials [34]. This suggests better palliative effects from the more prolonged schedules. Although a slight survival advantage may be seen with the 30 Gy/10 fractions regimen over the 12 Gy/2 fractions regimen, this is confined to patients with a good initial response [37]. Therefore, the dose fractionation schedule should be chosen based on patients’ prognosis, and the more prolonged dose fractionation schedules should be used for patients who are expected to live long enough to experience neurologic progression as well as the late radiation toxicity associated with large fraction sizes [38].
In the assessment of tumor response, a thorough imaging study of dose response based on tumor size and histology in 108 patients with 336 measurable lesions after WBRT (30 Gy in 10 fractions) was performed by Nieder et al. [39]. An overall response rate of 59% was observed at up to three months. Complete response rate by tumor type was 37% for SCLC, 25% for squamous cell carcinoma, and 14% for non-breast adenocarcinoma. An improved response rate was observed for smaller tumors without necrosis. In a separate study, the biologically effective dose (BED) was generated to compare different dose fractionation schedules by Nieder et al. [40]. Increasing BED was found to correlate with increased partial remission based on tumor size.
4.2. Surgery
In clinical practice, surgical resection is indicated for histological confirmation of diagnosis when the diagnosis is in doubt, and for immediate relief of neurological symptoms due to increased intracranial pressure [12]. Resection of a single brain metastasis has become a standard treatment option after the publication of several prospective studies evaluating the role of surgery combined with WBRT in the treatment of brain metastases [41,42]. In a prospective study of 48 patients by Patchell et al., patients were randomly assigned to surgical removal of the brain tumor followed by radiotherapy or needle biopsy and radiotherapy [41]. Patients began WBRT 36 Gy/12 fractions within 14 days after surgery, whereas patients in the WBRT alone arm began radiotherapy within 48 hours of biopsy or study entry. The recurrence rates at the site of original metastasis for the surgery arm and the WBRT alone arm were 20% and 52%, respectively. The length of time from treatment to the recurrence of the original brain metastasis was significantly shorter for the WBRT alone arm than the surgical arm (median 21 versus >59 weeks, p < 0.0001). The median survival after surgery and adjuvant WBRT was much longer at 40 weeks versus 15 weeks with WBRT alone (p < 0.01). In addition, the patients in the surgical group maintained functional independence (KPS score of ≥70) much longer than the patients treated with radiation alone (median, 38 weeks versus 8 weeks, p < 0.005). The results from this study were confirmed in another study by Noordijk et al. [42], which demonstrated a median survival advantage with the addition of surgery (10 versus 6 months, p = 0.04). This survival advantage was most pronounced in patients with stable extracranial disease and patients ≤60 years old. In contrast, a study of 84 patients by Mintz et al. failed to demonstrate any survival advantage with surgery plus radiation [43]. This is most likely due to the fact that a significant proportion of the patients enrolled presented with active systemic disease and lower functional performance scores compared with the other two studies. The results from all three studies suggest that patients with a single brain metastasis and positive prognostic features, such as the control of extracranial disease and young age, will benefit more from surgical resection followed by WBRT compared with WBRT alone.
Surgery is usually limited to the dominant, symptomatic lesion in patients with multiple metastases. Surgery combined with adjuvant WBRT or stereotactic radiosurgery (SRS) have demonstrated similar survival outcome in patients with multiple lesions compared with patients with single brain metastasis in several single-institution studies [44,45,46]. Furthermore, the survival outcome from resection of all lesions approaches that from resection of a single lesion as shown by Bindal et al. [46]. Modern 30-day surgical mortality rates after resection of a single metastasis range from 0% to 10%. Surgical morbidity includes neurologic deficits (0% to 13%) and non-neurologic complications (0% to 20%) such as thromboembolism, and wound infections [5].
In a separate study, the benefit of adding WBRT after complete surgical resection of a single lesion (based on MRI at 2–5 days after surgery) was investigated by Patchell et al. [47]. The overall median follow up was 43 weeks in the observation group and 48 weeks in the radiation group. Postoperative WBRT was found to have superior local control (90% versus 54%; p < 0.001), distant intracranial control (86% versus 63%; p < 0.01), and overall intracranial control (82% versus 30%; p < 0.001) rates when compared with those who underwent surgical resection alone. However, no overall survival benefit was seen, despite the fact that patients who underwent WBRT were less likely to die from neurological causes than patients in the observation group (14% versus 44%; p = 0.003). The results of this study have recently been confirmed by a randomized Phase III study in Europe, EORTC 22952-26001 [48]. In this study, 359 patients were enrolled with non-progressing primary tumors that had metastasized to the brain. For all patients, brain metastases were initially treated with surgery or radiosurgery. Subsequently, the patients were randomized to prophylactic WBRT or observation. The median survival was 9.5 versus 10 months, respectively. Overall survival was 10.7 versus 10.9 months, respectively. However, WBRT was associated with superior progression-free survival (PFS), intracranial control, and fewer neurologic deaths. This may suggest an overall improvement in patients’ quality of life when WBRT is added to surgical resection.
4.3. Stereotactic Radiosurgery (SRS) with and without WBRT
SRS is a noninvasive technique that delivers a high dose of radiation to a precisely defined target volume through multiple coplanar or non-coplanar intersecting beams, as well as rotational arcs. This approach allows the center of the target to receive a very high dose relative to the surrounding normal brain tissue, as the intersecting beams achieve a very sharp dose gradient (dose fall-off). In recent years, SRS has emerged as an effective alternative to surgery for up to four small brain metastases. This is mainly due to the pseudospherical shape, well-defined margin, and the relatively small size of brain metastases at presentation [49]. As the lesions increase in size, the dose fall-off becomes less rapid, thus increasing the dose to the volume of normal brain immediately adjacent to the tumor. This increases the risk of edema and radiation necrosis, which may require surgery six months or longer after SRS. As a result, SRS is typically delivered to small lesions up to 4 cm in size [50]. The maximum tolerated dose (MTD) was determined in an RTOG Phase I dose escalation trial, RTOG 90-05, based on tumor size [51]. In this study, the MTD was found to be 24 Gy for lesions ≤2 cm, 18 Gy for lesions 2.1–3 cm, and 15 Gy for lesions 3.1–4 cm in maximum diameter. Each dose level was associated with incidence rates of grade 3–5 CNS toxicity of 14%, 20%, and 8%, respectively. The biological effects of SRS on tumors are largely unknown. However, recent studies have suggested the involvement of endothelial cell apoptosis, microvascular dysfunction, or the induction of a T-cell response against the tumor in addition to the radiation-induced DNA damage [52,53,54].
| n | Median FU | Local Control | Median Survival | |
|---|---|---|---|---|
| Zabel et al. [55] | 80 | 6 mo | 96% at 3 mo | 4.5 mo |
| Kim et al. [56] | 77(71 +WBRT) | 8 mo | 85% | 10 mo |
| Williams et al. [57] | 14/ 30 | n/a | 100% | 7.9 mo |
| Sheehan et al. [58] | 273 | n/a | 86% | Adeno: 10 mo |
| Non-adeno: 7 mo | ||||
| Sheehan et al. [59] | 27 | n/a | 86% | 4.5 mo |
| Mariya et al. [60] | 84 | 8.5 mo | 77% at 1 year | 9 mo |
Abbreviations: FU: follow up; WBRT: whole brain radiotherapy; mo: months
Among various studies, patients with good functional performance status, no active systemic disease, and longer time from the diagnosis of primary lung cancer often had better prognosis and lived longer (Table 4). Because of the excellent local control rates achieved by SRS, whether its addition to WBRT will lead to a survival benefit over WBRT alone has been investigated in many studies. This approach could be especially beneficial for patients who are not candidates for a craniotomy because of tumor location or existing medical contraindications. Three randomized studies have evaluated the efficacy of WBRT alone versus WBRT + SRS. Most patients had lung tumor histology in two of the published studies [61,62]. In the first randomized study by Kondziolka et al. [61], the local control rate at one year was found to be significantly better when SRS was added to WBRT in a small number of patients (92% versus 0%, p = 0.0016). However, no survival benefit was found with the addition of SRS. This study defined local recurrence as any increase in lesion size on MRI rather than the more usually employed RECIST (revised response evaluation criteria in solid tumors) system. In addition, this study was not controlled for corticosteroid use, radiation changes, or other factors possibly affecting the lesion size on MRI. Therefore, this study is difficult to interpret. The largest study done to date is the randomized controlled Phase III trial (RTOG-9508) of WBRT alone versus WBRT and SRS (Table 5). This RTOG trial enrolled 333 patients with one to three brain metastases and a KPS of ≥70 [62]. The primary end point was overall survival. No statistically significant difference in overall survival was found between the WBRT and SRS and the WBRT alone arms (6.5 and 5.7 months, respectively, p = 0.1356). However, WBRT and SRS led to a significant decrease in local recurrence at one year despite the fact that 19% of the patients initially assigned to the SRS boost arm did not receive SRS for various reasons (18 versus 29%, p = 0.01). In planned subgroup analysis, increased median survival (6.5 versus 4.9 months; p = 0.039) was associated with WBRT and SRS in patients with a single brain metastasis. An SRS boost also resulted in improvement in KPS and decreased steroid use at six months, suggesting an improvement in the quality of life with the addition of the SRS boost. This is a very important observation, as the primary objective of treatment in patients with brain metastases is the improvement of their quality of life since their overall survival is often very poor. In an unplanned subgroup analysis, an OS benefit was associated with RPA class I, tumor size ≥2 cm, and squamous/NSCLC histology. However, these three cohorts are exploratory subsets that required an adjusted p value of 0.0056 to reach significance [63]. On multivariate analysis using Cox regression, however, RPA class I for both single and multiple lesions and lung primary histology for multiple lesions were found to be significant beneficial prognostic factors. Overall, this study is considered by most to be a negative trial with regard to major end points for multiple metastases. The third study is a three-arm study (SRS, SRS and WBRT, and WBRT alone) from Brown University, reported in abstract form [64]. Superior local control and fewer brain metastases were reported with the addition of an SRS boost. However, no p value was reported, nor was any attempt made to stratify for further surgery, which would have made this a six-arm trial (the size of this trial would not be large enough to support a meaningful analysis for this reason). Furthermore, the SRS dose was unconventional because the tumor dose was not individualized based on tumor size or volume. All of these methodological flaws made this study difficult to interpret.
Table 5.
Randomized study of SRS boost for patients with brain metastases, Radiation Therapy Oncology Group (RTOG) 95-08.
| WBRT + SRS | WBRT alone | SRS alone | p value | |
|---|---|---|---|---|
| (n = 333; 1–3 lesions) | ||||
| Primary end point: Overall survival | 37.5 Gy/15 fx | |||
| 1–3 lesions | 5.7 mo | 6.5 mo | NS | |
| Single brain metastasis | 6.5 mo | 4.9 mo | 0.04 | |
| (planned subgroup analysis) | ||||
| Secondary end points | ||||
| Local control (1 year) | 82% | 71% | 0.01 | |
| Neurologic death rate | 28% | 31% | NS | |
| Performance outcome | ||||
| KPS stable/improved | ||||
| at 3 months | 50% | 33% | 0.02 | |
| at 6 months | 43% | 27% | 0.03 | |
| Mental status | NS | |||
| Unplanned subgroup analysis: Overall survival | ||||
| Largest tumor > 2 cm | 6.5 mo | 5.3 mo | 0.04 | |
| RPA class I | 11.6 mo | 9.6 mo | 0.05 | |
| Squamous/NSCLC | 5.9 mo | 3.9 mo | 0.05 | |
| Other Outcomes | ||||
| Response rate (3 mo) | ||||
| Tumor | 73% | 62% | 0.04 | |
| Edema | 70% | 47% | 0.002 | |
Abbreviations: SRS: stereotactic radiosurgery; WBRT: whole-brain radiotherapy; fx: fraction; NS: not significant; KPS, Karnofsky performance score; RPA: recursive partitioning analysis; NSCLC: non-small cell lung cancer; mo: months
The role of adjuvant WBRT after SRS was investigated in a randomized Phase III trial, Japanese Radiation Oncology Study Group 99-1, by Aoyoma et al. [65]. The primary study end point was overall survival, but the study was not powered to detect any overall survival difference. This study randomized 132 patients with one to four brain metastases to SRS alone or SRS and WBRT. No survival difference was detected (8.0 versus 7.5 mo for SRS versus SRS and WBRT, p = 0.42). The one year intracranial failure rate was decreased with the addition of WBRT (46.8% versus 76.4%, p < 0.001). More importantly, the average time to deterioration based on the Mini-Mental Status Examination (MMSE) was 16.5 months in the SRS + WBRT arm and 7.6 months in the SRS alone arm (p = 0.05) [66]. The results from this study suggest that WBRT can decrease brain failure and its neurological sequalae when added to SRS.
To date, only limited investigations have directly compared surgery and SRS for asymptomatic patients with good functional performance status and limited numbers of brain metastases. In the randomized Phase III study by Roos et al., SRS and surgery were compared in the setting of adjuvant WBRT [67]. However, this study was closed owing to the slow accrual of only 19 patients. Due to the limited number of patients, no difference in CNS failure-free survival, overall survival, or intracranial control was found. In another randomized Phase III study by Muacevic et al., 70 patients were randomized to SRS or microsurgical resection plus WBRT [68]. The inclusion criteria were: single brain metastasis of ≤ 3 cm in an operable site, KPS ≥ 70, and controlled extracranial disease with a life expectancy of at least four months. This study was also closed prematurely due to poor accrual. The final analysis of 64 patients demonstrated no difference in terms of survival, neurological death rates, and local control. However, patients in the SRS alone group did experience more distant recurrences (p = 0.04). This difference was lost after the effects of salvage SRS were accounted for. SRS was associated with shorter hospital stays, less frequent and shorter timed steroid application, and less acute low grade toxicity. But no difference in toxicity profile and quality of life were observed six months after treatment due to the small numbers of patients experiencing adverse effects at that time (SRS: 2, Surgery + WBRT: 6). Due to lack of adequate accrual, no firm conclusions can be made with regard to selection criteria for SRS ± WBRT or surgery and adjuvant WBRT in patients with operable single brain metastasis. We believe that the selection of SRS or surgical resection as initial therapy depends on the size, location, and the presentation of neurological symptoms, as well as each institution’s own policies. These two approaches are complementary in nature and are feasible for most patients as alternative treatment options.
4.4. Systemic Therapy and Radiosensitization
Other approaches to enhance the management of brain metastases have been investigated owing to the poor outcome after WBRT. As shown by Patchell et al., the intracranial recurrence rate after a median follow up of 15 weeks in patients with single brain metastasis treated with WBRT alone was 52% [41]. This rate could be worse in the setting of multiple brain metastases. Such investigations are especially important in the treatment of lung cancer, as it has the highest incidence of brain metastases among all malignancies. In fact, a primary lung cancer can be assumed in 30–70% of patients who have a single brain metastasis [69]. The systemic treatment of brain metastases has generally been difficult owing to the effectiveness of the blood-brain barrier in preventing most chemotherapeutic agents from reaching the CNS. However, the blood-brain barrier may be disrupted when the tumor grows to a certain size, leading to neo-angiogenesis of more permeable vessels. These changes can usually be seen on CT or MRI as the accumulation of contrast medium and the development of edema. In fact, response rates of brain metastases to chemotherapy alone of 43% to 100% for metastases from SCLC and 0% to 38% for metastases from NSLCL have been observed in small single-institution Phase II studies [69]. This has led to a series of prospective studies investigating the radiosensitizing effects of various systemic agents (Table 6). However, no such agent has demonstrated any survival benefit thus far, but several agents have demonstrated increased response rates when combined with WBRT: temozolomide (an oral alkylating agent), nitrosourea + tegafur (masked compound of 5-fluorouracil), motexafin gadolinium (a metallotexaphrin that localizes within tumors more than in normal tissues), and efaproxiral (an allosteric modifier of hemoglobin that leads to increased oxygen release into tissue). Overall, there is no strong evidence supporting the use of radiosensitizers with WBRT in current clinical practice.
| First Author/Study Group | Arms | Response Rate | p Value | Median Survival (months) | p Value |
|---|---|---|---|---|---|
| Komarnicky/RTOG 79-16• [70] | 30 Gy/10 fx | 45% | NS | 4.5 | NS |
| 30 Gy/6 fx | 42% | 4.1 | |||
| 30 Gy/6 fx + misonidazole | 45% | 3.1 | |||
| 30 Gy/10 fx + misonidazole | 45% | 3.9 | |||
| Phillips/RTOG 89-05 [71] | 37.5 Gy/15 fx | 12%* | NS | 6.12 | NS |
| 37.5 Gy/15 fx + BrdUrd | 27%* | 4.3 | |||
| Ushio/Japan [72] | 40 Gy (1.5-2 Gy/fx) | 36% | < 0.05† | 27 | NS |
| 40 Gy + CCNU | 69% | 29 | |||
| 40 Gy + CCNU + Tegafur | 74% | 30.5 | |||
| Robinet/France (NSCLC only) [73] | 30 Gy/10 fx after cisplatin & vinorelbine | 21% | NS | 6 | NS |
| 30 Gy/10 fx concurrent with cisplatin & vinorelbine | 20% | 5.25 | |||
| Neuhaus/Germany (NSCLC or SCLC) [74] | 40 Gy/20 fx | 14/47 | NS | N/A | NS |
| 40 Gy/20 fx + topotecan | 11/49 | ||||
| Guerrieri/Australia (NSCLC only) [75] | 20 Gy/5 fx | 10% | NS | 4.4 | NS |
| 20 Gy/5 fx + carboplatin | 29% | 3.7 | |||
| Knisely/RTOG 01-18 [76] | 37.5 Gy/15 fx | N/A | 3.9 | NS | |
| 37.5 Gy/15 fx + thalidomide | 3.9 | ||||
| Mehta/International‡ [77] | 30 Gy/10 fx | 8.8 mo | 0.004 | 5.8 | NS |
| 30 Gy/10 fx + MGd | 24.2 mo | 5.1 | |||
| Suh/REACH study [78] | 30 Gy/10 fx | 41% | 0.01$ | 4.4 | NS |
| 30 Gy/10 fx + efaproxiral | 54% | 5.4 | |||
| Verger/Spain [79] | 30 Gy/10 fx | 54% | 0.03Ş | 3.1 | NS |
| 30 Gy/10 fx + temozolomide | 72% | 4.5 | |||
| Antonadou/Greece [80] | 40 Gy/20 fx | 67% | 0.017 | 7.0 | NS |
| 40 Gy/20 fx + temozolomide | 96% | 8.6 |
• % survival time in KPS 90-100 range; *best response; † RT vs. RT + CCNU + Tegafur only; ‡ response as neurologic progression in patients from North America; $ response rates as shown are in lung/breast cancer patients only; Ş 90-day freedom from brain metastases;Abbreviations: RTOG: Radiation Therapy Oncology Group; fx: fractions; BrdUrd: bromodeoxyuridine; CCNU: lomustine; MGd: motexafin gadolinium; NS: not significant.
5. Neurocognitive Functioning after Brain Irradiation
WBRT is associated with many acute, subacute, and late side effects. The acute toxicities such as fatigue, hair loss, and skin reaction are mild and self-limiting. The late toxicities are usually observed in patients with limited brain metastases and well controlled extracranial disease because these patients tend to survive longer. Late toxicities include diffuse white matter injury or cerebral atrophy and neurocognitive deficits. Neurocognitive function after cranial irradiation is being evaluated more closely as the efficacy of systemic therapy improves over time. This is of special importance in advanced stage lung cancer owing to the high frequency and short onset of brain metastases from lung cancer.
Neurocognitive impairment has been found frequently in long-term survivors of SCLC after prophylactic WBRT [81,82] and has been seen in patients with existing brain metastases as well. In a cohort of 98 patients with single brain metastasis, four of 38 patients (11%) who survived ≥ 1 year after postoperative WBRT developed severe dementia associated with ataxia and urinary incontinence [83]. All four patients were among a group of 23 patients (17%) who were treated with hypofractionated WBRT with fractions larger than 3 Gy/day. These toxicities were not observed in the patients who were treated with fractions ≤3 Gy/day. However, similar toxicities were seen in one patient who was treated with 3 Gy/day combined with intra-arterial chemotherapy. These findings suggest that large fractions and radiosensitizers, such as chemotherapy, may contribute to severe neurocognitive deficits in long-term survivors from brain metastases. However, such effects may not surface if the patients survive for less than one year. On the other hand, neurocognitive impairment was observed shortly after starting WBRT when patients underwent serial neurocognitive testing as shown by Welzel et al. [84]. But those authors recommended not avoiding WBRT since the neurocognitive dysfunction was restricted mainly to verbal memory. In addition, the risk of disease progression will always outweigh the risk of neurocognitive deficits secondary to brain irradiation since most recurrences can be associated with a neurologic deficit [85].
Some investigators believe that the neurocognitive outcome is directly related to intracranial tumor response after cranial irradiation, as neurocognitive deficits can be partially explained by intracranial tumor progression [86]. Furthermore, improvement in neurocognitive function in responding patients with multiple brain metastases also depends on the initial and posttreatment tumor volume [87,88]. In a study by Li et al., a battery of standardized neurocognitive tests was administered monthly for six months and then every three months until death by trained and certified nurses or clinical research associates to patients with unresectable brain metastases who were treated with WBRT [88]. At two months, patients with greater tumor shrinkage were found to have longer median survival, higher survival rate at one year, and longer time to neurocognitive deterioration. The cognitive gain was especially prominent in executive function and fine motor coordination. Nine patients were alive at 15 months, and the correlation between tumor shrinkage and executive function as well as fine motor coordination persisted. Furthermore, neurocogntive function was found to be influenced mostly by disease progression early on after WBRT. The patients who became long-term survivors also experienced larger tumor volume reductions after WBRT, and they had the best neurocognitive outcome.
The combination of SRS and WBRT over WBRT alone has been supported by the results of RTOG 9508 for patients with single brain metastasis, good functional performance status, and no active extracranial disease [62]. No difference in neurological deaths or mental status at six months between the two arms of this study was found. In addition, the rate of neurological deaths in the SRS boost arm was within the 25–50% range reported in other surgery or SRS series [62]. Because of the known toxicity associated with WBRT and the lack of any difference in survival between SRS alone and SRS plus WBRT as described in previous sections, the use of SRS alone as initial treatment for patients with a limited number of lesions has been advocated by many. The difference in neurocognitive function between patients undergoing SRS alone and those undergoing SRS and WBRT has been investigated in two prospective randomized controlled trials [66,89]. In the study by Aoyama et al. [66], neurocognitive function was assessed by serial MMSE after SRS + WBRT or SRS alone. No statistical difference in MMSE scores was found between the two arms, nor was any statistically significant difference found in the rate of MMSE score deterioration after a median follow up of 5.3 months. However, the time to neurological deterioration was significantly longer in patients who received SRS + WBRT than in those who received SRS alone (16.5 months versus 7.6 months, p = 0.05). This was thought to reflect the higher number of intracranial recurrences in the SRS alone group (11 versus 3 patients, p < 0.0001). Five patients who underwent SRS + WBRT, but none in the SRS alone arm, suffered a radiation toxic event. Although not statistically significant, a trend of continuous neurocognitive deterioration became prominent after 24 months in long-term survivors after SRS and WBRT. These findings from Aoyama et al. corroborate those from Regine et al. and Li et al. in that WBRT may help to improve neurocognitive function in patients with brain metastasis through its therapeutic effects on a short-term basis [66,86,88]. Moreover, significant numbers of patients treated with SRS alone may experience recurrence with neurological symptoms, leading to the recommendation that WBRT be used whenever indicated [85]. However, the late toxicity in terms of neurocognitive function from WBRT in long-term survivors cannot be ignored and warrants further investigation, as such effects may be masked owing to the short survival time of many patients on these studies of mostly far less than two years. Recently, the effects of initial treatment with SRS alone or SRS combined with WBRT on learning and memory function were investigated in a prospective randomized study by Chang et al. [89]. Most patients in this study had NSCLC, 1-2 lesions, and RPA class I or II. The GPA indices between the two arms were also well balanced. This study was designed to detect a 5-point decline in the Hopkins Verbal Learning Test–Revised (HVLT-R). The study was stopped when a significant decline in the HVLT-R score at four months was observed in the SRS plus WBRT arm compared with the SRS alone arm after accrual of 58 patients. Overall, the total recall difference persisted at six months. The patients who received SRS + WBRT demonstrated greater declines in executive function as well. Increased intracranial failure was observed in the SRS alone arm, with approximately 87% of the patients requiring salvage therapy. However, the one year survival rate was higher in the SRS alone arm (63% versus 21%, p = 0.003), possibly because of earlier systemic therapy in the SRS group and greater systemic disease burden in the SRS + WBRT arm. The authors argued for the initial treatment to be SRS alone with close follow up since intracranial recurrences are likely to be asymptomatic if discovered in their early stages by imaging studies.
Given the evidence described above, WBRT does seem to have a toxic effect on neurocognitive function over time. However, neurocognitive deterioration can be observed only in long-term survivors. Therefore, WBRT may be omitted in patients with good functional performance status and limited numbers of metastases if those patients have limited extracranial disease and are aware of the risk of intracranial failure associated with SRS alone and the risk of potential neurological deficits as a result of such failures. Thus, we recommend offering SRS alone to patients who can be monitored closely (e.g., every two months) with MRI. SRS plus WBRT should still be given serious consideration for patients with good functional performance status with controlled extracranial disease and single brain metastasis given the observed survival benefit observed in RTOG 9508 [62]. In contrast, WBRT can actually improve neurocognitive function of patients with radiosensitive tumors, such as lung cancer, poor prognosis, and a short lifespan. Thus WBRT should be recommended for such patients. In recent years, donepezil, a drug used to treat Alzheimer’s disease, was shown to have a positive effect on the cognitive function of patients who underwent irradiation for brain tumors [90]. The potential role of memantine, an agent that blocks the pathologic stimulation of the N-methyl-d-aspartate (NMDA) receptor (a receptor involved in learning and memory), in alleviating neurocognitive deficits from WBRT is being investigated in a randomized Phase III study, RTOG 0614, with results pending [91].
Also worth mentioning is the potential contribution of anticonvulsants to the development of late neurological symptoms from WBRT [92]. Therefore, any systemic agents (e.g., anticonvulsants, steroids) that can possibly influence the symptomatic outcome from brain irradiation should be carefully assessed and controlled for in future prospective studies to reach firm conclusions regarding the incidence of late radiation toxicity from brain irradiation.
6. Prophylactic Brain Irradiation (PCI)
6.1. SCLC
SCLC is known for its high risk of early hematogeneous dissemination, especially to the brain. Upon initial diagnosis, up to 24% of patients may have brain metastases when MRI of the brain is included as part of the staging evaluation [93]. Most patients with SCLC will ultimately develop brain metastases if they live long enough. Prophylactic WBRT has been advocated by many to delay the development of brain metastases and reduce the rate of distant relapse in the brain [94,95]. Many older randomized studies have demonstrated statistically significant reductions in brain metastases from 16–73% to 0–13% with the use of PCI, although none was able to demonstrate any survival benefit [96,97,98,99,100,101]. This is mainly from the lack of patient stratification based on tumor stage (limited versus extensive) and response to definitive therapy. However, PCI was suggested to improve survival in patients who had a complete response (CR) to induction treatment in several retrospective studies [102,103,104]. Subsequent randomized studies of PCI have focused on patients who have achieved a CR after initial treatment. Although these studies could not demonstrate a survival advantage with PCI individually, a 5.3% increase in 3-year OS in patients who received PCI (p = 0.01) was detected when individual data from 987 CR patients enrolled between 1965 and 1995 into seven trials comparing PCI to observation were analyzed in a meta-analysis [105]. The Most of the patients were men (75%) with good performance status (97%) and limited-stage disease (86%). CR in the chest was assessed by chest X-ray, bronchoscopy, or thoracic CT. The cumulative incidence of brain metastasis at three years decreased from 58.6% in the observation group to 33.3% in the PCI group (p < 0.001). A trend toward decreased risk of brain metastasis was observed with increased radiation dose when four dose regimens were compared (8 Gy/1 fraction, 24-25 Gy/8-12 fractions, 30 Gy/10 fractions, and 36–40 Gy/18–20 fractions, p = 0.02). In addition, PCI seems to have a greater effect on the incidence of brain metastases if delivered sooner after induction therapy (p = 0.01). The association of PCI and a survival benefit was demonstrated again in CR patients in another meta-analysis of 12 randomized trials involving 1547 patients by Meert et al. [106]. Based on these meta-analyses, PCI became a part of the standard of care for SCLC patients in CR.
The survival advantage associated with PCI was also demonstrated in patients with extensive stage SCLC who had no response to four to six cycles of chemotherapy [107]. Disease-progression-free survival was significantly longer in the PCI group (14.7 weeks versus 12.0 weeks, p = 0.02), as was median survival (6.7 months versus 5.4 months, p = 0.003). The risk of symptomatic brain metastases was significantly decreased with PCI at one year (14.6% versus 40.4%, p < 0.001). Notably, brain imaging was not required for this trial. Therefore, many patients in the PCI group may have been treated for asymptomatic brain metastasis.
Based on the evidence summarized above, PCI should be offered to any patient with limited stage SCLC with CR after initial treatment, or extensive stage SCLC with any response after initial chemotherapy as the standard of care.
Although improvement was seen with PCI, a 33% incidence of brain metastases is still observed three years after PCI as demonstrated in a meta-analysis by Aupérin et al. [105]. Because of the poor prognosis associated with brain metastases after PCI and a possible dose-response effect observed in the same meta-analysis, a Phase III randomized prospective study was conducted by the PCI Collaborative Group to address the question of dose effects in patients with limited stage SCLC and CR after definitive therapy [108]. The standard dose of 25 Gy/10 fractions was compared to 36 Gy delivered in either 18 daily fractions or 24 twice-daily fractions in this study. No statistically significant difference in the total incidence of brain metastases was found at two years between the two dose groups (29% standard dose groups versus 23% higher dose group, p = 0.80). However, a significantly lower incidence of brain metastases as the first site of failure at two years was observed in the higher dose group (6% versus 12%, p = 0.005). The higher dose group had a lower two year overall survival rate (37% versus 42%, p = 0.05), which was most likely due to increased intrathoracic failure in this group relative to the standard dose group (48% versus 40% at two years, p = 0.02). These findings imply that intrathoracic disease control affects both the incidence of brain metastases after PCI and overall survival after multimodality treatment. On the other hand, these findings may also reflect the heterogeneous T and N categories of the patients among the study arms, possibly leading to the prevalence of poorer intrathoracic control for locally advanced tumors seen more commonly in one arm over another. Furthermore, the utility of higher doses for PCI is only rational in a select group of patients in whom intrathoracic disease is well controlled. Currently, 25 Gy delivered in 10 fractions is still recommended as the standard of care given the lack of evidence for increased intracranial control associated with higher doses and the concern over potential adverse effects on neurocognitive function from WBRT. However, other dose fractionation regimens are reasonable alternatives as well (e.g., 30 Gy in 15 fractions).
6.2. NSCLC
The development of brain metastases is also prevalent in NSCLC. In stage III patients, the incidence of brain metastases during the course of treatment can reach approximately ≥ 50% [109,110]. Nonsquamous histology, bulky mediastinal nodes (>2 cm), increased numbers of positive mediastinal nodes, involvement of several nodal stations, younger age, the use of neoadjuvant chemotherapy, and prolonged survival were all found to be associated with the increased incidence of brain metastases in various studies [110,111,112,113,114,115,116,117]. Brain metastasis is also usually the most common site of distant failure [118,119]. The results of selected studies on the incidence of brain metastasis after combined modality treatment are presented in Table 7.
Table 7.
Incidence of brain metastases after combined modality treatments for non-small cell lung cancer (NSCLC).
| Stage | Treatment | Brain Metastases (%) | Median survival (mo) | ||
|---|---|---|---|---|---|
| Overall Survival | Brain as the 1st site of failure | ||||
| Wang et al. [110] | III | S ± adjuvant chemo | 38.1 | 26.5 | 29.5 |
| Ceresoli et al. [114] | IIB/III | Chemo/RT ± S | 29 (2 yr) | 22 | 21 |
| Robnett et al. [115] | II/III | Chemo/RT | 30% (2 yr) | 19 | 14.5 |
| Komaki et al. [117] | II/III | RT | N/A | 6-18 | 9 |
| Mamon et al. [118] | IIIA | Chemo/RT/S | 40 (3 yr) | 34 (3 yr) | 21 |
| Germain et al. [119] | III | Chemo/RT | 27 | 21 | 19.2 |
| Carolan et al. [120] | III | Chemo/RT ± S | 34.9 | 18.1 | 25.6 |
Abbreviations: mo: months; S: surgical resection; Chemo: chemotherapy; RT: radiotherapy; yr: years
| Primary Therapy | Brain | Overall | Neurocognitive Deficits Associated with PCI | |||
|---|---|---|---|---|---|---|
| Failures (%) | Survival (%) | |||||
| No PCI | PCI | No PCI | PCI | |||
| Cox et al. [121] | RT | 13 | 6 | NA | Not formally assessed | |
| Russell et al. [122] | RT | 19 | 9 | 21 | 13 | Not formally assessed |
| Umsawasdi et al. [123] | Chemo/RT ± S | 27 | 4 | ~ 17.5% after 39 mo with or without PCI | Not formally assessed | |
| Pöttgen et al. [124] | Chemo/ RT/S | 34.7 | 7.8 | 16%-18% at 5 years with or without PCI | None after five years | |
| Movsas
et al. [125] (Outcome at one year) | RT/S ± Chemo | 18 | 7.7 | 76.9 | 75.6 | Immediate recall and delayed recall |
Abbreviations: PCI: prophylactic cranial irradiation; RT: radiotherapy; Chemo: chemotherapy; S: surgical resection; mo: months
Because of the poor prognosis associated with brain metastases and its prevalence in locally advanced NSCLC, the potential role of PCI has been investigated in several studies (Table 8). Although found to significantly decrease the incidence of intracranial metastases by some [121,122,123,124,125], no randomized study has been able to demonstrate any survival benefit from PCI in locally advanced NSCLC. Thus, PCI is currently not a part of the standard of care for locally advanced NSCLC. However, the prognostic factors found in retrospective studies may guide the section of patients for future prospective randomized studies to identify a subgroup of patients for whom PCI can lead to a survival benefit.
6.3. Neurocognitive Functioning after PCI
Significant late toxicity has been reported for patients with SCLC treated with PCI and concurrent chemotherapy or treated with large fractions [126]. Two randomized controlled trials have specifically examined neurocognitive function after PCI for SCLC [127,128]. Arriagada et al. randomized 300 patients with SCLC in complete remission to PCI versus observation in a prospective study from France [127]. Neuropsychological assessment was performed at baseline and on follow up to 48 months by a neurologist for 229 patients. The results of 83% baseline testing were considered normal in both arms. Overall, no difference was found between the two treatment arms in terms of higher functions, mood, walking, cerebellar function, tendon reflexes, sensibility, or cranial nerve function after two years. No statistically significant difference in the two year rates of abnormalities between the two arms was observed. In a similar study by Gregor et al. [128], 314 patients with limited stage SCLC in CR were randomized to PCI or no PCI. Neurocognitive function was formally assessed with a battery of tests, including the national adult reading test, the paced auditory serial addition task, the Rey Osterrieth complex figure test, and the auditory verbal learning test. The quality of life and anxiety and depression were assessed with Rotterdam symptom checklist and the Hospital anxiety and depression scale. Tests of cognitive function revealed cognitive impairment in 24% to 41% of patients in each group. However, no significant difference was found between the two arms at the baseline. Furthermore, no difference between the two arms was observed in neurocognitive function or gross quality of life, level of anxiety, or depression at one year. Findings were similar in a recent prospective randomized trial evaluating PCI in locally advanced NSCLC by Pöttgen et al. [124]. Of 11 evaluable long-term surviving patients, no deficits in attention, memory, associative learning, and information processing were found by using a battery of neurocognitive tests in patients who received PCI and those who did not. However, this lack of difference can also be explained by the small number of patients. In contrast, increased decline in both immediate and late recall was observed in the Hopkins verbal learning test at one year when patients with stage III NSCLC underwent PCI 30 Gy in 15 fractions in the Phase III prospective randomized study RTOG 0214 [125]. These findings may clarify neurocognitive function after PCI as the findings mature. The inclusion of neuropsychometric testing has not been common practice in the past. Its inclusion in current and future trials will enhance our understanding of the long-term neurocognitive effects of PCI and WBRT in general.
7. Local Therapy for Synchronous, Solitary Brain Metastasis from NSCLC
Some proportion of patients with NSCLC present with synchronous brain metastasis. Five year overall survival rates of over 20% have been reported after both the brain and the primary site were treated aggressively (Table 9).
| n | Stage of Chest Disease | Brain Therapy | Definitive Therapy | 5 Year Overall Survival (%) | |
|---|---|---|---|---|---|
| Hu et al. [129] | 84 | I-III | S/SRS | RT ± Chemo | 7.6 |
| Stage I: 50 (3 year) | |||||
| Flannery [130] | 42 | I-III | SRS | S ± chemo/RT | 21 |
| Bonnette et al. [131] | 99 | I-III | S | S | 11 |
| Billing et al. [132] | 28 | I-III | S/WBRT | S ± chemo/RT | 21.4 |
| Ampil et al. [133] | 72 | I-III | WBRT/SRS | RT | 13% (1 year) |
| Lo et al. [134] | 18 | I-III | S/SRS | S | 27 |
Abbreviations: S: Surgical resection; SRS: stereotactic radiosurgery; Chemo: chemotherapy; WBRT: whole brain radiotherapy
After SRS, overall survival was significantly higher for those given definitive (as opposed to non-definitive) thoracic therapy in a study of 42 patients by Flannery et al. [130]. Furthermore, higher survival was demonstrated to be associated with early stage disease in the chest and better KPS [129,130,132]. A survival benefit was also observed for patients with more than one synchronous brain metastasis when those patients also had good functional performance status and received thoracic therapy [135,136,137]. All of these findings support the delivery of local therapy to the chest for patients with good functional performance status and limited numbers of brain metastasis. However, the survival benefit from local therapy still needs to be validated in a prospective randomized controlled trial.
8. Future Investigations
Given the lack of any survival benefit demonstrated for adjuvant WBRT after surgical resection or SRS and its potential neurotoxicity, the utility of SRS to provide a boost dose to the tumor bed after craniotomy for patients with limited numbers of brain metastases has been investigated in recent years. In a study of 72 patients (43% NSCLC) with 1-4 brain metastases and 76 cavities after surgical resection, a median dose of 18.0 Gy was delivered to the median 79% isodose line at the periphery of the tumor bed [138]. The actuarial local control rate in this study was 79% at two years, and the distant control rate was 47% at 12 months. Three patients underwent surgical resection of a region of necrosis. Use of less conformal plans translated into a local control rate of 100%, thus the authors recommended a planning target volume margin of 2 mm around the resection cavity. In a similar study of 52 patients (46% NSCLC) with up to four lesions, a local failure rate of 7.7% was observed after a median follow up of 13 months [139]. The distant failure rate was 44% after a median of 16 months after resection, and the median survival was 15 months. Similar results have been reported in other single-institution studies [141,142]. Equivalent local control between surgery followed by adjuvant WBRT or SRS is suggested by these small studies, but these findings remain to be validated in a prospective randomized study. However, the risk of distant recurrence remains high with adjuvant SRS alone, making this approach inappropriate for patients with solitary brain metastasis, good functional performance status, and primary disease controlled locally because of the potential for aggressive treatments to improve survival in these patients, especially for patients with lung cancer [142,143]. Therefore, WBRT may still be warranted in patients with good prognosis in addition to surgery and adjuvant SRS, if the potential toxicity is tolerable. The feasibility of this approach was investigated in a small study of 27 patients (70% NSCLC); the actuarial two-year local control was 94%, and the two year actuarial incidence of new brain metastasis was 30% [144]. Only one patient required reoperation for symptomatic radiation necrosis at 16 months after treatment. The median survival was 17.6 months. Whether this approach will lead to a survival benefit still requires further investigation in a randomized trial.
As mentioned previously, SRS can spare adjacent normal tissue by achieving a sharp dose gradient at the periphery of the tumor target volume. However, this advantage is diminished with large lesions. To spare normal brain tissue, the dose delivered needs to be decreased to avoid potential neurotoxicity [51,145]. The tumor response is usually impaired as a result of this [146]. Therefore, fractionated stereotactic radiotherapy has been proposed owing to the advantages of reoxygenation of hypoxic cells within large lesions and significant increases in late-responding tissue sparing if the radiation dose is fractionated [147]. Thus, the therapeutic ratio can be significantly increased when large brain metastases are treated with a high dose delivered in several fractions with a stereotactic set-up. This concept has been validated in a small study, in which patients with large brain metastases (average volume 21.2 cm3) were treated safely with fractionated stereotactic radiotherapy, and a local control rate of 83% has been achieved [148]. These findings were confirmed in a larger retrospective study of patients with large brain metastases treated with this technique [149]. Similarly, many single-institution studies have shown excellent clinical outcome and toxicity profile from fractionated stereotactic radiotherapy with or without use of a frame (Table 10). These studies suggest that local control seems to be related to tumor size [155] and that intracranial control outside of the treated area seems to be poor when fractionated stereotactic radiotherapy is used alone. However, its combination with WBRT was shown to be feasible with good intracranial control and toxicity profile [156,157], which may be a better option for patients who present with neurological deficits from large, but few, brain metastases. However, the patient selection criteria for this technique, alone or as a boost, needs further investigation in prospective studies. Also, it is important to be aware that a bigger margin than that used for SRS may be needed when patients are not precisely immobilized.
| N (patients/ metastases) | Dose (Gy) | Response | 1-year Overall Survival (%) | Distant Failure in the Brain | Toxicity | |
|---|---|---|---|---|---|---|
| De Salles et al. [148] | 26/41 | 6 Gy × 2-3 | LC 83% | NR | NR | NR |
| FU 2-18 mo | ||||||
| Nishizaki et al. [149] | 71/148 | 7.8-30.1 Gy/1-3 fractions | Median FU: 11 mo | 47 | 35.2 % at a median FU of 6.6 mo | No permanent symptoms from radionecrosis |
| LC: 83% | ||||||
| Manning et al. [150] | 32/57 | 6-12 Gy × 3; | 31% ≤ 25% | 44 | 13% after ≥ 6 mo | Seizure: 12% |
| WBRT for all patients | 31% > 25% | Radionecrosis: 6% | ||||
| 16% PD | ||||||
| Aoyama et al. [151] | 87/159 | 8.75 Gy × 4 | 1 yr LC: 81% | 39 | 60% at 1 yr | Symptomatic radionecrosis: 2.7% |
| 2 yr LC: 69% | ||||||
| Aoki et al. [152] | 44/65 | 18-30 Gy/ 3-5 fractions | 1 yr LC: 71.9% | 50.8 | 31% at 1 yr | No severe complications |
| Ernst-Stecken et al. [153] | 51/72 | 6 Gy × 5 | 1 yr LC: 76% | Median survival: 11 mo | NR | Increased radionecrosis if V4Gy > 23 cm3 (70% vs. 14%, p = 0.001) |
| 7 Gy × 5 | ||||||
| SRT alone or with WBRT | ||||||
| Fahrig et al. [154] | 150/228 | 6-7 Gy × 5 | CR: 46% | 66 | NR | 10% toxicity; 1 symptomatic hemorrhage from melanoma; 2 had to be operated on for radionecrosis; |
| 4 Gy × 10 | 31% | |||||
| 5 Gy × 7 | 47% | |||||
| Median FU: 28 mo | No grade 5 toxicity; | |||||
| No toxicity with 4 Gy × 10. | ||||||
| Kwon et al. [155] | 36/66 | 20-36 Gy/ 4-6 | 1 yr LC: 68.2%; | 43.9 | 25.9% at a median FU of 6.47 mo | Radionecrosis: 5.8% |
| Tumors < 1 cm3 had better LC | ||||||
| Lindvall et al. [156] | 61/77 | 8 Gy × 5 | LC: 84% (no WBRT); 100% (WBRT); mean 3.7 mo after SRT | Mean survival from time of SRT: 6.1 mo | 25% after a median of 3.7 mo after SRT alone, but none in WBRT + SRT patients who were followed radiologically | 4.7% radionecrosis after SRT + WBRT |
| ± WBRT | ||||||
| Giubilei et al. [157] | 30/44 | 6 Gy × 3 | 1 yr LC: 86.1% | 36.6 | 12.1% at 1 yr | No acute or late complications |
| 8 Gy × 4 | ||||||
| WBRT for all patients |
Abbreviations: CR: complete response; FU: follow up; NR: not reported; LC: local control; mo: months; WBRT: whole brain radiotherapy; PD: progressive disease; SRT: stereotactic radiotherapy; yr: year
In patients with good prognostic factors, such as 1–3 brain metastases, RPA class 1–2, controlled extracranial disease, GPA of ≥ 2.5, young age, and high KPS scores, aggressive treatment of brain metastasis with WBRT followed by a regular external beam boost to the gross tumor or the surgical bed has been investigated. This approach has been consistently shown to be associated with increased local control comparable to that reported for WBRT + SRS, as well as a median survival time of over 12 months, significantly better than WBRT alone with or without surgical resection [158,159]. Radiation delivered as a simultaneous integrated boost with intensity-modulated radiotherapy has been shown to produce a sharper dose gradient than that from WBRT followed by SRS for the treatment of brain metastasis [160,161]. This leads to improved normal tissue sparing owing to the ability to optimize the dose to the normal brain and to account for dose spillage from the boost dose to the adjacent brain tissue in the planning of WBRT. This not only spares more normal brain tissue but also shortens treatment time for patients with multiple lesions. The feasibility of this approach has been demonstrated in a single-institution Phase I study through the use of helical tomotherapy, which combines delivery of intensity-modulated radiotherapy with megavoltage CT imaging for precise radiation delivery through image guidance [162]. In this study, 48 patients (50% of whom had lung cancer) were treated with WBRT 30 Gy in 10 fractions and a simultaneous integrated boost to the brain metastases safely escalated from 5 to 30 Gy in 10 fractions. No grade 3–5 dose limiting toxicity was encountered. However, this study had a median follow up of only 7.72 months and a median overall survival time of only 5.29 months. Given the small number of patients in this study, no firm conclusions can be made regarding tumor response and survival outcome. Worth mentioning is the application of helical tomotherapy in the treatment of recurrent brain metastases from lung and breast cancer with a simultaneous integrated boost. The safe delivery of 30 Gy to the gross disease and 15 Gy to the whole brain in 10 fractions for up to 11 lesions was reported by Sterzing et al. [163]. In this report, an excellent dose conformality index was achieved, and no severe toxicity was observed; the patients remained recurrence-free at six and 12 months of follow up. Based on this limited evidence, the simultaneous integrated boost approach may be an excellent treatment approach with intensity modulation of doses to the target and the adjacent brain tissue. Depending on the degree of immobilization, no standard has been established regarding the planning target volume margin for gross disease, and margins from 0 to 10 mm have been reported [158,161,162,163]. Further conclusions regarding this matter can be made as the existing data mature. Recently, excellent dose sparing of radiosensitive structures, such as the hippocampus, was reported when brain metastases were treated with the simultaneous integrated boost approach, which further supports the use of this approach for normal tissue sparing [164,165].
Other future work involves targeting therapy to the epidermal growth factor receptor (EGFR) family of four homologous receptors, EGFR (ERBB1), HER-2/neu (ERBB2), HER-3 (ERBB3), and HER-4 (ERBB4). EGFR activation leads to receptor tyrosine-kinase activation and activation of a series of downstream signaling activities that mediate tumor cell proliferation, migration, invasion, and the suppression of apoptosis [166]. As a result, inhibiting EGFR by binding its intracellular adenosine triphosphate-binding site with small-molecule tyrosine kinase inhibitors has been investigated as a treatment strategy for NSCLC [167]. Among these inhibitors, erlotinib has shown a survival benefit when combined with chemotherapy for advanced stage NSCLC [168]. However, tumor response is mainly limited to patients who possess somatic mutations in the kinase domain of the EGFR gene [169]. These patients are usually of East Asian descent, female, nonsmokers, with adenocarcinoma [170]. In a small series of 41 patients with brain metastasis from lung adenocarcinoma, gefitinib was shown to have antitumor activity (10% major response). Intracranial control was associated with previous WBRT [171]. In another study by Kim et al. [172], median progression-free survival and overall survival times of 7.1 and 18.8 months were observed in East Asian, nonsmoking patients with lung adenocarcinoma and asymptomatic synchronous brain metastasis after treatment with either gefitinib 250 mg or erlotinib 150 mg once daily. Both studies suggest a potential role for EGFR inhibitors in the treatment of brain metastases. Additive effects may be produced when both EGFR inhibitors and WBRT were delivered, as patients who received both treatments have better disease control and longer overall survival [171,172]. Several studies have demonstrated increased response to EGFR inhibitors, as well as prolonged time to intracranial progression and improved overall survival, in patients with mutations in the EGFR gene [173,174]. The presence of EGFR mutations was shown to enhance radiation response; for patients with EGFR mutation and brain metastases from lung adenocarcinoma, WBRT delivered concurrently with EGFR inhibitors produced a response rate of 84% [175]. However, severe toxicities, including grade 5 interstitial lung disease, have been reported in patients treated with concurrent erlotinib and WBRT [176,177]. The unexpected lung toxicity from EGFR inhibitors needs further investigation for the safe administration of these drugs.
9. Conclusions
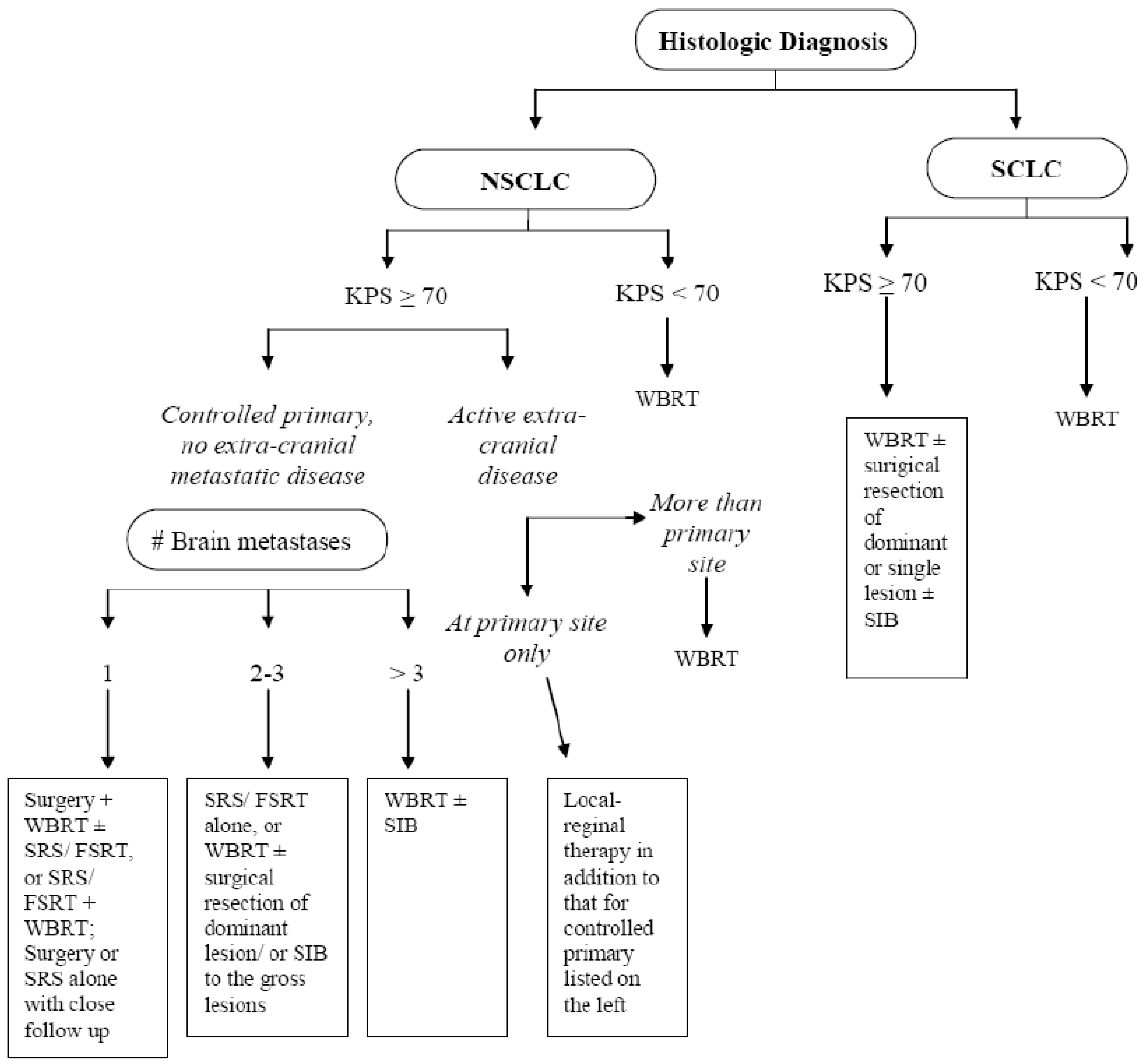
In summary, patients with brain metastases from lung cancer have several treatment options, which are summarized in Figure 1. The choice of treatment will greatly influence the overall prognosis for patients with advanced stage lung cancer. Based on current evidence, combined modality treatment of brain metastases has greatly improved the survival of patients with single lesions, good functional performance status, and controlled extracranial disease, as demonstrated in prospective randomized studies. Neurocognitive deterioration remains a concern for patients with excellent functional performance status who are receiving WBRT ± SRS. However, radiotherapy may improve neurocognitive function in a select group of patients who present with neurological impairment from brain lesions at baseline shortly after treatment. PCI for SCLC is currently part of the standard of care, but PCI for NSCLC is still investigational. Local therapy should be considered for patients with early stage intrathoracic disease and brain as the sole site of metastasis. To further improve treatment outcome for brain metastasis, options including an SRS boost to the surgical bed alone, fractionated stereotactic radiotherapy, and WBRT with a simultaneous integrated boost are currently under investigation. Among these options, fractionated stereotactic radiotherapy allows the delivery of a high dose in a few fractions, which is a more biologically sound approach for large lesions. This technique can also potentially decrease the toxicity from SRS because a lower dose is delivered per fraction over multiple fractions, thus greatly reducing the risk of late normal tissue damage. WBRT with a simultaneous integrated boost allows dose optimization such that a high dose is given to the target volume while the dose delivered to the whole brain is kept below a certain threshold. This achieves increased tumor dose, while sparing as much normal brain tissue as possible to prevent neurological toxicity from radiotherapy. Such an approach holds great promise in the future. Radiosensitization is not currently indicated clinically. However, the use of EGFR inhibitors ± WBRT has demonstrated good response of intracranial disease in patients with EGFR mutations, and this strategy also warrants further clinical investigation.
Figure 1.
Algorithm for the initial treatment of brain metastases from lung cancer.

References
- Schouten, L.J.; Rutten, J.; Huveneers, H.A.; Twijnstra, A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 2002, 94, 2698–2705. [Google Scholar] [CrossRef]
- Barnholtz-Sloan, J.S.; Sloan, A.E.; Davis, F.G.; Vigneau, F.D.; Lai, P.; Sawaya, R.E. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the metropolitan Detroit cancer surveillance system. J. Clin. Oncol. 2004, 22, 2865–2872. [Google Scholar]
- Kwok, Y.; Patchell, R.A.; Regine, W.F. Management of overt central nervous system metastases: Brain and spinal cord. In Principles and Practice of Lung Cancer, 4th edition; Pass, H.I., Carbone, D.P., Minna, J.D., Johnson, D.H., Scagliotti, G.V., Turrisi, A.T., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 911–926. [Google Scholar]
- Hirsch, V. Systemic therapies in metastatic non-small-cell lung cancer with emphasis on targeted therapies: The rational approach. Curr. Oncol. 2010, 17, 13–23. [Google Scholar]
- Larson, D.A.; Rubenstein, J.L.; McDermott, M.W. Metastatic cancer to the brain. In Cancer: Principles and Practice of Oncology, 8th edition; DeVita, D.T., Lawrence, T.S., Rosenberg, S.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 2462–2475. [Google Scholar]
- Gavrilovic, I.T.; Posner, J.B. Brain metastases: Epidemiology and pathophysiology. J. Neurooncol. 2005, 75, 5–14. [Google Scholar] [CrossRef]
- Johnson, J.D.; Young, B. Demographics of brain metastasis. Neurosurg. Clin. N. Am. 1996, 7, 337–344. [Google Scholar]
- Schottenfeld, D. The etiology and epidemiology of lung cancer. In Principles & Practice of Lung Cancer, 4th edition; Pass, H.I., Carbone, D.P., Minna, J.D., Johnson, D.H., Scagliotti, G.V., Turrisi, A.T., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 3–22. [Google Scholar]
- Kelly, K.; Bunn, P.A. Is it time to reevaluate our approach to the treatment of brain metastases in patients with non-small cell lung cancer? Lung Cancer 1998, 20, 85–91. [Google Scholar] [CrossRef]
- Cox, J.D.; Yesner, R. Adenocarcinoma of the lung – recent results from VA Lung Group. Am. Rev. Respir. Dis. 1979, 120, 1025–1029. [Google Scholar]
- Shi, A.A.; Digumarthy, S.R.; Temel, J.S.; Halpern, E.F.; Kuester, L.B.; Aquino, S.L. Does initial staging or tumor histology better identify asymptomatic brain metastases in patients with non-small cell lung cancer? J. Thorac. Oncol. 2006, 1, 205–210. [Google Scholar]
- Zabel, A.; Debus, J. Treatment of brain metastases from non-small-cell lung cancer (NSCLC): Radiotherapy. Lung Cancer 2004, 45, 247–252. [Google Scholar] [CrossRef]
- Posner, J.B. Brain metastases: 1995. A brief review. J. Neurooncol. 1996, 27, 287–293. [Google Scholar] [CrossRef]
- Davis, P.C.; Hudgins, P.A.; Peterman, S.B.; Hoffman, J.C., Jr. Diagnosis of cerebral metastases: Double-dose delayed CT vs contrast-enhanced MR imaging. Am. J. Neuroradiol. 1991, 12, 293–300. [Google Scholar]
- Schaefer, P.W.; Budzik, R.F., Jr.; Gonzalez, R.G. Imaging of cerebral metastases. Neurosurg. Clin. N. Am. 1996, 7, 393–423. [Google Scholar]
- Wen, P.Y.; Loeffler, J.S. Overview of the clinical manifestations, diagnosis, and management of patients with brain metastases. UpToDate. 2010. Available online: http://www.uptodate.com (Accessed on 26 May 2010).
- Chang, D.B.; Yang, P.C.; Luh, K.T.; Luh, K.T.; Kuo, S.H.; Hong, R.L.; Lee, L.N. Late survival of non-small cell lung cancer patients with brain metastases: Influence of treatment. Chest 1992, 101, 1293–1297. [Google Scholar] [CrossRef]
- Richards, P.; McKissock, W. Intracranial metastases. Br. Med. J. 1963, 5322, 15–18. [Google Scholar] [CrossRef]
- Lang, E.F.; Slater, J. Metastatic brain tumors: Results of surgical and nonsurgical treatment. Surg. Clin. North Am. 1964, 44, 865–872. [Google Scholar]
- Zimm, S.; Wampler, G.L.; Stalblein, D.; Hazra, T.; Young, H.F. Intracranial metastases in solid tumor patients: Natural history and results of treatment. Cancer 1981, 48, 384–394. [Google Scholar] [CrossRef]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Gaspar, L.E.; Scott, C.; Murray, K.; Curran, W. Validation of the RTOG recursive partitioning analysis (RPA) classification for brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 1001–1006. [Google Scholar] [CrossRef]
- Kepka, L.; Cieslak, E.; Bujko, K.; Fijuth, J.; Wierzchowski, M. Results of whole-brain radiotherapy for patients with brain metastases from lung cancer: The RTOG RPA intra-classes analysis. Acta Oncol. 2005, 44, 389–398. [Google Scholar] [CrossRef]
- Videtic, G.M.M.; Adelstein, D.J.; Mekhail, T.M.; Rice, TW.; Stevens, GH.; Lee, SY.; Suh, J.H. Validation of the RTOG recursive partitioning analysis (RPA) classification for small-cell lung cancer-only brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 240–243. [Google Scholar] [CrossRef]
- Gülbas, H.; Erkal, S.H.; Serin, M. The use of recursive partitioning analysis grouping in patients with brain metastases from non-small-cell lung cancer. Jpn. J. Clin. Oncol. 2006, 36, 193–196. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Chao, S.T.; Sneed, P.K.; Luo, X.; Suh, J.; Roberge, D.; Bhatt, A.; Jensen, A.W.; Brown, P.D.; Shih, H.; Kirkpatrick, J.; Schwer, A.; Gaspar, L.E.; Fiveash, J.B.; Chiang, V.; Knisely, J.; Sperduto, C.M.; Mehta, M. Diagnosis-specific prognostic factors, indexes, and treatment outcomes for patients with newly diagnosed brain metastases: A multi-institutional analysis of 4,259 patients. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 655–661. [Google Scholar]
- Ruderman, N.B.; Hall, T.C. Use of glucocorticoids in the palliative treatment of metastatic brain tumors. Cancer 1965, 18, 298–306. [Google Scholar] [CrossRef]
- Batchelor, T.; DeAngelis, L.M. Medical management of cerebral metastases. Neurosurg. Clin. North Am. 1996, 7, 435–446. [Google Scholar]
- Vecht, C.J.; Hovestadt, A.; Verbiest, H.B.; van Vliet, J.J.; van Putten, W.L. Dose-effect relationship of dexamethasone on Karnofsky performance in metastatic brain tumors: A randomized study of doses of 4, 8, and 16 mg per day. Neurology 1994, 44, 675–80. [Google Scholar] [CrossRef]
- Hempen, C.; Weiss, E.; Hess, C.F. Dexamethasone treatment in patients with brain metastases and primary brain tumors: Do the benefits outweigh the side-effects? Supp. Care Cancer 2002, 10, 322–328. [Google Scholar] [CrossRef]
- Forsyth, P.A.; Weaver, S.; Fulton, D.; Brasher, P.M.; Sutherland, G.; Stewart, D.; Hagen, N.A.; Barnes, P.; Cairncross, J.G.; DeAngelis, L.M. Prophylactic anticonvulsants in patients with brain tumor. Can. J. Neurol. Sci. 2003, 30, 106–112. [Google Scholar]
- Borgelt, B.; Gelber, R.; Kramer, S.; Brady, L.W.; Chang, C.H.; Davis, L.W.; Perez, C.A.; Hendrickson, F.R. The palliation of brain metastases: Final results of the first two studies by the radiation therapy oncology group. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Borgelt, B.; Gelber, R.; Larson, M.; Hendrickson, F.; Griffin, T.; Roth, R. Ultra-rapid high dose irradiation schedules for the palliation of brain metastases: Final results of the first two studies by the radiation therapy oncology group. Int. J. Radiat. Oncol. Biol. Phys. 1981, 7, 1633–1638. [Google Scholar]
- Murray, K.J.; Scott, C.; Greenberg, H.M.; Emami, B.; Seider, M.; Vora, N.L.; Olson, C.; Whitton, A.; Movsas, B.; Curran, W. A randomized phase III study of accelerated hyperfractionation versus standard in patients with unresected brain metastases: A report of the Radiation Therapy Oncology Group (RTOG) 9104. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 571–574. [Google Scholar] [CrossRef]
- Haie-Meder, C.; Pellae-Cosset, B.; Laplanche, A.; Lagrange, J.L.; Tuchais, C.; Nogues, C.; Arriagada, R. Results of a randomized clinical trial comparing two radiation schedules in the palliative treatment of brain metastases. Radiother. Oncol. 1993, 26, 111–116. [Google Scholar] [CrossRef]
- Priestman, T.J.; Dunn, J.; Brada, M.; Rampling, R.; Baker, P.G. Final results of the Royal College of Radiologists’ Trial comparing two different radiotherapy schedules in the treatment of cerebral metastases. Clin. Oncol. 1996, 8, 308–315. [Google Scholar] [CrossRef]
- DeAngelis, L.M.; Delattre, J.V.; Posner, J.B. Radiation-induced dementia in patients cured of brain metastases. Neurology 1989, 39, 789–796. [Google Scholar] [CrossRef]
- Nieder, C.; Berberich, W.; Schnabel, K. Tumor-related prognostic factors for remission of brain metastases after radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 25. [Google Scholar] [CrossRef]
- Nieder, C.; Nestle, U.; Walter, K.; Niewald, M.; Schnabel, K. Dose/effect relationships for brain metastases. J. Cancer Res. Clin. Oncol. 1998, 124, 346–350. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A randomized trial of surgery in the treatment of single metastases to the brain. New Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Noordijk, E.M.; Vecht, C.J.; Haaxma-Reiche, H.; Padberg, G.W.; Voormolen, J.H.; Hoekstra, F.H.; Tans, J.T.; Lambooij, N.; Metsaars, J.A.; Wattendorff, A.R.; Brand, R.; Hermans, J. The choice of treatment of single brain metastasis should be based on extracranial tumor activity and age. Int. J. Radiat. Oncol. Biol. Phys. 1994, 29, 711–717. [Google Scholar] [CrossRef]
- Mintz, A.H.; Kestle, J.; Rathbone, M.P.; Gaspar, L.; Hugenholtz, H.; Fisher, B.; Duncan, G.; Skingley, P.; Foster, G.; Levine, M. A randomized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer 1996, 78, 1470–1476. [Google Scholar] [CrossRef]
- Paek, S.H.; Audu, P.B.; Sperling, M.R.; Cho, J.; Andrews, D.W. Reevaluation of surgery for the treatment of brain metastases: Review of 208 patients with single or multiple brain metastases treated at one institution with modern neurological techniques. Neurosurgery 2005, 56, 1021–1034. [Google Scholar]
- Stark, A.M.; Tscheslog, H.; Buhl, R; Held-Feindt, J.; Mehdorn, H.M. Surgical treatment for brain metastases: Prognostic factors and survival in 177 patients. Neurosurg. Rev. 2005, 28, 115–119. [Google Scholar] [CrossRef]
- Bindal, R.K.; Sawaya, R.; Leavens, M.E.; Lee, J.J. Surgical treatment of multiple brain metastases. J. Neurosurg. 1993, 79, 748–754. [Google Scholar]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative radiotherapy in the treatment of single metastases to the brain: A randomized trial. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; Hassel, M.B.; Kouri, M.; Valeinis, E.; van den Berge, D.; Collette, S.; Collette, L.; Mueller, R.P. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases – results of the EORTC 22952-26001 study. J. Clin. Oncol. 2011, in press. [Google Scholar]
- Suh, J.H. Stereotactic radiosurgery for the management of brain metastases. N. Engl. J. Med. 2010, 362, 1119–1127. [Google Scholar] [CrossRef]
- Suh, J.H.; Chao, S.T.; Vogelbaum, M.A. Management of brain metastases. Curr. Neurol. Neurosci. Rep. 2009, 9, 223–230. [Google Scholar] [CrossRef]
- Shaw, E.; Scott, C.; Souhami, L.; Dinapoli, R.; Kline, R.; Loeffler, J.; Farnan, N. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastses: Final report of RTOG protocol 90-05. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 291–298. [Google Scholar] [CrossRef]
- Fuks, Z.; Kolesnick, R. Engaging the vascular component of the tumor response. Cancer Cell 2005, 8, 89–91. [Google Scholar] [CrossRef]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Wang, Y.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; Weichselbaum, R.R.; Fu, Y.X. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: Changing strategies for cancer treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef]
- Garcia-Barros, M.; Paris, F.; Cordon-Cardo, C.; Lyden, D.; Rafii, S.; Haimovitz-Friedman, A.; Fuks, Z.; Kolesnick, R. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science 2003, 300, 1155–1159. [Google Scholar] [CrossRef]
- Zabel, A.; Milker-Zabel, S.; Thilmann, C.; Zuna, I.; Rhein, B.; Wannenmacher, M.; Debus, J. Treatment of brain metastases in patients with non-small cell lung cancer (NSCLC) by stereotactic LINAC-based radiosurgery: Prognostic factors. Lung Cancer 2002, 37, 87–94. [Google Scholar]
- Kim, Y.S.; Kondziolka, D.; Flickinger, J.C.; Lunsford, L.D. Stereotactic radiosurgery for patients with nonsmall cell lung carcinoma metastatic to the brain. Cancer 1997, 80, 2075–2083. [Google Scholar] [CrossRef]
- Williams, J.; Enger, C.; Wharam, M.; Tsai, D.; Brem, H. Stereotactic radiosurgery for brain metastases: Comparison of lung carcinoma vs. non-lung tumors. J. Neurooncol. 1998, 37, 79–85. [Google Scholar] [CrossRef]
- Sheehan, J.P.; Sun, M.H.; Kondziolka, D.; Flickinger, J.; Lunsford, L.D. Radiosurgery for non-small cell lung carcinoma metastatic to the brain: Long-term outcomes and prognostic factors influencing patient survival time and local tumor control. J. Neurosurg. 2002, 97, 1276–1281. [Google Scholar] [CrossRef]
- Sheehan, J.; Kondziolka, D.; Flickinger, J.; Lunsford, L.D. Radiosurgery for patients with recurrent small cell lung carcinoma metastatic to the brain: Outcomes and prognostic factors. J. Neurosurg. 2005, 102, S247–254. [Google Scholar] [CrossRef]
- Mariya, Y.; Sekizawa, G.; Matsuoka, Y.; Seki, H.; Sugawara, T. Outcome of stereotactic radiosurgery for patients with non-small cell lung cancer metastatic to the brain. J. Radiat. Res. 2010, 51, 333–342. [Google Scholar] [CrossRef]
- Kondziolka, D.; Patel, A.; Lunsford, L.D.; Kassam, A.; Flickinger, J.C. Stereotactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multiple brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 427–434. [Google Scholar]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.P.; Souhami, L.; Rotman, M.; Mehta, M.P.; Curran, W.J., Jr. Whole brain radiation therapy with and without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomized trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef]
- Elveen, T.; Andrews, D.W. Summary of RTOG 95-08 phase III randomized trial of whole brain radiation with or without stereotactic radiosurgery boost, including presentation of a clinical case study. Am. J. Oncol. Rev. 2004, 3, 592–600. [Google Scholar]
- Chougule, P.B.; Burton-Williams, M.; Saris, S.; Zheng, Z.; Ponte, B.; Noren, G.; Alderson, L.; Friehs, G.; Wazer, D.; Epstein, M. Randomized treatment of brain metastases with gamma knife radiosurgery, whole brain radiotherapy or both. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, S114. [Google Scholar]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; Kunieda, E.; Inomata, T.; Hayakawa, K.; Katoh, N.; Kobashi, G. Stereotactic radiosurgery plus whole-brain radiation therapy vs sterotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef]
- Aoyama, H.; Tago, M.; Kato, N.; Toyoda, T.; Kenjyo, M.; Hirota, S.; Shioura, H.; Inomata, T.; Kunieda, E.; Hayakawa, K.; Nakagawa, K.; Kobashi, G.; Shirato, H. Neurocognitive function of patients with brain metastases who received either whole brain radiotherapy plus stereotactic radiosurgery or radiosurgery alone. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1388–1395. [Google Scholar] [CrossRef]
- Roos, D.E.; Wirth, A.; Burmeister, B.H.; Spry, N.A.; Drummond, K.J.; Beresford, J.A.; McClurem, B.E. Whole brain irradiation following surgery or radiosurgery for solitary brain metastases: Mature results of a prematurely closed randomized Trans-Tasman Radiation Oncology Group trial (TROG 98.05). Radiother. Oncol. 2006, 80, 318–322. [Google Scholar] [CrossRef]
- Muacevic, A.; Wowra, B.; Siefert, A.; Tonn, J.C.; Steiger, H.J.; Kreth, F.W. Microsurgery plus whole brain irradiation versus Gamma Knife surgery alone for treatment of single metastases to the brain: A randomized controlled multicentre phase III trial. J. Neurooncol. 2008, 87, 299–307. [Google Scholar] [CrossRef]
- Schuette, W. Treatment of brain metastases from lung cancer: Chemotherapy. Lung Cancer 2004, 45, S253–S257. [Google Scholar] [CrossRef]
- Komarnicky, L.T.; Phillips, T.L.; Martz, K.; Asbell, S.; Isaacson, S.; Urtasun, R. A randomized phase III protocol for the evaluation of misonidazole combined with radiation in the treatment of patients with brain metastases (RTOG-7916). Int. J. Radiat. Oncol. Biol. Phys. 1991, 20, 53–58. [Google Scholar] [CrossRef]
- Phillips, T.L.; Scott, C.B.; Leibel, S.A.; Rotman, M.; Weigensberg, I.J. Results of a randomized comparison of radiotherapy and bromodeoxyuridine with radiotherapy alone for brain metastases: Report of RTOG trial 89-05. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 339–348. [Google Scholar] [CrossRef]
- Ushio, Y.; Arita, N.; Hayakawa, T.; Mogami, H.; Hasegawa, H.; Bitoh, S.; Oku, Y.; Ikeda, H.; Kanai, N.; Kanoh, M.; et al. Chemotherapy of brain metastases from lung carcinoma: A controlled randomized study. Neurosurgery 1991, 28, 201–205. [Google Scholar] [CrossRef]
- Robinet, G.; Thomas, P.; Breton, J.L.; Léna, H.; Gouva, S.; Dabouis, G.; Bennouna, J.; Souquet, P.J.; Balmes, P.; Thiberville, L.; Fournel, P.; Quoix, E.; Riou, R.; Rebattu, P.; Pérol, M.; Paillotin, D.; Mornex, F. Results of a phase III study of early versus delayed whole brain radiotherapy with concurrent cisplatin and vinorelbine combination in inoperable brain metastasis of non-small-cell lung cancer: Groupe Français de Pneumo-Cancérologie (GFPC) Protocol 95-1. Ann. Oncol. 2001, 12, 59–67. [Google Scholar] [CrossRef]
- Neuhaus, T.; Ko, Y.; Muller, R.P.; Grabenbauer, G.G.; Hedde, J.P.; Schueller, H.; Kocher, M.; Stier, S.; Fietkau, R. A phase III trial of topotecan and whole brain radiation therapy for patients with CNS-metastases due to lung cancer. Br. J. Cancer 2009, 100, 291–297. [Google Scholar] [CrossRef]
- Guerrieri, M.; Wong, K.; Ryan, G.; Millward, M.; Quong, G.; Ball, D.L. A randomised phase III study of palliative radiation with concomitant carboplatin for brain metastases from non-small cell carcinoma of the lung. Lung Cancer 2004, 46, 107–111. [Google Scholar] [CrossRef]
- Knisely, J.P.S.; Berkey, B.; Chakravarti, A.; Yung, A.W.; Curran, W.J., Jr.; Robins, H.I.; Movsas, B.; Brachman, D.G.; Henderson, R.H.; Mehta, M.P. A phase III study of conventional radiation therapy plus thalidomide versus conventional radiation therapy for multiple brain metastases (RTOG 0118). Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 79–86. [Google Scholar] [CrossRef]
- Mehta, M.P.; Shapiro, W.R.; Phan, S.C.; Gervais, R.; Carrie, C.; Chabot, P.; Patchell, R.A.; Glantz, M.J.; Recht, L.; Langer, C.; Sur, R.K.; Roa, W.H.; Mahe, M.A.; Fortin, A.; Nieder, C.; Meyers, C.A.; Smith, J.A.; Miller, R.A.; Renschler, M.F. Motexafin gadolinium combined with prompt whole brain radiotherapy prolongs time to neurologic progression in non-small-cell lung cancer patients with brain metastases: Results of a phase III trial. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1069–1076. [Google Scholar] [CrossRef]
- Suh, J.H.; Stea, B.; Nabid, A.; Kresl, J.J.; Fortin, A.; Mercier, J.P.; Senzer, N.; Chang, E.L.; Boyd, A.P.; Cagnoni, P.J.; Shaw, E. Phase III study of efaproxiral as an adjunct to whole-brain radiation therapy for brain metastases. J. Clin. Oncol. 2006, 24, 106–114. [Google Scholar] [CrossRef]
- Verger, E.; Gil, M.; Yaya, R.; Viñolas, N.; Villà, S.; Pujol, T.; Quintó, L.; Graus, F. Temozolomide and concomitant whole brain radiotherapy in patients with brain metastases: A phase II randomized trial. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 185–191. [Google Scholar] [CrossRef]
- Antonadou, D.; Paraskevaidis, M.; Sarris, G.; Coliarakis, N.; Economou, I.; Karageorgis, P.; Throuvalas, N. Phase II randomized trial of temozolomide and concurrent radiotherapy in patients with brain metastases. J. Clin. Oncol. 2002, 20, 3644–3650. [Google Scholar] [CrossRef]
- Johnson, B.E.; Patronas, N.; Hayes, W.; Grayson, J.; Becker, B.; Gnepp, D.; Rowland, J.; Anderson, A.; Glatstein, E.; Ihde, D.C.; Frank, J.A. Neurologic, computed cranial tomographic, and magnetic resonance imaging abnormalities in patients with small-cell lung cancer: Further follow up of 6- to 13-year survivors. J. Clin. Oncol. 1990, 8, 48–56. [Google Scholar]
- Cull, A.; Gregor, A.; Hopwood, P.; Macbeth, F.; Karnicka-Mlodkowska, H.; Thatcher, N.; Burt, P.; Stout, R.; Stepniewska, K.; Stewart, M. Neurological and cognitive impairment in long-term survivors of small cell lung cancer. Eur. J. Cancer 1994, 30, 1067–1074. [Google Scholar] [CrossRef]
- DeAngelis, L.M.; Mandell, L.R.; Thaler, H.T.; Kimmel, D.W.; Galicich, J.H.; Fuks, Z.; Posner, J.B. The role of postoperative radiotherapy after resection of single brain metastases. Neurosurgery 1989, 24, 798–805. [Google Scholar] [CrossRef]
- Welzel, G.; Fleckenstein, K.; Schaefer, J.; Hermann, B.; Kraus-Tiefenbacher, U.; Mai, S.K.; Wenz, F. Memory function before and after whole brain radiotherapy in patients with and without brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 1311–1318. [Google Scholar] [CrossRef]
- Regine, W.F.; Huhn, J.L.; Patchell, R.A.; St Clair, W.H.; Strottmann, J.; Meigooni, A.; Sanders, M.; Young, A.B. Risk of symptomatic brain tumor recurrence and neurologic deficit after radiosurgery alone in patients with newly diagnosed brain metastases: Results and implications. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 333–338. [Google Scholar] [CrossRef]
- Regine, W.F.; Scott, C.; Murray, K.; Curran, W. Neurocognitive outcome in brain metastases patients treated with accelerated-fractionation vs. accelerated-hyperfractionated radiotherapy: An analysis from radiation therapy oncology group study 91-04. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 711–717. [Google Scholar] [CrossRef]
- Meyers, C.A.; Smith, J.A.; Bezjak, A.; Mehta, M.P.; Liebmann, J.; Illidge, T.; Kunkler, I.; Caudrelier, J.M.; Eisenberg, P.D.; Meerwaldt, J.; Siemers, R.; Carrie, C.; Gaspar, L.E.; Curran, W.; Phan, S.C.; Miller, R.A.; Renschler, M.F. Neurocognitive function and progression in patients with brain metastases treated with whole-brain radiation and motexafin gadolinium: Results of a randomized phase III trial. J. Clin. Oncol. 2004, 22, 157–165. [Google Scholar]
- Li, J.; Bentzen, S.M.; Renschler, M.; Mehta, M.P. Regression after whole-brain radiation therapy for brain metastases correlates with survival and improved neurocognitive function. J. Clin. Oncol. 2007, 25, 1260–1266. [Google Scholar] [CrossRef]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; Meyers, C.A. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomized controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Shaw, E.G.; Rosdhal, R.; D’Agostino, R.B., Jr.; Lovato, J.; Naughton, M.J.; Robbins, M.E.; Rapp, S.R. Phase II study of donepezil in irradiated brain tumor patients: Effect on cognitive function, mood, and quality of life. J. Clin. Oncol. 2006, 24, 1415–1420. [Google Scholar] [CrossRef]
- RTOG 0614, a randomized, phase III, double-blind, placebo-controlled trial of memantine for prevention of cognitive dysfunction in patients receiving whole-brain radiotherapy. Available online: http://www.rtog.org (Accessed 7 November 2010).
- Nieder, C.; Leicht, A.; Motaref, B.; Nestle, U.; Niewald, M.; Schnabel, K. Late radiation toxicity after whole-brain radiotherapy: The influence of antiepileptic drugs. Am. J. Clin. Oncol. 1999, 22, 573–579. [Google Scholar]
- Hochstenbag, M.M.H.; Twijnstra, A.; Wilmink, J.T.; Wouters, E.F.; ten Velde, G.P. Asymptomatic brain metastases (BM) in small cell lung cancer (SCLC): MR-imaging is useful at initial diagnosis. J. Neurooncol. 2000, 48, 243–248. [Google Scholar] [CrossRef]
- Nugent, J.L.; Bunn, P.A., Jr.; Matthews, M.J.; Ihde, D.C.; Cohen, M.H.; Gazdar, A.; Minna, J.D. CNS metastases in small bronchogenic carcinoma: Increasing frequency and changing pattern with lengthening of survival. Cancer 1979, 44, 1885–1893. [Google Scholar] [CrossRef]
- Komaki, R.; Cox, J.D.; Whitson, W. Risk of brain metastasis from small cell carcinoma of the lung related to length of survival and prophylactic irradiation. Cancer Treat. Rep. 1981, 65, 811–814. [Google Scholar]
- Beiler, D.D.; Kane, R.C.; Bernath, A.M.; Cashdollar, M.R. Low dose elective brain irradiation in small cell carcinoma of the lung. Int. J. Radiat. Oncol. Biol. Phys. 1979, 5, 941–945. [Google Scholar] [CrossRef]
- Maurer, L.H.; Tulloh, M.; Weiss, R.B.; Blom, J.; Leone, L.; Glidewell, O.; Pajak, T.F. A randomized combined modality trial in small cell carcinoma of the lung: Comparison of combination chemotherapy-radiation therapy versus cyclophosphamide-radiation therapy effects of maintenance chemotherapy and prophylactic whole brain irradiation. Cancer 1980, 45, 30–39. [Google Scholar] [CrossRef]
- Eagan, R.T.; Frytak, S.; Lee, R.E.; Creagan, E.T.; Ingle, J.N.; Nichols, W.C. A case for preplanned thoracic and prophylactic whole brain radiation therapy in limited small-cell lung cancer. Cancer Clin. Trials 1981, 4, 261–266. [Google Scholar]
- Jackson, D.V., Jr.; Richards, F., 2nd.; Cooper, M.R.; Ferree, C.; Muss, H.B.; White, D.R.; Spurr, C.L. Prophylactic cranial irradiation in small cell carcinoma of the lung. A randomized study. JAMA 1977, 237, 2730–2733. [Google Scholar] [CrossRef]
- Seydel, H.G.; Creech, R.; Pagano, M.; Salazar, O.; Rubin, P.; Concannon, J.; Carbone, P.; Mohuiddin, M.; Perez, C.; Matthews, M. Prophylactic versus no brain irradiation in regional small cell lung carcinoma. Am. J. Clin. Oncol. 1985, 218–223. [Google Scholar]
- Niiranen, A.; Holsti, P.; Salmo, M. Treatment of small cell lung cancer. Two-drug versus four-drug chemotherapy and loco-regional irradiation with or without prophylactic cranial irradiation. Acta Oncol. 1989, 28, 501–505. [Google Scholar] [CrossRef]
- Rosen, S.T.; Makuch, R.W.; Lichter, A.S.; Ihde, D.C.; Matthews, M.J.; Minna, J.D.; Glatstein, E.; Bunn, P.A., Jr. Role of prophylactic cranial irradiation in prevention of central nervous system metastases in small cell lung cancer. Potential benefit restricted to patients with complete response. Am. J. Med. 1983, 74, 615–624. [Google Scholar] [CrossRef]
- Rosenstein, M.; Armstrong, J.; Kris, M.; Shank, B.; Scher, H.; Fass, D.; Harrison, L.; Fuks, Z.; Leibel, S. A reappraisal of the role of prophylactic cranial irradiation in limited small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 1992, 24, 43–48. [Google Scholar] [CrossRef]
- Rubenstein, J.H.; Dosoretz, D.E.; Katin, M.J.; Blitzer, P.H.; Salenius, S.A.; Floody, P.A.; Harwin, W.N.; Teufel, T.E.; Raymond, M.G.; Reeves, J.A.; Hart, L.L.; McCleod, M.J.; Pizarro, A.; Gabarda, A.L.; Rana, V.G. Low doses of prophylactic cranial irradiation effective in limited stage small cell carcinoma of the lung. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 329–337. [Google Scholar] [CrossRef]
- Aupérin, A.; Arriagada, R.; Pignon, J.P.; Le Péchoux, C.; Gregor, A.; Stephens, R.J.; Kristjansen, P.E.; Johnson, B.E.; Ueoka, H.; Wagner, H.; Aisner, J. Prophylactic cranial irradiation for patients with small cell lung cancer in complete remission. Prophylactic cranial irradiation overview collaborative group. N. Engl. J. Med. 1999, 341, 476–484. [Google Scholar] [CrossRef]
- Meert, A.P.; Paesmans, M.; Berghmans, T.; Martin, B.; Mascaux, C.; Vallot, F.; Verdebout, J.M.; Lafitte, J.J.; Sculier, J.P. Prophylactic cranial irradiation in small cell lung cancer: A systematic review of the literature with meta-analysis. BMC Cancer 2001, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Slotman, B.; Faivre-Finn, C.; Kramer, G.; Rankin, E.; Snee, M.; Hatton, M.; Postmus, P.; Collette, L.; Musat, E.; Senan, S.; EORTC Radiation Oncology Group and Lung Cancer Group. Prophylactic cranial irradiation in extensive small-cell lung cancer. N. Engl. J. Med. 2007, 357, 664–672. [Google Scholar] [CrossRef]
- le Péchoux, C.; Dunant, A.; Senan, S.; Wolfson, A.; Quoix, E.; Faivre-Finn, C.; Ciuleanu, T.; Arriagada, R.; Jones, R.; Wanders, R.; Lerouge, D.; Laplanche, A.; Prophylactic Cranial Irradiation (PCI) Collaborative Group. Standard-dose versus higher-dose prophylactic cranial irradiation (PCI) in patients with limited-stage small-cell lung cancer in complete remission after chemotherapy and thoracic radiotherapy (PCI 99-01, EORTC 22003-08004, RTOG 0212, and IFCT 99-01): A randomized clinical trial. Lancet Oncol. 2009, 10, 467–474. [Google Scholar] [CrossRef]
- Gore, E. Prophylactic cranial irradiation in non-small cell lung cancer. In Principles and Practice of Lung Cancer, 4th Edition; Pass, H.I., Carbone, D.P., Minna, J.D., Johnson, D.H., Scagliotti, G.V., Turrisi, A.T., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 837–844. [Google Scholar]
- Wang, S.Y.; Ye, X.; Ou, W.; Lin, Y.B.; Zhang, B.B.; Yang, H. Risk of cerebral metastases for postoperative locally advanced non-small-cell lung cancer. Lung Cancer 2009, 64, 238–243. [Google Scholar] [CrossRef]
- Perez, C.A.; Pajak, T.F.; Simpson, J.R.; Mohiuddin, M.; Brady, L.W.; Perez-Tamayo, R.; Rotman, M. Long-term observations of patterns of failure in patients with unresectable non-oat cell carcinoma of the lung treated with definitive radiotherapy. Cancer 1987, 59, 1874–1881. [Google Scholar] [CrossRef]
- Komaki, R.; Cox, J.D.; Stark, R. Frequency of brain metastasis in adenocarcinoma and large cell carcinoma of the lung: Correlation with survival. Int. J. Radiat. Oncol. Biol. Phys. 1983, 9, 1467–1470. [Google Scholar] [CrossRef]
- Cox, J.D.; Scott, C.B.; Byhardt, R.W.; Emami, B.; Russell, A.H.; Fu, K.K.; Parliament, M.B.; Komaki, R.; Gaspar, L.E. Addition of chemotherapy to radiation therapy alters failure patterns by cell type within non-small cell carcinoma of lung (NSCLC): Analysis of Radiation Therapy Oncology Group (RTOG) trials. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 505–509. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Reni, M.; Chiesa, G.; Carretta, A.; Schipani, S.; Passoni, P.; Bolognesi, A.; Zannini, P.; Villa, E. Brain metastases in locally advanced nonsmall cell lung carcinoma after multimodality treatment: Risk factors analysis. Cancer 2002, 95, 605–612. [Google Scholar] [CrossRef]
- Robnett, T.J.; Machtay, M.; Stevenson, J.P.; Algazy, K.M.; Hahn, S.M. Factors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinoma. J. Clin. Oncol. 2001, 19, 1344–1349. [Google Scholar]
- Andre, F.; Grunenwald, D.; Pujol, J.L.; Girard, P.; Dujon, A.; Brouchet, L.; Brichon, P.Y.; Westeel, V.; Le Chevalier, T. Patterns of relapse of N2 nonsmall-cell lung carcinoma patients treated with preoperative chemotherapy: Should prophylactic cranial irradiation be reconsidered? Cancer 2001, 91, 2394–2400. [Google Scholar] [CrossRef]
- Komaki, R.; Scott, C.B.; Byhardt, R.; Emami, B.; Asbell, S.O.; Russell, A.H.; Roach, M.; Parliament, M.B.; Gaspar, L.E. Failure patterns by prognostic group determined by recursive partitioning analysis (RPA) of 1547 patients on four Radiation Therapy Oncology Group (RTOG) studies in inoperable nonsmall-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 263–267. [Google Scholar]
- Mamon, H.J.; Yeap, B.Y.; Jänne, P.A.; Reblando, J.; Shrager, S.; Jaklitsch, M.T.; Mentzer, S.; Lukanich, J.M.; Sugarbaker, D.J.; Baldini, E.H.; Berman, S.; Skarin, A.; Bueno, R. High risk of brain metastases in surgically staged IIIA non-small-cell lung cancer patients treated with surgery, chemotherapy, and radiation. J. Clin. Oncol. 2005, 23, 1530–1537. [Google Scholar] [CrossRef]
- Germain, F.; Wai, E.S.; Berthelet, E.; Truong, P.T.; Lesperance, M. Brain metastasis is an early manifestation of distant failure in stage III nonsmall cell lung cancer patients treated with radical chemoradiation therapy. Am. J. Clin. Oncol. 2008, 31, 561–566. [Google Scholar] [CrossRef]
- Carolan, H.; Sun, A.Y.; Bezjak, A.; Yi, Q.L.; Payne, D.; Kane, G.; Waldron, J.; Leighl, N.; Feld, R.; Burkes, R.; Keshavjee, S.; Shepherd, F. Does the incidence and outcome of brain metastases in locally advanced non-small cell lung cancer justify prophylactic cranial irradiation or early detection? Lung Cancer 2005, 49, 109–115. [Google Scholar] [CrossRef]
- Cox, J.D.; Stanley, K.; Petrovich, Z.; Paig, C.; Yesner, R. Cranial irradiation in cancer of the lung of all cell types. JAMA 1981, 245, 469–472. [Google Scholar] [CrossRef]
- Russell, A.H.; Pajak, T.E.; Selim, H.M.; Paradelo, J.C.; Murray, K.; Bansal, P.; Cooper, J.D.; Silverman, S.; Clement, J.A. Prophylactic cranial irradiation for lung cancer patients at high risk for development of cerebral metastasis: Results of a prospective randomized trial conducted by the Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 637–643. [Google Scholar] [CrossRef]
- Umsawasdi, T.; Valdivieso, M.; Chen, T.T.; Barkley, H.T., Jr.; Booser, D.J.; Chiuten, D.F.; Dhingra, H.M.; Murphy, W.K.; Dixon, C.L.; Farha, P.; et al. Role of elective brain irradiation during combined chemoradiotherapy for limited disease non-small cell lung cancer. J. Neurooncol. 1984, 2, 253–259. [Google Scholar]
- Pöttgen, C.; Eberhardt, W.; Grannass, A.; Korfee, S.; Stüben, G.; Teschler, H.; Stamatis, G.; Wagner, H.; Passlick, B.; Petersen, V.; Budach, V.; Wilhelm, H.; Wanke, I.; Hirche, H.; Wilke, H.J.; Stuschke, M. Prophylactic cranial irradiation in operable stage IIIA non-small-cell lung cancer treated with neoadjuvant chemoradiotherapy: Results from a German multicenter randomized trial. J. Clin. Oncol. 2007, 25, 4987–4992. [Google Scholar] [CrossRef]
- Movsas, B.; Bae, K.; Meyers, C.; Gore, E.; Bonner, J.; Sun, A.; Schild, S.; Gaspar, L.E.; Bogart, J.; Choy, H. Phase III study of prophylactic cranial irradiation vs. observation in patients with stage III non-small-cell lung cancer: Neurocognitive and quality of life analysis of RTOG 0214 (abstract). Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, S1. [Google Scholar]
- ohnson, B.E.; Becker, B.; Goff, W.B., 2nd.; Petronas, N.; Krehbiel, M.A.; Makuch, R.W.; McKenna, G.; Glatstein, E.; Ihde, D.C. Neurologic, neuropsychologic, and computed cranial tomography scan abnormalities in 2- to 10-year survivors of small-cell lung cancer. J. Clin. Oncol. 1985, 3, 1659–1667. [Google Scholar]
- Arriagada, R.; le Chevalier, T.; Borie, F.; Rivière, A.; Chomy, P.; Monnet, I.; Tardivon, A.; Viader, F.; Tarayre, M.; Benhamou, S. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. J. Natl. Cancer Inst. 1995, 87, 183–190. [Google Scholar] [CrossRef]
- Gregor, A.; Cull, A.; Stephens, R.J.; Kirkpatrick, J.A.; Yarnold, J.R.; Girling, D.J.; Macbeth, F.R.; Stout, R.; Machin, D. Prophylactic cranial irradiation is indicated following complete response to induction therapy in small cell lung cancer: Results of a multicentre randomized trial. Eur. J. Cancer 1997, 33, 1752–1758. [Google Scholar] [CrossRef]
- Hu, C.; Chang, E.L.; Hassenbusch, S.J., 3rd.; Allen, P.K.; Woo, S.Y.; Mahajan, A.; Komaki, R.; Liao, Z. Nonsmall cell lung cancer presenting with synchronous solitary brain metastasis. Cancer 2006, 106, 1998–2004. [Google Scholar] [CrossRef]
- Flannery, T.W.; Suntharalingam, M.; Regine, W.F.; Chin, L.S.; Krasna, M.J.; Shehata, M.K.; Edelman, M.J.; Kremer, M.; Patchell, R.A.; Kwok, Y. Long-term survival in patients with synchronous, solitary brain metastasis from non-small-cell lung cancer treated with radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 19–23. [Google Scholar] [CrossRef]
- Bonnette, P.; Puyo, P.; Gabriel, C.; Giudicelli, R.; Regnard, J.F.; Riquet, M.; Brichon, P.Y.; Groupe Thorax. Surgical management of non-small cell lung cancer with synchronous brain metastases. Chest 2001, 119, 1469–1475. [Google Scholar] [CrossRef]
- Billing, P.S.; Miller, D.L.; Allen, M.S.; Deschamps, C.; Trastek, V.F.; Pairolero, P.C. Surgical treatment of primary lung cancer with synchronous brain metastases. J. Thorac. Cardiovasc. Surg. 2001, 122, 548–553. [Google Scholar] [CrossRef]
- Ampil, F.; Caldito, G.; Milligan, S.; Mills, G.; Nanda, A. The elderly with synchronous non-small cell lung cancer and solitary brain metastasis: Does palliative thoracic radiotherapy have a useful role? Lung Cancer 2007, 57, 60–65. [Google Scholar] [CrossRef]
- Lo, C.K.; Yu, C.H.; Ma, C.C.; Ko, K.M.; Leung, S.C. Surgical management of primary non-small-cell carcinoma of lung with synchronous solitary brain metastasis: Local experience. Hong Kong Med. J. 2010, 16, 186–191. [Google Scholar]
- Sánchez de Cos, J.; Sojo González, M.A.; Montero, M.V.; Pérez Calvo, M.C.; Vicente, M.J.; Valle, M.H. Non-small cell lung cancer and silent brain metastasis survival and prognostic factors. Lung Cancer 2009, 63, 140–145. [Google Scholar] [CrossRef]
- Yang, S.; Kim, D.G.; Chung, H.; Chung, H.T.; Paek, S.H.; Hyun Kim, J.; Jung, H.W.; Han, D.H. Pulmonary resection in patients with nonsmall-cell lung cancer treated with gamma-knife radiosurgery for synchronous brain metastases. Cancer 2008, 112, 1780–1786. [Google Scholar] [CrossRef]
- Nakayama, H.; Tokuuye, K.; Komatsu, Y.; Ishikawa, H.; Shiotani, S.; Nakada, Y.; Akine, Y. Stereotactic radiotherapy for patients who initially presented with brain metastases from non-small cell carcinoma. Acta Oncol. 2004, 43, 736–739. [Google Scholar] [CrossRef]
- Soltys, S.G.; Adler, J.R.; Lipani, J.D.; Jackson, P.S.; Choi, C.Y.; Puataweepong, P.; White, S.; Gibbs, I.C.; Chang, S.D. Stereotactic radiosurgery of the postoperative resection cavity for brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 187–193. [Google Scholar] [CrossRef]
- Karlovits, B.J.; Quigley, M.R.; Karlovits, S.M.; Miller, L.; Johnson, M.; Gayou, O.; Fuhrer, R. Stereotactic radiosurgery boost to the resection bed for oligometastatic brain disease: Challenging the tradition of adjuvant whole-brain radiotherapy. Neurosurg. Focus 2009, 27, 1–6. [Google Scholar]
- Do, L.; Pezner, R.; Radany, E.; Liu, A.; Staud, C.; Badie, B. Resection followed by stereotactic radiosurgery to resection cavity for intracranial metastases. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 486–491. [Google Scholar] [CrossRef]
- Jagannathan, J.; Yen, C.P.; Ray, D.K.; Schlesinger, D.; Oskouian, R.J.; Pouratian, N.; Shaffrey, M.E.; Larner, J.; Sheehan, J.P. Gamma knife radiosurgery to the surgical cavity following resection of brain metastases. J. Neurosurg. 2009, 111, 431–438. [Google Scholar] [CrossRef]
- Chao, S.T.; Barnett, G.H.; Liu, S.W.; Reuther, A.M.; Toms, S.A.; Vogelbaum, M.A.; Videtic, G.M.; Suh, J.H. Five-year survivors of brain metastases: A single-institution report of 32 patients. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 801–809. [Google Scholar] [CrossRef]
- Kondziolka, D.; Martin, J.J.; Flickinger, J.C.; Friedland, D.M.; Brufsky, A.M.; Baar, J.; Agarwala, S.; Kirkwood, J.M.; Lunsford, L.D. Long-term survivors after gamma knife radiosurgery for brain metastases. Cancer 2005, 104, 2784–2791. [Google Scholar] [CrossRef]
- Roberge, D.; Petrecca, K.; el Refae, M.; Souhami, L. Whole-brain radiotherapy and tumor bed radiosurgery following resection of solitary brain metastases. J. Neurooncol. 2009, 95, 95–99. [Google Scholar] [CrossRef]
- Flickinger, J.C.; Kondziolka, D.; Pollock, B.E.; Maitz, A.H.; Lunsford, L.D. Complications from arteriovenous malformation radiosurgery: Multivariate analysis and risk modeling. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 485–490. [Google Scholar] [CrossRef]
- Shiau, C.Y.; Sneed, P.K.; Shu, H.K.; Lamborn, K.R.; McDermott, M.W.; Chang, S.; Nowak, P.; Petti, P.L.; Smith, V.; Verhey, L.J.; Ho, M.; Park, E.; Wara, W.M.; Gutin, P.H.; Larson, D.A. Radiosurgery for brain metastases: Relationship of dose and pattern of enhancement to local control. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 375–383. [Google Scholar] [CrossRef]
- Hall, E.J.; Brenner, D.J. The radiobiology of radiosurgery: Rationale for different treatment regimes for AVMs and malignancies. Int. J. Radiat. Oncol. Biol. Phys. 1993, 25, 381–385. [Google Scholar] [CrossRef]
- De Salles, A.; Hariz, M.; Bajada, C.; Goetsch, S.; Bergenheim, T.; Selch, M.; Holly, F.E.; Solberg, T.; Becker, D.P. Comparison between radiosurgery and stereotactic fractionated radiation for the treatment of brain metastases. Acta Neurochir. (Wien) 1993, 58, S115–118. [Google Scholar]
- Nishizaki, T.; Saito, K.; Jimi, Y.; Harada, N.; Kajiwara, K.; Nomura, S.; Ishihara, H.; Yoshikawa, K.; Yoneda, H.; Suzuki, M.; Gibbs, I.C. The role of cyberknife radiosurgery/radiotherapy for brain metastases of multiple or large-size tumors. Minim. Invasive Neurosurg. 2006, 49, 203–209. [Google Scholar] [CrossRef]
- Manning, M.A.; Cardinale, R.M.; Benedict, S.H.; Kavanagh, B.D.; Zwicker, R.D.; Amir, C.; Broaddus, W.C. Hypofractionated stereotactic radiotherapy as an alternative to radiosurgery for the treatment of patients with brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 603–608. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Onimaru, R.; Kagei, K.; Ikeda, J.; Ishii, N.; Sawamura, Y.; Miyasaka, K. Hypofractionated stereotactic radiotherapy alone without whole-brain irradiation for patients with solitary and oligo brain metastasis using noninvasive fixation of the skull. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 793–800. [Google Scholar] [CrossRef]
- Aoki, M.; Abe, Y.; Hatayama, Y.; Kondo, H.; Basaki, K. Clinical outcome of hypofractionated conventional conformation radiotherapy for patients with single and no more than three metastatic brain tumors, with noninvasive fixation of the skull without brain irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 414–418. [Google Scholar] [CrossRef]
- Ernst-Stecken, A.; Ganslandt, O.; Lambrecht, U.; Sauer, R.; Grabenbauer, G. Phase II trial of hypofractionated stereotactic radiotherapy for brain metastases: Results and toxicity. Radiother. Oncol. 2006, 81, 18–24. [Google Scholar] [CrossRef]
- Fahrig, A.; Ganslandt, O.; Lambrecht, U.; Grabenbauer, G.; Kleinert, G.; Sauer, R.; Hamm, K. Hypofractionated stereotactic radiotherapy for brain metastases. Strahlenther. Onkol. 2007, 183, 625–630. [Google Scholar] [CrossRef]
- Kwon, A.K.; DiBiase, S.J.; Wang, B.; Hughes, S.L.; Milcarek, B.; Zhu, Y. Hypofractionated stereotactic radiotherapy for the treatment of brain metastases. Cancer 2009, 115, 890–898. [Google Scholar] [CrossRef]
- Lindvall, P.; Bergström, P.; Löfroth, P.O.; Henriksson, R.; Bergenheim, A.T. Hypo-fractionated conformal stereotactic radiotherapy alone or in combination with whole-brain radiotherapy in patients with cerebral metastasis. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1460–1466. [Google Scholar] [CrossRef]
- Giubilei, C.; Ingrosso, G.; d’Andrea, M.; Benassi, M.; Santoni, R. Hypofractionated stereotactic radiotherapy in combination with whole brain radiotherapy for brain metastases. J. Neurooncol. 2009, 91, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Casanova, N.; Mazouni, Z.; Bieri, S.; Combescure, C.; Pica, A.; Weber, D.C. Whole brain radiotherapy with a conformational external beam radiation boost for lung cancer patients with 1-3 brain metastases: A multiinstitutional study. Radiat. Oncol. 2010, 5, 13. [Google Scholar] [CrossRef]
- Rades, D.; Pluemer, A.; Veninga, T.; Dunst, J.; Schild, S.E. A boost in addition to whole-brain radiotherapy improves patient outcome after resection of 1 or 2 brain metastases in recursive partitioning analysis class 1 and 2 patients. Cancer 2007, 110, 1551–1559. [Google Scholar] [CrossRef]
- Bauman, G.; Yartsev, S.; Fisher, B.; Kron, T.; Laperriere, N.; Heydarian, M.; VanDyk, J. Simultaneous infield boost with helical tomotherapy for patients with 1 to 3 brain metastases. Am. J. Clin. Oncol. 2007, 30, 38–44. [Google Scholar] [CrossRef]
- Lagerwaard, F.J.; van der Hoorn, E.A.P.; Verbakel, W.F.; Haasbeek, C.J.; Slotman, B.J.; Senan, S. Whole-brain radiotherapy with simultaneous integrated boost to multiple brain metastases using volumetric modulated arc therapy. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 253–259. [Google Scholar] [CrossRef]
- Rodrigues, G.; Yartsev, S.; Yaremko, B.; Perera, F.; Dar, A.R.; Hammond, A.; Lock, M.; Yu, E.; Ash, R.; Caudrelier, J.M.; Khuntia, D.; Bailey, L.; Bauman, G. Phase I trial of simultaneous in-field boost with helical tomotherapy for patients with one to three brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2011, in press. [Google Scholar]
- Sterzing, F.; Welzel, T.; Sroka-Perez, G.; Schubert, K.; Debus, J.; Herfarth, K.K. Reirradiation of multiple brain metastases with helical tomotherapy. A multifocal simultaneous integrated boost for eight or more lesions. Strahlenther. Onkol. 2009, 185, 89–93. [Google Scholar] [CrossRef]
- Gutiérrez, A.N.; Westerly, D.C.; Tomé, W.A.; Jaradat, H.A.; Mackie, T.R.; Bentzen, S.M.; Khuntia, D.; Mehta, M.P. Whole brain radiotherapy with hippocampal avoidance and simultaneously integrated brain metastases boost: A planning study. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 589–597. [Google Scholar] [CrossRef]
- Hsu, F.; Carolan, H.; Nichol, A.; Cao, F.; Nuraney, N.; Lee, R.; Gete, E.; Wong, F.; Schmuland, M.; Heran, M.; Otto, K. Whole brain radiotherapy with hippocampal avoidance and simultaneous integrated boost for 1-3 brain metastases: A feasibility study using volumetric modulated arc therapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1480–1485. [Google Scholar] [CrossRef]
- Jorissen, R.N.; Walker, F.; Pouliot, N.; Garrett, T.P.; Ward, C.W.; Burgess, A.W. Epidermal growth factor receptor: Mechanisms of activation and signaling. Exp. Cell Res. 2003, 284, 31–53. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Rivera, M.P. Targeted therapy for the treatment of advanced non-small cell lung cancer: A review of the epidermal growth factor receptor antagonists. Chest 2005, 128, 3975–3984. [Google Scholar] [CrossRef]
- Gazdar, A.F. Epidermal growth factor receptor inhibition in lung cancer: The evolving role of individualized therapy. Cancer Metastasis Rev. 2010, 29, 37–48. [Google Scholar] [CrossRef]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G.; Louis, D.N.; Christiani, D.C.; Settleman, J.; Haber, D.A. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.M.; Lee, H.; Toyooka, S.; Shimizu, N.; Fujisawa, T.; Feng, Z.; Roth, J.A.; Herz, J.; Minna, J.D.; Gazdar, A.F. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Cappuzzo, F.; Gregorc, V.; Bartolini, S.; Crinò, L.; Villa, E. Gefitinib in patients with brain metastases from non-small-cell lung cancer: A prospective trial. Ann. Oncol. 2004, 15, 1042–1047. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, D.H.; Choi, Y.; Yoon, D.H.; Kim, S.W.; Suh, C.; Lee, J.S. Epidermal growth factor receptor tyrosine kinase inhibitors as a first-line therapy for never-smokers with adenocarcinoma of the lung having asymptomatic synchronous brain metastasis. Lung Cancer 2009, 65, 351–354. [Google Scholar] [CrossRef]
- Eichler, A.F.; Kahle, K.T.; Wang, D.L.; Joshi, V.A.; Willers, H.; Engelman, J.A.; Lynch, T.J.; Sequist, L.V. EGFR mutation status and survival after diagnosis of brain metastasis in nonsmall cell lung cancer. NeuroOncology 2010, 2, 1193–1199. [Google Scholar]
- Porta, R.; Massutí, B.; Paz-Ares, L.; Reguart, N.; Sánchez, J.M.; Mayo, C.; Lianes, P.; Queralt, C.; Guillem, V.; Salinas, P.; Catot, S.; Isla, D.; Pradas, A.; Gúrpide, A.; de Castro, J.; Polo, E.; Puig, T.; Tarón, M.; Colomer, R.; Rosell, R. Brain metastases from lung cancer responding to erlotinib: The importance of EGFR mutation. Eur. Respir. J 2011, in press. [Google Scholar]
- Gow, C.H.; Chien, C.R.; Chang, Y.L.; Chiu, Y.H.; Kuo, S.H.; Shih, J.Y.; Chang, Y.C.; Yu, C.J.; Yang, C.H.; Yang, P.C. Radiotherapy in lung adenocarcinoma with brain metastases: Effects of activating epidermal growth factor receptor mutations on clinical response. Clin. Cancer Res. 2008, 14, 162–168. [Google Scholar] [CrossRef]
- Lind, J.S.W.; Lagerwaard, F.J.; Smit, E.F.; Senan, S. Phase I study of concurrent whole brain radiotherapy and erlotinib for multiple brain metastases from non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1391–1396. [Google Scholar] [CrossRef]
- Olmez, I.; Donahue, B.R.; Butler, J.S.; Huang, Y.; Rubin, P.; Xu, Y. Clinical outcomes in extracranial tumor sites and unusual toxicities with concurrent whole brain radiation (WBRT) and erlotinib treatment in patients with non-small cell lung cancer (NSCLC) with brain metastasis. Lung Cancer 2010, in press. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Chi, A.; Komaki, R. Treatment of Brain Metastasis from Lung Cancer. Cancers 2010, 2, 2100-2137. https://doi.org/10.3390/cancers2042100
AMA Style
Chi A, Komaki R. Treatment of Brain Metastasis from Lung Cancer. Cancers. 2010; 2(4):2100-2137. https://doi.org/10.3390/cancers2042100
Chicago/Turabian StyleChi, Alexander, and Ritsuko Komaki. 2010. "Treatment of Brain Metastasis from Lung Cancer" Cancers 2, no. 4: 2100-2137. https://doi.org/10.3390/cancers2042100