
Clinical and Analytical Performance of ELISA Salivary Serologic Assay to Detect SARS-CoV-2 IgG in Children and Adults



 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. Samples Analysis
2.3. Precision Assessment
2.4. Linearity Assessment
2.5. Impact of Sample Collection Time on Salivary Ab Levels
2.6. Statistical Analyses
2.7. Ethical Statement
3. Results
3.1. Performance Verification and Precision Analysis
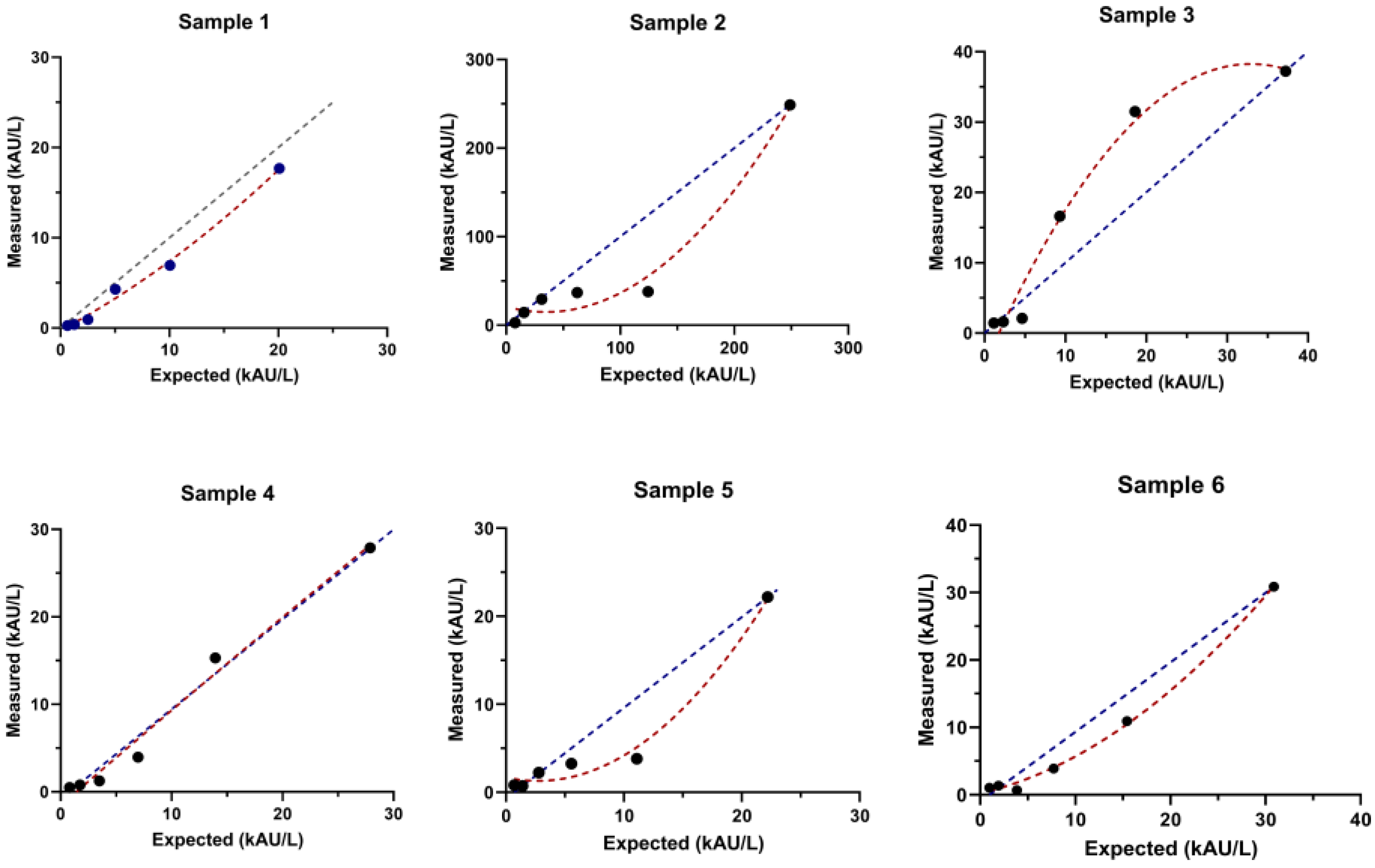
3.2. Linearity Assessment
3.3. Clinical Study
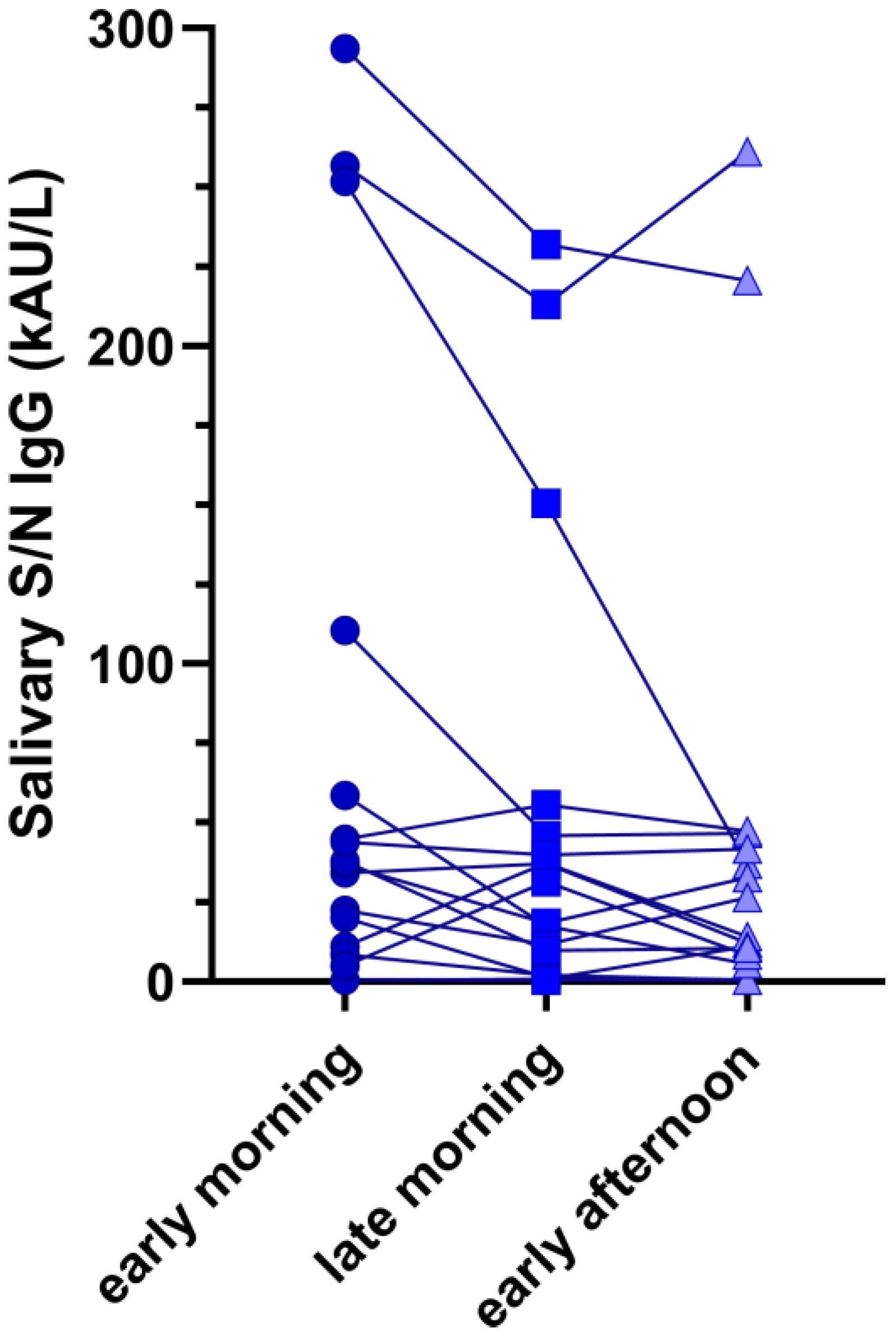
3.4. Impact of Sample Collection Time on Salivary Ab
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statement on the Fourteenth Meeting of the International Health Regulations (2005) Emergency Committee regarding the Coronavirus Disease (COVID-19) Pandemic; World Health Organization (WHO): Geneva, Switzerland, 2023.
- Craig, K.J.T.; Rizvi, R.; Willis, V.C.; Kassler, W.J.; Jackson, G.P. Effectiveness of Contact Tracing for Viral Disease Mitigation and Suppression: Evidence-Based Review. JMIR Public Health Surveill. 2021, 7, e32468. [Google Scholar] [CrossRef] [PubMed]
- Cosma, C.; Galla, L.; Padoan, A.; Furlan, G.; Marchioro, L.; Zaninotto, M.; Basso, D.; Plebani, M. SARS-CoV-2 specific T-cell humoral response assessment after COVID-19 vaccination using a rapid direct real-time PCR amplification. Clin. Chem. Lab. Med. (CCLM) 2023, 61, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Padoan, A.; Cosma, C.; Bonfante, F.; Della Rocca, F.; Barbaro, F.; Santarossa, C.; DallOlmo, L.; Pagliari, M.; Bortolami, A.; Cattelan, A.; et al. SARS-CoV-2 neutralizing antibodies after one or two doses of Comirnaty (BNT162b2 BioNTech/Pfizer): Kinetics and comparison with chemiluminescent assays. Clin. Chim. Acta 2021, 523, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Sheikh-Mohamed, S.; Sanders, E.C.; Gommerman, J.L.; Tal, M.C. Guardians of the oral and nasopharyngeal galaxy: IgA and protection against SARS-CoV-2 infection. Immunol. Rev. 2022, 309, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Chiara, C.D.; Cantarutti, A.; Costenaro, P.; Donà, D.; Bonfante, F.; Cosma, C.; Ferrarese, M.; Cozzani, S.; Petrara, M.R.; Carmona, F.; et al. Long-term Immune Response to SARS-CoV-2 Infection Among Children and Adults After Mild Infection. JAMA Netw. Open 2022, 5, e2221616. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.E.; Asfour, A.; Sewell, T.B.; Hooe, B.; Pryce, P.; Earley, C.; Shen, M.Y.; Kerner-Rossi, M.; Thakur, K.T.; Vargas, W.S.; et al. Neurological issues in children with COVID-19. Neurosci. Lett. 2021, 743, 135567. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Z.; Cheng, X.Q.; Li, J.Y.; Zhang, P.; Yi, P.; Xu, X.; Zhou, X.D. Saliva in the diagnosis of diseases. Int. J. Oral Sci. 2016, 29, 133–137. [Google Scholar] [CrossRef]
- Sharma, A.; Farouk, I.A.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Rai, P.; Kumar, B.K.; Deekshit, V.K.; Karunasagar, I.; Karunasagar, I. Detection technologies and recent developments in the diagnosis of COVID-19 infection. Appl. Microbiol. Biotechnol. 2021, 105, 441–455. [Google Scholar] [CrossRef]
- Li, D.; Calderone, R.; Nsouli, T.M.; Reznikov, E.; Bellanti, J.A. Salivary and serum IgA and IgG responses to SARS-CoV-2-spike protein following SARS-CoV-2 infection and after immunization with COVID-19 vaccines. Allergy Asthma Proc. 2022, 43, 419–430. [Google Scholar] [CrossRef]
- Wang, Y.; Upadhyay, A.; Pillai, S.; Khayambashi, P.; Tran, S.D. Saliva as a diagnostic specimen for SARS-CoV-2 detection: A scoping review. Oral Dis. 2022, 28, 2362–2390. [Google Scholar] [CrossRef] [PubMed]
- Kaczor-Urbanowicz, K.E.; Martin Carreras-Presas, C.; Aro, K.; Tu, M.; Garcia-Godoy, F.; Wong, D.T.W. Saliva diagnostics—Current views and directions. Exp. Biol. Med. 2017, 242, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Pisanic, N.; Randad, P.R.; Kruczynski, K.; Manabe, Y.C.; Thomas, D.L.; Pekosz, A.; Klein, S.L.; Betenbaugh, M.J.; Clarke, W.A.; Laeyendecker, O.; et al. COVID-19 Serology at Population Scale: SARS-CoV-2-Specific Antibody Responses in Saliva. J. Clin. Microbiol. 2020, 59, 10-1128. [Google Scholar] [CrossRef] [PubMed]
- Klingler, J.; Lambert, G.S.; Itri, V.; Liu, S.; Bandres, J.C.; Enyindah-Asonye, G.; Liu, X.; Simon, V.; Gleason, C.R.; Kleiner, G.; et al. Detection of Antibody Responses Against SARS-CoV-2 in Plasma and Saliva from Vaccinated and Infected Individuals. Front. Immunol. 2021, 12, 759688. [Google Scholar] [CrossRef] [PubMed]
- Padoan, A.; Bonfante, F.; Cosma, C.; Chiara, C.D.; Sciacovelli, L.; Pagliari, M.; Bortolami, A.; Costenaro, P.; Musso, G.; Basso, D.; et al. Analytical and clinical performances of a SARS-CoV-2 S-RBD IgG assay: Comparison with neutralization titers. Clin. Chem. Lab. Med. (CCLM) 2021, 59, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Clinical Laboratory Standards Institute. Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach—CLSI Document EP06-A; Clinical Laboratory Standards Institute: Wayne, PA, USA, 2003. [Google Scholar]
- Padoan, A.; Cosma, C.; Bonfante, F.; Della Rocca, F.; Barbaro, F.; Santarossa, C.; Dall’Olmo, L.; Pagliari, M.; Bortolami, A.; Cattelan, A.; et al. Neutralizing antibody titers six months after Comirnaty vaccination: Kinetics and comparison with SARS-CoV-2 immunoassays. Clin. Chem. Lab. Med. (CCLM) 2021, 60, 456–463. [Google Scholar] [CrossRef]
- Civita, E.L.; Zannella, C.; Brusa, S.; Romano, P.; Schettino, E.; Salemi, F.; Carrano, R.; Gentile, L.; Punziano, A.; Lagnese, G.; et al. BNT162b2 Elicited an Efficient Cell-Mediated Response against SARS-CoV-2 in Kidney Transplant Recipients and Common Variable Immunodeficiency Patients. Viruses 2023, 15, 1659. [Google Scholar] [CrossRef]
- Du, W.; Yu, J.; Wang, H.; Zhang, X.; Zhang, S.; Li, Q.; Zhang, Z. Clinical characteristics of COVID-19 in children compared with adults in Shandong Province China. Infection 2020, 48, 445–452. [Google Scholar] [CrossRef]
- Arteaga-Müller, G.Y.; Olivo-Gutierrez, M.; Favela-Aragon, K.L.; Hernández-Castillo, P.A.; Esquivel-Gomez, V.; Camacho-Ortiz, A. Prevalence of antibodies against SARS-CoV-2 in hemodialysis patients. Int. Urol. Nephrol. 2021, 54, 457–458. [Google Scholar] [CrossRef]
- Di Chiara, C.; Boracchini, R.; Sturniolo, G.; Barbieri, A.; Costenaro, P.; Cozzani, S.; Pieri, M.D.; Liberati, C.; Zin, A.; Padoan, A.; et al. Clinical features of COVID-19 in Italian outpatient children and adolescents during Parental Delta, and Omicron waves: A prospective, observational, cohort study. Front. Pediatr. 2023, 11, 1193857. [Google Scholar] [CrossRef]
- Turtle, L.; Thorpe, M.; Drake, T.M.; Swets, M.; Palmieri, C.; Russell, C.D.; Ho, A.; Aston, S.; Wootton, D.G.; Richter, A.; et al. Outcome of COVID-19 in hospitalised immunocompromised patients: An analysis of the WHO ISARIC CCP-UK prospective cohort study. PLoS Med. 2023, 20, e1004086. [Google Scholar] [CrossRef] [PubMed]
- Oyeniran, S.J.; Wang, H.; Everhart, K.; Mack, K.; Harvey, K.; Leber, A.L. Performance comparison of three commercial tests for the detection of SARS-CoV-2 antibodies in a common set of pediatric samples. J. Immunol. Methods 2023, 520, 113536. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.M. Multisystem Inflammatory Syndrome in Children (MIS-C). Curr. Allergy Asthma Rep. 2022, 22, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Michailidou, E.; Poulopoulos, A.; Tzimagiorgis, G. Salivary diagnostics of the novel coronavirus SARS-CoV-2 (COVID-19). Oral Dis. 2022, 28, 867–877. [Google Scholar] [CrossRef]
- Hettegger, P.; Huber, J.; Paßecker, K.; Soldo, R.; Kegler, U.; Nöhammer, C.; Weinhäusel, A. High similarity of IgG antibody profiles in blood and saliva opens opportunities for saliva based serology. PLoS ONE 2019, 14, e0218456. [Google Scholar] [CrossRef]
- Torul, D.; Omezli, M.M. Is saliva a reliable biofluid for the detection of COVID-19? Dent. Med. Probl. 2021, 58, 229–235. [Google Scholar] [CrossRef]
- Egorov, A.I.; Griffin, S.M.; Fuzawa, M.; Kobylanski, J.; Grindstaff, R.; Padgett, W.; Simmons, S.; Hallinger, D.R.; Styles, J.N.; Wickersham, L.; et al. A Multiplex Noninvasive Salivary Antibody Assay for SARS-CoV-2 Infection and Its Application in a Population-Based Survey by Mail. Microbiol. Spectr. 2021, 9, e00693-21. [Google Scholar] [CrossRef]
- Guerra, E.N.S.; de Castro, V.T.; dos Santos, J.A.; Acevedo, A.C.; Chardin, H. Saliva is suitable for SARS-CoV-2 antibodies detection after vaccination: A rapid systematic review. Front. Immunol. 2022, 13, 1006040. [Google Scholar] [CrossRef]
- Casian, J.G.; Angel, A.N.; Lopez, R.; Bagos, C.; MacMullan, M.A.; Bui, M.L.; Chellamathu, P.; Das, S.; Turner, F.; Slepnev, V.; et al. Saliva-Based ELISAs for Effective SARS-CoV-2 Antibody Monitoring in Vaccinated Individuals. Front. Immunol. 2021, 12, 701411. [Google Scholar] [CrossRef]
- Keuning, M.W.; Grobben, M.; Bijlsma, M.W.; Anker, B.; Berman-de Jong, E.P.; Cohen, S.; Felderhof, M.; de Groen, A.E.; de Groof, F.; Rijpert, M.; et al. Differences in systemic and mucosal SARS-CoV-2 antibody prevalence in a prospective cohort of Dutch children. Front. Immunol. 2022, 13, 976382. [Google Scholar] [CrossRef]
- Azzi, L.; Gasperina, D.D.; Veronesi, G.; Shallak, M.; Maurino, V.; Baj, A.; Gianfagna, F.; Cavallo, P.; Dentali, F.; Tettamanti, L.; et al. Mucosal immune response after the booster dose of the BNT162b2 COVID-19 vaccine. eBioMedicine 2023, 88, 104435. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.I.; Dropulic, L.; Wang, K.; Gangler, K.; Morgan, K.; Liepshutz, K.; Krogmann, T.; Ali, M.A.; Qin, J.; Wang, J.; et al. Comparison of Levels of Nasal Salivary, and Plasma Antibody to Severe Acute Respiratory Syndrome Coronavirus 2 during Natural Infection and After Vaccination. Clin. Infect. Dis. 2022, 76, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Boey, L.; Roelants, M.; Merckx, J.; Hens, N.; Desombere, I.; Duysburgh, E.; Vandermeulen, C. Age-dependent seroprevalence of SARS-CoV-2 antibodies in school-aged children from areas with low and high community transmission. Eur. J. Pediatr. 2022, 181, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Liew, F.; Talwar, S.; Cross, A.; Willett, B.J.; Scott, S.; Logan, N.; Siggins, M.K.; Swieboda, D.; Sidhu, J.K.; Efstathiou, C.; et al. SARS-CoV-2-specific nasal IgA wanes 9 months after hospitalisation with COVID-19 and is not induced by subsequent vaccination. eBioMedicine 2023, 87, 104402. [Google Scholar] [CrossRef]
- Evans, J.P.; Zeng, C.; Carlin, C.; Lozanski, G.; Saif, L.J.; Oltz, E.M.; Gumina, R.J.; Liu, S.-L. Neutralizing antibody responses elicited by SARS-CoV-2 mRNA vaccination wane over time and are boosted by breakthrough infection. Sci. Transl. Med. 2022, 14, eabn8057. [Google Scholar] [CrossRef]
- Madsen, J.R.; Holm, B.E.; Pérez-Alós, L.; Bayarri-Olmos, R.; Rosbjerg, A.; Fogh, K.; Pries-Heje, M.M.; Møller, D.L.; Hansen, C.B.; Heftdal, L.D.; et al. Short-Lived Antibody-Mediated Saliva Immunity against SARS-CoV-2 after Vaccination. Microbiol. Spectr. 2023, 11, e04947-22. [Google Scholar] [CrossRef]
- Notarte, K.I.; Ver, A.T.; Velasco, J.V.; Pastrana, A.; Catahay, J.A.; Salvagno, G.L.; Yap, E.P.H.; Martinez-Sobrido, L.; Torrelles, J.B.; Lippi, G.; et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: A systematic review. Crit. Rev. Clin. Lab. Sci. 2022, 59, 373–390. [Google Scholar] [CrossRef]
- Notarte, K.I.; Catahay, J.A.; Peligro, P.J.; Velasco, J.V.; Ver, A.T.; Guerrero, J.J.; Liu, J.; Lippi, G.; Benoit, S.W.; Henry, B.M.; et al. Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature. Vaccines 2023, 11, 724. [Google Scholar] [CrossRef]
- Garziano, M.; Utyro, O.; Poliseno, M.; Santantonio, T.A.; Saulle, I.; Strizzi, S.; Caputo, S.L.; Clerici, M.; Introini, A.; Biasin, M. Natural SARS-CoV-2 Infection Affects Neutralizing Activity in Saliva of Vaccinees. Front. Immunol. 2022, 13, 820250. [Google Scholar] [CrossRef]
- MacMullan, M.A.; Ibrayeva, A.; Trettner, K.; Deming, L.; Das, S.; Tran, F.; Moreno, J.R.; Casian, J.G.; Chellamuthu, P.; Kraft, J.; et al. ELISA detection of SARS-CoV-2 antibodies in saliva. Sci. Rep. 2020, 10, 20818. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | Children | Adults | p-Value * | |
|---|---|---|---|---|
| n | 187 | 95 (50.8%) | 92 (49.2%) | - |
| Age (mean ± SD) | 24.66 ± 17.15 | 9.01 ± 3.3 | 40.8 ± 8.4 | t = 34.4, p < 0.001 |
| Gender | 105/82 (F/M) | 49/46 (F/M) | 56/36 (F/M) | Fisher’s exact test, p = 0.239 |
| Comorbidities | 30/187 (16.0%) | 17/95 (17.9%) | 13/92 (14.1%) | Fisher’s exact test, p = 0.552 |
| Prolonged therapy | 25/183 ^ | 16/94 (17.0%) ^ | 9/89 (10.1%) ^ | Fisher’s exact test, p = 0.201 |
| Previous SARS-CoV-2 infection | 154/187 (82.35%) | 80/95 (84.21%) | 74/92 (80.43%) | Fisher’s exact test, p = 0.567 |
| Time from last COVID-19 or vaccination (median and IQR $) | 175.3 ± 82.7 | 174.5 ± 72.5 | 176.1 ± 92.3 | t = 0.119, p = 0.904 |
| Salivary N/S RBD IgG (kAU/L) | 29.7 (0.5–87.4) | 2.96 (0.5–67.5) | 50.6 (0.5–127.6) | χ2 = 6.4, p = 0.019 |
| Anti SARS-CoV-2 S-RBD IgG (kBAU/L) (median and IQR $) | 1672.5 (514.4–3345.8) | 1138.8 (321.3–2706.3) | 2022.9 (808.4–4118.3) | χ2 = 10.4, p = 0.001 |
| Time from Vaccine-Induced Immunization or Time from SARS-CoV-2 Infection | Salivary N/S IgG (kAU/L), Median (IQR), (n) | Serum S-RBD IgG (kBAU/L) Median (IQR), (n) | ||
|---|---|---|---|---|
| Children | Adults | Children | Adults | |
| <113 days | 2.01 (0.5 to 18.1) (n = 21) | 59.4 (2.02 to 117.9) (n = 22) | 1719 (526 to 3596) (n = 21) | 3136 (1382 to 4178) (n = 22) |
| 113 to 180 days | 12.2 (0.5 to 60.7) (n = 16) | 73.8 (0.5 to 192.0) (n = 23) | 1302 (431 to 2521) (n = 16) | 2319 (419 to 5364) (n = 23) |
| 181 to 210 days | 31.9 (0.5 to 110.2) (n = 28) | 47.5 (0.5 to 68.8) (n = 17) | 1426 (378 to 2821) (n = 28) | 1961 (787 to 3345) (n = 17) |
| >210 days | 2.2 (0.5 to 47.1) (n = 30) | 49.1 (1.3 to 328.5) (n = 30) | 800 (89 to 2340) (n = 30) | 1585 (800 to 5523) (n = 30) |
| Children | Adults | |||
|---|---|---|---|---|
| Variables | Coefficients (95%CI) | p-Value | Coefficients (95%CI) | p-Value |
| Age | 0.13 (0.07–0.20) | p < 0.001 | −0.03 (−0.59–(−0.001)) | p = 0.040 |
| Gender | 0.09 (−0.37–0.55) | p = 0.686 | 0.13 (−0.37–0.63) | p = 0.600 |
| Comorbidities | −0.50 (−1.08–0.09) | p = 0.095 | −0.57 (−1.27–0.13) | p = 0.110 |
| Prolonged therapy | −0.57 (−1.12–0.09) | p = 0.092 | −0.06 (−0.89–0.78) | p = 0.890 |
| Previous SARS-CoV-2 infection | 0.10 (−0.58–0.76) | p = 0.770 | −0.52 (−1.12–0.09) | p = 0.750 |
| Time from last COVID-19 or vaccination | −0.001 (−0.004–0.001) | p = 0.316 | 0.0001 (−0.003–0.004) | p = 0.730 |
| Children | Adults | |||
|---|---|---|---|---|
| Variables | Coefficients (95%CI) | p-Value | Coefficients (95%CI) | p-Value |
| Age | 0.08 (0.20–0.15) | p = 0.010 | −0.01 (-0.23–0.01) | p = 0.550 |
| Gender | 0.04 (−0.35–0.44) | p = 0.830 | 0.04 (−0.26–(0.35)) | p = 0.780 |
| Comorbidities | −0.86 (−1.34–(−0.38)) | p = 0.001 | −0.61 (−1.01–(−0.2)) | p = 0.004 |
| Prolonged therapy | −0.95 (−1.43–(−0.48)) | p < 0.001 | −0.33 (−0.83–0.16) | p = 0.190 |
| Previous SARS-CoV-2 infection | 0.95 (0.43–1.47) | p = 0.001 | 0.29 (−0.08–0.67) | p = 0.120 |
| Time from last COVID-19 or vaccination | 0.0001 (−0.002–0.003) | p = 0.910 | −0.001 (−0.003–0.0003) | p = 0.110 |
| log10 Salivary Anti-SARS-CoV-2 N/S IgG | log10 Anti-SARS-CoV-2 S-RBD IgG | |||
|---|---|---|---|---|
| Children | Adults | Children | Adults | |
| Coefficients (95%CI), p-Value | Coefficients (95%CI), p-Value | Coefficients (95%CI), p-Value | Coefficients (95%CI), p-Value | |
| Age | 33.9 (14.5 to 53.3), p = 0.001 | −2.99 (−13.30 to 7.31), p = 0.565 | 0.093 (0.044 to 0.142), p < 0.001 | −0.002 (−0.019 to 0.015), p = 0.785 |
| Gender | 134.9 (5.6 to 264.1), p = 0.041 | 176.4 (−2.9 to 355.6), p = 0.054 | 0.22 (−0.09 to 0.54), p =1.44 | 0.16 (−0.12 to 0.45), p = 0.266 |
| Comorbidities | 219.9 (−56.9 to 496.7), p = 0.158 | −153.5 (−524.3 to 217.4), p = 0.412 | 0.355 (−0.351 to 1.062), p = 0.320 | −0.93 (−1.53 to −0.34), p = 0.002 |
| Prolonged therapy | −45.7 (−327.2 to 235.7), p = 0.747 | 226.3 (−191.9 to 644.5), p = 0.285 | −0.43 (−1.12 to 0.26), p = 0.218 | 0.42 (−0.25 to 1.09), p = 0.216 |
| Previous SARS-CoV-2 infection | 130.9 (−89.6 to 351.6), p = 0.152 | −68.7 (−295.9 to 158.4), p = 0.548 | 0.21 (−0.31 to 0.73), p = 0.429 | 0.11 (−0.25 to 0.48), p = 0.533 |
| Time from last COVID-19 or vaccination (days) | −0.82 (−1.71 to 0.07), p = 0.070 | −0.099 (−1.073 to 0.874), p = 0.839 | 0.0002 (−0.002 to 0.002), p = 0.856 | −0.001 (−0.003 to 0.0003), p = 0.109 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padoan, A.; Cosma, C.; Di Chiara, C.; Furlan, G.; Gastaldo, S.; Talli, I.; Donà, D.; Basso, D.; Giaquinto, C.; Plebani, M. Clinical and Analytical Performance of ELISA Salivary Serologic Assay to Detect SARS-CoV-2 IgG in Children and Adults. Antibodies 2024, 13, 6. https://doi.org/10.3390/antib13010006
Padoan A, Cosma C, Di Chiara C, Furlan G, Gastaldo S, Talli I, Donà D, Basso D, Giaquinto C, Plebani M. Clinical and Analytical Performance of ELISA Salivary Serologic Assay to Detect SARS-CoV-2 IgG in Children and Adults. Antibodies. 2024; 13(1):6. https://doi.org/10.3390/antib13010006
Chicago/Turabian StylePadoan, Andrea, Chiara Cosma, Costanza Di Chiara, Giulia Furlan, Stefano Gastaldo, Ilaria Talli, Daniele Donà, Daniela Basso, Carlo Giaquinto, and Mario Plebani. 2024. "Clinical and Analytical Performance of ELISA Salivary Serologic Assay to Detect SARS-CoV-2 IgG in Children and Adults" Antibodies 13, no. 1: 6. https://doi.org/10.3390/antib13010006