Therapeutic Monoclonal Antibodies Targeting Immune Checkpoints for the Treatment of Solid Tumors

Abstract
:1. Introduction
2. Immunotherapy Overview
2.1. Overview
2.2. CTLA-4 Inhibitors
2.2.1. Background
2.2.2. Mechanism of Action
2.2.3. Indications
2.3. PD-1 Inhibitors
2.3.1. Background
2.3.2. Mechanism of Action
2.3.3. Indications
2.4. PD-L1 Inhibitors
2.4.1. Background
2.4.2. Mechanism of Action
2.4.3. Indications
2.5. LAG-3 Inhibitors
2.5.1. Background
2.5.2. Mechanism of Action
2.5.3. Indications
2.6. TIM-3 Inhibitors
2.6.1. Background
2.6.2. Mechanism of Action
2.6.3. Indications
2.7. CD40 Agonists
2.7.1. Background
2.7.2. Mechanism of Action
2.7.3. Indications
2.8. OX40 Agonists
2.8.1. Background
2.8.2. Mechanism of Action
2.8.3. Indications
3. Clinical Evidence
3.1. Overview
3.2. CTLA-4 Inhibitors
3.2.1. Ipilimumab
Overview
Melanoma
Renal Cell Carcinoma
Non-Small Cell Lung Cancer
3.2.2. Tremelimumab
3.3. PD-1 Inhibitors
3.3.1. Nivolumab
Overview
Bladder Cancer
Colorectal Cancer
Head and Neck Squamous Cell Carcinoma
Hepatocellular Carcinoma
Hodgkin Lymphoma
Melanoma
Non-Small Cell Lung Cancer
Renal Cell Carcinoma
Small Cell Lung Cancer
3.3.2. Pembrolizumab
Overview
Cervical Cancer
Gastric Cancer
Head and Neck Squamous Cell Carcinoma
Hepatocellular Carcinoma
Hodgkin Lymphoma
Lung Cancer
Melanoma
Merkel Cell Carcinoma
MSI-H or dMMR Tumors (Tissue-Agnostic)
Primary Mediastinal B-Cell Lymphoma
Renal Cell Carcinoma
3.4. PD-L1 Inhibitors
3.4.1. Atezolizumab
Overview
Bladder Cancer
Breast Cancer (Triple-Negative)
Non-small Cell Lung Cancer
Small Cell Lung Cancer
3.4.2. Avelumab
Bladder Cancer
Merkel Cell Carcinoma
Renal Cell Carcinoma
3.4.3. Durvalumab
Bladder Cancer
Non-Small Cell Lung Cancer
3.5. LAG-3 Inhibitors
3.5.1. Relatlimab
3.5.2. Ongoing Studies
3.6. TIM-3 Inhibitors
3.7. CD40 Agonists
3.7.1. APX0050M
Melanoma
Pancreatic Cancer
3.7.2. CP-870,893
Metastatic Melanoma
Pancreatic Cancer
3.7.3. Ongoing Studies
3.8. OX40 Agonists
3.8.1. 9B12
Advanced Solid Malignancies
3.8.2. Ongoing Studies
3.9. Combination Therapies
4. Immunotherapy Resistance and Its Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Abbreviation | Interpretation |
| AE | adverse event |
| ALK | anaplastic lymphoma kinase |
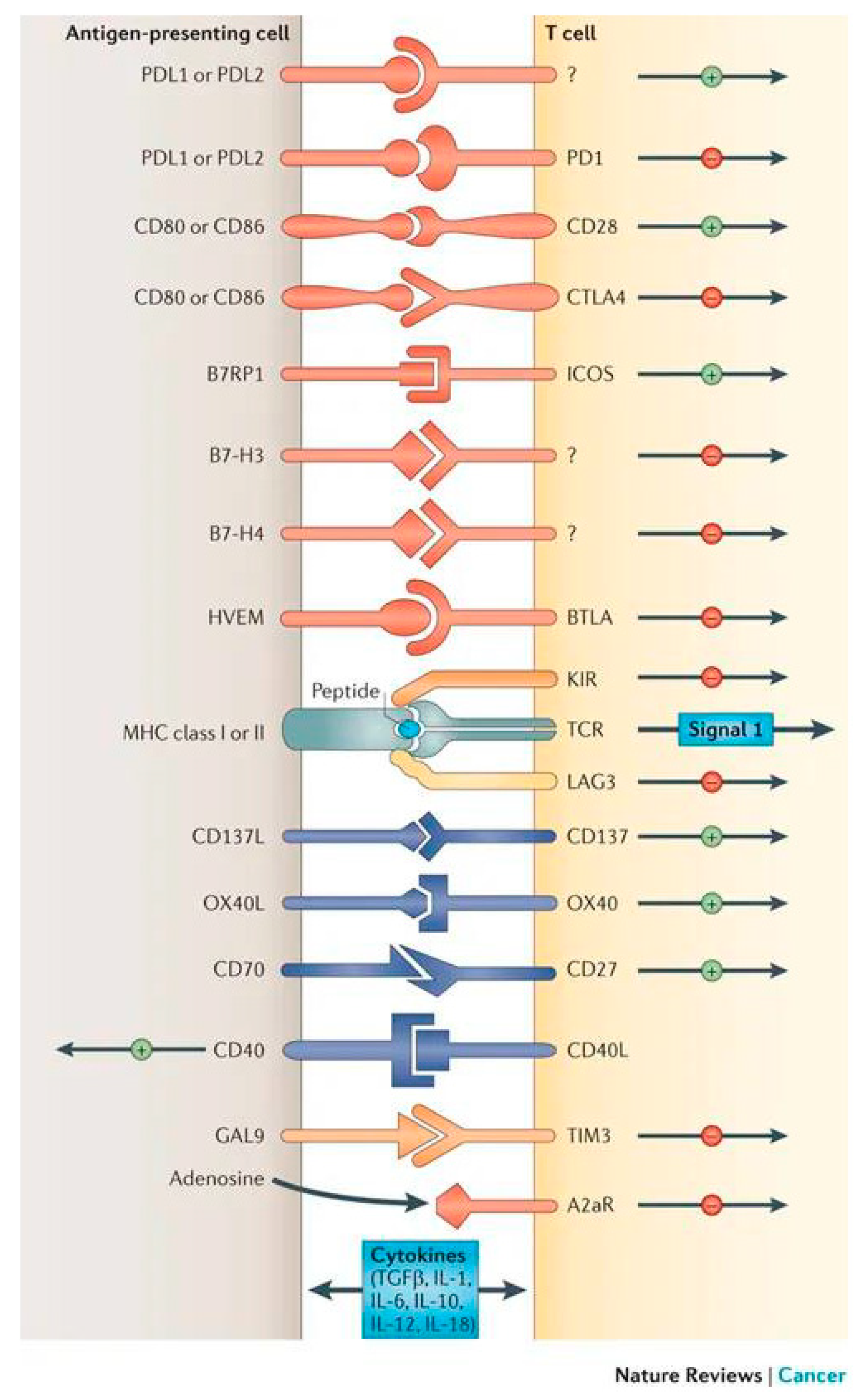
| APC | antigen-presenting cell |
| ASCT | autologous stem-cell transplantation |
| B2M | beta-2-microglobulin |
| BTLA | B and T lymphocyte attenuator |
| CAF | cancer-associated fibroblast |
| CCR4 | C-C chemokine receptor type 4 |
| CD | cluster of differentiation |
| CD40L | CD40 ligand |
| cHL | classical Hodgkin lymphoma |
| CR | complete response |
| CRC | colorectal cancer |
| CRR | complete response rate |
| CSCC | cervical squamous cell carcinoma |
| CSF-1 | colony stimulating factor 1 |
| CTLA-4 | cytotoxic T-lymphocyte-associated protein 4 |
| DLT | dose-limiting toxicity |
| dMMR | DNA mismatch repair-deficient |
| EGFR | epidermal growth factor receptor |
| ER | endoplasmic reticulum |
| FDA | Food and Drug Administration |
| GAL9 | galectin-9 |
| GBM | glioblastoma multiforme |
| GEJ | gastroesophageal junction |
| GITR | glucocorticoid-induced tumor necrosis factor receptor |
| HCC | hepatocellular carcinoma |
| HL | Hodgkin lymphoma |
| HLA | human leukocyte antigen |
| HR | hazard ratio |
| HVEM | tumor necrosis factor receptor superfamily member 14 |
| ICOS | inducible T-cell co-stimulator |
| IDO | indoleamine 2,3-dioxygenase |
| IFN | interferon |
| IL | interleukin |
| KIR | killer cell immunoglobulin-like receptors |
| LAG-3 | lymphocyte-activation gene-3 |
| mAb | monoclonal antibody |
| MCC | Merkel cell carcinoma |
| M-CSF | macrophage colony-stimulating factor |
| MDSC | myeloid-derived suppressor cell |
| MHC | major histocompatibility complex |
| MSI-H | microsatellite instability-high |
| MTD | maximum tolerated dose |
| MɸII | type II macrophage |
| NK | natural killer |
| NSCLC | non-small cell lung cancer |
| NsqNSCLC | non-squamous non-small cell lung cancer |
| ORR | objective response rate |
| OS | overall survival |
| OX40L | OX40 ligand |
| PD-1 | programmed cell death protein-1 |
| PD-L1 | programmed death-ligand 1 |
| PD-L2 | programmed death-ligand 2 |
| PFS | progression-free survival |
| PI3K | phosphatidyl-inositol 3-kinase |
| PRR | partial response rate |
| RCC | renal cell carcinoma |
| rrPMBCL | relapsed/refractory primary mediastinal B-cell lymphoma |
| SCLC | small cell lung cancer |
| sqNSCLC | squamous non-small cell lung cancer |
| TAP | transporter associated with antigen processing |
| TCR | T cell receptor |
| TGF-β | transforming growth factor-beta |
| TIM-3 | T cell immunoglobulin and mucin-domain containing-3 |
| TME | tumor microenvironment |
| TNBC | triple-negative breast cancer |
| TNF | tumor necrosis factor |
| Treg | regulatory T cell |
| VEGF | vascular endothelial growth factor |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target | mAb Function | Drug Examples | IgG Class | Epitope | Affinity (Human Targets) | Year of First FDA Approval | FDA-Approved Indications | Examples of Indications with Clinical Data but no FDA Approval |
|---|---|---|---|---|---|---|---|---|
| CTLA-4 | Antagonist | Ipilimumab (Bristol-Myers Squibb), tremelimumab (MedImmune/AstraZeneca) | I: IgG1 T: IgG2 | I: CTLA-4 F, G strands; TBS 1709 Å2 [4] T: CTLA-4 F, G stands; TBS 1802 Å2 [4,21] | I: Kd = 18.2 nM (CTLA-4) [4,21] T: Kd = 5.9 nM (CTLA-4) [4,21] | 2011 | I: Melanoma, RCC, CRC T: -- | I: NSCLC, Prostate cancer, SCLC T: Melanoma, mesothelioma, NSCLC |
| PD-1 | Antagonist | Nivolumab (Bristol-Myers Squibb), pembrolizumab (Merck & Co) | N: IgG4 P: IgG4 | N: PD-1 N-loop; TBS 1487 Å2 [21] P: PD-1 CD loop; TBS 2126 Å2 [21] | N: Kd = 2.6-3.1 nM (PD-1) [125,126] P: Kd = 29.0 pM (PD-1) [125,126] | 2014 | N: Bladder cancer, CRC, HCC, HL, HNSCC, melanoma, NSCLC, RCC, SCLC P: Bladder cancer, CSCC, ESCC, gastric or GEJ adenocarcinoma, HCC, HL, HNSCC, MCC, melanoma, MSI-H/dMMR tumors (tissue-agnostic), NSCLC, PMBCL, RCC, SCLC, endometrial carcinoma | N: Anal cancer, GBM, Gastric/GEJ cancer, mesothelioma P: Nasopharyngeal carcinoma |
| PD-L1 | Antagonist | Atezolizumab (Roche-Genentech), avelumab (Merck/Pfizer), durvalumab MedImmune/AstraZeneca | At: IgG1 Av: IgG1 D: IgG1 | At: PD-L1 CC’FG β-sheet; TBS 1970 Å2 [23] Av: PD-L1 CC’FG β-sheet and N-terminus; TBS 1865 Å2 [23] D: PD-L1 CC’FG β-sheet and N-terminus; TBS 2106 Å2 [23] | At: Kd = 0.4 nM (PD-L1) [23] Av: Kd = 42.1 pM (PD-L1) [23] D: Kd = 22.0 pM (PD-L1) [23] | 2016 | At: Bladder cancer, NSCLC, SCLC, TNBC Av: Bladder cancer, MCC, RCC D: Bladder cancer, NSCLC | At: Melanoma Av: NSCLC D: Mesothelioma |
| Therapy | Cancer | Study | Phase | Stage of Disease | Treatment Regimen | N | Median OS (Months) | Median PFS (Months) | ORR (%) | CRR (%) | Grade III/IV AEs (%) | Resultant FDA-Approved Indication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ipilimumab | CRC | Overman et al. (2018) [127] CheckMate 142 | II | Recurrent of metastatic dMMR/MSI-H disease | Nivolumab 3 mg/kg + ipilimumab 1 mg/kg Q3wks x4 followed by nivolumab 3 mg/kg Q2wks | 119 | NR | NR | 49 (95% CI: 39.5–58.1) | 4 | 32.0 | Approved in combination with nivolumab for previously treated MSI-H/dMMR metastatic CRC (July 2018) |
| Melanoma | Hodi et al. (2010) [38] | III | Unresectable, stage III/IV disease | A. Ipilimumab 3mg/kg + gp100 peptide vaccine B. Ipilimumab 3mg/kg monotherapy C. gp100 peptide vaccine monotherapy (all Q3wks.) | 676 A = 403 B = 137 C = 136 | A. 10.0 (95% CI: 8.5–11.5) B. 10.1 (95% CI: 8.0–13.8) C. 6.4 (95% CI: 5.5–8.7) (HR = 0.68, p < 0.001 A vs. C; HR = 0.66, p = 0.003 B vs. C) | -- | A. 5.7 (95% CI: 3.7–8.4) B. 10.9 (95% CI: 6.3–17.4) C. 1.5 (p = 0.04 A vs. B; p = 0.04 A vs. C; p = 0.001 B vs. C) | A. 0.2 B. 1.5 C. 0 | A.+ B. 10–15 C. 3.0 | Unresectable or metastatic melanoma (March 2011) | |
| Postow et al. (2015) [128] CheckMate-069 | II | Metastatic melanoma with no prior treatment | A. Ipilimumab 3 mg/kg + nivolumab 1 mg/kg Q3wks followed by nivolumab 3 mg/kg Q2wks B. Ipilimumab 3 mg/kg + placebo Q3wks followed by placebo Q2wks | 142 A. 95 B. 47 | -- | A. NR B. 4.4 HR = 0.4, p < 0.001 | In BRAF wild-type group: A. 61 B. 11 p < 0.001 | In BRAF wild-type group: A. 16 B. 0 | A. 54% B. 20% | Approved in combination with nivolumab for the treatment of BRAF V600 wild type unresectable or metastatic melanoma (October 2015) | ||
| Larkin et al. (2015) [129] CheckMate 067 | III | Previously untreated, stage III (unresectable) or stage IV disease with known BRAF V600 mutation status | A: Nivolumab 1mg/kg + ipilimumab 3mg/kg Q3wks., followed by nivolumab 3mg/kg Q2wks. B: Nivolumab 3mg/kg + placebo Q2wks. C. Ipilimumab 2mg/kg + placebo Q3wks. | 945 A = 314 B = 316 C = 315 | -- | A. 11.5 (95% CI: 8.9–16.7) B. 6.9 (95% CI: 4.3–9.5) C. 2.9 (95% CI: 2.8-3.4) (HR = 0.42, p < 0.001 A vs. C; HR = 0.57, p < 0.001 B vs. C) | A. 57.6 (95% CI: 52.0–63.2) B. 43.7 (95% CI: 38.1–49.3) C. 19 (95% CI: 14.9–23.8) | A. 11.5 B. 8.9 C. 2.2 | A. 55.0 B. 16.3 C. 27.3 | Expanded indication: in combination with nivolumab for unresectable or metastatic melanoma regardless of BRAF V600 mutation status (January 2016) | ||
| Eggermont et al. (2015) [130] EORTC 18071 | III | Completely resected, stage III disease | A. Ipilimumab 10mg/kg Q3wks. for 4 doses, then Q3months thereafter B. Placebo | 951 A = 475 B = 476 | -- | A. 11.6 (95% CI: 8.7–15.5) B. 8.4 (95% CI: 7.0–10.8) (HR = 0.75; p = 0.0013) | -- | -- | A. 54% B. 25% | Expanded indication: adjuvant treatment of cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm following complete resection, including total lymphadenectomy (October 2015) | ||
| Merchant et al. (2016) [131] | I | ≤21 years of age with progressive or recurrent solid tumors | Dose escalation cohorts given ipilimumab 1, 3, 5, or 10 mg/m2 IV Q3wks in 3 + 3 design | 33 | -- | -- | 0 | 0 | 27% | |||
| Geoerger et at. (2017) [132] | II | Patients ages 12-18 with unresectable stage III or IV malignant melanoma | A. Ipilimumab 3 mg/kg Q3wks B. Ipilimumab 10 mg/kg Q3wks | 12 A = 4 B = 8 | A. 18.2 (95% CI: 8.9–18.2) B. NR (95% CI: 5.2-NR) | A. 2.6 months (95% CI: 2.3–8.5) B. 2.9 months (95% CI: 0.7-NR) | Overall: 17 A: 0 B: 28.6 | A: 0 B: 0 | A. 25 B. 62.5 | Approval expanded to include pediatric patients 12 years and older with unresectable or metastatic melanoma | ||
| Long et al. (2018) [133] | II | Stage IV disease with active brain metastases (Groups A,B—asymptomatic and/or CNS treatment naïve; Group C—symptomatic and/or failed prior treatment) | A. Nivolumab 1mg/kg + ipilimumab 3mg/kg Q3wks x4, followed by nivolumab 3mg/kg Q2wks. B. Nivolumab 3mg/kg Q2wks. C. Nivolumab 3mg/kg Q2wks. | 79 A = 36 B = 27 C = 16 | -- | -- | A. 46 (95% CI: 29–63) B. 20 (95% CI: 7–41) C: 6 (95% CI: 0–30) | A. 19 B. 12 C. 0 | A. 62 B. 44 C. 9 | -- | ||
| NSCLC | Lynch et al. (2012) [41] | II | Chemotherapy naïve disease | A. Paclitaxel + carboplatin + placebo B. Paclitaxel + carboplatin + concurrent ipilimumab 10mg/kg Q3wks. x4, then paclitaxel + carboplatin + placebo Q3wks. x2 C. Paclitaxel + carboplatin + placebo Q3wks. x2, then addition of ipilimumab to regimen at 10mg/kg Q3wks. x4 | 204 A = 66 B = 70 C = 68 | A. 8.3 (95% CI: 6.8–12.4) B. 9.7 (95% CI: 7.6–12.5) C. 12.2 (95% CI: 9.3–14.4) (HR = 0.99, p = 0.48 B vs. A; HR = 0.87, p = 0.23 C vs. A) | A. 4.2 (95% CI: 2.8-5.3) B. 4.1 (95% CI: 2.8–5.3) C. 5.1 (95% CI: 4.2–5.7) (HR = 0.88, p = 0.25 B vs. A; HR = 0.69; p = 0.02 C vs. A) | A; 14 (95% CI: 6–24) B: 21 (95% CI: 13–33) C: 32 (95% CI: 22–45) | A. 0 B. 0 C. 0 | A. 37 B. 41 C. 39 | -- | |
| Govindan et al. (2017) [42] | III | Metastatic or recurrent disease, chemotherapy naïve | A. Paclitaxel + carboplatin + ipilimumab 10mg/kg Q3wks., then ipilimumab maintenance Q12wks. B. Paclitaxel + carboplatin + placebo Q3wks., then placebo maintenance Q12wks. | 749 A = 388 B = 361 | A. 13.4 B. 12.4 (HR = 0.9, p = 0.25) | A. 5.6 B. 5.6 (HR = 0.87) | A. 45.3 (95% CI: 36.9–54.0) B. 26.9 (95% CI: 20.2–34.4) | A. <1 B. <1 | A. 51 B. 35 | -- | ||
| Hellman et al. (2018) [134] CheckMate 227 | III | Metastatic or recurrent disease, high mutational burden | A. Nivolumab 3mg/kg Q2wks. + ipilimumab 1mg/kg Q6wks. B. Platinum doublet therapy Q3wks. C. Nivolumab 240mg Q2wks. | 1739 (1:1:1 ratio) | -- | A: 7.2 (95% CI: 5.5–13.2) B: 5.5 (95% CI: 4.4–5.8) C: 4.2 (95% CI: 2.7–8.3) (HR = 0.58, p < 0.001 A vs. B; HR = 0.95, p = 0.78 C vs. B) | A. 45.3 (95% CI: 36.9–54.0) B. 26.9 (95% CI: 20.2–34.4) | A: 3.6 B: 0.6 | A: 31.2 B: 36.1 C: 18.9 | -- | ||
| Prostate cancer | Slovin et al. (2013) [135] | I/II | Metastatic castration resistant disease | Ipilimumab 2mg/kg, 5mg/kg, or 10mg/kg Q3wks. +/- radiation | 71 | 17.4 (95% CI: 11.5–24.7) | -- | -- | 4 | 32 | -- | |
| RCC | Motzer et al. (2018) [39] CheckMate 214 | III | Advanced, untreated disease | A. Nivolumab 3mg/kg + ipilimumab 1mg/kg Q2wks. B. Sunitinib 50mg QD for 4 wks. | 1096 A = 550 B = 546 | A. NR (95% CI: 28.2–NR) B. 26.0 (95% CI: 22.1–NR) (HR = 0.63, p < 0.001) | A. 11.6 (95% CI: 8.7–15.5) B. 8.4 (95% CI: 7.0–10.8) (HR = 0.82, p = 0.03) | A. 42 (95% CI: 37–47) B. 27 (95% CI: 22–31) (p < 0.001) | A. 9 B. 1 | A: 46 B: 63 | Combination ipilimumab/nivolumab for intermediate- or poor-risk, previously untreated advanced RCC (April 2018) | |
| SCLC | Reck et al. (2013) [136] | II | Chemotherapy naïve, extensive disease | A. Paclitaxel + carboplatin + placebo B. Paclitaxel + carboplatin + concurrent ipilimumab 10mg/kg Q3wks. x4, then paclitaxel + carboplatin + placebo Q3wks. x2 C. Paclitaxel + carboplatin Q3wks. x2, then addition of ipilimumab to regimen at 10mg/kg Q3wks. x4 | 130 A = 45 B = 43 C = 42 | A. 9.9 (95% CI: 8.6–11.7) B: 9.1 (95% CI: 6.7–13.0) C: 12.9 (95% CI: 7.9–16.5) (HR = 0.95, p = 0.41 B vs. A; HR = 0.75, p = 0.13 C vs. A) | A. 5.3 (95% CI: 4.7–5.7) B. 5.7 (95% CI: 5.2–6.9) C. 6.4 (95% CI: 5.3–7.8) (HR = 0.75, p = 0.11 B vs. A; HR = 0.64, p = 0.03 C vs. A) | A. 49 (95% CI: 34–64) B. 33 (95% CI: 19–49) C. 57 (95% CI: 41–72) | A: 0 B: 2 C: 0 | A: 30 B: 43 C. 50 | -- | |
| Reck et al. (2016) [137] CA184-156 | III | Newly diagnosed, extensive disease | A. Chemotherapy with etoposide and either cisplatin or carboplatin plus ipilimumab 10mg/kg Q3wks. followed by ipilimumab maintenance Q12wks. B. Chemotherapy with etoposide and either cisplatin or carboplatin plus placebo Q3wks. followed by placebo maintenance Q12wks. | 954 A = 478 B = 476 | A. 11.0 (95% CI: 10.5–11.3) B. 10.9 (95% CI: 10.0––11.5) (HR = 0.94, p = 0.38) | A. 4.6 (95% CI: 4.5–5.0) B. 4.4 (95% CI: 4.4–4.6) (HR = 0.85; p = 0.02) | A. 62 (95% CI: 58–67) B: 62 (95% CI: 58–67) | A: <1 B: 0 | A: 48 B: 44 | -- | ||
| Tremelimumab | Melanoma | Ribas et al. (2013) [138] | III | Treatment naive unresectable stage IIIc/IV disease | A. Tremelimumab 15 mg/kg Q90days B. Physician’s choice of standard of care chemotherapy | 655A = 328 B = 327 | A. 12.58 B. 10.71 HR = 0.88, p = 0.127 | -- | A. 10.7 (95% CI: 7.8–14.9) B. 9.8 (95% CI: 6.8–13.5) | A. 3 B. 2 | A. 52 B. 37 | |
| Mesothelioma | Calabro et al. (2015) [139] | II | Chemotherapy-resistant, stage III disease | Tremelimumab 10mg/kg Q4wks. x6, then Q12wks. | 29 | 11.3 (95% CI: 3.4–19.2) | 6.2 (95% CI: 5.7–6.7) | -- | 0 | 7 | Orphan Drug Designation for treatment of malignant mesothelioma (April 2015) | |
| Maio et al. (2017) [43] | IIb | Unresectable pleural or peritoneal disease | A. Tremelimumab 10mg/kg Q4wks. x4, then Q12wks. B. Placebo | 568A = 382 B = 189 | A. 7.7 (95% CI: 6.8–8.9) B. 7.3 (95% CI: 6.8–8.9) (HR = 0.92, p = 0.41) | A. 2.8 (95% CI: 2.8–2.8) B. 2.7 (95% CI: 2.7–2.8) (HR = 0.81, p = 0.03) | A. 4.5 (95% CI: 2.6–7.0) B. 1.1 (95% CI: 0.1–3.8) | A. 0 B. 0 | A. 65 B. 48 | -- | ||
| NSCLC | Rizvi et al. (2018) [140] | III | Chemotherapy naïve disease | A. Durvalumab 20mg/kg Q4wks B. Durvalumab 20mg/kg + tremelimumab 1mg/kg Q4wks. C. Chemotherapy x6 cycles | 488(1:1:1 ratio) | A. 16.3 (97.5% CI: 0.56–1.02) B. 11.9 (98.8% CI: 0.61–1.17) C. 12.9 (HR = 0.76, p = 0.036 A vs. C; HR = 0.85, p = 0.202 B vs. C) | A. – B. 3.9 (99.5% CI: 0.72–1.53) C. 5.4 (HR = 1.05; p = 0.705 B vs. C) | -- | -- | A: 14.6 B: 22.1 C: 33.8 | -- |
| Cancer | Study | Phase | Stage of Disease | Treatment Regimen | N | Median OS (Months) | Median PFS (Months) | ORR (%) | CRR (%) | Grade III/IV AEs (%) | Resultant FDA-Approved Indication |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anal SCC | Morris et al. (2017) [141] | II | Treatment refractory metastatic squamous cell cancer of the anal canal | Nivolumab 3 mg/kg Q2wks | 37 | 11.5 (95% CI: 7.1-NE) | 4.1 (95% CI: 3.0–7.9) | 24 (95% CI: 15–33) | 5.4 | 13.5 | -- |
| Bladder cancer | Sharma et al. (2017) [44] CheckMate 275 | II | Metastatic urothelial carcinoma, history of ≥1 treatment of platinum therapy | Nivolumab 3mg/kg Q2wks. | 270 | All. 8.7 (95% CI: 6.1-NE) PD-L1+. 11.30 (95% CI: 8.7-NE) PD-L1-. 6.0 (4.3–8.1) | All. 2 months (95% CI: 1.9–2.6) | All. 19.6 (95% CI: 15.0–24.9) | All. 2% | All. 18.0% | Locally advanced or metastatic urothelial carcinoma with disease progression during or following platinum chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant platinum chemotherapy (February 2017) |
| CRC | Overman et al. (2017) [45] | II | Recurrent or metastatic dMMR/MSI-H disease | Nivolumab 3mg/kg Q2wks. | 74 | NR | 14.3 (95% CI: 4.3-NE) | 31 (95% CI: 20.8–42.9) | 0 | 21.0 | Patients 12 years and older with dMMR/MSI-H metastatic CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan (August 2017) |
| Overman et al. (2018) [127] CheckMate 142 | II | Recurrent of metastatic dMMR/MSI-H disease | Nivolumab 3 mg/kg + ipilimumab 1 mg/kg Q3wks x4 followed by nivolumab 3 mg/kg Q2wks | 119 | NR | NR | 49 (95% CI: 39.5-58.1) | 4 | 32.0 | Approved in combination with ipilimumab for previously treated MSI-H/dMMR metastatic CRC (July 2018) | |
| Gastric or GEJ cancer | Kang et al. (2017) [142] | III | Unresectable advanced or recurrent disease refractory to, or intolerant of, standard therapy | A. Nivolumab 3 mg/kg Q2wks B. Placebo | 493 A = 330 B = 163 | A. 5.26 (95% CI: 4.60–6.37) B. 4.14 (95% CI: 3.42–4.86) HR = 0.63, p < 0.0001 | A. 1.61 (95% CI: 1.54-2.30) B. 1.45 (95% CI: 1.45–1.54) HR = 0.60, p < 0.0001 | A. 11.2 (95% CI: 7.7–15.6) B. 0 (95% CI: 0–2.8) | A. 0 B. 0 | A. 10 B. 4 | -- |
| GBM | Reardon et al. (2017) [143] Checkmate 143 | III | Patients with first recurrence of GBM | A. Nivolumab 3 mg/kg Q2wks B. Bevacizumab 10 mg/kg Q2wks | 369 A = 184 B = 185 | A. 9.8 (95% CI: 8.2–11.8) B. 10.0 (95% CI: 9.0–11.8) HR = 1.04, p = 0.76 | A. 1.5 (95% CI: 1.5–1.5) B. 3.5 (95% CI: 2.9–4.6) HR = 1.97, p < 0.0001 | A. 8 B. 23 | -- | A. 18 B. 15 | -- |
| CheckMate 498 (2019) [144] | III | Centrally confirmed treatment naive MGMT-unmethylated disease | A. Nivolumab + radiation B. Temozolomide + radiation | ~550 | Primary endpoint of OS not met | -- | -- | -- | -- | -- | |
| Checkmate 548 (2019) [145] | III | Newly diagnosed MGMT-methylated disease | A. Nivolumab + radiation + temozolomide B. Radiation + temozolomide (standard of care) | -- | Primary endpoint of PFS not met | -- | -- | -- | -- | ||
| HCC | El-Khoueiry et al. (2017) [47] CheckMate 040 | I/II | Advanced disease | Nivolumab 3mg/kg Q2wks. | 214 | -- | 4.0 (95% CI: 2.9–5.4) | 20 (95% CI: 15–26) | 1.0 | 19.0 | Advanced HCC in patients who have been previously treated with sorafenib (September 2017) |
| HL | Ansell et al. (2015) [49] CheckMate 039 | I | Relapsed or refractory disease | Nivolumab 3mg/kg on week 1, week 4, then Q2wks. thereafter | 23 | -- | -- | 87 (95% CI: 66–97) | 17 | 52.0 | -- |
| Younes et al. (2016) [50] CheckMate 205 | II | Relapsed refractory classical HL following ASCT and BV | Nivolumab 3mg/kg Q2wks. | 80 | -- | 10.0 (95% CI: 8.4-NE) | 66.3 (95% CI: 54.8–76.4) | 9.0 | 25.0 | cHL that has relapsed or progressed after ASCT and post-transplant BV (May 2016) | |
| HNSCC | Ferris et al. (2016) [46] CheckMate 141 | III | Recurrent or metastatic disease | A: Nivolumab 3 mg/kg Q2wks. B: Standard single agent chemotherapy (cetuximab, MTX, docetaxel) | 361 A = 240 B = 121 | A. 7.5 (95% CI: 5.5–9.1) B. 5.1 (95% CI: 4.0–6.0) (HR = 0.70, p = 0.01) | A. 2.0 (95% CI: 1.9–2.1) B: 2.3 (95% CI: 1.9–3.1) (HR = 0.89, p = 0.32) | A. 13.3 (95% CI: 9.3–18.3) B. 5.8 (2.4–11.6) | A. 2.5 B. 0.8 | A. 13.1 B. 35.1 | Recurrent or metastatic HNSCC with disease progression on or after a platinum-based therapy (November 2016) |
| Melanoma | Robert et al. (2014) [65] CheckMate 066 | III | Metastatic disease w/o BRAF mutation | A. Nivolumab 3mg/kg Q2wks. B. Dacarbazine 1000 mg/m2 Q3wks. | 418 A = 210 B = 208 | A. NR B. 10.8 (95% CI: 9.3–12.1 | A. 5.1 (95% CI: 3.5–10.8) B. 2.2 (95% CI: 2.1–2.4) (HR = 0.43, p < 0.001) | A. 40.0 (95% CI: 33.3–47.0) B. 13.9 (9.5–19.4) | A. 7.6 B. 1.0 | A. 11.7 B. 17.6 | -- |
| Postow et al. (2015) [128] CheckMate 069 | II | Metastatic melanoma with no prior treatment | A. Ipilimumab 3 mg/kg + nivolumab 1 mg/kg Q3wks followed by nivolumab 3 mg/kg Q2wks B. Ipilimumab 3 mg/kg + placebo Q3wks followed by placebo Q2wks | 142 A. 95 B. 47 | -- | A. Not reached B. 4.4 HR = 0.4, p < 0.001 | In BRAF wild-type group: A. 61 B. 11 p < 0.001 | In BRAF wild-type group: A. 16 B. 0 | A. 54% B. 20% | Approved in combination with ipilimumab for the treatment of BRAF V600 wild type unresectable or metastatic melanoma (October 2015) | |
| Weber et al. (2015) [51] CheckMate 037 | III | Metastatic disease | A. Nivolumab 3mg/kg B. Investigator’s choice of chemotherapy | 405A = 272 B = 133 | -- | A. 4.7 (95% CI: 2.3–6.5) B. 4.2 (95% CI: 2.1–6.3) (HR = 0.82) | A. 31.7 (95% CI: 23.5–40.8) B. 10.6 (95% CI: 3.5–23.1) | A. 3.3 B. 0.0 | A. 9.0 B. 31.0 | Unresectable or metastatic melanoma and disease progression following ipilimumab and, if BRAF V600 mutation positive, a BRAF inhibitor (December 2014, based on interim analysis). | |
| Larkin et al. (2015) [129] CheckMate 067 | III | Previously untreated, stage III (unresectable) or stage IV disease with known BRAF V600 mutation status | A: Nivolumab 1mg/kg + ipilimumab 3mg/kg Q3wks., followed by nivolumab 3mg/kg Q2wks. B: Nivolumab 3mg/kg + placebo Q2wks.C. Ipilimumab 2mg/kg + placebo Q3wks. | 945 A = 314 B = 316 C = 315 | -- | A. 11.5 (95% CI: 8.9–16.7) B. 6.9 (95% CI: 4.3–9.5) C. 2.9 (95% CI: 2.8–3.4) (HR = 0.42, p < 0.001 A vs. C; HR = 0.57, p < 0.001 B vs. C) | A. 57.6 (95% CI: 52.0–63.2) B. 43.7 (95% CI: 38.1–49.3) C. 19 (95% CI: 14.9–23.8) | A. 11.5 B. 8.9 C. 2.2 | A. 55.0 B. 16.3 C. 27.3 | Expanded indication: unresectable or metastatic melanoma regardless of BRAF V600 mutation status (January 2016) | |
| Weber et al. (2017) [146] CheckMate 238 | III | Completely resected, advanced disease | A. Nivolumab 3mg/kg Q2wks. B. Ipilimumab 10mg/kg Q3wks. | 906 A = 453 B = 453 | -- | 12-month PFS rate: A. 70.5% (95% CI: 66.1–74.5) B. 60.8% (95% CI: 56.0–65.2) (HR = 0.65, p < 0.001) | -- | -- | A. 14.4 B. 45.9 | Expanded indication: adjuvant treatment for melanoma with involvement of lymph nodes or in patients with metastatic disease who have undergone complete resection (December 2017) | |
| Mesothelioma | Scherpereel et al. (2019) [147] IFCT-1501 MAPS2 | II | Malignant pleural mesothelioma with progression after first- or second-line treatments | A. Nivolumab 3 mg/kg Q2wks B. Nivolumab 3 mg/kg Q2wks + ipilimumab 1 mg/kg Q6wks | 125 A = 63 B = 62 | A. 11.0 (95% CI: 6.7–17.7) B. 15.9 (95% CI: 10.7–NR) | A. 4.0 (95% CI: 2.8–5.7) B. 5.6 (95% CI: 3.1–8.3) | A. 19 (95% CI: 8–29) B. 28 (95% CI: 16–49) | -- | A. 14 B. 26 | -- |
| NSCLC | Rizvi et al. (2015) [148] CheckMate 063 | II | Advanced sqNSCLC | Nivolumab 3mg/kg Q2wks. | 117 | 8.2 (95% CI: 6.1–10.9) | 1.9 (95% CI: 1.8–3.2) | 14.5 (95% CI: 8.7–22.2) | 1.0 | 17.0 | -- |
| Brahmer et al. (2015) [52] CheckMate 017 | III | Advanced sqNSCLC | A. Nivolumab 3mg/kg Q2wks. B. Docetaxel 75mg/m2 Q3wks. | 272 A = 135 B = 137 | A. 9.2 (95% CI: 7.3–13.3) B. 6.0 (95% CI: 5.1–7.3) (HR = 0.59, p < 0.001) | A. 3.5 (95% CI: 2.1–4.9) B. 2.8 (95% CI: 2.1–3.5) (HR = 0.62, p < 0.001) | A. 20 (95% CI: 14–28) B. 9 (95% CI: 5–15) (p = 0.008) | A. 1.0 B. 0.0 | A. 7.0 B. 55.0 | Metastatic sqNSCLC with progression on or after platinum-based chemotherapy (March 2015) | |
| Borghaei et al. (2015) [53] CheckMate 057 | III | Stage IIIB, IV, or recurrent NsqNSCLC | A. Nivolumab 3mg/kg Q2wks. B. Docetaxel 75mg/m2 Q3wks. | 582 A = 292 B = 290 | A. 12.2 (95% CI: 9.7–15.0) B. 9.4 (95% CI: 8.1–10.7) (HR = 0.73, p = 0.002) | A. 2.3 (95% CI: 2.2–3.3) B. 4.2 (95% CI: 3.5–4.9) | A. 19 (95% CI: 15–24) B. 12 (95% CI: 9–17) (p = 0.02) | A. 1.0 B. <1.0 | A. 10.0 B. 54.0 | Expanded indication: Metastatic NSCLC (squamous or non-squamous) with progression on or after platinum-based therapy (October 2015) | |
| Carbone et al. (2017) [149] CheckMate 026 | III | Untreated stage IV or recurrent disease with PD-L1 expression ≥1% | A. Nivolumab 3mg/kg Q2wks. B. Investigator’s choice of platinum doublet chemotherapy | 541 A = 271 B = 270 | A. 14.4 (95% CI: 11.7-17.4) B. 13.2 (95% CI: 10.7-17.1) (HR = 1.02) | A. 4.2 (95% CI: 3.0-5.6) B. 5.9 (95% CI: 5.4-6.9) (HR = 1.15, p = 0.25) | A. 26 (95% CI: 20–33) B. 33 (95% CI: 27–40) | A. 2.0 B. <1.0 | A. 18 B. 51 | -- | |
| Vokes et al. (2018) [54] CheckMate017, CheckMate 057 | III | Advanced NSCLC (pooled analyses of CheckMate 017 and CheckMate 57) | A. Nivolumab 3mg/kg Q2wks. B. Docetaxel 75mg/m2 Q3wks. | Pooled 854 A = 427 B = 427 Liver mets A = 99 B = 94 | Pooled analysis:A. 11.1 (95% CI: 9.2–13.1) B. 8.1 (95% CI: 7.2–9.2) (HR = 0.70) Liver mets: A. 6.8 (95% CI: 4.9–10.4) B. 5.9 (95% CI: 4.7–7.3) (HR = 0.68) | Pooled analysis: A. 2.56 (95% CI: 2.20–3.48) B. 3.52 (95% CI: 3.15–4.21) (HR = 0.80) Liver mets: -- | Ongoing responses at minimum 3 yrs. follow up: A. 24 B. 0 | A. 4.0 B. 0.0 | Pooled analysis: A. 44 B. -- Liver mets: A. 8 B. -- | -- | |
| RCC | Motzer et al. (2015) [150] | II | Metastatic disease | A. Nivolumab 0.3mg/kg Q3wks. B. Nivolumab 2mg/kg Q3wks. C. Nivolumab 10mg/kg Q3wks. | 168 | A. 18.2 (80% CI: 16.2–24.0) B. 25.0 (80% CI: 19.8–28.8) C. 24.7 (95% CI: 15.3–26.0) (HR = 0.8 for B vs. A; HR = 0.9 for C vs. A) | A. 2.7 (80% CI: 1.9–3.0) B. 4.0 (80% CI: 2.8–4.2) C. 4.2 (80% CI: 2.8–5.5) | A. 20 (80% CI: 13.4–28.2) B. 22 (80% CI: 15.0–31.3) C. 20 (80% CI: 13.4–29.1) (p = 1.0) | A. 2.0 B. 2.0 C. 0.0 | A. 5 B. 17 C. 13 | -- |
| Motzer et al. (2015) [55] CheckMate 025 | III | Advanced disease | A. Nivolumab 3mg/kg Q2wks. B. Everolimus 10mg QD | 821 A = 410 B = 411 | A. 25.0 (95% CI: 21.7-NE) B. 19.6 (95% CI: 17.6–23.1) (HR = 0.73, p = 0.0018) | A. 4.6 (95% CI: 3.7–5.4) B. 4.4 (95% CI: 3.7–5.5) (HR = 0.88, p = 0.11) | A. 25 B. 5 (p < 0.001) | A. 1.0 B. <1.0 | A. 19.0 B. 37.0 | Advanced RCC with history of prior anti-angiogenic therapy (November 2015) | |
| Motzer et al. (2018) [39] CheckMate 214 | III | Advanced, untreated disease | A. Nivolumab 3mg/kg + ipilimumab 1mg/kg Q2wks. B. Sunitinib 50mg QD for 4 wks. | 1096 A = 550 B = 546 | A. NR (95% CI: 28.2–NE) B. 26.0 (95% CI: 22.1-NE) (HR = 0.63, p ≤ 0.001) | A. 11.6 (95% CI: 8.7–15.5) B. 8.4 (95% CI: 7.0–10.8) (HR = 0.82, p = 0.03) | A. 42 (95% CI: 37–47) B. 27 (95% CI: 22–31) (p < 0.001) | A. 9 B. 1 | A: 46 B: 63 | Expanded indication: Combination nivolumab/ipilimumab for intermediate- or poor-risk, previously untreated advanced RCC (April 2018) | |
| SCLC | Antonia et al. (2016) [56] CheckMate 032 | I/II | Limited-stage or extensive stage disease, after failing platinum-based chemotherapy and one other line of treatment | A. Nivolumab 3mg/kg Q2wks. B. Nivolumab 1mg/kg + ipilimumab 1mg/kg Q3wks. C. Nivolumab 1mg/kg + ipilimumab 3mg/kg Q3wks. D. Nivolumab 3 mg/kg + ipilimumab 1mg/kg Q3wks. | 216 A = 98 B = 3 C = 61 D = 54 | A. 4.4 (95% CI: 3.0–9.3) B. -- C. 4.4 (95% CI: 3.6–18.0) D. 6.0 (95% CI: 3.6–11.0) | A. 1.4 (95% CI: 1.4–1.9) B. -- C. 2.6 (95% CI: 1.4–4.1) D. 1.4 (1.3–2.2) | A. 10 (95% CI: 5–18) B. 33 (95% CI: 0.9–91.0) C. 23 (95% CI: 13–36) D. 19 (95% CI: 9–31) | A. 0.0 B. – C. 2.0 D. 0.0 | A. 13.0 B. 0.0 C. 30.0 D. 19.0 | Metastatic SCLC with progression after platinum-based chemotherapy and at least one other line of therapy (August 2018) |
| Cancer | Study | Phase | Stage of Disease | Treatment Regimen | N | Median OS (Months) | Median PFS (Months) | ORR (%) | CRR (%) | Grade III/IV AEs (%) | Resultant FDA-Approved Indication |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bladder cancer | Bellmunt et al. (2017) [151] KEYNOTE-045 | III | Metastatic urothelial carcinoma that recurred or progressed after platinum chemotherapy | A. Pembrolizumab 200mg Q3wks. B. Investigator’s choice of paclitaxel, docetaxel, or vinflunine Q3wks. | 542 A. 270 B. 272 | A. 10.3 B. 7.4 (HR = 0.73, p = 0.002) | A. 2.1 B. 3.3 (HR = 0.98, p = 0.42) | A. 21 B. 11 | -- | A. 15.0 B. 49.4 | Locally advanced or metastatic urothelial carcinoma with progression during or following platinum-containing chemotherapy or within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy (May 2017) |
| Balar et al. (2017) [152] KEYNOTE-052, with update from O’Donnell et al. (2019) [153] | II | Advanced urothelial carcinoma ineligible for platin | Pembrolizumab 200mg Q3wks. | 370 CPS < 10. 251 CPS ≥ 10. 110 | Combined: 11.3 CPS < 10: 9.7 CPS ≥ 10: 18.5 | Combined: 2 months | Combined: 28.4 CPS < 10: 20.0 CPS ≥ 10: 10.0 | Combined: 9.0 | 21 | Expanded indication: locally advanced or metastatic urothelial carcinoma who are not eligible for cisplatin-containing therapy and whose tumors express PD-L1 (CPS ≥ 10), or in patients who are not eligible for any platinum-containing chemotherapy regardless of PD-L1 status (June 2018) | |
| CSCC | Chung et al. (2019) [57] KEYNOTE-158 | II | Recurrent or metastatic advanced disease that has failed one or more lines of chemotherapy | Pembrolizumab 200mg Q3wks. | 98 CPS < 1. 16 CPS ≥ 1. 82 | Combined: 9.4 CPS ≥ 1: 11 | Combined: 2.1 CPS ≥ 1: 2.1 | Combined: 12.2 CPS < 1:1.0 CPS ≥ 1:14.6 | Combined: 3 | 12.2 | Second-line for recurrent or metastatic cervical cancer with CPS ≥ 1 (June 2018) |
| Endometrial Carcinoma | Makker et al. (2019) [94] KEYNOTE-146 | II | Metastatic endometrial cancer that had progressed following at least one prior systemic therapy | Pembrolizumab 200mg IV Q3wks + lenvatinib 20mg PO QD | 108, 94 of which were not MSI-H or dMMR | -- | -- | 38.3 | 10.6 | 52 | Approved in combination with lenvatinib for the treatment of patients with advanced endometrial carcinoma that is not MSI-H or dMMR, or who have disease progression following prior systemic therapy and are not candidates for curative surgery or radiation (September 2019) |
| Esophageal cancer | Shah et al. (2019) [154] KEYNOTE-180 | II | Advanced, metastatic esophageal cancer that progressed after 2 or more lines of therapy | Pembrolizumab 200mg Q3wks. | 121 ESCC. 63 EAC. 58 | ESCC: 6.8 EAC: 3.9 CPS < 10: 5.4 CPS ≥ 10: 6.4 (HR = 0.64) | ESCC: 2.1 EAC: 1.9 CPS < 10: 2.0 CPS ≥ 10: 2.0 (HR = 0.66) | ESCC: 14.3 EAC: 5.2 CPS < 10: 6.3 CPS ≥ 10: 13.8 | ESCC: 0.0 EAC: 0.0 | Combined: 11.60 | Recurrent locally advanced or metastatic squamous cell carcinoma of the esophagus whose tumors express PD-L1 (CPS ≥ 10) (July 2019) |
| Kojima et al. (2019) [155] KEYNOTE-181 | III | Locally advanced or metastatic disease | A. Pembrolizumab 200mg Q3wks. B. Investigator’s choice of paclitaxel, docetaxel, or irinotecan | 628 ESCC. 401 CPS ≥ 10. 222 | ESCC: A. 8.2 B. 7.1 (HR = 0.78, p = 0.0095) CPS ≥ 10: A. 9.3 B. 6.7 (HR = 0.69, p = 0.0074) | -- | -- | -- | A. 18 B. 41 | As above, with Shah et al. (2019) | |
| Gastric or GEJ adenocarcinoma | Fuchs et al. (2018) [58] KEYNOTE-059 | II | Gastric/GEJ adenocarcinoma previously treated with 2 or more systemic therapies including fluoropyrimidine and platinum, and HER2/neu if indicated | Pembrolizumab 200mg Q3wks. | 259 | 5.6 | 2.0 | Overall: 11.6 PD-L1+: 15.5 PD-L1-: 6.4 | 2.4 | 17.8 | Second-line therapy for patients with recurrent, locally advanced, or metastatic esophageal squamous cell carcinoma (September 2017) |
| HCC | Zhu et al. (2018) [62] KEYNOTE-224 | II | HCC with prior treatment with sorafenib | Pembrolizumab 200mg Q3wks. | 104 | 12.9 | 4.8 | 17 | 1 | 24 | Monotherapy for HCC that had been previously treated with sorafenib (November 2018) |
| HL | Chen et al. (2017) [63] KEYNOTE-087 | Recurrent or relapsed cHL | Pembrolizumab 200 mg Q3wks. in 3 cohorts: A. After ASCT and BV B. After salvage chemotherapy and BV C. After ASCT only | 210 A. 69 B. 81 C. 60 | NR 24-month OS rate: A. 92.5 B. 90.6 C. 89.4 | Overall: 13.7 A. 16.4 B. 11.1 C. 19.4 | Overall: 71.9 A. 76.8 B. 66.7 C. 73.3 | A. 26.1 B. 25.9 C. 31.7 | 11.9 | Refractory or relapsed cHL after three or more lines of prior therapy (March 2017) | |
| HNSCC | Seiwert et al. (2016) [59] KEYNOTE-012 | Ib | Recurrent or metastatic disease with PD-L1 positive status | Pembrolizumab 10mg/kg Q2wks. | 60 | 13 | 2 | 18 | 2 | 17 | Metastatic or recurrent HNSCC with disease progression on or after platinum therapy (August 2016) |
| Burtness et al. (2018) [61] KEYNOTE-048 | III | Locally incurable recurrent or metastatic disease and no prior systemic therapy | A. Pembrolizumab 200mg Q3wks. B. Pembrolizumab 200mg Q3wks. + 6 cycles of platinum therapy C. Cetuximab + 6 cycles of platinum + FU | 882 A. 301 B. 281 C. 300 | Overall: B. 11.5 C. 10.7 (HR = 0.83, p = 0.0199) CPS ≥ 20: B. 14.7 C. 11 (HR = 0.60, p = 0.0004) CPS ≥ 1: B. 13.6 C. 10.4 (HR = 0.65, p < 0.0001) | NR Overall: HR = 1.29 CPS ≥ 20: HR = 0.76, p = 0.5 No further PFS analysis done | Overall: B. 16.9 C. 36.0 CPS ≥ 20: B. 42.9 C. 38.2 CPS ≥ 1: B. 36.4 C. 35.7 | -- | A. 54.7 B. 85.1 C. 83.3 | -- | |
| Rischin et al. 2019 [156] (KEYNOTE-048 final analysis) | III | Locally incurable recurrent or metastatic disease and no prior systemic therapy | A. Pembrolizumab 200mg Q3wks. B. Pembrolizumab 200mg Q3wks. + 6 cycles of platinum therapy C. Cetuximab + 6 cycles of platinum + FU | 882 A. 301 B. 281 C. 300 | CPS ≥ 20: A. 14.9 C. 10.7 (HR = 0.61 p = 0.0015) CPS ≥ 1: A. 12.3 C. 10.3 (HR = 0.65, p < 0.0001) Overall B. 13.0 C. 10.7 (HR = 0.77, p = 0.0067) | CPS ≥ 20: A. 3.4 C. 5.0 (HR = 0.99) CPS ≥ 1: A. 3.2 C. 5.0 (HR = 1.15) Overall B. 4.9 C. 5.1 (HR = 0.92 p = 0.3394) | CPS ≥ 20: A. 23 C. 36 CPS ≥ 1: A. 19 C. 35 Overall B. 36 C. 36 | CPS ≥ 20: A. 8 C. 3 CPS ≥ 1: A. 5 C. 13 Overall B. 6 C. 3 | A. 54.7 B. 85.1 C. 83.3 | First line treatment of patients with metastatic or unresectable recurrent HNSCC, as monotherapy in patients whose tumors express PD-L1 or in combination with platinum and fluorouracil (June 2019) | |
| Cohen et al. (2019) [60] KEYNOTE-040 | III | Recurrent or metastatic disease | A. Pembrolizumab 10mg/kg Q3wks. B. Investigator’s choice of MTX, docetaxel, cetuximab | 495 A. 247 B. 248 | CPS ≥ 1: A. 8.7 B. 7.1 | A. 2.1 B. 2.3 (HR = 0.95, p = 0.030) | A. 14.6 B. 10.1 | -- | A. 13 B. 36 | Expanded indication: combination with platinum and fluorouracil (FU) as first-line treatment of metastatic or unresectable, recurrent HNSCC, and as single agent for patients whose tumors express PD-L1 and CPS ≥ 1 (June 2019) | |
| MCC | Nghiem et al. (2019) [69] KEYNOTE-017 | II | Recurrent locally advanced Merkel Cell Carcinoma or metastatic MCC with no prior therapy | Pembrolizumab 2mg/kg Q3wks. | 50 | NR | 16.8 | 56 | -- | 28 | Treatment of adult and pediatric patients with recurrent locally advanced or metastatic MCC (December 2018) |
| Melanoma | Robert et al. (2014) [65] KEYNOTE-001 | I | Unresectable or metastatic disease with progression following ipilimumab and, if BRAF V600 mutation positive, BRAF inhibitor | A. Pembrolizumab 2mg/kg Q3wks. B. Pembrolizumab 10mg/kg Q3wks. | 173 A. 89 B. 84 | 12-month survival rate: A. 58 B. 63 (HR = 1.09) | A. 5.1 B. 3.2 (HR = 0.84) | Combined: 26 A. 26 B. 26 (p = 0.96) | A. 1 B. 1 | Combined: 12 A. 15 B. 8 | Unresectable or metastatic melanoma with disease progression following ipilimumab and, if BRAF V600 mutation positive, BRAF inhibitor (September 2014) |
| Ribas et al. (2015) [66] KEYNOTE-002 | II | Advanced melanoma following ipilimumab and, if BRAF V600 positive, BRAF inhibitor | A. Pembrolizumab 2mg/kg Q3wks.B. Pembrolizumab 10mg/kg Q3wks.B. Investigator’s choice of paclitaxel + carboplatin, paclitaxel, carboplatin, dacarbazine, or temozolomide | 540 A. 180 B. 181 C. 179 | -- | A. 2.9 B. 2.9 C. 2.7 (HR = 0.57, p < 0.0001 A vs. C; HR = 0.50, p < 0.0001 B vs. C) | A. 38 B. 46 C. 8 | A. 2 B. 3 C. 0 | A. 11 B. 14 C. 26 | -- | |
| Robert et al. (2015) [67] KEYNOTE-006 | III | Stage III or IV melanoma with no more than 1 prior treatment | A. Pembrolizumab 10mg/kg Q2wks. B. Pembrolizumab 10mg/kg Q3wks.C. Ipilimumab 3mg/kg Q3wks. | 834 A. 279 B. 277 C. 278 | NR for all groups 12-month OS rate: A. 74.1 B. 68.1 C. 58.2 (HR = 0.63, p < 0.0005 A vs. C; HR = 0.69, p = 0.0036 B vs. C) | A. 5.5 B. 4.1 C. 2.8 (HR = 0.58, p < 0.001 A vs. C; HR = 0.58, p < 0.001 B vs. C) | A. 33.7 B. 32.9 C. 11.9 (p < 0.001 A vs. C; p < 0.001 B vs. C) | A. 5.0 B. 6.1 C. 1.4 | A. 13.3 B. 10.1 C. 19.9 | Expanded indication: first-line treatment of unresectable or metastatic melanoma (December 2015) | |
| Eggermont et al. (2018) [68] KEYNOTE-054 | III | Completely resected stage III disease | A. Pembrolizumab 200mg Q3wks. B. Placebo | 1019 A. 514 B. 505 | -- | Median recurrence-free survival A. NR B. 20.4 (HR = 0.57, p < 0.001) | Recurrence rate: A. 26 B. 43 | -- | A. 14.7 B. 3.4 | Expanded indication: adjuvant treatment of melanoma following complete resection (February 2019) | |
| MSI-H or dMMR | Le et al. (2018) [157] KEYNOTE-164 | II | Metastatic CRC with >2 prior treatments including FU, oxaliplatin, and irinotecan +/- anti-VEGF/EGFR mAb | Pembrolizumab 200mg Q3wks. | 61 | NR | 4.1 | 32 | 3.1 | 11 | Adult and pediatric patients with MSI-H or dMMR solid tumors that have progressed with no other treatment alternatives or colorectal cancer that has progressed after fluoropyrimidine, oxaliplatin, and irinotecan (May 2017) |
| KEYNOTE-016, 018, 028, 158 [70] | MSI-H/dMMR CRC, gastric, bladder, breast, biliary, endometrial, esophageal cancer | Pembrolizumab at varying doses | 149 CRC = 90 Other types = 59 | -- | -- | Combined: 39.6 CRC: 36 Other: 46 | 7.4 | -- | -- | ||
| NPC | Hsu et al. (2017) [158] KEYNOTE-028 | Ib | Unresectable or metastatic disease, failure on standard therapy, PD-L1 expression in 1% or more of tumor cells | Pembrolizumab 10 mg/kg Q2wks | 27 | 16.5 (95% CI: 10.1-NR) | 3.7 (95% CI: 2.1–13.4) | 25.9 (95% CI: 11.1–46.3) | 0 | 29.6 | -- |
| NSCLC | Garon et al. (2015) [64] KEYNOTE-001 | I | Advanced disease | A. Pembrolizumab 2mg/kg Q3wks. B. Pembrolizumab 10mg/kg Q3wks. C. Pembrolizumab 10mg/kg Q2wks. | 495 Prior treatment = 394 No prior treatment = 101 | Combined: 12.0 Prior treatment: 9.3 No prior treatment: 16.2 | Combined: 3.7 Prior treatment: 3.0 No prior treatment: 6.0 | Combined: 19.4 Prior treatment: 18.0 No prior treatment: 24.8 | -- | Combined: 9.5 | Metastatic NSCLC with PD-L1 expression and disease progression on or after platinum therapy; those with EGFR or ALK tumor mutations should have disease progression on FDA-approved therapy for these mutations prior to pembrolizumab (October 2015) |
| Reck et al. (2016) [159] KEYNOTE-024 interim analysis | III | Previously untreated NSCLC with TPS≥50% and no EGFR or ALK mutations | A. Pembrolizumab 200mg Q3wks B. Investigator’s choice platinum therapy | 305 A = 154 B = 151 | MOS not reached, overall survival greater in group A with HR = 0.6, p = 0.005) | A. 10.3 B. 6.0 (HR = 0.5, p < 0.001) | A. 44.8 B. 27.8 | -- | A. 26.6 B. 53.3 | First line therapy metastatic NSCLC with TPS>50% and no EGFR, ALK mutations (October 2016) | |
| Herbst et al. (2016) [160] KEYNOTE-010 | II/III | Previously treated metastatic NSCLC with TPS>1% | A. Pembrolizumab 2mg/kg Q3wks.B. Pembrolizumab 10mg/kg Q3wks.C. Docetaxel 75mg/m2 Q3wks. | 1034 A = 345 B = 346 C = 343 | A. 10.4 B. 12.7 C. 8.5 (HR = 0.71, p ≤ 0.001 A vs. C; HR = 0.61, p ≤ 0.001 B vs. C) | A. 3.9 B. 4.0 C. 4.0 (HR = 0.88, p = 0.068 A vs. C; HR = 0.79, p = 0.005 B vs. C) | A. 18 B. 19 C. 9 | -- | A. 13 B. 16 C. 35 | Expanded indication: second-line therapy for metastatic NSCLC with TPS >1% following disease progression on or after platinum chemotherapy (October 2016) | |
| Gandhi et al. (2018) [161] KEYNOTE-189 | III | Previously untreated metastatic NsqNSCLC without ALK or EGFR mutations | A. Pemetrexed and platinum-based therapy + pembrolizumab Q3wks.B. Placebo Q2wks. x 4 cycles, then pembrolizumab/placebo for up to 35 cycles + pemetrexed | 616 A = 405 B = 202 | A. NR B. 11.3 (HR = 0.49, p ≤ 0.0001) | A. 8.8 B. 4.8 (HR = 0.52, p ≤ 0.0001) | A. 47.6 B. 18.9 | A. 0.5 B. 0.5 | A. 67.2 B. 65.8 | Expanded indication: first-line therapy in combination with platinum-based chemotherapy and pemetrexed for metastatic NsqNSCLC without EGFR or ALK genomic aberrations (May 2018) | |
| Paz-Ares et al. (2018) [162] KEYNOTE-407 | III | Untreated metastatic squamous disease | A. Pembrolizumab 200mg + carboplatin + paclitaxel/nab-paclitaxel for first 4 cyclesB. saline placebo + carboplatin and paclitaxel or nab-paclitaxel for first 4 cycles | 559 A = 278 B = 281 | A. 15.9 B. 11.3 (HR = 0.64, p = 0.0017) | A. 6.4 B. 4.8 (HR = 0.56, p ≤ 0.0001) | A. 58 B. 35 | -- | A. 69.8 B. 68.2 | Expanded indication: first-line therapy in combination with carboplatin and paclitaxel/nab-paclitaxel for metastatic sqNSCLC (October 2018) | |
| Reck et al. (2019) [163] KEYNOTE-024 | III | Metastatic disease with TPS > 50% without ALK or EGFR mutations | A. Pembrolizumab 200mg Q3wks. B. Investigator’s choice of platinum-based chemo (platinum-based therapy + paclitaxel/pemetrexed/gemcitabine) | 305 A = 154 B = 151 | A. 30 B. 14.2 (HR = 0.60, p = 0.005) | A. 10.3 B. 6.0 (HR = 0.50, p ≤ 0.001) | A. 44.8 B. 27.8 | A. 4 B. 1 | A. 26.6 B. 53.3 | Expanded indication: first-line treatment for stage III/IV NSCLC that is not amenable to surgical resection or definitive chemoradiation with TPS ≥1% and without EGFR or ALK mutations (April 2019) | |
| PMBCL | Armand et al. (2018) [71] KEYNOTE-170 | II | Refractory or relapsed disease after or who were ineligible for ASCT w/ ≥2 lines of therapy | Pembrolizumab 200mg Q3wks. | 53 | NR | 5.5 | 45 | 11 | 26 | Approved as monotherapy in refractory or relapsed PMBCL after or who were ineligible for ASCT w/ ≥2 lines of therapy (June 2018) |
| RCC | Rini et al. (2019) [73] KEYNOTE-426 | I | Preciously untreated advanced disease | A. 200mg Pembrolizumab Q3wks. + axitinib 5mg BIDB. Sunitinib 50mg daily for first 4 weeks of each 6-week cycle | 861 A = 432 B = 423 | NR (HR = 0.53, p < 0.0001) | A. 15.1 B. 11.1 (HR = 0.69, p < 0.001) | A. 59.3 B. 35.7 (p < 0.001) | -- | A. 75.8 B. 70.6 | First-line therapy in combination with axitinib for patients with advanced RCC (April 2019) |
| SCLC | Ott et al. (2017) [164] KEYNOTE-028 | I | SCLC or other lung neuroendocrine tumor with PD-L1≥1% that has previously failed platinum therapy plus etoposide | Pembrolizumab 10mg/kg Q2wks. | 24 | 9.7 | 1.9 | 33.3 | 4.2 | 33 | -- |
| Chung et al. (2019) [165] KEYNOTE-158 | II | Unresectable or metastatic disease that has failed 2 prior lines of therapy | Pembrolizumab 200mg Q3wks. | 98 | 9.4 | 2.1 | 12.20 | 3 | 12.20 | Second-line therapy for SCLC or other lung neuroendocrine tumor that has failed previous platinum-based therapy and one other prior line of therapy (June 2019) |
| Therapy | Cancer | Study | Phase | Stage of Disease | Treatment Regimen | N | Median OS (months) | Median PFS (months) | ORR (%) | CRR (%) | Grade III/IV AEs (%) | Resultant FDA-Approved Indication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atezolizumab | Bladder cancer | Rosenberg et al. (2016) [74] IMvigor210 | II | Inoperable locally advanced or metastatic urothelial carcinoma | Atezolizumab 1200mg Q3wks. | 310 | 11.4 (95% CI: 9.0-NE) | 2.1 (95% CI: 2.1–2.1) | Overall: 15 (95% CI: 11–19) IC2/3: 26 (95% CI: 18–36) IC1/2/3: 18 (95% CI: 13–24) | 15 | 16 | Locally advanced or metastatic urothelial carcinoma with disease progression during or following platinum-containing chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum containing chemotherapy (May 2016) |
| Balar et al. (2017) [166] IMvigor210 | II | Locally advanced or metastatic urothelial carcinoma who were cisplatin ineligible | Atezolizumab 1200mg Q3wks. | 119 | 15.9 (95% CI: 9.0-NE) | 2.7 (95% CI: 2.1–4.2) | 23 (95% CI:16–31) | 9 | 19 | Expanded indication: first line treatment for locally advanced or metastatic urothelial carcinoma not eligible for cisplatin-containing chemotherapy or within 12 months of neoadjuvant or adjuvant chemotherapy (April 2017) | ||
| Powles et al. (2018) [75] IMvigor211 | III | Metastatic urothelial carcinoma with progression after platinum therapy | A. Atezolizumab 1200mg Q3wks. B. Investigator’s choice of vinflunine, paclitaxel, or docetaxel | 931 A = 467 B = 464 | A. 11.1 (95% CI: 8.6-15.5) B. 10.6 (95% CI: 8.4-12.2) (HR = 0.87, p = 0.412) | A. 2.1 (95% CI: 1.2–2.2) B. 4.0 (95% CI: 3.4–4.2) | A. 13.4 (95% CI: 10.5–16.9) B. 13.4 (95% CI: 10.5–16.9) | A. 3.0 B. 3.0 | A. 20 B. 43 | Expanded indication: locally advanced or metastatic urothelial carcinoma ineligible for cisplatin-containing therapy and tumor expressing PD-L1 in at least 5% of tumor area, or not eligible for platinum-containing therapy regardless of PD-L1 status (June 2018) | ||
| Breast cancer, triple-negative | Schmid et al. (2018) [76] IMpassion130 | III | Unresectable locally advanced TNBC | A. Atezolizumab 840mg Q2wks. + nab-paclitaxel 100mg/m2 on days 1, 8, and 15 of every 28-day cycle B. Placebo + nab-paclitaxel at dosing above | 902 A = 451 B = 451 | A. 21.3 B. 17.6 (HR = 0.84, p = 0.08) | A. 7.2 B. 5.5 (HR = 0.80, p = 0.002) | A. 56.0 (95% CI: 51.3–60.6) B. 45.9 (95% CI: 41.2–50.6) (p = 0.002) | A. 7.1 B. 1.6 | A. 48.7 B. 42.2 | Unresectable or metastatic TNBC with at least 1% tumor expression of PD-L1 (March 2019) | |
| Melanoma | Sullivan et al. (2019) [167] | Ib | BRAF V600 mutated metastatic disease | A. Atezolizumab + vemurafenib 720 mg BID B. Vemurafenib 960 mg BID x49d followed by vemurafenib 720 mg BID x7d, followed by vemurafenib + atezolizumab 720 mg BID C. Vemurafenib 960 mg BID x21d, followed by vemurafenib 720 mg BID x7d, followed by vemurafenib + atezolizumab 720 mg BID D. Vemurafenib 960 mg BID + cobimetinib 60 mg QD x21d, followed by vemurafenib 720 mg BID x7d, followed by vemurafenib + atezolizumab 720 mg BID + cobimetinib 60 mg QD | A. 3 B. 8 C. 6 D. 39 | A. 46.9 (95% CI: 2.8-NE) B. 46.2(95% CI: 10.7-NE) C. 33.2 (95% CI: 24.1-NE) D. NR (95% CI: NE) | A. 2.7(95% CI: 1.7–22.0) B. 9.3(95% CI: 3.8-NE) C. 14.1 (95% CI: 10.2–38.5) D. 12.9 (95% CI: 8.7–21.4) | A. 33.3 (95% CI: 0.8–90.6) B. 75.0 (95% CI: 34.9–96.8) C. 100 (95% CI: 54.1–100.0) D. 71.8 (95% CI: 55.1–85.0) | A. 33.3 (95% CI: 0.8–90.6) B. 12.5 (95% CI: 0.3–52.7) C. 16.7 (95% CI: 0.4–64.1) D. 20.5 (95% CI: 9.3–36.5) | A. 100 B. 87.5 C. 83.3 D. 66.7 | -- | |
| NSCLC | Fehrenbacher et al. (2016) [77] POPLAR | II | Previously treated advanced or metastatic disease | A. Atezolizumab 1200mg Q3wks. B. Docetaxel 75mg/m2 Q3wks. | 287 A = 144 B = 143 | A. 12.6 B. 9.7 (HR = 0.73) | A. 2.7 B. 3.0 (HR = 0.94, p = 0.645) | A. 17.0 (95% CI: 11.0–23.8) B. 15 (95% CI: 9.3–21.4) | -- | A. 11 B. 39 | Metastatic NSCLC that had progressed during or following platinum-based therapy (October 2016) | |
| Rittmeyer et al. (2017) [168] OAK | III | Previously treated stage IIIB or IV disease | A. Atezolizumab 1200mg Q3wks. B. Docetaxel 75mg/m2 Q3wks. | 850 A = 425 B = 425 | A. 13.8 (95% CI: 11.8–15.7) B. 9.6 (95% CI: 8.6–11.2) (HR = 0.74, p = 0.0004) | A. 2.8 (95% CI: 2.6–4.0) B. 4.0 (95% CI: 2.9–4.3) (HR = 0.91, p = 0.38) | A. 58 B. 57 | A. 1 B. <1 | A. 37 B. 54 | As above for Fehrenbacher et al. (2016) | ||
| Socinski et al. (2018) [78] IMpower150 | III | Metastatic NsqNSCLC without prior therapy | A. Atezolizumab 1200mg + bevacizumab 15mg/kg + paclitaxel 200mg/m2 (or 175mg/m2 for Asian patients) + carboplatin 6mg/mL/min B. Carboplatin + paclitaxel + bevacizumab at doses above | 800 A = 400 B = 400 | A. 19.2 B. 14.7 (HR = 0.78, p = 0.02) | A. 8.3 B. 6.8 (HR = 0.62, p < 0.001) | A. 63.5 (95% CI: 58.2–68.5) B. 48.0 (95% CI: 42.5–53.6) | A. 3.7 B. 1.2 | A. 55.7 B. 47.7 | Expanded indication: combination with bevacizumab, paclitaxel, and carboplatin for first-line treatment of metastatic NsqNSCLC without EGFR or ALK mutation (December 2018) | ||
| SCLC | Horn et al. (2018) [79] IMpower133 | III | Extensive stage SCLC without prior treatment | A. Atezolizumab 1200mg + carboplatin 5mg/mL/min + etoposide 100mg/m2 x4 cycles, then maintenance atezolizumab 1200mg Q3wks. B. Placebo + carboplatin + etoposide at doses above x4 cycles, then placebo afterward | 403 A = 201 B = 202 | A. 12.3 (95% CI: 10.8–15.9) B. 10.3 (95% CI: 9.3–11.3) (HR = 0.70, p = 0.0069) | A. 5.2 (95% CI: 4.4–5.6) B. 4.3 (95% CI: 4.2–5.4) (HR = 0.77, p = 0.0170) | A. 60.2 (95% CI: 53.1–67.0) B. 64.4 (95% CI: 57.3–71.0) | A. 2.5 B. 1.0 | A. 56.6 B. 56.1 | Combination with carboplatin and etoposide for first-line treatment in patients with extensive stage SCLC (March 2019) | |
| Avelumab | Bladder cancer | Apolo et al. (2017) [80] JAVELIN | Ib | Metastatic urothelial carcinoma refractory to at least 1 previous treatment | Avelumab 10mg/kg Q2wks. | 44 | 13.7 (95% CI: 8.5-NE) | 11.6 (95% CI: 6.1–17.4) | 18.2 (95% CI: 8.2–32.7) | 11.4 | 6.8 | Locally advanced or metastatic urothelial carcinoma with disease progression during or following platinum chemotherapy or within 12 months of neoadjuvant or adjuvant chemotherapy (May 2017) |
| MCC | Kaufman et al. (2016) [81] JAVELIN Merkel 200 | II | Stage IV, therapy refractory disease | Avelumab 10mg/kg Q2wks. | 88 | 11.3 (95% CI: 7.5–14.0) | 2.7 (95% CI: 1.4–6.9) | 31.8 (95% CI: 21.9–43.1) | 9 | 5 | Treatment of patients 12 years and older with metastatic MCC (March 2017) | |
| NSCLC | Barlesi et al. (2018) [169] JAVELIN Lung 200 | III | Stage IIIb/IV or recurrent disease with progression after treatment with a platinum-containing doublet | A. Avelumab 10 mg/kg Q2wks B. Docetaxel 75 mg/m2 Q3wks | 792 A = 396 B = 396 | A. 10.5 (95% CI: 9.2–12.9) B. 9.9 (95% CI: 8.1–11.8) HR = 0.90, p = 0.12 | A. 2.8 (95% CI: 2.7–3.5) B. 4.2 (95% CI: 3.3–5.2) HR = 1.16, p = 0.95 | A. 15 B. 11 Odds ratio=1.40, p = 0.055 | A. 1 B. 1 | A. 10 B. 49 | ||
| RCC | Motzer et al. (2019) [82] JAVELIN Renal 101 | III | Previously untreated disease | A. Avelumab 10mg/kg Q2wks. + axitinib 5mg BID B. Sunitinib 50mg QD | 886 A = 442 B = 444 | NR for both groups (HR = 0.78, p = 0.14) | A. 13.8 (95% CI: 11.1-NE) B. 7.2 (95% CI: 5.7-9.7) (HR = 0.61, p < 0.001) | Overall: A. 51.4 (95% CI: 46.6-56.1) B. 25.7 (95% CI: 21.7-30.0) PD-L1+: A. 55.2 (95% CI: 49.0–61.2) B. 25.5 (95% CI: 20.6–30.9) | Overall: A. 3.4 B. 1.8 PD-L1+: A. 4.4 B. 2.1 | A. 71.2 B. 71.5 | Combination with axitinib for first-line treatment for advanced RCC (May 2019) | |
| Durvalumab | Bladder cancer | Massard et al. (2016) [83] | I/II | Metastatic urothelial cancer | Durvalumab 10mg/kg Q2wks. | 61 | -- | -- | Overall: 31% (95% CI: 17.6–47.4) PD-L1 positive: 46.4% (95% CI: 27.5–66.1) PD-L1 negative: 0% (95% CI: 0.0–23.2) | -- | 4.9 | -- |
| Powles et al. (2017) [170] (updated results of previous study) | I/II | Metastatic Urothelial Cancer | Durvalumab 10mg/kg Q2wks. | 191 | Overall: 18.2 (95% CI: 8.1-NE) PD-L1 high: 20.0 (95% CI: 11.6-NE) PD-L1 low/-: 8.1 (95% CI: 3.1-NE) | Overall: 1.5 (95% CI: 1.4–1.9) PD-L1 high: 2.1 (95% CI: 1.4–2.8) PD-L1 low/-: 1.4 (95% CI: 1.3–1.5) | Overall: 17.8 (95% CI: 12.7-24.0) PD-L1 high: 27.6 (95% CI: 19–37.5) PD-L1 low/-: 5.1 (95% CI: 1.4–12.5) | Overall: 3.7 PD-L1 high: 4.1 PD-L1 low/-: 2.5 | 6.8 | Locally advanced or metastatic urothelial carcinoma with disease progression during or following platinum chemotherapy or progression within 12 months of neoadjuvant or adjuvant treatment with platinum therapy (May 2017) | ||
| Mesothelioma | Nowak et al. (2018) [171] DREAM | II | Radiation naive malignant pleural mesothelioma | Durvalumab 1125 mg + cisplatin 75 mg/m2 +pemetrexed 500 mg/m2 3-weekly x6 followed by durvalumab 1125 mg 3-weekly | 54 | -- | -- | 61 | -- | 57 | -- | |
| NSCLC | Antonia et al. (2017) [84] PACIFIC | Phase III | Stage III NSCLC who did not have progression after 2 or more cycles of platinum-based chemotherapy | A. Durvalumab 10mg/kg Q2wks. B. Placebo | 713 A = 473 B = 236 | Not done at time of study | A. 16.8 (95% CI: 13.0–18.1) B. 5.6 (95% CI: 4.6–7.8) (HR = 0.52, p < 0.001) | A. 28.4 (95% CI: 24.3–32.9) B. 16 (95% CI: 11.3–21.6) (p < 0.001) | A. 1.4 B. 0.5 | A. 29.9 B. 26.1 | Consolidation therapy for unresectable stage III NSCLC that has not progressed following concurrent platinum-based chemotherapy and radiation therapy |
| ClinicalTrial.gov Identifier | Year Opened | Drug(s) | Class | Phase | Estimated Enrollment | Disease | Arms/Interventions | Anticipated Completion |
|---|---|---|---|---|---|---|---|---|
| NCT01968109 | 2013 | 1. Relatlimab 2. Nivolumab | 1. Anti-LAG-3 2. Anti-PD-1 | I/IIa | 2000 | Advanced solid tumors | Relatlimab dose escalation and cohort expansion study alone or in combination with nivolumab | 2023 |
| NCT02060188 | 2014 | 1. Nivolumab 2. Ipilimumab 3. Cobimetinib 4. Daratumumab 5. Relatlimab | 1. Anti-PD-1 2. Anti-CTLA-4 3. MEK inhibitor 4. Anti-CD38 5. Anti-LAG3 | II | 340 | Recurrent and metastatic MSI-H and non-MSI-H colon cancer | Nivolumab alone or in combination with ipilimumab, cobimetinib, daratumumab, or relatlimab | 2020 |
| NCT02061761 | 2014 | 1. Relatlimab 2. Nivolumab | 1. Anti-LAG-3 2. Anti-PD-1 | I/IIa | 132 | Relapsed or refractory B-cell malignancies | Relatlimab alone or in combination with nivolumab | 2020 |
| NCT02488759 | 2015 | 1. Nivolumab 2. Ipilimumab 3. Relatlimab 4. Daratumumab | 1. Anti-PD-1 2. Anti-CTLA-4 3. Anti-LAG-3 4. Anti-CD38 | I/II | 600 | Virus-positive and virus-negative solid tumors | Nivolumab alone or in combination with ipilimumab, relatlimab, or daratumumab | 2019 |
| NCT02608268 | 2015 | 1. MBG453 2. Spartalizumab | 1. Anti-TIM-3 2. Anti-PD-1 | I | 250 | Advanced solid tumors | MPG453 alone or in combination with spartalizumab | 2019 |
| NCT02658981 | 2016 | 1. Relatlimab 2. Urelumab 3. Nivolumab | 1. Anti-LAG-3 2. Anti-CD137 3. Anti-PD-1 | I | 100 | Recurrent GBM | Relatlimab or urelumab alone or in combination with nivolumab | 2020 |
| NCT02750514 | 2016 | 1. Nivolumab 2. Ipilimumab 3. Relatlimab 4. Dasatinib 5. BMS-986205 | 1. Anti-PD-1 2. Anti-CTLA-4 3. Anti-LAG-3 4. TK inhibitor 5. Anti-IDO1 | II | 504 | Advanced NSCLC | Nivolumab alone or nivolumab + ipilimumab or nivolumab + relatlimab or nivolumab + dasatinib or nivolumab + BMS-986205 | 2021 |
| NCT02935634 | 2016 | 1. Nivolumab 2. Ipilimumab 3. Relatlimab 4. BMS-986205 | 1. Anti-PD-1 2. Anti-CTLA-4 3. Anti-LAG-3 4. Anti-IDO1 | II | 300 | Advanced gastric cancer | Nivolumab + ipilimumab or nivolumab + relatlimab or nivolumab + BMS-986205 | 2021 |
| NCT02996110 | 2016 | 1. Nivolumab 2. Ipilimumab 3. Relatlimab 4. BMS-986205 5. BMS-813160 | 1. Anti-PD-1 2. Anti-CTLA-4 3. Anti-LAG-3 4. Anti-IDO1 5. Anti-CCR2/CCR5 | II | 200 | Advanced RCC | Nivolumab + ipilimumab or nivolumab + relatlimab or nivolumab + BMS-986205 or nivolumab + BMS-813160 | 2022 |
| NCT03311412 | 2017 | 1. Sym021 2. Sym022 3. Sym023 | 1. Anti-PD-1 2. Anti-LAG-3 3. Anti-TIM-3 | I | 102 | Advanced solid tumors or lymphomas | Sym021 alone or in combination with either Sym022 or Sym023 | 2020 |
| NCT03219268 | 2017 | 1. MGD013 2. Margetuximab | 1. Dual anti-PD-1/LAG-3 2. Anti-HER2 | I | 255 | (A) Unresectable or metastatic solid neoplasms (B) HER2-positive breast cancer | (A) MGD013 dose escalation study (B) MGD013 in combination with margetuximab | 2022 |
| NCT03470922 | 2018 | 1. Nivolumab 2. Relatlimab | 1. Anti-PD-1 2. Anti-LAG-3 | II/III | 700 | Previously untreated or unresectable melanoma | Nivolumab alone or in combination with relatlimab | 2022 |
| NCT03440437 | 2018 | FS118 | Dual anti-PD-L1/LAG-3 | I | 51 | Advanced malignancies that progressed on or after PD-1/PD-L1 containing therapy | FS118 dose escalation and cohort expansion study | 2020 |
| NCT03623854 | 2018 | 1. Relatlimab 2. Nivolumab | 1. Anti-LAG-3 2. Anti-PD-1 | II | 20 | Advanced chordoma | Relatlimab in combination with nivolumab | 2022 |
| NCT03610711 | 2018 | 1. Nivolumab 2. Relatlimab | 1. Anti-PD-1 2. Anti-LAG-3 | I/II | 30 | Advanced esophagogastric cancer following targeted systemic radiation | Nivolumab alone or in combination with relatlimab | 2024 |
| NCT03743766 | 2018 | 1. Nivolumab 2. Relatlimab | 1. Anti-PD-1 2. Anti-LAG-3 | II | 42 | Metastatic melanoma naïve to prior immunotherapy | Nivolumab alone or relatlimab alone or combination nivolumab + relatlimab | 2022 |
| NCT03459222 | 2018 | 1. Relatlimab 2. Nivolumab 3. BMS-986205 4. Ipilimumab | 1. Anti-LAG-3 2. Anti-PD-1 3. Anti-IDO1 4. Anti-CTLA-4 | I/II | 230 | Advanced solid tumors | Relatlimab in combination with nivolumab + BMS-986205 or relatlimab in combination with nivolumab + ipilimumab | 2022 |
| NCT03744468 | 2018 | 1. BGB-A425 2. Tislelizumab | 1. Anti-TIM-3 2. Anti-PD-1 | I/II | 162 | Advanced solid tumors | BGB-A425 in combination with tislelizumab | 2021 |
| NCT03680508 | 2018 | 1. TSR-022 2. TSR-042 | 1. Anti-TIM-3 2. Anti-PD-1 | II | 42 | Advanced HCC | TSR-022 in combination with TSR-042 | 2022 |
| NCT03961971 | 2019 | 1. MBG453 2. Spartalizumab | 1. Anti-TIM-3 2. Anti-PD-1 | I | 15 | Recurrent GBM | MBG453 in combination with spartalizumab and stereotactic radiosurgery | 2023 |
| ClinicalTrial.Gov Identifier | Year Opened | Drug(s) | Class | Phase | Estimated Enrollment | Disease | Arms/Interventions | Anticipated Completion |
|---|---|---|---|---|---|---|---|---|
| NCT02304393 | 2014 | 1. Atezolizumab 2. Selicrelumab | 1. Anti-PD-L1 2. CD40 agonist | I | 142 | Advanced solid malignancies | Dose escalation of selicrelumab in combination with atezolizumab followed by dose expansion of dose expansion of selicrelumab in combination with atezolizumab | 2019 |
| NCT02665416 | 2016 | 1. Selicrelumab 2. Vanucizumab 3. Bevacizumab | 1. CD40 agonist 2. Anti-VEGF-A and Anti-Ang-2 3. Anti-VEGF-A | I/II | 170 | Advanced or metastatic solid tumors | Dose escalation of selicrelumab in combination with vanucizumab followed by dose expansion of selicrelumab in combination with bevacizumab | 2020 |
| NCT03092856 | 2017 | 1. Axitinib 2. PF-04518600 | 1. TK Inhibitor 2. OX40 agonist | II | 104 | Metastatic or recurrent RCC | Axitinib alone or in combination with PF-04518600 | 2021 |
| NCT02706353 | 2017 | 1. APX005M 2. Pembrolizumab | 1. CD40 agonist 2. Anti-PD-1 | I/II | 41 | Metastatic melanoma | Dose escalation of APX005M in combination with pembrolizumab followed by dose expansion of APX005M in combination with pembrolizumab | 2020 |
| NCT03217747 | 2017 | 1. Avelumab2. Utomilumab 3. PF-04518600 | 1. Anti-PD-L12. Anti-CD137 3. OX40 agonist | I/II | 184 | Advanced solid malignancies | Avelumab + utomilumab or avelumab + PF-04518600 or avelumab + utomilumab + PF-04518600 or avelumab + RT | 2023 |
| NCT03410901 | 2018 | 1. SD-101 2. BMS 986178 | 1. TLR9 Agonist 2. OX40 agonist | I | 15 | Advanced lymphomas | Combination SD-101 + BMS 986178 + RT | 2020 |
| NCT03389802 | 2018 | 1. APX005M | 1. CD40 agonist | I | 45 | Pediatric CNS tumors | Dose escalation of APX005M alone | 2022 |
| NCT03336606 | 2018 | 1. MEDI0562 | 1. OX40 agonist | I | 35 | HNSCC, melanoma | MEDI0562 at varying dose schedules prior to surgical resection | 2024 |
| NCT03892525 | 2019 | 1. Selicrelumab 2. Atezolizumab | 1. CD40 agonist 2. Anti-PD-L1 | I | 44 | Recurrent or refractory NHL | Intratumoral selicrelumab in combination with atezolizumab | 2023 |
| NCT03719430 | 2019 | 1. Doxorubicin 2. APX005M | 1. Anthracycline 2. CD40 agonist | II | 27 | Advanced soft tissue sarcoma | Combination doxorubicin + APX005M | 2023 |
References
- Brunet, J.-F.; Denizot, F.; Luciani, M.-F.; Roux-Dosseto, M.; Suzan, M.; Mattei, M.-G.; Golstein, P. A New Member of the Immunoglobulin Superfamily—CTLA-4. Nature 1987, 328, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of Antitumor Immunity by CTLA-4 Blockade. Available online: https://link-galegroup-com.ezproxy4.library.arizona.edu/apps/doc/A18175424/AONE?sid=lms (accessed on 11 August 2019).
- Boomer, J.S.; Green, J.M. An Enigmatic Tail of CD28 Signaling. Cold Spring Harb. Perspect. Biol. 2010, 2, a002436. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Chai, Y.; Qi, J.; Zhang, C.W.H.; Tong, Z.; Shi, Y.; Yan, J.; Tan, S.; Gao, G.F. Remarkably Similar CTLA-4 Binding Properties of Therapeutic Ipilimumab and Tremelimumab Antibodies. Oncotarget 2017, 8, 67129–67139. [Google Scholar] [CrossRef] [PubMed]
- Hargadon, K.M.; Johnson, C.E.; Williams, C.J. Immune Checkpoint Blockade Therapy for Cancer: An Overview of FDA-Approved Immune Checkpoint Inhibitors. Int. Immunopharmacol. 2018, 62, 29–39. [Google Scholar] [CrossRef]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG Subclasses and Allotypes: From Structure to Effector Functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef]
- Simpson, T.R.; Li, F.; Montalvo-Ortiz, W.; Sepulveda, M.A.; Bergerhoff, K.; Arce, F.; Roddie, C.; Henry, J.Y.; Yagita, H.; Wolchok, J.D.; et al. Fc-Dependent Depletion of Tumor-Infiltrating Regulatory T Cells Co-Defines the Efficacy of Anti-CTLA-4 Therapy against Melanoma. J. Exp. Med. 2013, 210, 1695–1710. [Google Scholar] [CrossRef]
- Selby, M.J.; Engelhardt, J.J.; Quigley, M.; Henning, K.A.; Chen, T.; Srinivasan, M.; Korman, A.J. Anti-CTLA-4 Antibodies of IgG2a Isotype Enhance Antitumor Activity through Reduction of Intratumoral Regulatory T Cells. Cancer Immunol. Res. 2013, 1, 32–42. [Google Scholar] [CrossRef]
- Du, X.; Tang, F.; Liu, M.; Su, J.; Zhang, Y.; Wu, W.; Devenport, M.; Lazarski, C.A.; Zhang, P.; Wang, X.; et al. A Reappraisal of CTLA-4 Checkpoint Blockade in Cancer Immunotherapy. Cell Res. 2018, 28, 416–432. [Google Scholar] [CrossRef]
- Arce Vargas, F.; Furness, A.J.S.; Litchfield, K.; Joshi, K.; Rosenthal, R.; Ghorani, E.; Solomon, I.; Lesko, M.H.; Ruef, N.; Roddie, C.; et al. Fc Effector Function Contributes to the Activity of Human Anti-CTLA-4 Antibodies. Cancer Cell 2018, 33, 649–663.e4. [Google Scholar] [CrossRef]
- Kavanagh, B.; O’Brien, S.; Lee, D.; Hou, Y.; Weinberg, V.; Rini, B.; Allison, J.P.; Small, E.J.; Fong, L. CTLA4 Blockade Expands FoxP3+ Regulatory and Activated Effector CD4+ T Cells in a Dose-Dependent Fashion. Blood 2008, 112, 1175–1183. [Google Scholar] [CrossRef]
- Retseck, J.; VanderWeele, R.; Lin, H.-M.; Lin, Y.; Butterfield, L.H.; Tarhini, A.A. Phenotypic and Functional Testing of Circulating Regulatory T Cells in Advanced Melanoma Patients Treated with Neoadjuvant Ipilimumab. J. Immunother. Cancer 2016, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Comin-Anduix, B.; Economou, J.S.; Donahue, T.R.; De La Rocha, P.; Morris, L.F.; Jalil, J.; Dissette, V.B.; Shintaku, I.P.; Glaspy, J.A.; et al. Intratumoral Immune Cell Infiltrates, FoxP3, and Indoleamine 2,3-Dioxygenase in Patients with Melanoma Undergoing CTLA4 Blockade. Clin. Cancer Res. 2009, 15, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Subudhi, S.K.; Blando, J.; Scutti, J.; Vence, L.; Wargo, J.A.; Allison, J.P.; Ribas, A.; Sharma, P. Anti-CTLA-4 Immunotherapy Does Not Deplete FOXP3+ Regulatory T Cells (Tregs) in Human Cancers. Clin. Cancer Res. 2018, 25, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Agata, Y.; Shibahara, K.; Honjo, T. Induced Expression of PD-1, a Novel Member of the Immunoglobulin Gene Superfamily, upon Programmed Cell Death. EMBO J. 1992, 11, 3887–3895. [Google Scholar] [CrossRef] [PubMed]
- Agata, Y.; Kawasaki, A.; Nishimura, H.; Ishida, Y.; Tsubata, T.; Yagita, H.; Honjo, T. Expression of the PD-1 Antigen on the Surface of Stimulated Mouse T and B Lymphocytes. Int. Immunol. 1996, 8, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Callahan, M.K.; Wolchok, J.D. Immune Checkpoint Blockade in Cancer Therapy. J. Clin. Oncol. 2015, 33, 1974–1982. [Google Scholar] [CrossRef] [Green Version]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef]
- Zhang, N.; Tu, J.; Wang, X.; Chu, Q. Programmed Cell Death-1/Programmed Cell Death Ligand-1 Checkpoint Inhibitors: Differences in Mechanism of Action. Immunotherapy 2019, 11, 429–441. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, H.T.; Shin, W.; Chae, J.; Choi, J.; Kim, S.H.; Lim, H.; Won Heo, T.; Park, K.Y.; Lee, Y.J.; et al. Structural Basis of Checkpoint Blockade by Monoclonal Antibodies in Cancer Immunotherapy. Nat. Commun. 2016, 7. [Google Scholar] [CrossRef]
- Flies, D.B.; Chen, L. The New B7s: Playing a Pivotal Role in Tumor Immunity. J. Immunother. 2007, 30, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.T.; Lee, J.Y.; Lim, H.; Lee, S.H.; Moon, Y.J.; Pyo, H.J.; Ryu, S.E.; Shin, W.; Heo, Y.-S. Molecular Mechanism of PD-1/PD-L1 Blockade via Anti-PD-L1 Antibodies Atezolizumab and Durvalumab. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Bono, P.; Bhatia, S.; Melero, I.; Nyakas, M.S.; Svane, I.-M.; Larkin, J.; Gomez-Roca, C.; Schadendorf, D.; Dummer, R.; et al. LBA18Efficacy of BMS-986016, a Monoclonal Antibody That Targets Lymphocyte Activation Gene-3 (LAG-3), in Combination with Nivolumab in Pts with Melanoma Who Progressed during Prior Anti–PD-1/PD-L1 Therapy (Mel Prior IO) in All-Comer and Biomarker-Enriched Populations. Ann. Oncol. 2017, 28 (Suppl. 5). [Google Scholar] [CrossRef]
- Triebel, F.; Jitsukawa, S.; Baixeras, E.; Roman-Roman, S.; Genevee, C.; Viegas-Pequignot, E.; Hercend, T. LAG-3, a Novel Lymphocyte Activation Gene Closely Related to CD4. J. Exp. Med. 1990, 171, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Huard, B.; Tournier, M.; Hercend, T.; Triebel, F.; Faure, F. Lymphocyte-Activation Gene 3/Major Histocompatibility Complex Class II Interaction Modulates the Antigenic Response of CD4+ T Lymphocytes. Eur. J. Immunol. 1994, 24, 3216–3221. [Google Scholar] [CrossRef]
- Long, L.; Zhang, X.; Chen, F.; Pan, Q.; Phiphatwatchara, P.; Zeng, Y.; Chen, H. The Promising Immune Checkpoint LAG-3: From Tumor Microenvironment to Cancer Immunotherapy. Genes Cancer 2018, 9, 176–189. [Google Scholar] [CrossRef]
- Andrews, L.P.; Marciscano, A.E.; Drake, C.G.; Vignali, D.A.A. LAG3 (CD223) as a Cancer Immunotherapy Target. Immunol. Rev. 2017, 276, 80–96. [Google Scholar] [CrossRef]
- Patel, J.; Bozeman, E.N.; Selvaraj, P. Taming Dendritic Cells with TIM-3: Another Immunosuppressive Strategy Used by Tumors. Immunotherapy 2012, 4, 1795–1798. [Google Scholar] [CrossRef]
- He, Y.; Cao, J.; Zhao, C.; Li, X.; Zhou, C.; Hirsch, F.R. TIM-3, a Promising Target for Cancer Immunotherapy. OncoTargets Ther. 2018, 11, 7005–7009. [Google Scholar] [CrossRef]
- Vonderheide, R.H. The Immune Revolution: A Case for Priming, Not Checkpoint. Cancer Cell 2018, 33, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Dempke, W.C.M.; Fenchel, K.; Uciechowski, P.; Dale, S.P. Second- and Third-Generation Drugs for Immuno-Oncology Treatment-The More the Better? Eur. J. Cancer 2017, 74, 55–72. [Google Scholar] [CrossRef] [PubMed]
- van Kooten, C.; Banchereau, J. CD40-CD40 Ligand. J. Leukoc. Biol. 2000, 67, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Piechutta, M.; Berghoff, A.S. New Emerging Targets in Cancer Immunotherapy: The Role of Cluster of Differentiation 40 (CD40/TNFR5). ESMO Open 2019, 4 (Suppl. 3), e000510. [Google Scholar] [CrossRef] [PubMed]
- Sugamura, K.; Ishii, N.; Weinberg, A.D. Therapeutic Targeting of the Effector T-Cell Co-Stimulatory Molecule OX40. Nat. Rev. Immunol. 2004, 4, 420–431. [Google Scholar] [CrossRef]
- Willoughby, J.; Griffiths, J.; Tews, I.; Cragg, M.S. OX40: Structure and Function - What Questions Remain? Mol. Immunol. 2017, 83, 13–22. [Google Scholar] [CrossRef]
- So, T.; Song, J.; Sugie, K.; Altman, A.; Croft, M. Signals from OX40 Regulate Nuclear Factor of Activated T Cells C1 and T Cell Helper 2 Lineage Commitment. Proc. Natl. Acad. Sci. USA 2006, 103, 3740–3745. [Google Scholar] [CrossRef]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Motzer, R.J.; Rini, B.I.; McDermott, D.F.; Frontera, O.A.; Hammers, H.J.; Carducci, M.A.; Salman, P.; Escudier, B.; Beuselinck, B.; Amin, A.; et al. Nivolumab plus Ipilimumab versus Sunitinib in First-Line Treatment for Advanced Renal Cell Carcinoma: Extended Follow-up of Efficacy and Safety Results from a Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2019. [Google Scholar] [CrossRef]
- Lynch, T.J.; Bondarenko, I.; Luft, A.; Serwatowski, P.; Barlesi, F.; Chacko, R.; Sebastian, M.; Neal, J.; Lu, H.; Cuillerot, J.-M.; et al. Ipilimumab in Combination with Paclitaxel and Carboplatin as First-Line Treatment in Stage IIIB/IV Non–Small-Cell Lung Cancer: Results From a Randomized, Double-Blind, Multicenter Phase II Study. J. Clin. Oncol. 2012, 30, 2046–2054. [Google Scholar] [CrossRef]
- Govindan, R.; Szczesna, A.; Ahn, M.-J.; Schneider, C.-P.; Gonzalez Mella, P.F.; Barlesi, F.; Han, B.; Ganea, D.E.; Von Pawel, J.; Vladimirov, V.; et al. Phase III Trial of Ipilimumab Combined with Paclitaxel and Carboplatin in Advanced Squamous Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2017, 35, 3449–3457. [Google Scholar] [CrossRef] [PubMed]
- Maio, M.; Scherpereel, A.; Calabrò, L.; Aerts, J.; Cedres Perez, S.; Bearz, A.; Nackaerts, K.; Fennell, D.A.; Kowalski, D.; Tsao, A.S.; et al. Tremelimumab as Second-Line or Third-Line Treatment in Relapsed Malignant Mesothelioma (DETERMINE): A Multicentre, International, Randomised, Double-Blind, Placebo-Controlled Phase 2b Trial. Lancet Oncol. 2017, 18, 1261–1273. [Google Scholar] [CrossRef]
- Sharma, P.; Retz, M.; Siefker-Radtke, A.; Baron, A.; Necchi, A.; Bedke, J.; Plimack, E.R.; Vaena, D.; Grimm, M.-O.; Bracarda, S.; et al. Nivolumab in Metastatic Urothelial Carcinoma after Platinum Therapy (CheckMate 275): A Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2017, 18, 312–322. [Google Scholar] [CrossRef]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.-J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in Patients with Metastatic DNA Mismatch Repair-Deficient or Microsatellite Instability-High Colorectal Cancer (CheckMate 142): An Open-Label, Multicentre, Phase 2 Study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in Patients with Advanced Hepatocellular Carcinoma (CheckMate 040): An Open-Label, Non-Comparative, Phase 1/2 Dose Escalation and Expansion Trial. Lancet Lond. Engl. 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Green, M.R.; Monti, S.; Rodig, S.J.; Juszczynski, P.; Currie, T.; O’Donnell, E.; Chapuy, B.; Takeyama, K.; Neuberg, D.; Golub, T.R.; et al. Integrative Analysis Reveals Selective 9p24.1 Amplification, Increased PD-1 Ligand Expression, and Further Induction via JAK2 in Nodular Sclerosing Hodgkin Lymphoma and Primary Mediastinal Large B-Cell Lymphoma. Blood 2010, 116, 3268–3277. [Google Scholar] [CrossRef]
- Ansell, S.M.; Lesokhin, A.M.; Borrello, I.; Halwani, A.; Scott, E.C.; Gutierrez, M.; Schuster, S.J.; Millenson, M.M.; Cattry, D.; Freeman, G.J.; et al. PD-1 Blockade with Nivolumab in Relapsed or Refractory Hodgkin’s Lymphoma. N. Engl. J. Med. 2015, 372, 311–319. [Google Scholar] [CrossRef]
- Younes, A.; Santoro, A.; Shipp, M.; Zinzani, P.L.; Timmerman, J.M.; Ansell, S.; Armand, P.; Fanale, M.; Ratanatharathorn, V.; Kuruvilla, J.; et al. Nivolumab for Classical Hodgkin’s Lymphoma after Failure of Both Autologous Stem-Cell Transplantation and Brentuximab Vedotin: A Multicentre, Multicohort, Single-Arm Phase 2 Trial. Lancet Oncol. 2016, 17, 1283–1294. [Google Scholar] [CrossRef]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.I.; Miller, W.H.; Lao, C.D.; et al. Nivolumab versus Chemotherapy in Patients with Advanced Melanoma Who Progressed after Anti-CTLA-4 Treatment (CheckMate 037): A Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Vokes, E.E.; Ready, N.; Felip, E.; Horn, L.; Burgio, M.A.; Antonia, S.J.; Frontera, O.A.; Gettinger, S.; Holgado, E.; Spigel, D.; et al. Nivolumab versus Docetaxel in Previously Treated Advanced Non-Small-Cell Lung Cancer (CheckMate 017 and CheckMate 057): 3-Year Update and Outcomes in Patients with Liver Metastases. Ann. Oncol. 2018, 29, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; López-Martin, J.A.; Bendell, J.; Ott, P.A.; Taylor, M.; Eder, J.P.; Jäger, D.; Pietanza, M.C.; Le, D.T.; De Braud, F.; et al. Nivolumab Alone and Nivolumab plus Ipilimumab in Recurrent Small-Cell Lung Cancer (CheckMate 032): A Multicentre, Open-Label, Phase 1/2 Trial. Lancet Oncol. 2016, 17, 883–895. [Google Scholar] [CrossRef]
- Chung, H.C.; Ros, W.; Delord, J.-P.; Perets, R.; Italiano, A.; Shapira-Frommer, R.; Manzuk, L.; Piha-Paul, S.A.; Xu, L.; Zeigenfuss, S.; et al. Efficacy and Safety of Pembrolizumab in Previously Treated Advanced Cervical Cancer: Results from the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2019, 37, 1470–1478. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.-P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients with Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and Clinical Activity of Pembrolizumab for Treatment of Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck (KEYNOTE-012): An Open-Label, Multicentre, Phase 1b Trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Soulières, D.; Tourneau, C.L.; Dinis, J.; Licitra, L.; Ahn, M.-J.; Soria, A.; Machiels, J.-P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus Methotrexate, Docetaxel, or Cetuximab for Recurrent or Metastatic Head-and-Neck Squamous Cell Carcinoma (KEYNOTE-040): A Randomised, Open-Label, Phase 3 Study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; De Castro, G.; Psyrri, A.; Baste Rotllan, N.; Neupane, P.C.; Bratland, Å.; et al. LBA8_PRKEYNOTE-048: Phase III Study of First-Line Pembrolizumab (P) for Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma (R/M HNSCC). Ann. Oncol. 2018, 29 (Suppl. 8). [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in Patients with Advanced Hepatocellular Carcinoma Previously Treated with Sorafenib (KEYNOTE-224): A Non-Randomised, Open-Label Phase 2 Trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Chen, R.; Zinzani, P.L.; Fanale, M.A.; Armand, P.; Johnson, N.A.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; et al. Phase II Study of the Efficacy and Safety of Pembrolizumab for Relapsed/Refractory Classic Hodgkin Lymphoma. J. Clin. Oncol. 2017, 35, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Wolchok, J.D.; Hodi, F.S.; Hamid, O.; Kefford, R.; Weber, J.S.; Joshua, A.M.; Hwu, W.-J.; Gangadhar, T.C.; et al. Anti-Programmed-Death-Receptor-1 Treatment with Pembrolizumab in Ipilimumab-Refractory Advanced Melanoma: A Randomised Dose-Comparison Cohort of a Phase 1 Trial. Lancet Lond. Engl. 2014, 384, 1109–1117. [Google Scholar] [CrossRef]
- Ribas, A.; Puzanov, I.; Dummer, R.; Schadendorf, D.; Hamid, O.; Robert, C.; Hodi, F.S.; Schachter, J.; Pavlick, A.C.; Lewis, K.D.; et al. Pembrolizumab versus Investigator-Choice Chemotherapy for Ipilimumab-Refractory Melanoma (KEYNOTE-002): A Randomised, Controlled, Phase 2 Trial. Lancet Oncol. 2015, 16, 908–918. [Google Scholar] [CrossRef]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef]
- Nghiem, P.; Bhatia, S.; Lipson, E.J.; Sharfman, W.H.; Kudchadkar, R.R.; Brohl, A.S.; Friedlander, P.A.; Daud, A.; Kluger, H.M.; Reddy, S.A.; et al. Durable Tumor Regression and Overall Survival in Patients with Advanced Merkel Cell Carcinoma Receiving Pembrolizumab as First-Line Therapy. J. Clin. Oncol. 2019, 37, 693–702. [Google Scholar] [CrossRef]
- Pembrolizumab in MSI-H or dMMR Solid Tumors: ‘First Tissue/Site-Agnostic’ Approval by FDA - The ASCO Post. Available online: https://www.ascopost.com/issues/february-10-2018/pembrolizumab-in-msi-h-or-dmmr-solid-tumors-first-tissuesite-agnostic-approval-by-fda/ (accessed on 11 August 2019).
- Armand, P.; Rodig, S.J.; Melnichenko, V.; Thieblemont, C.; Bouabdallah, K.; Tumyan, G.; Özcan, M.; Portino, S.; Fogliatto, L.; Caballero, D.; et al. Pembrolizumab in Patients with Relapsed or Refractory Primary Mediastinal Large B-Cell Lymphoma (PMBCL): Data from the Keynote-013 and Keynote-170 Studies. Blood 2018, 132 (Suppl. 1), 228. [Google Scholar] [CrossRef]
- Atkins, M.B.; Plimack, E.R.; Puzanov, I.; Fishman, M.N.; McDermott, D.F.; Cho, D.C.; Vaishampayan, U.; George, S.; Olencki, T.E.; Tarazi, J.C.; et al. Axitinib in Combination with Pembrolizumab in Patients with Advanced Renal Cell Cancer: A Non-Randomised, Open-Label, Dose-Finding, and Dose-Expansion Phase 1b Trial. Lancet Oncol. 2018, 19, 405–415. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in Patients with Locally Advanced and Metastatic Urothelial Carcinoma Who Have Progressed Following Treatment with Platinum-Based Chemotherapy: A Single-Arm, Multicentre, Phase 2 Trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus Chemotherapy in Patients with Platinum-Treated Locally Advanced or Metastatic Urothelial Carcinoma (IMvigor211): A Multicentre, Open-Label, Phase 3 Randomised Controlled Trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus Docetaxel for Patients with Previously Treated Non-Small-Cell Lung Cancer (POPLAR): A Multicentre, Open-Label, Phase 2 Randomised Controlled Trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Apolo, A.B.; Infante, J.R.; Balmanoukian, A.; Patel, M.R.; Wang, D.; Kelly, K.; Mega, A.E.; Britten, C.D.; Ravaud, A.; Mita, A.C.; et al. Avelumab, an Anti–Programmed Death-Ligand 1 Antibody, In Patients with Refractory Metastatic Urothelial Carcinoma: Results from a Multicenter, Phase Ib Study. J. Clin. Oncol. 2017, 35, 2117–2124. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Russell, J.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbé, C.; Linette, G.P.; Milella, M.; et al. Avelumab in Patients with Chemotherapy-Refractory Metastatic Merkel Cell Carcinoma: A Multicentre, Single-Group, Open-Label, Phase 2 Trial. Lancet Oncol. 2016, 17, 1374–1385. [Google Scholar] [CrossRef]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Massard, C.; Gordon, M.S.; Sharma, S.; Rafii, S.; Wainberg, Z.A.; Luke, J.; Curiel, T.J.; Colon-Otero, G.; Hamid, O.; Sanborn, R.E.; et al. Safety and Efficacy of Durvalumab (MEDI4736), an Anti–Programmed Cell Death Ligand-1 Immune Checkpoint Inhibitor, in Patients with Advanced Urothelial Bladder Cancer. J. Clin. Oncol. 2016, 34, 3119–3125. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Ye, X.; Piotrowski, A.F.; Desai, A.S.; Ahluwalia, M.S.; Walbert, T.; Fisher, J.D.; Desideri, S.; Belcaid, Z.; Jackson, C.; et al. Updated Phase I Trial of Anti-LAG-3 or Anti-CD137 Alone and in Combination with Anti-PD-1 in Patients with Recurrent GBM. J. Clin. Oncol. 2019, 37 (Suppl. 15), 2017. [Google Scholar] [CrossRef]
- Kluger, H.; Weiss, S.A.; Olszanski, A.J.; Schuchter, L.; Linette, G.P.; Garland, L.; Iannotti, N.O.; Johnson, M.; Avsar, E.; Srivastava, M.K.; et al. Abstract CT089: Phase Ib/II of CD40 Agonistic Antibody APX005M in Combination with Nivolumab (Nivo) in Subjects with Metastatic Melanoma (M) or Non-Small Cell Lung Cancer (NSCLC). Cancer Res. 2019, 79 (Suppl. 13), CT089. [Google Scholar] [CrossRef]
- O’Hara, M.H.; O’Reilly, E.M.; Rosemarie, M.; Varadhachary, G.; Wainberg, Z.A.; Ko, A.; Fisher, G.A.; Rahma, O.; Lyman, J.P.; Cabanski, C.R.; et al. Abstract CT004: A Phase Ib Study of CD40 Agonistic Monoclonal Antibody APX005M Together with Gemcitabine (Gem) and Nab-Paclitaxel (NP) with or without Nivolumab (Nivo) in Untreated Metastatic Ductal Pancreatic Adenocarcinoma (PDAC) Patients. Cancer Res. 2019, 79 (Suppl. 13), CT004. [Google Scholar] [CrossRef]
- Bajor, D.L.; Mick, R.; Riese, M.J.; Richman, L.P.; Xu, X.; Torigian, D.A.; Stelekati, E.; Sweeney, M.; Sullivan, B.; Schuchter, L.M.; et al. Abstract CT137: Combination of Agonistic CD40 Monoclonal Antibody CP-870,893 and Anti-CTLA-4 Antibody Tremelimumab in Patients with Metastatic Melanoma. Cancer Res. 2015, 75 (Suppl. 15), CT137. [Google Scholar] [CrossRef]
- Beatty, G.L.; Torigian, D.A.; Chiorean, E.G.; Saboury, B.; Brothers, A.; Alavi, A.; Troxel, A.B.; Sun, W.; Teitelbaum, U.R.; Vonderheide, R.H.; et al. A Phase I Study of an Agonist CD40 Monoclonal Antibody (CP-870,893) in Combination with Gemcitabine in Patients with Advanced Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2013, 19, 6286–6295. [Google Scholar] [CrossRef] [Green Version]
- Linch, S.N.; McNamara, M.J.; Redmond, W.L. OX40 Agonists and Combination Immunotherapy: Putting the Pedal to the Metal. Front. Oncol. 2015, 5, 34. [Google Scholar] [CrossRef]
- Redmond, W.L.; Linch, S.N.; Kasiewicz, M.J. Combined Targeting of Costimulatory (OX40) and Coinhibitory (CTLA-4) Pathways Elicits Potent Effector T Cells Capable of Driving Robust Antitumor Immunity. Cancer Immunol. Res. 2014, 2, 142–153. [Google Scholar] [CrossRef]
- Curti, B.D.; Kovacsovics-Bankowski, M.; Morris, N.; Walker, E.; Chisholm, L.; Floyd, K.; Walker, J.; Gonzalez, I.; Meeuwsen, T.; Fox, B.A.; et al. OX40 Is a Potent Immune Stimulating Target in Late Stage Cancer Patients. Cancer Res. 2013, 73, 7189–7198. [Google Scholar] [CrossRef]
- Tang, J.; Yu, J.X.; Hubbard-Lucey, V.M.; Neftelinov, S.T.; Hodge, J.P.; Lin, Y. Trial Watch: The Clinical Trial Landscape for PD1/PDL1 Immune Checkpoint Inhibitors. Nat. Rev. Drug Discov. 2018, 17, 854–855. [Google Scholar] [CrossRef] [PubMed]
- Makker, V.; Rasco, D.; Vogelzang, N.J.; Brose, M.S.; Cohn, A.L.; Mier, J.; Di Simone, C.; Hyman, D.M.; Stepan, D.E.; Dutcus, C.E.; et al. Lenvatinib plus Pembrolizumab in Patients with Advanced Endometrial Cancer: An Interim Analysis of a Multicentre, Open-Label, Single-Arm, Phase 2 Trial. Lancet Oncol. 2019, 20, 711–718. [Google Scholar] [CrossRef]
- Pitt, J.M.; Vétizou, M.; Daillère, R.; Roberti, M.P.; Yamazaki, T.; Routy, B.; Lepage, P.; Boneca, I.G.; Chamaillard, M.; Kroemer, G.; et al. Resistance Mechanisms to Immune-Checkpoint Blockade in Cancer: Tumor-Intrinsic and -Extrinsic Factors. Immunity 2016, 44, 1255–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, J.S.; Long, G.V.; Scolyer, R.A.; Teng, M.W.L.; Smyth, M.J. Resistance to PD1/PDL1 Checkpoint Inhibition. Cancer Treat. Rev. 2017, 52, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of Resistance to Immune Checkpoint Inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef]
- Gubin, M.M.; Zhang, X.; Schuster, H.; Caron, E.; Ward, J.P.; Noguchi, T.; Ivanova, Y.; Hundal, J.; Arthur, C.D.; Krebber, W.-J.; et al. Checkpoint Blockade Cancer Immunotherapy Targets Tumour-Specific Mutant Antigens. Nature 2014, 515, 577–581. [Google Scholar] [CrossRef]
- Marincola, F.M.; Jaffee, E.M.; Hicklin, D.J.; Ferrone, S. Escape of Human Solid Tumors from T-Cell Recognition: Molecular Mechanisms and Functional Significance. Adv. Immunol. 2000, 74, 181–273. [Google Scholar]
- Sucker, A.; Zhao, F.; Real, B.; Heeke, C.; Bielefeld, N.; Maβen, S.; Horn, S.; Moll, I.; Maltaner, R.; Horn, P.A.; et al. Genetic Evolution of T-Cell Resistance in the Course of Melanoma Progression. Clin. Cancer Res. 2014, 20, 6593–6604. [Google Scholar] [CrossRef]
- Liu, C.; Peng, W.; Xu, C.; Lou, Y.; Zhang, M.; Wargo, J.A.; Chen, J.Q.; Li, H.S.; Watowich, S.S.; Yang, Y.; et al. BRAF Inhibition Increases Tumor Infiltration by T Cells and Enhances the Antitumor Activity of Adoptive Immunotherapy in Mice. Clin. Cancer Res. 2013, 19, 393–403. [Google Scholar] [CrossRef]
- Spranger, S.; Bao, R.; Gajewski, T.F. Melanoma-Intrinsic β-Catenin Signalling Prevents Anti-Tumour Immunity. Nature 2015, 523, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.S.; Zaretsky, J.M.; Escuin-Ordinas, H.; Garcia-Diaz, A.; Hu-Lieskovan, S.; Kalbasi, A.; Grasso, C.S.; Hugo, W.; Sandoval, S.; Torrejon, D.Y.; et al. Primary Resistance to PD-1 Blockade Mediated by JAK1/2 Mutations. Cancer Discov. 2017, 7, 188–201. [Google Scholar] [CrossRef] [PubMed]
- Kryczek, I.; Zou, L.; Rodriguez, P.; Zhu, G.; Wei, S.; Mottram, P.; Brumlik, M.; Cheng, P.; Curiel, T.; Myers, L.; et al. B7-H4 Expression Identifies a Novel Suppressive Macrophage Population in Human Ovarian Carcinoma. J. Exp. Med. 2006, 203, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Kuang, D.-M.; Zhao, Q.; Peng, C.; Xu, J.; Zhang, J.-P.; Wu, C.; Zheng, L. Activated Monocytes in Peritumoral Stroma of Hepatocellular Carcinoma Foster Immune Privilege and Disease Progression through PD-L1. J. Exp. Med. 2009, 206, 1327–1337. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Cagnon, L.; Costa-Nunes, C.M.; Baumgaertner, P.; Montandon, N.; Leyvraz, L.; Michielin, O.; Romano, E.; Speiser, D.E. Frequencies of Circulating MDSC Correlate with Clinical Outcome of Melanoma Patients Treated with Ipilimumab. Cancer Immunol. Immunother. 2014, 63, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Marelli, G.; Howells, A.; Lemoine, N.R.; Wang, Y. Oncolytic Viral Therapy and the Immune System: A Double-Edged Sword Against Cancer. Front. Immunol. 2018, 9, 866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andtbacka, R.H.I.; Kaufman, H.L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; Delman, K.A.; Spitler, L.E.; Puzanov, I.; Agarwala, S.S.; et al. Talimogene Laherparepvec Improves Durable Response Rate in Patients with Advanced Melanoma. J. Clin. Oncol. 2015, 33, 2780–2788. [Google Scholar] [CrossRef]
- Ribas, A.; Dummer, R.; Puzanov, I.; VanderWalde, A.; Andtbacka, R.H.I.; Michielin, O.; Olszanski, A.J.; Malvehy, J.; Cebon, J.; Fernandez, E.; et al. Oncolytic Virotherapy Promotes Intratumoral T Cell Infiltration and Improves Anti-PD-1 Immunotherapy. Cell 2018, 174, 1031–1032. [Google Scholar] [CrossRef]
- Schouppe, E.; De Baetselier, P.; Van Ginderachter, J.A.; Sarukhan, A. Instruction of Myeloid Cells by the Tumor Microenvironment. Oncoimmunology 2012, 1, 1135–1145. [Google Scholar] [CrossRef]
- Liu, T.; Han, C.; Wang, S.; Fang, P.; Ma, Z.; Xu, L.; Yin, R. Cancer-Associated Fibroblasts: An Emerging Target of Anti-Cancer Immunotherapy. J. Hematol. Oncol. 2019, 12, 86. [Google Scholar] [CrossRef]
- Awad, R.M.; De Vlaeminck, Y.; Maebe, J.; Goyvaerts, C.; Breckpot, K. Turn Back the TIMe: Targeting Tumor Infiltrating Myeloid Cells to Revert Cancer Progression. Front. Immunol. 2018, 9, 1977. [Google Scholar] [CrossRef] [PubMed]
- Shurin, G.V.; Ouellette, C.E.; Shurin, M.R. Regulatory Dendritic Cells in the Tumor Immunoenvironment. Cancer Immunol. Immunother. 2012, 61, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Fridlender, Z.G.; Sun, J.; Kim, S.; Kapoor, V.; Cheng, G.; Ling, L.; Worthen, G.S.; Albelda, S.M. Polarization of Tumor-Associated Neutrophil Phenotype by TGF-Beta: “N1” versus “N2” TAN. Cancer Cell 2009, 16, 183–194. [Google Scholar] [CrossRef]
- Ma, Y.; Aymeric, L.; Locher, C.; Kroemer, G.; Zitvogel, L. The Dendritic Cell-Tumor Cross-Talk in Cancer. Curr. Opin. Immunol. 2011, 23, 146–152. [Google Scholar] [CrossRef]
- Ostrand-Rosenberg, S.; Sinha, P. Myeloid-Derived Suppressor Cells: Linking Inflammation and Cancer. J. Immunol. 2009, 182, 4499–4506. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.; Giannoudis, A.; Corke, K.P.; Gill, D.; Wells, M.; Ziegler-Heitbrock, L.; Lewis, C.E. Hypoxia-Induced Gene Expression in Human Macrophages: Implications for Ischemic Tissues and Hypoxia-Regulated Gene Therapy. Am. J. Pathol. 2003, 163, 1233–1243. [Google Scholar] [CrossRef]
- Corzo, C.A.; Condamine, T.; Lu, L.; Cotter, M.J.; Youn, J.-I.; Cheng, P.; Cho, H.-I.; Celis, E.; Quiceno, D.G.; Padhya, T.; et al. HIF-1α Regulates Function and Differentiation of Myeloid-Derived Suppressor Cells in the Tumor Microenvironment. J. Exp. Med. 2010, 207, 2439–2453. [Google Scholar] [CrossRef]
- Mahadevan, N.R.; Zanetti, M. Tumor Stress inside out: Cell-Extrinsic Effects of the Unfolded Protein Response in Tumor Cells Modulate the Immunological Landscape of the Tumor Microenvironment. J. Immunol. 2011, 187, 4403–4409. [Google Scholar] [CrossRef]
- Kalinski, P. Regulation of Immune Responses by Prostaglandin E2. J. Immunol. 2012, 188, 21–28. [Google Scholar] [CrossRef]
- Sato, T.; Terai, M.; Tamura, Y.; Alexeev, V.; Mastrangelo, M.J.; Selvan, S.R. Interleukin 10 in the Tumor Microenvironment: A Target for Anticancer Immunotherapy. Immunol. Res. 2011, 51, 170–182. [Google Scholar] [CrossRef]
- Flavell, R.A.; Sanjabi, S.; Wrzesinski, S.H.; Licona-Limón, P. The Polarization of Immune Cells in the Tumour Environment by TGFbeta. Nat. Rev. Immunol. 2010, 10, 554–567. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadeh, M.; Rosenberg, S.A. TGF-Beta 1 Attenuates the Acquisition and Expression of Effector Function by Tumor Antigen-Specific Human Memory CD8 T Cells. J. Immunol. 2005, 174, 5215–5223. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Thudium, K.B.; Han, M.; Wang, X.-T.; Huang, H.; Feingersh, D.; Garcia, C.; Wu, Y.; Kuhne, M.; Srinivasan, M.; et al. In Vitro Characterization of the Anti-PD-1 Antibody Nivolumab, BMS-936558, and In Vivo Toxicology in Non-Human Primates. Cancer Immunol. Res. 2014, 2, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Fessas, P.; Lee, H.; Ikemizu, S.; Janowitz, T. A Molecular and Preclinical Comparison of the PD-1–Targeted T-Cell Checkpoint Inhibitors Nivolumab and Pembrolizumab. Semin. Oncol. 2017, 44, 136–140. [Google Scholar] [CrossRef]
- Overman, M.J.; Lonardi, S.; Wong, K.Y.M.; Lenz, H.-J.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; Van Cutsem, E.; McDermott, R.; Hill, A.; et al. Durable Clinical Benefit with Nivolumab Plus Ipilimumab in DNA Mismatch Repair–Deficient/Microsatellite Instability–High Metastatic Colorectal Cancer. J. Clin. Oncol. 2018, 36, 773–779. [Google Scholar] [CrossRef]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Chiarion-Sileni, V.; Grob, J.-J.; Dummer, R.; Wolchok, J.D.; Schmidt, H.; Hamid, O.; Robert, C.; Ascierto, P.A.; Richards, J.M.; et al. Adjuvant Ipilimumab versus Placebo after Complete Resection of High-Risk Stage III Melanoma (EORTC 18071): A Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol. 2015, 16, 522–530. [Google Scholar] [CrossRef]
- Merchant, M.S.; Wright, M.; Baird, K.; Wexler, L.H.; Rodriguez-Galindo, C.; Bernstein, D.; Delbrook, C.; Lodish, M.; Bishop, R.; Wolchok, J.D.; et al. Phase I Clinical Trial of Ipilimumab in Pediatric Patients with Advanced Solid Tumors. Clin. Cancer Res. 2016, 22, 1364–1370. [Google Scholar] [CrossRef]
- Geoerger, B.; Bergeron, C.; Gore, L.; Sender, L.; Dunkel, I.J.; Herzog, C.; Brochez, L.; Cruz, O.; Nysom, K.; Berghorn, E.; et al. Phase II Study of Ipilimumab in Adolescents with Unresectable Stage III or IV Malignant Melanoma. Eur. J. Cancer 2017, 86, 358–363. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination Nivolumab and Ipilimumab or Nivolumab Alone in Melanoma Brain Metastases: A Multicentre Randomised Phase 2 Study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Ciuleanu, T.-E.; Pluzanski, A.; Lee, J.S.; Otterson, G.A.; Audigier-Valette, C.; Minenza, E.; Linardou, H.; Burgers, S.; Salman, P.; et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N. Engl. J. Med. 2018, 378, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Slovin, S.F.; Higano, C.S.; Hamid, O.; Tejwani, S.; Harzstark, A.; Alumkal, J.J.; Scher, H.I.; Chin, K.; Gagnier, P.; McHenry, M.B.; et al. Ipilimumab Alone or in Combination with Radiotherapy in Metastatic Castration-Resistant Prostate Cancer: Results from an Open-Label, Multicenter Phase I/II Study. Ann. Oncol. 2013, 24, 1813–1821. [Google Scholar] [CrossRef]
- Reck, M.; Bondarenko, I.; Luft, A.; Serwatowski, P.; Barlesi, F.; Chacko, R.; Sebastian, M.; Lu, H.; Cuillerot, J.-M.; Lynch, T.J. Ipilimumab in Combination with Paclitaxel and Carboplatin as First-Line Therapy in Extensive-Disease-Small-Cell Lung Cancer: Results from a Randomized, Double-Blind, Multicenter Phase 2 Trial. Ann. Oncol. 2013, 24, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Luft, A.; Szczesna, A.; Havel, L.; Kim, S.-W.; Akerley, W.; Pietanza, M.C.; Wu, Y.; Zielinski, C.; Thomas, M.; et al. Phase III Randomized Trial of Ipilimumab Plus Etoposide and Platinum Versus Placebo Plus Etoposide and Platinum in Extensive-Stage Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 3740–3748. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Kefford, R.; Marshall, M.A.; Punt, C.J.A.; Haanen, J.B.; Marmol, M.; Garbe, C.; Gogas, H.; Schachter, J.; Linette, G.; et al. Phase III Randomized Clinical Trial Comparing Tremelimumab With Standard-of-Care Chemotherapy in Patients with Advanced Melanoma. J. Clin. Oncol. 2013, 31, 616–622. [Google Scholar] [CrossRef]
- Calabrò, L.; Morra, A.; Fonsatti, E.; Cutaia, O.; Fazio, C.; Annesi, D.; Lenoci, M.; Amato, G.; Danielli, R.; Altomonte, M.; et al. Efficacy and Safety of an Intensified Schedule of Tremelimumab for Chemotherapy-Resistant Malignant Mesothelioma: An Open-Label, Single-Arm, Phase 2 Study. Lancet Respir. Med. 2015, 3, 301–309. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Chul Cho, B.; Reinmuth, N.; Lee, K.H.; Ahn, M.-J.; Luft, A.; van den Heuvel, M.; Cobo, M.; Smolin, A.; Vicente, D.; et al. LBA6Durvalumab with or without Tremelimumab vs Platinum-Based Chemotherapy as First-Line Treatment for Metastatic Non-Small Cell Lung Cancer: MYSTIC. Ann. Oncol. 2018, 29 (Suppl. 10). [Google Scholar] [CrossRef]
- Morris, V.K.; Salem, M.E.; Nimeiri, H.; Iqbal, S.; Singh, P.; Ciombor, K.; Polite, B.; Deming, D.; Chan, E.; Wade, J.L.; et al. Nivolumab for Previously Treated Unresectable Metastatic Anal Cancer (NCI9673): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol. 2017, 18, 446–453. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Boku, N.; Satoh, T.; Ryu, M.-H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.-S.; Muro, K.; Kang, W.K.; et al. Nivolumab in Patients with Advanced Gastric or Gastro-Oesophageal Junction Cancer Refractory to, or Intolerant of, at Least Two Previous Chemotherapy Regimens (ONO-4538-12, ATTRACTION-2): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Reardon, D.A.; Omuro, A.; Brandes, A.A.; Rieger, J.; Wick, A.; Sepulveda, J.; Phuphanich, S.; De Souza, P.; Ahluwalia, M.S.; Lim, M.; et al. OS10.3 Randomized Phase 3 Study Evaluating the Efficacy and Safety of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma: CheckMate 143. Neuro-oncology 2017, 19 (Suppl. 3), iii21. [Google Scholar] [CrossRef]
- Primary Endpoint Not Met in Phase III CheckMate498 Trial of MGMT-Unmethylated GBM. Available online: https://www.targetedonc.com/news/primary-endpoint-not-met-in-phase-iii-checkmate498-trial-of-mgmtunmethylated-gbm (accessed on 11 October 2019).
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.-L.; Mathurin, P.; Edeline, J.; Kudo, M.; Han, K.-H.; Harding, J.J.; Merle, P.; et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann. Oncol. 2019, 30, mdz394.029. [Google Scholar] [CrossRef]
- Weber, J.; Mandala, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- Scherpereel, A.; Mazieres, J.; Greillier, L.; Lantuejoul, S.; Dô, P.; Bylicki, O.; Monnet, I.; Corre, R.; Audigier-Valette, C.; Locatelli-Sanchez, M.; et al. Nivolumab or Nivolumab plus Ipilimumab in Patients with Relapsed Malignant Pleural Mesothelioma (IFCT-1501 MAPS2): A Multicentre, Open-Label, Randomised, Non-Comparative, Phase 2 Trial. Lancet Oncol. 2019, 20, 239–253. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Mazières, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and Safety of Nivolumab, an Anti-PD-1 Immune Checkpoint Inhibitor, for Patients with Advanced, Refractory Squamous Non-Small-Cell Lung Cancer (CheckMate 063): A Phase 2, Single-Arm Trial. Lancet Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.-E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef]
- Motzer, R.J.; Rini, B.I.; McDermott, D.F.; Redman, B.G.; Kuzel, T.M.; Harrison, M.R.; Vaishampayan, U.N.; Drabkin, H.A.; George, S.; Logan, T.F.; et al. Nivolumab for Metastatic Renal Cell Carcinoma: Results of a Randomized Phase II Trial. J. Clin. Oncol. 2015, 33, 1430–1437. [Google Scholar] [CrossRef]
- Bellmunt, J.; De Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; Wit, R.D.; Pang, L.; et al. First-Line Pembrolizumab in Cisplatin-Ineligible Patients with Locally Advanced and Unresectable or Metastatic Urothelial Cancer (KEYNOTE-052): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- O’Donnell, P.H.; Balar, A.V.; Vuky, J.; Castellano, D.E.; Bellmunt, J.; Powles, T.; Bajorin, D.F.; Grivas, P.; Hahn, N.M.; Plimack, E.R.; et al. KEYNOTE-052: Phase 2 Study Evaluating First-Line Pembrolizumab (Pembro) in Cisplatin-Ineligible Advanced Urothelial Cancer (UC)—Updated Response and Survival Results. J. Clin. Oncol. 2019, 37 (Suppl. 15), 4546. [Google Scholar] [CrossRef]
- Shah, M.A.; Kojima, T.; Hochhauser, D.; Enzinger, P.; Raimbourg, J.; Hollebecque, A.; Lordick, F.; Kim, S.-B.; Tajika, M.; Kim, H.T.; et al. Efficacy and Safety of Pembrolizumab for Heavily Pretreated Patients with Advanced, Metastatic Adenocarcinoma or Squamous Cell Carcinoma of the Esophagus: The Phase 2 KEYNOTE-180 Study. JAMA Oncol. 2019, 5, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Muro, K.; Francois, E.; Hsu, C.-H.; Moriwaki, T.; Kim, S.-B.; Lee, S.-H.; Bennouna, J.; Kato, K.; Lin, S.; et al. Pembrolizumab versus Chemotherapy as Second-Line Therapy for Advanced Esophageal Cancer: Phase III KEYNOTE-181 Study. J. Clin. Oncol. 2019, 37 (Suppl. 4), 2. [Google Scholar] [CrossRef]
- Rischin, D.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; De Castro, G.; Psyrri, A.; Baste, N.; Neupane, P.C.; Bratland, A.; et al. Protocol-Specified Final Analysis of the Phase 3 KEYNOTE-048 Trial of Pembrolizumab (Pembro) as First-Line Therapy for Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma (R/M HNSCC). J. Clin. Oncol. 2019, 37 (Suppl. 15), 6000. [Google Scholar] [CrossRef]
- Le, D.T.; Kavan, P.; Kim, T.W.; Burge, M.E.; Van Cutsem, E.; Hara, H.; Boland, P.M.; Van Laethem, J.-L.; Geva, R.; Taniguchi, H.; et al. KEYNOTE-164: Pembrolizumab for Patients with Advanced Microsatellite Instability High (MSI-H) Colorectal Cancer. J. Clin. Oncol. 2018, 36 (Suppl. 15), 3514. [Google Scholar] [CrossRef]
- Hsu, C.; Lee, S.-H.; Ejadi, S.; Even, C.; Cohen, R.B.; Le Tourneau, C.; Mehnert, J.M.; Algazi, A.; van Brummelen, E.M.J.; Saraf, S.; et al. Safety and Antitumor Activity of Pembrolizumab in Patients with Programmed Death-Ligand 1–Positive Nasopharyngeal Carcinoma: Results of the KEYNOTE-028 Study. J. Clin. Oncol. 2017, 35, 4050–4056. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus Docetaxel for Previously Treated, PD-L1-Positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010): A Randomised Controlled Trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Şenler, F.Ç.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Ott, P.A.; Elez, E.; Hiret, S.; Kim, D.-W.; Morosky, A.; Saraf, S.; Piperdi, B.; Mehnert, J.M. Pembrolizumab in Patients with Extensive-Stage Small-Cell Lung Cancer: Results From the Phase Ib KEYNOTE-028 Study. J. Clin. Oncol. 2017, 35, 3823–3829. [Google Scholar] [CrossRef]
- Chung, H.C.; Piha-Paul, S.A.; Lopez-Martin, J.; Schellens, J.H.M.; Kao, S.; Miller, W.H.; Delord, J.-P.; Gao, B.; Planchard, D.; Gottfried, M.; et al. Abstract CT073: Pembrolizumab after Two or More Lines of Prior Therapy in Patients with Advanced Small-Cell Lung Cancer (SCLC): Results from the KEYNOTE-028 and KEYNOTE-158 Studies. Cancer Res. 2019, 79 (Suppl. 13), CT073. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as First-Line Treatment in Cisplatin-Ineligible Patients with Locally Advanced and Metastatic Urothelial Carcinoma: A Single-Arm, Multicentre, Phase 2 Trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef]
- Sullivan, R.J.; Hamid, O.; Gonzalez, R.; Infante, J.R.; Patel, M.R.; Hodi, F.S.; Lewis, K.D.; Tawbi, H.A.; Hernandez, G.; Wongchenko, M.J.; et al. Atezolizumab plus Cobimetinib and Vemurafenib in BRAF -Mutated Melanoma Patients. Nat. Med. 2019, 25, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus Docetaxel in Patients with Previously Treated Non-Small-Cell Lung Cancer (OAK): A Phase 3, Open-Label, Multicentre Randomised Controlled Trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Barlesi, F.; Vansteenkiste, J.; Spigel, D.; Ishii, H.; Garassino, M.; De Marinis, F.; Özgüroğlu, M.; Szczesna, A.; Polychronis, A.; Uslu, R.; et al. Avelumab versus Docetaxel in Patients with Platinum-Treated Advanced Non-Small-Cell Lung Cancer (JAVELIN Lung 200): An Open-Label, Randomised, Phase 3 Study. Lancet Oncol. 2018, 19, 1468–1479. [Google Scholar] [CrossRef]
- Powles, T.; O’Donnell, P.H.; Massard, C.; Arkenau, H.-T.; Friedlander, T.W.; Hoimes, C.J.; Lee, J.L.; Ong, M.; Sridhar, S.S.; Vogelzang, N.J.; et al. Efficacy and Safety of Durvalumab in Locally Advanced or Metastatic Urothelial Carcinoma: Updated Results from a Phase 1/2 Open-Label Study. JAMA Oncol. 2017, 3, e172411. [Google Scholar] [CrossRef]
- Nowak, A.K.; Lesterhuis, W.J.; Hughes, B.G.M.; Brown, C.; Kok, P.S.; O’Byrne, K.J.; John, T.; Pavlakis, N.; Kao, S.C.-H.; Yip, S.; et al. DREAM: A Phase II Study of Durvalumab with First Line Chemotherapy in Mesothelioma—First Results. J. Clin. Oncol. 2018, 36 (Suppl. 15), 8503. [Google Scholar] [CrossRef]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gravbrot, N.; Gilbert-Gard, K.; Mehta, P.; Ghotmi, Y.; Banerjee, M.; Mazis, C.; Sundararajan, S. Therapeutic Monoclonal Antibodies Targeting Immune Checkpoints for the Treatment of Solid Tumors. Antibodies 2019, 8, 51. https://doi.org/10.3390/antib8040051
Gravbrot N, Gilbert-Gard K, Mehta P, Ghotmi Y, Banerjee M, Mazis C, Sundararajan S. Therapeutic Monoclonal Antibodies Targeting Immune Checkpoints for the Treatment of Solid Tumors. Antibodies. 2019; 8(4):51. https://doi.org/10.3390/antib8040051
Chicago/Turabian StyleGravbrot, Nicholas, Kacy Gilbert-Gard, Paras Mehta, Yarah Ghotmi, Madhulika Banerjee, Christopher Mazis, and Srinath Sundararajan. 2019. "Therapeutic Monoclonal Antibodies Targeting Immune Checkpoints for the Treatment of Solid Tumors" Antibodies 8, no. 4: 51. https://doi.org/10.3390/antib8040051