
Direct Esthetic Composite Restorations in Anterior Teeth: Managing Symmetry Strategies



1
Department of Dentistry, IRCCS San Raffaele Hospital and Dental School, Vita Salute University, 20132 Milan, Italy
2
Private Practice, 80035 Nola, Italy
3
Department of Neuroscience, Reproductive and Odontostomatological Sciences, University of Naples “Federico II”, 80131 Naples, Italy
*
Author to whom correspondence should be addressed.
Symmetry 2021, 13(5), 797; https://doi.org/10.3390/sym13050797
Submission received: 18 April 2021
/
Revised: 27 April 2021
/
Accepted: 1 May 2021
/
Published: 3 May 2021
(This article belongs to the Special Issue Symmetry in Dentistry: From the Clinic to the Lab)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:A novel procedure for symmetric and consistent layer thickness management in esthetic direct restoration of anterior teeth is presented. For the purpose of obtaining a satisfactory final outcome of an esthetic direct restoration, it is crucial to standardize either margin preparation design and dentin and enamel layer thickness. Leaving too much space for the final translucent layer may lead in fact to “low value—gray” restorations if not correctly managed. The most common tool used to check layer thickness is the sagittal silicone index, which is reliable but involves planning; therefore, it requires two stages appointments. In this clinical case, a novel procedure is used to prepare, to model and to check thickness of composite shades in a single appointment, thus providing a symmetric esthetic outcome. A healthy 21-year-old woman referred to our dental office for the esthetic rehabilitation of both maxillary central incisors. The correct composite bilateral and symmetric layer thickness management provided a predictable esthetic outcome of the restorations. The main objective of this case presentation is to describe a novel technique that is able to save chair-time and dental laboratory costs during direct restorations in anterior teeth.
1. Introduction
Most animals, and therefore human beings, are bilaterians [1], they have a bilateral symmetry [2] with respect to the sagittal plane. Bilateral symmetry (also referred to as mirror symmetry, mirror-image symmetry and reflection symmetry) find in the two maxillary central incisors one of its highest expressions. Since these teeth are the most important part of a smile, every clinician should take particular care to the following aspects related to symmetry:
For all these reasons, clinicians shall try to keep central incisors as symmetric as possible during the restorative procedures. This is performed easily in indirect restorations (veneers and crowns) because they are managed in the laboratory [9].
In direct restorations, there are some tools and procedures, which are the subject of this case presentation, that the clinician can take advantage from in order to provide symmetric esthetic restorations.
2. Case Presentation
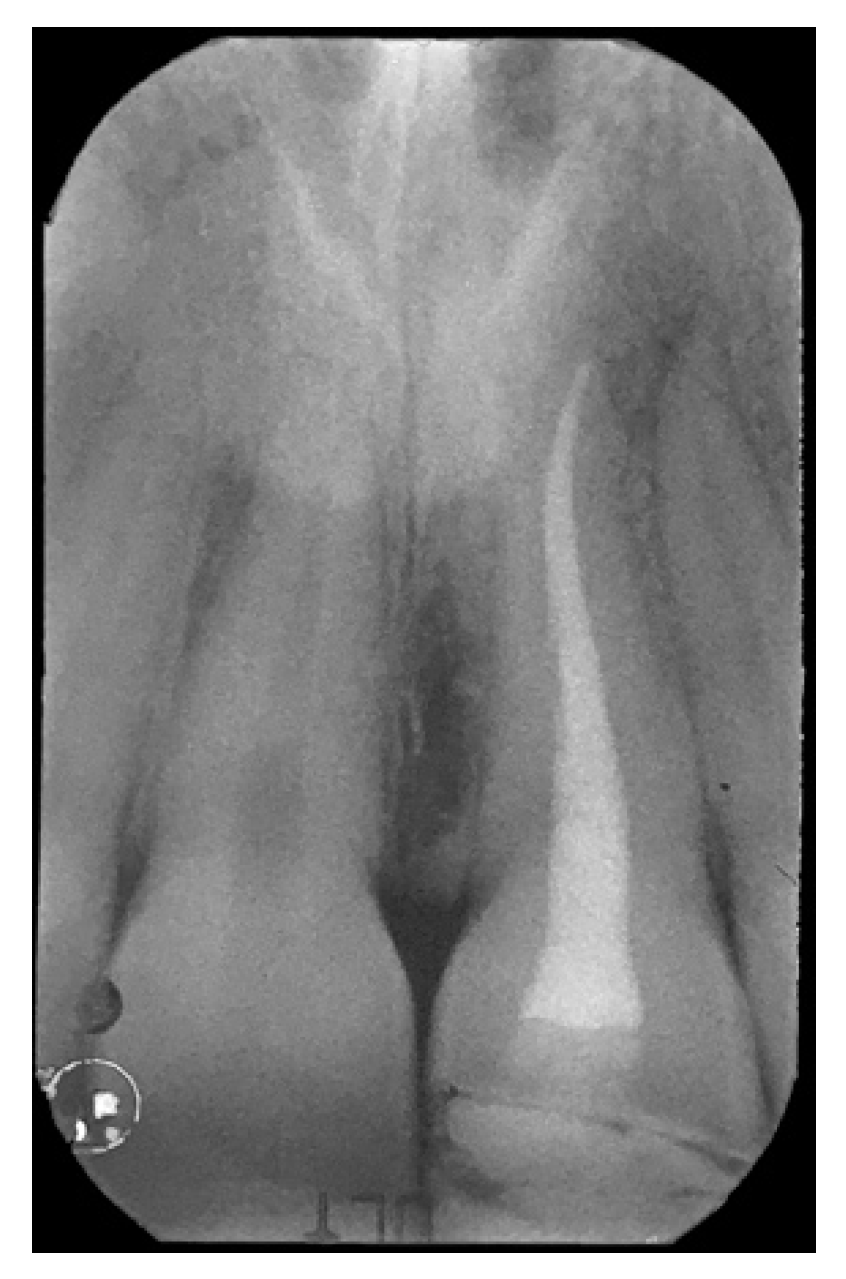
A healthy 21-year-old woman referred to the dental office for the esthetic rehabilitation of both central maxillary incisors. The patient had a good oral status, with full mouth plaque score (FMPS) and full mouth bleeding score (FMBS) equal to 0 and 1, respectively. After clinical examination (Figure 1), both restorations resulted in being incongruous in shape and color. Radiographic examination (Figure 2) revealed a satisfactory endodontic treatment. The translucent areas around the interface suggested a poor internal adaptation of the restorative material.
Because of the young age of the patient, a noninvasive treatment with direct restoration was proposed. As suggested by several authors, because of the quantity of the residual sound tissue, no post was planned for the left central incisor [10,11]. After having analyzed the smile-line of the patient (Figure 3), silicone impressions were taken with a polyether material (Impregum Penta + Permadyne Penta L, 3M Espe; St. Paul, MN, USA) in order to develop a diagnostic wax-up (Figure 4 and Figure 5) [12].
On the diagnostic wax-up, a palatal silicone index (Elite HD+, Zhermack, Badia Polesine, Italy) was created with a canine-to-canine extension (Figure 6). The palatal silicon index was modified with a scalpel in order to remove buccal portions and in order to have a passive fit during restorative procedures.
Before restorative procedures, the shades of both the sound tissue and the previous restorations were recorded, using commercial shade references tabs (Figure 7). In order to select the main dentinal shade, a small amount of composite (“button-try”) was placed on the unrestored part of the central incisor and cured (Figure 8) [13]. According to the collected shade information, a color map was sketched with the selection of the shades to be used to reproduce symmetrically both maxillary incisors (Figure 9).
The operatory field was cleaned with a chlorhexidine and pumice paste applied with a nylon rotating brush and then with a glycine powder blasting device (PROPHYflex KaVo Dental AG, Biberach, Germany). The upper arch was isolated with a rubber dam (R&S, Paris, France) from second right premolar to second left premolar, using 2A clamps (HuFriedy, Chicago, IL, USA) (Figure 10).
Restorations were carefully removed (Figure 11), using high-speed diamond burs (FG 001 G 014, Horico, Berlin, Germany) and low-speed carbide ones (Excavabur, Dentsply Sirona, York, PA, USA).
In order to symmetrically prepare the margin (therefore to allow a comparable quantity of material on both preparation margins), a calibrated bur (FG 277P021 Horico, Berlin, Germany) was used (Figure 12 and Figure 13). Adhesive procedures were then performed, using a 3-Step etch-and-rinse adhesive system (Optibond FL, Kerr, Bioggio, Switzerland) after etching with a 38% phosphoric acid gel (Ultra-Etch, Ultradent Product, Inc., South Jordan, UT, USA) and light cured for 20 s with a visible light-curing unit with an intensity of 1000 mW/cm2 (Valo, Ultradent, South Jordan, UT, USA).
Composite was then applied on the silicone index in order to mold palatal and incisal margin (Figure 14).
The silicone index, with the uncured composite (Clearfil Majesty ES-2 A2E, A2D, Kuraray Noritake Dental, Tokyo, Japan), was positioned in the mouth of the patient. The composite was cured from buccal and incisal area for 20″. The silicone index was then gently removed, and another 20″ light curing was performed from the palatal side. Distal and mesial walls were restored with the help of transparent convex mylar strips (Hawe Adapt, Kerr, Bioggio, Switzerland) and a wooden wedge (Sycamore, Kerr, Bioggio, Switzerland) (Figure 15 and Figure 16).
With the aid of the “OUT” tip of a clinical caliper (TNCALIBRA, HuFriedy, Chicago, IL, USA) (Figure 17), it was possible, during all the steps of the layering procedure, to quickly visualize the volume of composite needed to restore either the dentin and the enamel of both central incisors.
The tip “IN” of the same instruments was used to model, in a precise way, the internal dentinal body (Figure 18). This instrument allows a symmetric modeling and can define the internal mamelons typical of anterior maxillary incisors.
Although central incisors are symmetrical, little variations among mamelon length and width may provide a natural aspect (Figure 19).
The superficial enamel layer was then applied on both incisors and excess removed with the “OUT” tip of the abovementioned caliper. In order to provide both incisors with a symmetrical aspect, an opaque white staining material (Kolor + Plus, Kerr, Bioggio, Switzerland) was applied on the buccal aspect of the left central incisor in order to replicate the white spot present on the right central incisor (Figure 20).
Great care was taken in providing proper light curing to obtain the highest degree of conversion, in order to reduce possible staining and reduce potential monomer citotoxicity [14,15,16,17]. After last light curing, finishing (Figure 21) and polishing (Figure 22) were performed with burs, silicone points (Enhance, Dentsply Sirona, York, PA, USA), discs (Sof-Lex, 3M ESPE, St. Paul, MN, USA) and felts with diamond paste (Prisma Gloss, Dentsply Sirona, York, PA, USA).
After rubber dam removal (Figure 23), occlusion and functional movements were checked, and the patient was rescheduled for post-op evaluation 1 week later. At the recall appointment (Figure 24), post-op functional and structural evaluation (absence of fracture and marginal adaptation), biological evaluation (post-operative sensitivity) and esthetic evaluation (gloss, color stability) were performed and were fully satisfactory. As a final recommendation, oral hygiene instructions were reviewed, and the patient was rescheduled for a regular 6-month follow-up appointment. After 6 months, function and esthetic were checked, resulting in being fully satisfactory (Figure 25, Figure 26 and Figure 27). Patient expectations and post-treatment satisfaction were recorded in questionnaires, using a visual analogue scale, and they scored fully satisfactory. Operator also filled a questionnaire before and after the treatment, recording several variables, such as overall time of treatment, shade used, adhesive procedures performed, esthetic limitations, esthetic expectations and esthetic outcomes [18]. Bilateral symmetry was verified both form an anatomical and esthetic point of view, while the final outcome met the previously planned anatomy, shades, opacities and translucencies.
3. Discussion
Currently, composite resin is the first-choice material for direct restorations of anterior and posterior teeth [19,20].
Restorative procedures of direct anterior teeth based on the use of a silicone index are well established since many years [21,22,23,24,25].
Symmetric reproduction of bilateral anatomical elements is challenging for every clinician. Indirect restorations, while planned in the lab, can be manufactured precisely reproducing the correct symmetry, especially when working in a digital workflow. In direct restorations, dealing with a specular symmetry is more difficult and some authors have proposed strategies to manage this challenging situation [21].
A correct management for a predictable symmetric outcome involves every aspect of the restorative procedure. First of all, margins should be prepared with the same design and geometry, while different material, different thickness and different substrate may provide different esthetic outcomes [26,27]. Using a calibrated bur, as seen in this case report, can help the clinician in creating a consistent margin design though reducing the risk of color mismatch on the finishing line. Furthermore, the use of the same rotative instruments on a daily basis, while easily providing a reproducible margin definition, allows the clinicians to focus more on other more complex aspects of the restorative procedure. Besides preparation, composite layering plays a fundamental role in the final esthetic outcome. One of the most common procedure is to use a silicone index created in the lab. With this technique [22], it is possible to mold either the palatal and the incisal margin, replicating the planned anatomy. Several authors have tried to mold the buccal surface, but it is a very difficult task to achieve in a predictable way [28]. Several issues in fact have to be managed during a molding procedure from a buccal aspect: (1) any kind of imprecision on the previous restorative steps could cause the misalignment though the correct positioning of the buccal silicone; (2) interproximal excesses can be troublesome to manage and can result in overhangs whose removal could be very difficult and time consuming; (3) when a finishing margin line is available, it is difficult to manage correctly the quantity of restorative material—voids or excesses are difficult to manage even when vent holes are planned in advance. Therefore, the current approach in direct restorations in anterior teeth consists generally of three steps, as described by several authors [21,22,23,24,25]:
- Molding palatal wall and incisal margin;
- Building interproximal walls with matrices;
- Layering free-hand buccal surface.
The palatal silicone index can easily provide a symmetric outcome based on a pre-operative mock-up. Interproximal walls can be restored through the help of sectional convex matrices rather than straight mylar matrix strips [29]. Providing a symmetric interproximal outline can be achieved by twisting the matrices until the desired outline is achieved.
Once the frame (palatal, incisal and interproximal) is completed, it is possible to add internal dentinal shades according to the initial color chart [30]. Internal anatomy influences esthetic outcomes of a multi-layered restoration [31]. The choice of correct opaque and translucent shades can provide a natural aspect to the restoration and should be carefully performed. In the coronoapical direction, the incisal third of anterior maxillary teeth is generally characterized by a thin opaque incisal shade, then by a translucent area and then by the opaque dentinal body, often characterized by mamelons. Commercially available shades generally suggest enamel and dentin to be used with an anatomical criterion, but they are often used to reproduce more opaque areas (with dentinal shades) and more translucent ones (with enamel shades) [12,22,23,24,31,32].
While buccal surface, especially the outer layer, has to be managed free hand, an esthetic and symmetric outcome may be challenging. A correct and uniform thickness of the enamel layer is generally difficult to achieve. This depends first of all on the design and thickness of the underlying dentin. As reported by Friebel M. et al., the influence of the cover layer on the color impression depends on the layer thickness [33]. This finding was also corroborated by Vichi A. et al., who confirmed that layer thickness greatly influences the final aspect of a multi-layer composite restoration [34]. It is well-known, in fact, that exceeding in enamel thickness could provide a gray final outcome (low value). In order to check thickness during the layering procedures, clinicians have generally relied on sagittal silicon index [21,25,31,32]. This tool is reliable but has some drawbacks: it generally requires an additional appointment to take impressions in order to manufacture it; furthermore, it is “static”, as it only shows thickness around the cut of the silicone. This limit could be overcome by performing more cuts although this results in small silicone portions generally not stable and not rigid. Both tips of the caliper described in this case presentation have the characteristic to be anatomic while they follow an average convex shape typical of anterior teeth. Furthermore, they have the capability to be ready-to-use and can be moved mesially and distally in order to “dynamically” check the thickness along all the portions of the restoration. Another important aspect to take in consideration in order to obtain a mimetic restoration is the surface and texture. In the presented case, a step-by-step procedure was followed in order to provide a surface close to the adjacent teeth either for an esthetic purpose and to reduce biofilm formation which can cause discoloration and secondary caries [35,36,37,38].
Within the limitation of this single case presentation, it can be concluded that the described procedure may allow the practitioner a practical solution for symmetrical thickness management in anterior composite restorations. Further research is needed in the form of well-designed, randomized controlled trials with long-term follow-ups, in order to establish the reliability of the proposed technique.
4. Conclusions
A symmetric restoration of both central incisors is a challenging procedure. Clinicians can take advantage of several tools and procedures. The technique presented allows the clinician to easily prepare, model and check the thickness of multi-layered composite restorations. Thickness management is historically performed with a sagittal silicone index that requires two appointments. The proposed technique could be therefore considered a contribution to the well-known silicone index technique, while providing predictable symmetric multi-layered restorations in a single stage appointment, therefore allowing chair-time and laboratory costs savings.
Author Contributions
All authors contributed equally to this work. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Roberto Kaitsas for the endodontic treatment and Francesco Napolitano for the lab wax-up.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Finnerty, J.R. The origins of axial patterning in the metazoa: How old is bilateral symmetry? Int. J. Dev. Biol. 2003, 47, 523–529. [Google Scholar]
- Finnerty, J.R.; Pang, K.; Burton, P.; Paulson, D.; Martindale, M.Q. Origins of bilateral symmetry: Hox and dpp expression in a sea anemone. Science 2004, 304, 1335–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edler, R.J. Background Considerations to Facial Aesthetics. J. Orthod. 2001, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Gallão, S.; Ortolani, C.L.F.; Santos-Pinto, A.; Santos-Pinto, L.; Faltin Júnior, K. Photographic analysis of symmetry and aesthetic proportion of the anterior teeth. Rev. Inst. Ciênc Saúde 2009, 27, 400–404. [Google Scholar]
- Wang, Y.; Song, Y.; Zhong, Q.; Xu, C. Evaluation of influence factors on the width, length, and width to length ratio of the maxillary central incisor: A systematic review and meta-analysis. J. Esthet. Restor. Dent. 2021, 33, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Garn, S.M.; Lewis, A.B.; Walenga, A.J. Maximum-confidence values for the human mesiodistal crown dimension of human teeth. Arch. Oral Biol. 1968, 13, 841–844. [Google Scholar] [CrossRef]
- Mavroskoufis, F.; Ritchie, G. Variation in size and form between left and right maxillary central incisor teeth. J. Prosthet. Dent. 1980, 43, 254–257. [Google Scholar] [CrossRef]
- Rufenacht, C. Fundamentals of Esthetics; Quintessence Publishing: Chicago, IL, USA, 1990. [Google Scholar]
- Aljazairy, Y.H. Survival Rates for Porcelain Laminate Veneers: A Systematic Review. Eur. J. Dent. 2020. [Google Scholar] [CrossRef]
- Batista, V.E.D.S.; Bitencourt, S.B.; Bastos, N.A.; Pellizzer, E.P.; Goiato, M.C.; Dos Santos, D.M. Influence of the ferrule effect on the failure of fiber-reinforced composite post-and-core restorations: A systematic review and meta-analysis. J. Prosthet. Dent. 2020, 123, 239–245. [Google Scholar] [CrossRef]
- Paolone, G.; Saracinelli, M.; Devoto, W.; Putignano, A. Esthetic direct restorations in endodontically treated anterior teeth. Eur. J. Esthet. Dent. 2013, 8, 44–67. [Google Scholar]
- Dietschi, D. Free-Hand Bonding in the Esthetic Treatment of Anterior Teeth: Creating the Illusion. J. Esthet. Restor. Dent. 1997, 9, 156–164. [Google Scholar] [CrossRef]
- Korkut, B.; Türkmen, C. Longevity of direct diastema closure and recontouring restorations with resin composites in maxillary anterior teeth: A 4-year clinical evaluation. J. Esthet. Restor. Dent. 2020. [Google Scholar] [CrossRef]
- Sulaiman, T.A.; Rodgers, B.; Suliman, A.A.; Johnston, W.M. Color and translucency stability of contemporary resin-based restorative materials. J. Esthet. Restor. Dent. 2020. [Google Scholar] [CrossRef]
- Krifka, S.; Hiller, K.-A.; Bolay, C.; Petzel, C.; Spagnuolo, G.; Reichl, F.-X.; Schmalz, G.; Schweikl, H. Function of MAPK and downstream transcription factors in monomer-induced apoptosis. Biomaterials 2012, 33, 740–750. [Google Scholar] [CrossRef]
- Spagnuolo, G.; Desiderio, C.; Rivieccio, V.; Amato, M.; Rossetti, D.V.; D’Antò, V.; Schweikl, H.; Lupi, A.; Rengo, S.; Nocca, G. In vitro cellular detoxification of triethylene glycol dimethacrylate by adduct formation with N-acetylcysteine. Dent. Mater. 2013, 29, e153–e160. [Google Scholar] [CrossRef] [PubMed]
- Schweikl, H.; Spagnuolo, G.; Schmalz, G. Genetic and Cellular Toxicology of Dental Resin Monomers. J. Dent. Res. 2006, 85, 870–877. [Google Scholar] [CrossRef]
- Tin-Oo, M.M.; Saddki, N.; Hassan, N. Factors influencing patient satisfaction with dental appearance and treatments they desire to improve aesthetics. BMC Oral Health. 2011, 11, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demarco, F.F.; Collares, K.; Coelho-De-Souza, F.H.; Correa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Anterior composite restorations: A systematic review on long-term survival and reasons for failure. Dent. Mater. 2015, 31, 1214–1224. [Google Scholar] [CrossRef]
- Opdam, N.J.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of Posterior Composite Restorations. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Paolone, G. Direct composite restorations in anterior teeth. Managing symmetry in central incisors. Int. J. Esthet. Dent. 2014, 9, 12–25. [Google Scholar]
- Vanini, L. Light and color in anterior composite restorations. Pract. Periodontics Aesthetic Dent. 1996, 8, 684. [Google Scholar]
- Fahl, N., Jr. A polychromatic composite layering approach for solving a complex Class IV/direct veneer-diastema combination: Part I. Pract. Proced. Aesthet Dent. 2006, 18, 641–645. [Google Scholar] [PubMed]
- Fahl, N., Jr. A polychromatic composite layering approach for solving a complex Class IV/direct veneer/diastema combination: Part II. Pract. Proced. Aesthet Dent. 2007, 19, 17–22. [Google Scholar]
- Dietschi, D.; Ardu, S.; Krejci, I. A new shading concept based on natural tooth color applied to direct composite restorations. Quintessence Int. 2006, 37, 91–102. [Google Scholar]
- Trifkovic, B.; Powers, J.M.; Paravina, R.D. Color adjustment potential of resin composites. Clin. Oral Investig. 2018, 22, 1601–1607. [Google Scholar] [CrossRef]
- Pereira Sanchez, N.; Powers, J.M.; Paravina, R.D. Instrumental and visual evaluation of the color adjustment potential of resin composites. J. Esthet. Restor. Dent. 2019, 31, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Ammannato, R.; Ferraris, F.; Allegri, M. The “index cutback technique”: A three-dimensional guided layering approach in direct class IV composite restorations. Int. J. Esthet. Dent. 2017, 12, 450–466. [Google Scholar] [PubMed]
- Goyal, A.; Nikhil, V.; Singh, R. Diastema Closure in Anterior Teeth Using a Posterior Matrix. Case Rep. Dent. 2016, 2016, 8526. [Google Scholar] [CrossRef]
- Paolone, G.; Orsini, G.; Manauta, J.; Devoto, W.; Putignano, A. Composite shade guides and color matching. Int. J. Esthet. Dent. 2014, 9, 164–182. [Google Scholar]
- Paolone, G. Direct composites in anteriors: A matter of substrate. Int. J. Esthet. Dent. 2017, 12, 468–481. [Google Scholar]
- Devoto, W.; Saracinelli, M.; Manauta, J. Composite in everyday practice: How to choose the right material and simplify application techniques in the anterior teeth. Eur. J. Esthet. Dent. 2010, 5, 102–124. [Google Scholar]
- Friebel, M.; Pernell, O.; Cappius, H.-J.; Helfmann, J.; Meinke, M.C. Simulation of color perception of layered dental composites using optical properties to evaluate the benefit of esthetic layer preparation technique. Dent. Mater. 2012, 28, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Vichi, A.; Fraioli, A.; Davidson, C.L.; Ferrari, M. Influence of thickness on color in multi-layering technique. Dent. Mater. 2007, 23, 1584–1589. [Google Scholar] [CrossRef]
- Schroeder, T.; Da Silva, P.B.; Basso, G.R.; Franco, M.C.; Maske, T.T.; Cenci, M.S. Factors affecting the color stability and staining of esthetic restorations. Odontology 2019, 107, 507–512. [Google Scholar] [CrossRef]
- Marigo, L.; Nocca, G.; Fiorenzano, G.; Callà, C.; Castagnola, R.; Cordaro, M.; Paolone, G.; Sauro, S. Influences of Different Air-Inhibition Coatings on Monomer Release, Microhardness, and Color Stability of Two Composite Materials. BioMed Res. Int. 2019, 2019, 264. [Google Scholar] [CrossRef] [Green Version]
- Ionescu, A.C.; Cazzaniga, G.; Ottobelli, M.; Ferracane, J.L.; Paolone, G.; Brambilla, E. In vitro biofilm formation on resin-based composites cured under different surface conditions. J. Dent. 2018, 77, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, G.; Ottobelli, M.; Ionescu, A.C.; Paolone, G.; Gherlone, E.; Ferracane, J.L.; Brambilla, E. In vitro biofilm formation on resin-based composites after different finishing and polishing procedures. J. Dent. 2017, 67, 43–52. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Initial clinical situation.

Figure 2.
Pre-op X-ray.

Figure 3.
The smile of the patient before treatment.

Figure 4.
The wax-up developed by the dental lab technician.

Figure 5.
Palatal aspect of the diagnostic wax-up.

Figure 6.
Palatal silicone index created on the diagnostic wax-up.

Figure 7.
Shade selection of both sound tissue and previous restoration.

Figure 8.
The “button-try” on the cervical portion of the left maxillary central incisor.

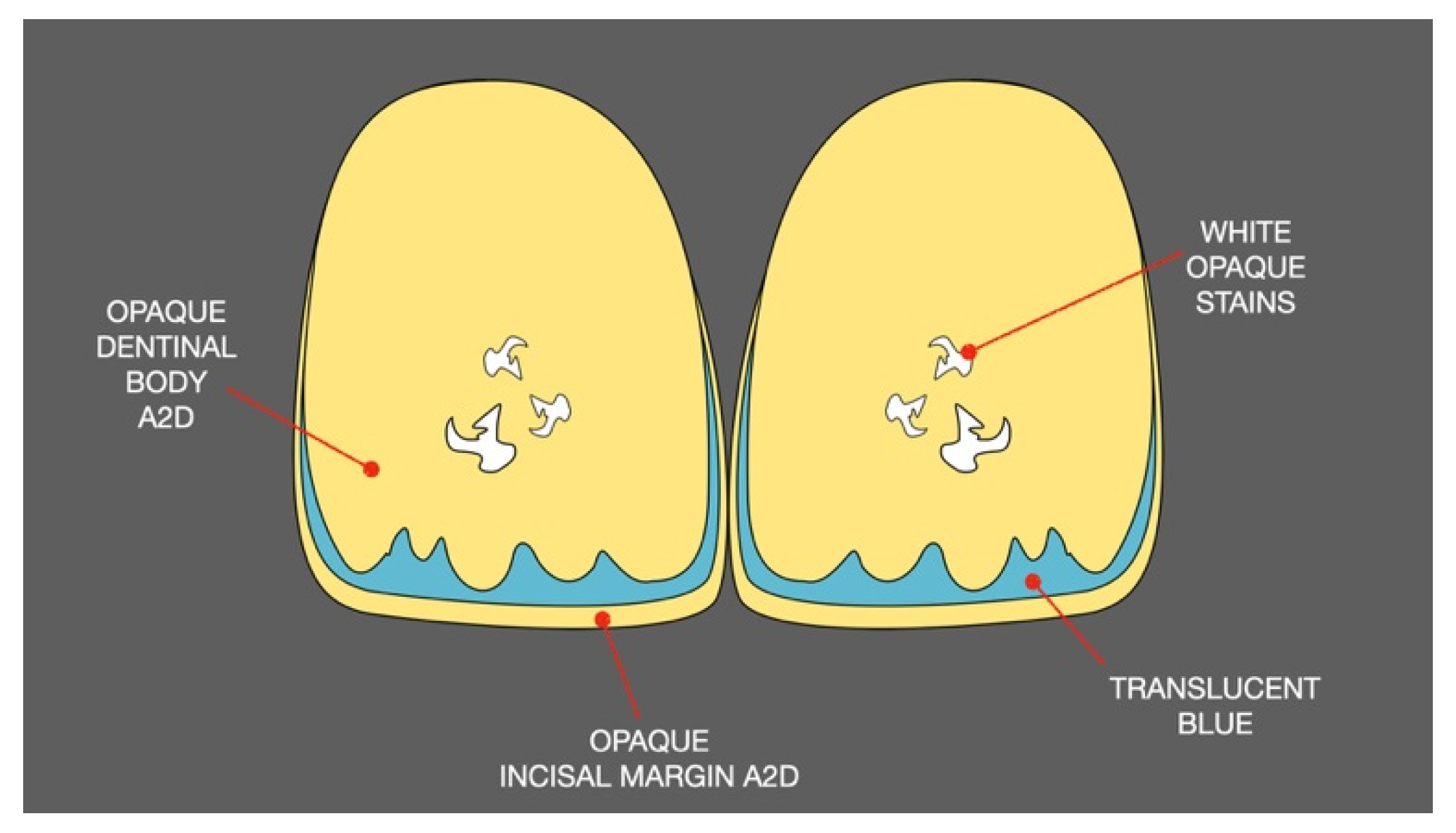
Figure 9.
The color-chart sketch prepared after shade analysis.

Figure 10.
Isolation of the operatory field with rubber dam.

Figure 11.
Previous restorations are removed.

Figure 12.
A symmetric preparation finishing line among both incisors is obtained with a calibrated bur.
Figure 12.
A symmetric preparation finishing line among both incisors is obtained with a calibrated bur.

Figure 13.
Finishing line preparation completed and adhesive procedures performed.

Figure 14.
Composite is placed on the silicon index.

Figure 15.
Completing the frame with the help of convex transparent sectional matrices.

Figure 16.
Both frames are completed.

Figure 17.
Buccal overall restoration thickness is checked with the “OUT” tip.

Figure 18.
Dentinal body is modeled with the “IN” tip.

Figure 19.
Internal anatomy completed.

Figure 20.
After the external enamel layer was applied, a white opaque stain was applied to improve the optical symmetry.
Figure 20.
After the external enamel layer was applied, a white opaque stain was applied to improve the optical symmetry.

Figure 21.
Finishing procedures are performed with burs and disks.

Figure 22.
Polishing procedure completed.

Figure 23.
Final aspect after rubber dam removal.

Figure 24.
The smile of the patient 1 week post-op.

Figure 25.
Six months post-op.

Figure 26.
Six months post-op X-ray.

Figure 27.
The smile of the patient 6 months post-op X-ray.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Paolone, G.; Scolavino, S.; Gherlone, E.; Spagnuolo, G. Direct Esthetic Composite Restorations in Anterior Teeth: Managing Symmetry Strategies. Symmetry 2021, 13, 797. https://doi.org/10.3390/sym13050797
AMA Style
Paolone G, Scolavino S, Gherlone E, Spagnuolo G. Direct Esthetic Composite Restorations in Anterior Teeth: Managing Symmetry Strategies. Symmetry. 2021; 13(5):797. https://doi.org/10.3390/sym13050797
Chicago/Turabian StylePaolone, Gaetano, Salvatore Scolavino, Enrico Gherlone, and Gianrico Spagnuolo. 2021. "Direct Esthetic Composite Restorations in Anterior Teeth: Managing Symmetry Strategies" Symmetry 13, no. 5: 797. https://doi.org/10.3390/sym13050797
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.