Spine Axial Presentation (SAP) is a new manual method of graphical spine presentation seen from the cephalad side. SAP can be obtained maually, without using a computer. The simplicity of this method and its high accessibility differs it from the “Top View” presented by De Smet [
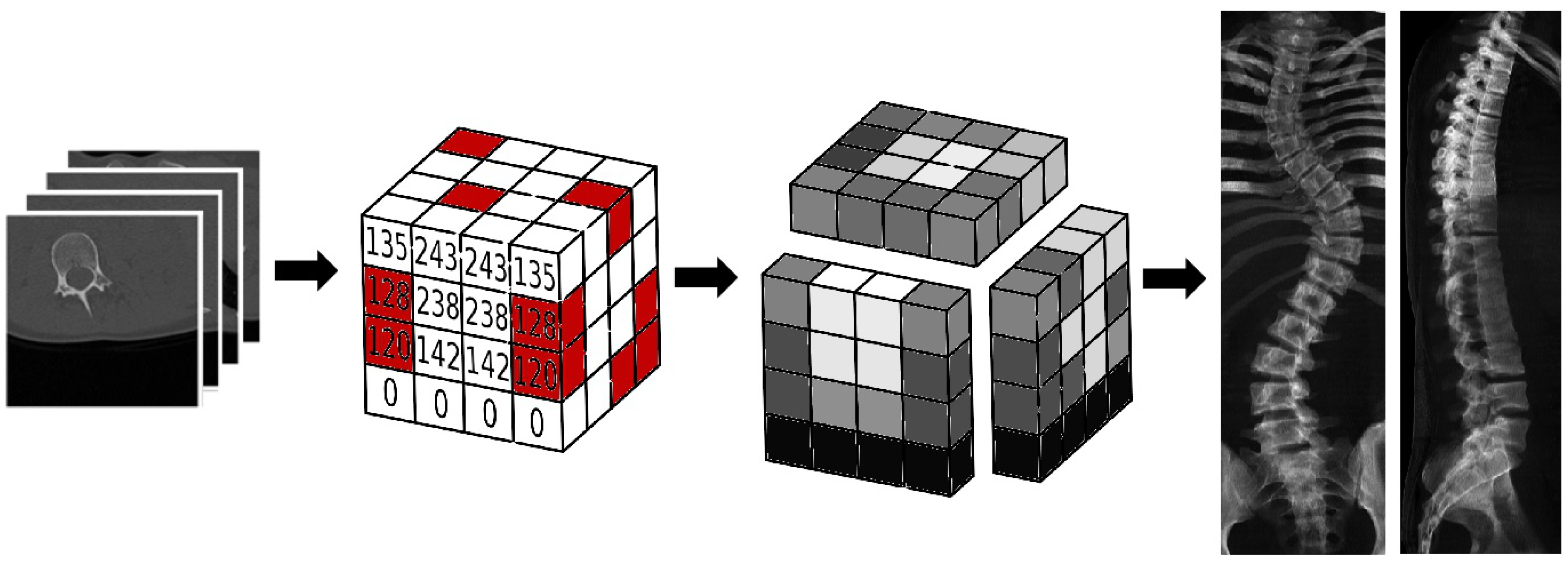
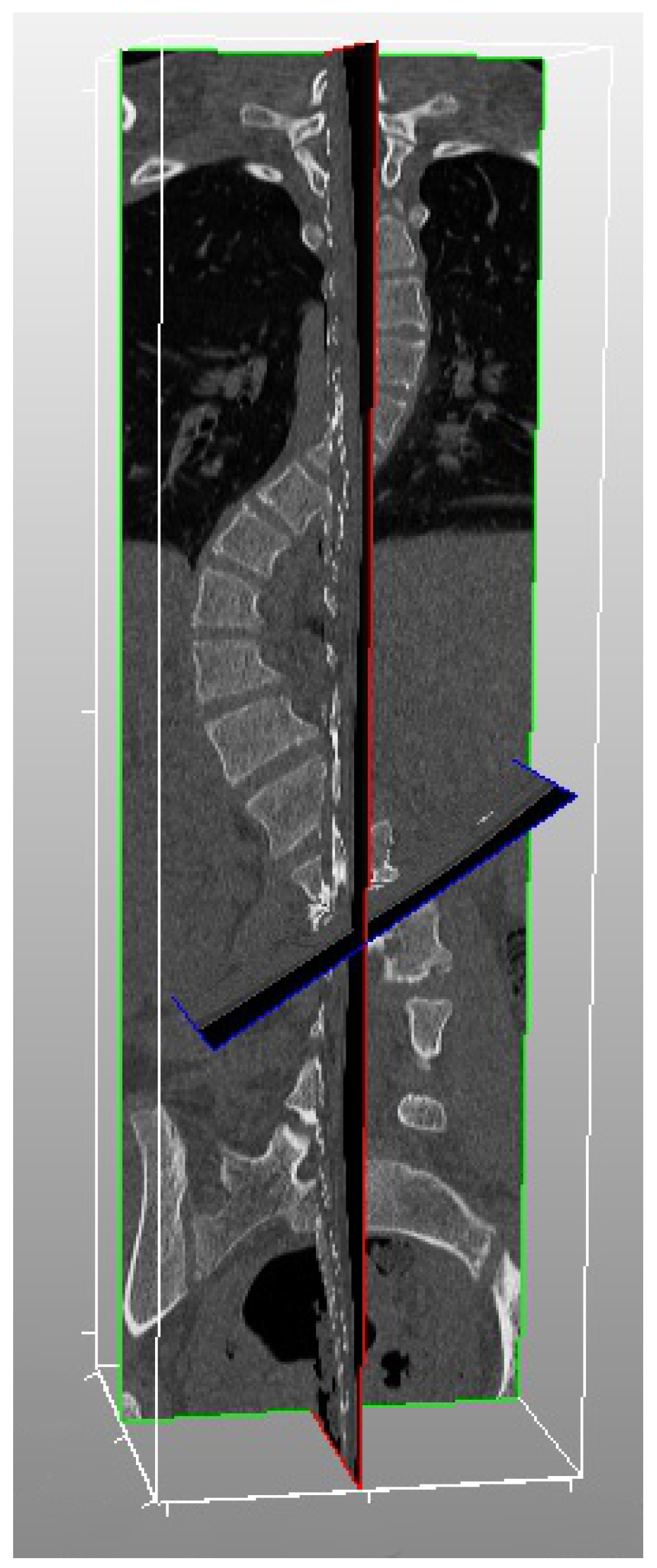
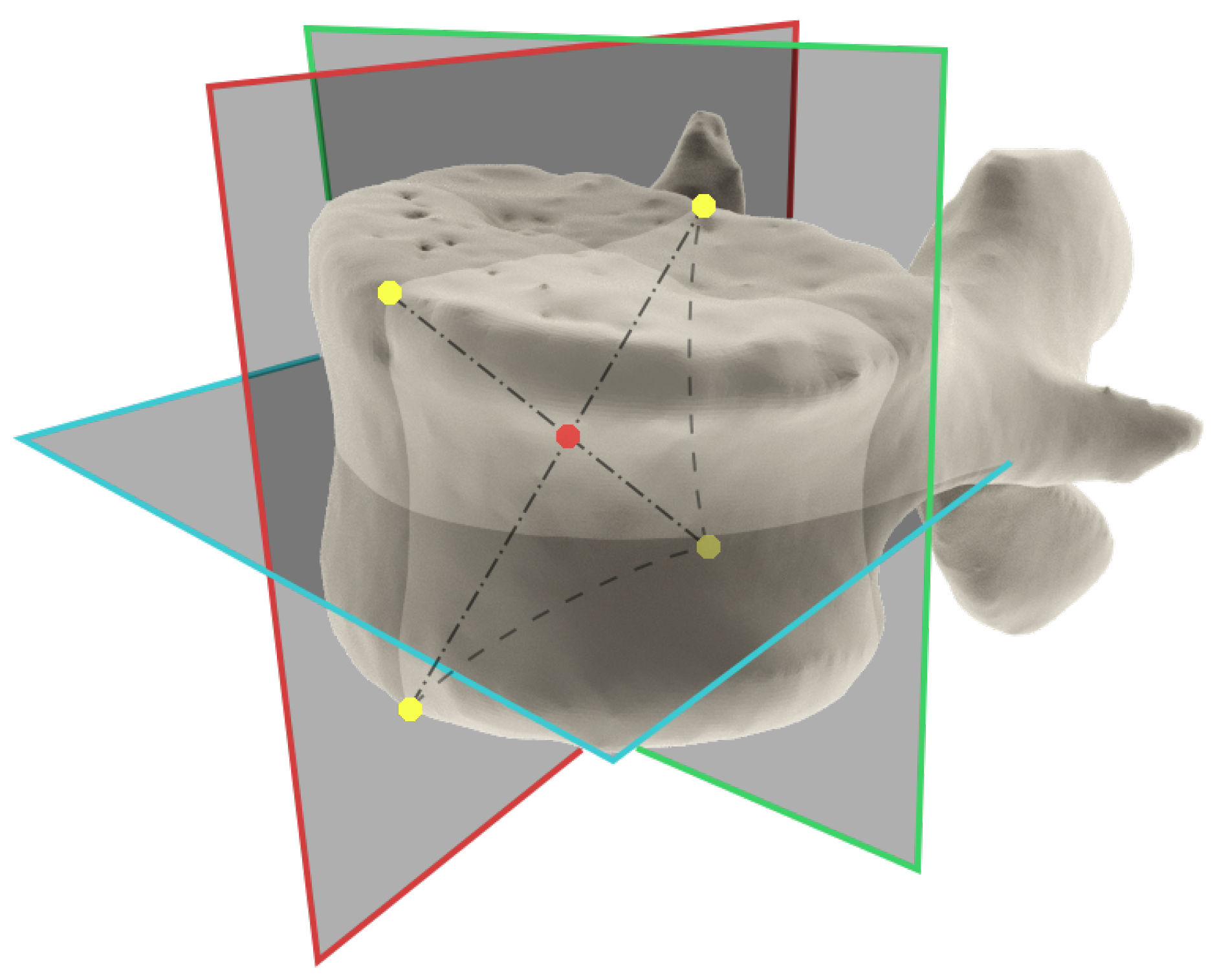
9]. CT scans are saved in DICOM file format. The information about location and spatial relations of structures is stored in form of voxels (a 3D pixels). The coordinates of voxels are predefined by the imaging system used. To obtain the central vertebral body points, one needs two sets of precise sections dissecting each vertebra. The section is not parallel to the upper or the lower vertebral lamina because the vertebra can be deformed by torsion [
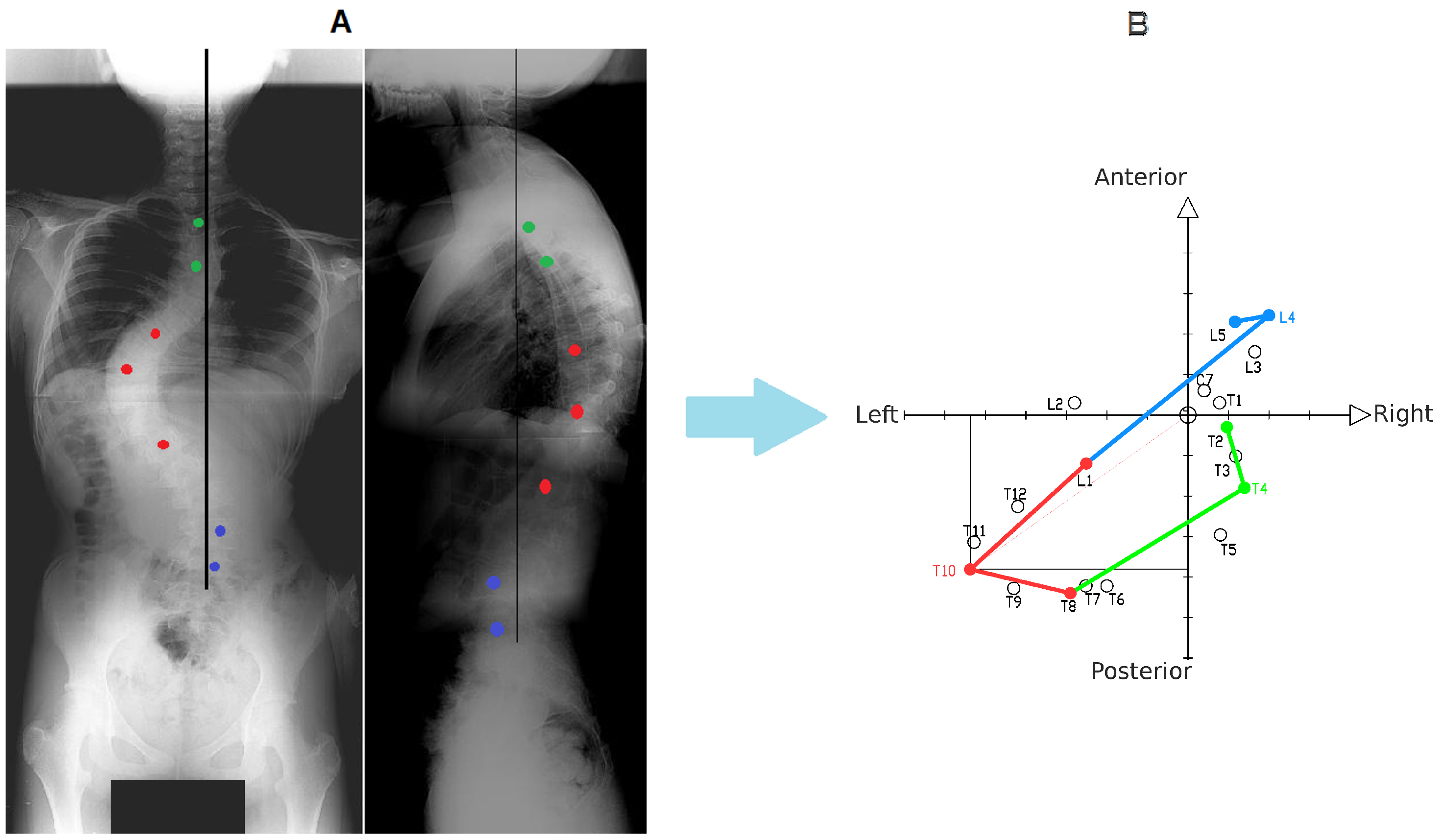
13]. In wedge shaped vertebra, the horizontal section parallel to the lower or the upper lamina does not dissect the vertebra body in half. The PNG file format was chosen for DRRs. PNG is a graphic data file format which uses lossless compression methods, as opposed to JPEG which loses some information and generates artifacts during compression. DEVIDE was used for vertebral column CT scans analysis. This software has the following characteristics: (1) it could present the vertebral column in three dissecting planes; (2) it allows marking points on each plane and extracting the coordinates; (3) it contains data export functionality (as separate file); (4) it supports DICOM and PNG files. The central vertebral points of lumbar part of the spinal column were easy to measure, even in case of scoliosis, on the X-rays. The size of lumbar vertebrae allow one to exactly mark their margins on both antero-posterior and sagittal images. Thoracic vertebrae are harder to asses because of the rib cage and bones of the upper extremity. Moreover when the angle of scoliosis is bigger one can observe that vertebral bodies can overlap on lateral images. Analysis of lateral images needed from observers a certain level of precision and knowledge in anatomical radiology. Analysis of AP images was much easier- even in severe scoliosis one can easily define the edges of vertebral bodies. The measurements of central vertebral points allow one to draw the Spine Axial Projection (SAP). SAP is a projection of spinal column onto the axial plane, it is a form of “Top View” [
12,
14,
15]. It is a presentation of vertebrae and their relations in space on axial plane. The central coordinate point of the SAP represents SVA and CSL. SVA and CSL represent the axis of compensated vertebral column; SAP allows to measure the direction and amount of deformation against SVA and CSL, so one can define the direction and the amount of the whole spinal column deformity. The Spine Axial Presentation shows as a True da Vinci Projection the localization and relationships between vertebrae and End Apical End planes (EAE-planes) [
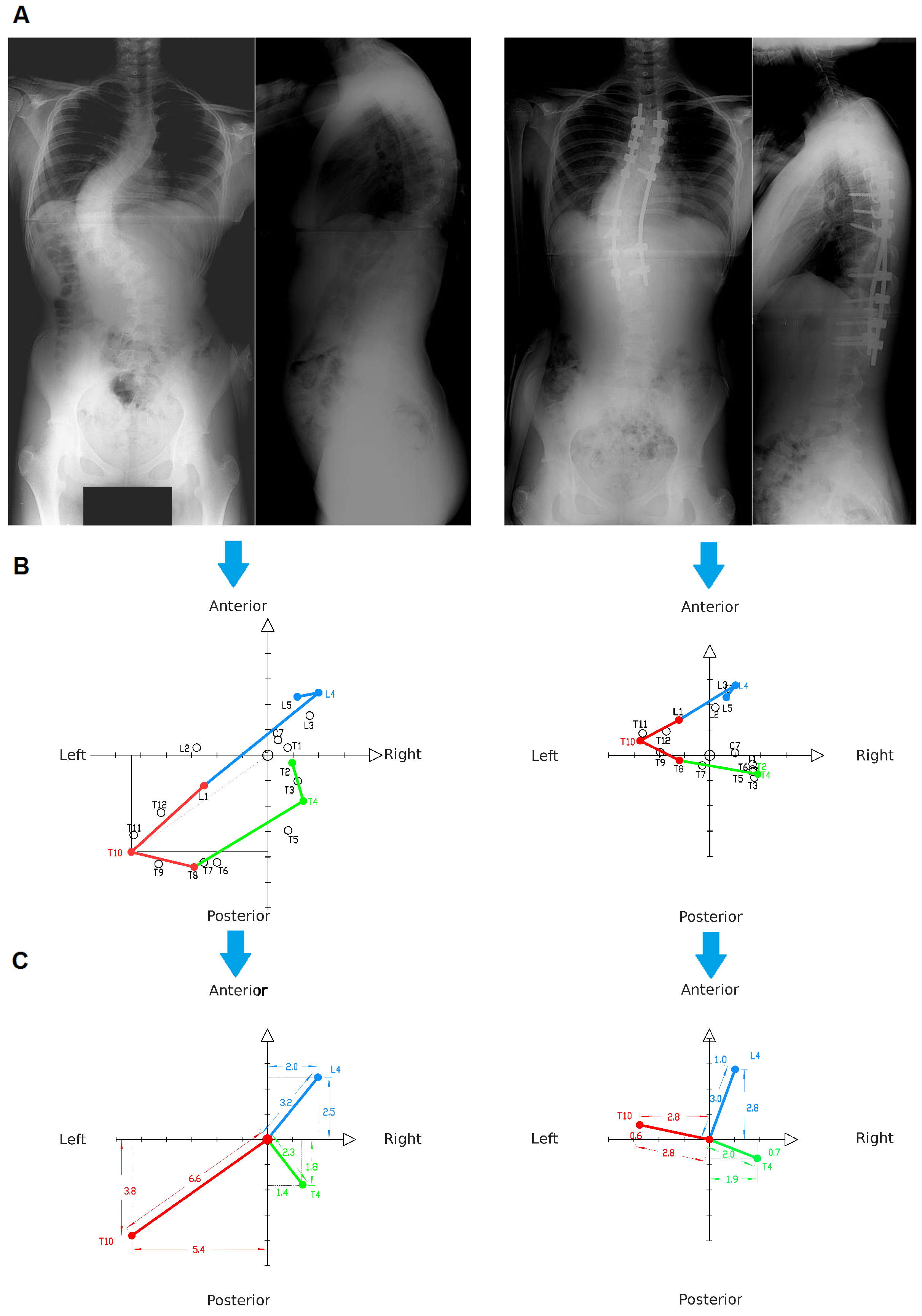
11]. As opposed to True da Vinci Projection, the SAP allows one to present the transverse top view of the spine without using the computer software. It could be done after measuring the distances between the central vertebral point, CSL and SVA. Spine Axial Presentation also provides information about the localization of EAE-planes. Drawing Spine Axial Presentation is time consuming, although it gives a surgeon additional information which, together with X-ray images, gives detailed knowledge of the whole deformity. It also allows patients to better understand their scoliotic deformities, so one can better explain planned treatment. Visual aids are important for good patient cooperation and patients’ improved understanding of their illness brings better patient outcomes. The patients are able to observe the deviation of vertebrae from their proper position and the direction in which the vertebrae are displaced (
Figure 6).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}