
Cochlear Implantation in Patients with Mitochondrial Gene Mutation: Decline in Speech Perception in Retrospective Long-Term Follow-Up Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Surgical Findings
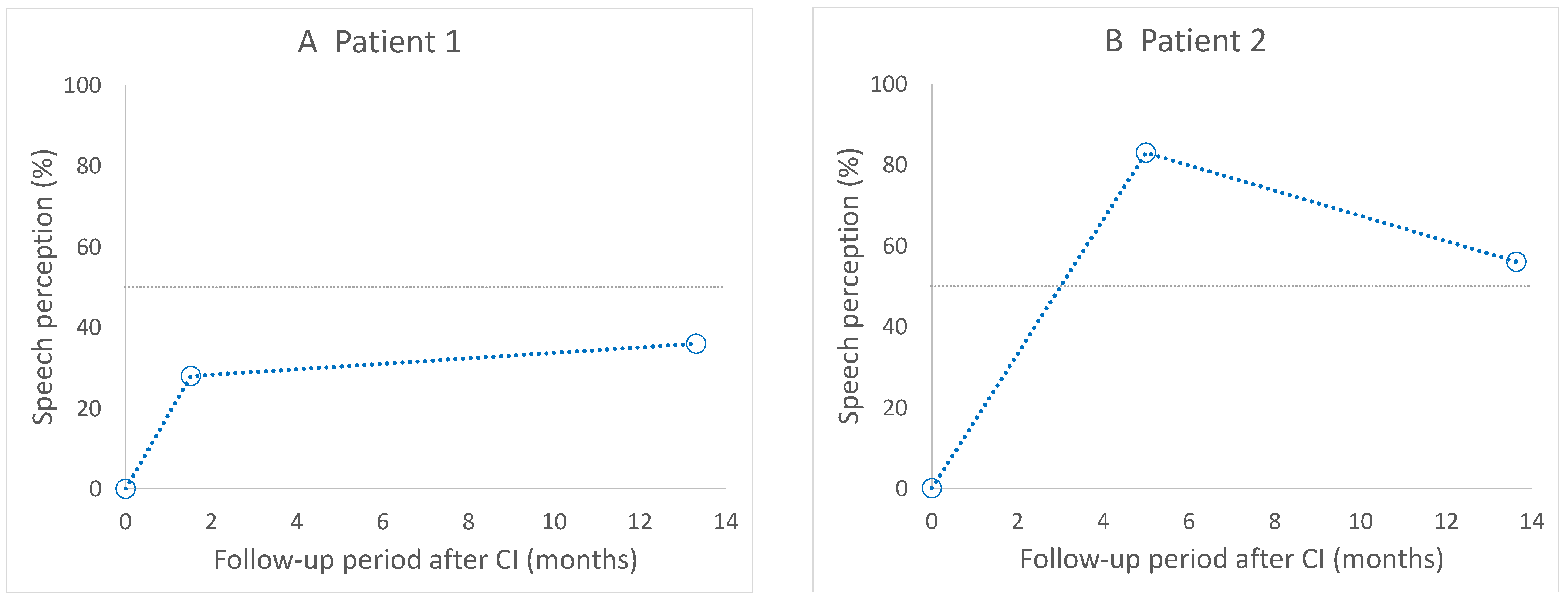
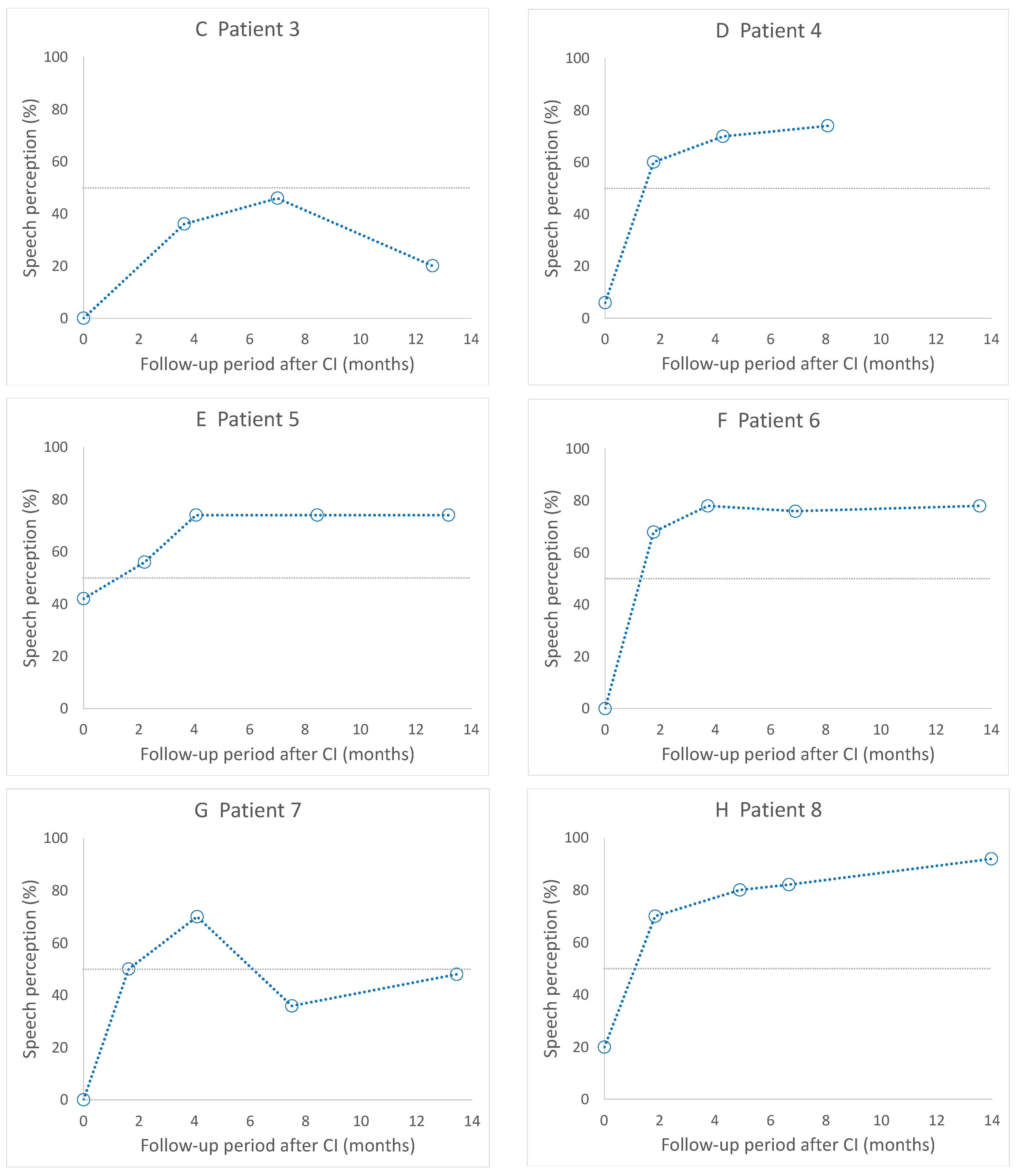
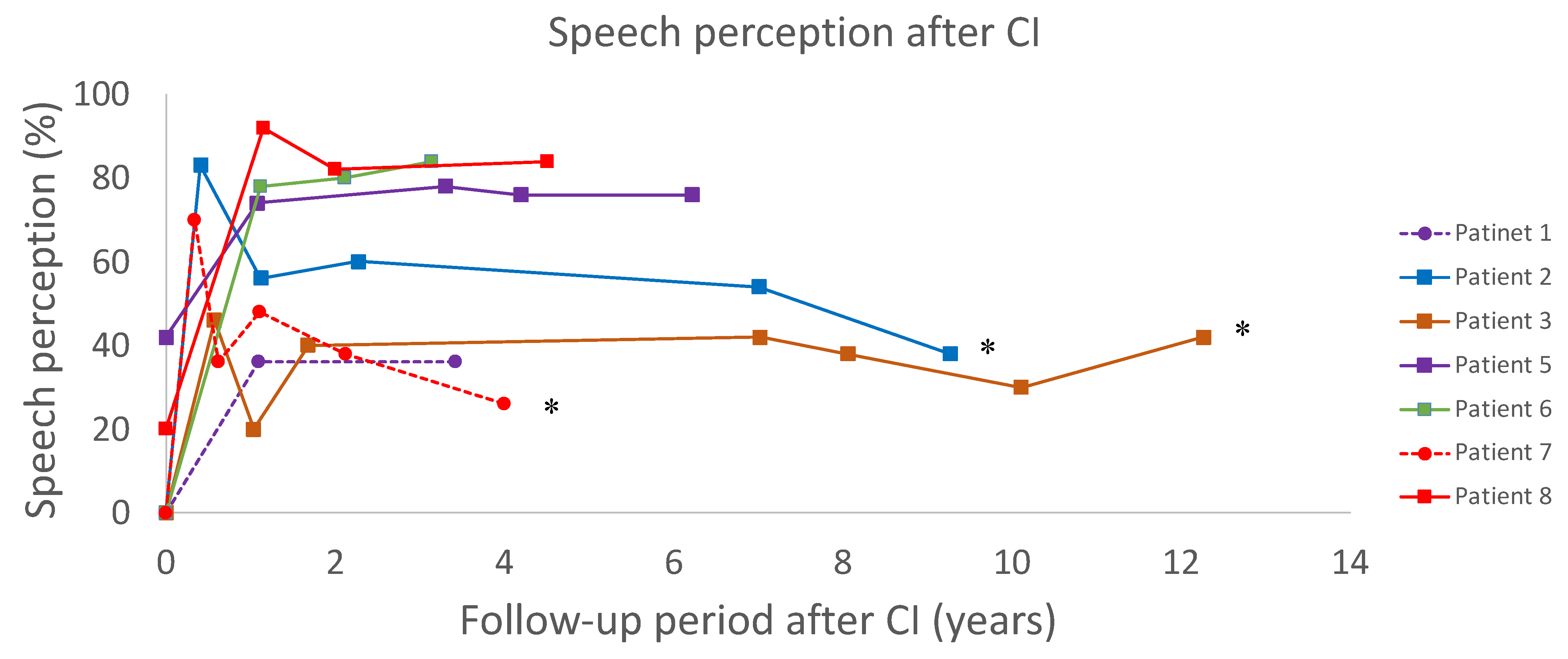
3.3. Postoperative Speech Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scarpelli, M.; Zappini, F.; Filosto, M.; Russignan, A.; Tonin, P.; Tomelleri, G. Mitochondrial sensorineural hearing loss: A retrospective study and a description of cochlear implantation in a MELAS patient. Genet. Res. Int. 2012, 2012, 287432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimauro, S.; Schon, E.A. Mitochondrial respiratory-chain diseases. N. Engl. J. Med. 2003, 348, 2656–2668. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.C. Diseases of the mitochondrial DNA. Ann. Rev. Biochem. 1992, 61, 1175–1212. [Google Scholar] [CrossRef]
- Chinnery, P.F.; Elliott, C.; Green, G.R.; Ress, A.; Coulthard, A.; Turnbull, D.M.; Griffiths, T.D. The spectrum of hearing loss due to mitochondrial DNA defects. Brain 2000, 123, 82–92. [Google Scholar] [CrossRef] [Green Version]
- Zwirner, P.; Wilichowski, E. Progressive sensorineural hearing loss in children with mitochondrial encephalomyopathies. Laryngoscope 2001, 111, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Sinnathuray, A.R.; Raut, V.; Awa, A.; Magee, A.; Toner, J.G. A review of cochlear implantation in mitochondrial sensorineural hearing loss. Otol. Neurotol. 2003, 24, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Kogelnik, A.M.; Lott, M.T.; Brown, M.D.; Navathe, S.B.; Wallace, D.C. MITOMAP: A human mitochondrial genome database. Nucleic Acids Res. 1996, 24, 177–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Servidei, S. Mitochondrial encephalomyopathies: Gene mutation. Neuromuscul. Disord. 2002, 12, 524–529. [Google Scholar] [CrossRef]
- Levinger, L.; Mörl, K.; Florentz, C. Mitochondrial TRNA 3′ end metabolism and human disease. Nucleic Acids Res. 2004, 32, 5430–5441. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Persi, E.; Lott, M.T.; Procaccio, V.; Poole, J.C.; Brandon, M.C.; Mishmar, D.; Yi, C.; Kreuziger, J.; Baldi, P.; Wallace, D.C. An enhanced MITOMAP with a global MtDNA mutational phylogeny. Nucleic Acids Res. 2004, 35, D823–D828. [Google Scholar] [CrossRef] [Green Version]
- Huizing, E.H.; de Groot, J.C. Human cochlear pathology in aminoglycoside ototoxicity—A review. Acta Otolaryngol. Suppl. 1987, 436, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Elverland, H.H.; Torbergsen, T. Audiologic findings in a family with mitochondrial disorder. Am. J. Otol. 1991, 12, 459–465. [Google Scholar] [PubMed]
- Lindsay, J.R.; Hinojosa, R. Histopathologic features of the inner ear associated with Kearns-Sayre syndrome. Arch. Otolaryngol. 1976, 102, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Sue, C.M.; Lipsett, L.J.; Crimmins, D.S.; Tsang, C.S.; Boyages, S.C.; Presgrave, C.M.; Gibson, W.P.; Byrne, E.; Morris, J.G. Cochlear origin of hearing loss in MELAS syndrome. Ann. Neurol. 1998, 43, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Yamasoba, T.; Oka, Y.; Tsukuda, K.; Nakamura, M.; Kaga, K. Auditory findings in patients with maternally inherited diabetes and deafness harboring a point mutation in the mitochondrial transfer RNA(Leu) (UUR) gene. Laryngoscope 1996, 106, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Tamagawa, Y.; Kitamura, K.; Hagiwara, H.; Ishida, T.; Nishizawa, M.; Saito, T.; Iwamoto, Y. Audiologic findings in patients with a point mutation at nucleotide 3243 of mitochondrial DNA. Ann. Otol. Rhinol. Laryngol. 1997, 106, 338–342. [Google Scholar] [CrossRef]
- Lupo, I.; Ciulla, L.; Cusimano, F.; Fierro, B.; Piccoli, F. Brainstem auditory evoked potentials in patients with mitochondrial encephalomyopathy. Acta Neurol. 1992, 14, 163–172. [Google Scholar]
- Vandana, V.P.; Bindu, P.S.; Sonam, K.; Govindaraj, P.; Taly, A.B.; Gayathri, N.; Chiplinkar, S.; Govindaraju, C.; Arvinda, H.R.; Nagappa, M.; et al. Audiological manifestations in mitochondrial encephalomyopathy lactic acidosis and stroke like episodes (MELAS) syndrome. Clin. Neurol. Neurosurg. 2016, 148, 17–21. [Google Scholar] [CrossRef]
- Di Mauro, S.; Schon, E.A. Mitochondrial disorders in the nervous system. Ann. Rev. Neurosci. 2008, 31, 91–123. [Google Scholar] [CrossRef]
- Roesch, S.; O’Sullivan, A.; Zimmermann, G.; Mair, A.; Lipuš, C.; Mayr, J.A.; Wortmann, S.B.; Rasp, G. Mitochondrial disease and hearing loss in children: A systematic review. Laryngoscope 2022, 1–14. [Google Scholar] [CrossRef]
- Takahashi, K.; Merchant, S.N.; Miyazawa, T.; Yamaguchi, T.; McKenna, M.J.; Kouda, H.; Iino, Y.; Someya, T.; Tamagawa, Y.; Takiyama, Y.; et al. Temporal bone histopathological and quantitative analysis of mitochondrial DNA in MELAS. Laryngoscope 2003, 113, 1362–1368. [Google Scholar] [CrossRef] [PubMed]
- Yamasoba, T.; Tsukuda, K.; Oka, Y.; Kobayashi, T.; Kaga, K. Cochlear histopathology associated with mitochondrial transfer RNA (Leu (UUR)) gene mutation. Neurology 1999, 52, 1705–1707. [Google Scholar] [CrossRef] [PubMed]
- Handzel, O.; Ungar, O.J.; Lee, D.J.; Nadol, J.B. Temporal bone histopathology in MELAS syndrome. Laryngoscope Investig. Otolaryngol. 2020, 5, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Kaga, K.; Nakamura, M.; Shinogami, M.; Tsuzuku, T.; Yamada, K.; Shindo, M. Auditory nerve disease of both ears revealed by auditory brainstem responses, electrocochleography and otoacoustic emissions. Scand. Audiol. 1996, 25, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Starr, A.; Picton, T.W.; Sininger, Y.; Hood, L.J.; Berlin, C.I. Auditory neuropathy. Brain A J. Neurol. 1996, 119, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Leruez, S.; Milea, D.; Defoort-Dhellemmes, S.; Colin, E.; Crochet, M.; Procaccio, V.; Ferré, M.; Lamblin, J.; Drouin, V.; Vincent-Delorme, C.; et al. Sensorineural hearing loss in OPA1-linked disorders. Brain A J. Neurol. 2013, 136, e236. [Google Scholar] [CrossRef]
- Sakai, Y.; Kaga, K.; Kodama, K.; Higuchi, A.; Miyamoto, J. Hearing evaluation in two sisters with a T8993G point mutation of mitochondrial DNA. Int. J. Pediatric Otorhinolaryngol. 2004, 68, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Himi, T.; Harabuchi, Y.; Hamamoto, M.; Kataura, A. Cochlear implantation in a patient with mitochondrial disease-Kearns-Sayre syndrome: A case report. Adv. Otorhinolaryngol. 1997, 52, 321–323. [Google Scholar] [CrossRef] [Green Version]
- Cullington, H.E. Cochlear implantation of a deaf blind patient with mitochondrial cytopathy. J. Laryngol. Otol. 1999, 113, 353–354. [Google Scholar] [CrossRef]
- Counter, P.R.; Hilton, M.P.; Webster, D.; Wardell, T.; Taylor, R.W.; Besley, G.; Turnbull, D.M.; Robinson, P.J. Cochlear implantation of a patient with a previously undescribed mitochondrial DNA defect. J. Laryngol. Otol. 2001, 115, 730–732. [Google Scholar] [CrossRef]
- Hill, D.; Wintersgill, S.; Scott, L.; Cadge, B.; Graham, J. Cochlear implantation in a profoundly deaf patient with MELAS syndrome. J. Neurosurg. Psychiatry 2001, 71, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raut, V.; Sinnathuray, A.R.; Toner, J.G. Cochlear implantation in a maternal inherited diabetes and deafness syndrome. J. Laryngol. Otol. 2002, 116, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Karkos, P.D.; Anari, S.; Johnson, I.J. Cochlear implantation in patients with MELAS syndrome. Eur. Arch. Otorhinolaryngol. 2005, 262, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Li, J.N.; Han, D.Y.; Ji, F.; Chen, A.T.; Wu, N.; Xi, X.; Shen, W.D.; Yang, S.M. Successful cochlear implantation in a patient MNGIE syndrome. Acta Otolaryngol. 2011, 131, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Nishizaki, K.; Fukushima, K.; Oda, Y.; Masuda, A.; Hayashi, S.; Nagayasu, N.; Yoshino, T.; Kashihara, K.; Takahashi, K.; Masuda, Y. Cochlear implantation for symptomatic hereditary deafness. Acta Otolaryngol. Suppl. 1999, 540, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Howes, T.; Madden, C.; Dasgupta, S.; Saeed, S.; Das, V. Role of mitochondrial variation in maternally inherited diabetes and deafness syndrome. J. Laryngol. Otol. 2008, 122, 1249–1252. [Google Scholar] [CrossRef]
- Yasumura, S.; Aso, S.; Fujisaka, M.; Watanabe, Y. Cochlear implantation in a patient with mitochondrial encephalopathy, lactic acidosis and stroke-like episodes syndrome. Acta Otolaryngol. 2003, 123, 55–58. [Google Scholar] [CrossRef]
- Yamamoto, N.; Okuyama, H.; Hiraumi, H.; Sakamoto, T.; Matsuura, H.; Ito, J. The outcome of cochlear implantation for mitochondrial disease patients with syndromic hearing loss. Otol. Neurotol. 2015, 36, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Nawal, Z.; Yasmin, N.; Jameel, M.; Peter, K.; Peter, M.; Manohar, B. Cochlear implantation outcomes in patients with mitochondrial hearing loss: A systematic review and narrative synthesis. J. Int. Adv. Otol. 2021, 17, 72–80. [Google Scholar] [CrossRef]
- Rosenthal, E.L.; Kileny, P.R.; Boerst, A.; Telian, S.A. Successful cochlear implantation in a patient with MELAS syndrome. Am. J. Otol. 1999, 20, 187–190. [Google Scholar]
- Pijl, S.; Westerberg, B.D. Cochlear implantation results in patients with Kearns-Sayre syndrome. Ear Hear. 2008, 29, 472–475. [Google Scholar] [CrossRef] [PubMed]
- Hilly, O.; Hwang, E.; Smith, L.; Shipp, D.; Nedzelski, J.M.; Chen, J.M.; Lin, V.W.Y. Cochlear implantation in elderly patients: Stability of outcome over time. J. Laryngol. Otol. 2016, 130, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Dillon, M.T.; Buss, E.; Adunka, M.C.; King, E.R.; Pillsbury, H.C.; Adunka, O.F.; Buchman, C.A. Long-term speech perception in elderly cochlear implant users. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 279–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffin, C.V.; Tyler, R.S.; Witt, S.A.; Dunn, C.C.; Gantz, B.J.; Rubinstein, J.T. Long-term performance of Clarion 1.0 cochlear implant users. Laryngoscope 2007, 117, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Breneman, A.I.; Gifford, R.H.; de Jong, M.D. Cochlear implantation in children with auditory neuropathy spectrum disorder: Long-term outcomes. J. Am. Acad. Audiol. 2012, 23, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, A.; Chaudhry, D.; Muzaffar, J.; Crundwell, G.; Monksfield, P.; Bance, M. Outcomes of cochlear implantation in patients with superficial siderosis: A systematic review and narrative synthesis. J. Int. Adv. Otol. 2020, 16, 443–455. [Google Scholar] [CrossRef]
- Yang, Z.; Cosetti, M. Safety and outcomes of cochlear implantation in the elderly: A review of recent literature. J. Otol. 2016, 11, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Mosnier, I.; Bebear, J.-P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artières, F.; Bordure, P.; Robier, A.; et al. Predictive factors of cochlear implant outcomes in the elderly. Audiol. Neuro-Otol. 2014, 19, 15–20. [Google Scholar] [CrossRef]
- Finsterer, J. Central nervous system manifestations of mitochondrial disorders. Acta Neurol Scand. 2006, 114, 217–238. [Google Scholar] [CrossRef]
- Iizuka, T.; Sakai, F.; Endo, M.; Suzuki, N. Response to sumatriptan in headache of MELAS syndrome. Neurology 2003, 61, 577–578. [Google Scholar] [CrossRef]
- Yamasoba, T.; Goto, Y.; Komaki, H.; Mimaki, M.; Sudo, A.; Suzuki, M. Cochlear damage due to germanium-induced mitochondrial dysfunction in guinea pigs. Neurosci. Lett. 2006, 395, 18–22. [Google Scholar] [CrossRef] [PubMed]
- De Laat, P.; Rodenburg, R.R.; Roeleveld, N.; Koene, S.; Smeitink, J.A.; Janssen, M.C. Six-year prospective follow-up study in 151 carriers of the mitochondrial DNA 3243 A > G variant. J. Med. Genet. 2021, 58, 48–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Disease | Causative Mutations | Age of Onset of Hearing Loss (years) | Age of Becoming Deaf (years) | Age at CI (years) | Observation Period (years) | Associated Symptoms |
|---|---|---|---|---|---|---|---|
| 1 | MIDD | A3243G | 30 | 53 | 53 | 3.4 | diabetes |
| 2 | MIDD | A3243G | 32 | 46 | 46 | 13 | diabetes |
| 3 | MIDD | A3243G | 38 | 44 | 44 | 12.2 | diabetes |
| 4 | MIDD | A3243G | 27 | 64 | 64 | 1.2 | diabetes |
| 5 | MIDD | A3243G | 10 | 50 | 51 | 6.2 | diabetes |
| 6 | MIDD | A3243G | 14 | 36 | 37 | 3.1 | diabetes |
| 7 | MELAS | A3243G | 10 | 44 | 46 | 4.0 | myopathy, lactic acidosis, stroke-like episode |
| 8 | − | A8296G | 7 | 21 | 22 | 4.5 | - |
| 9 | CPEO | RRM2Bs | 5 | 43 | 43 | 2.2 | mild external ophthalmoplegia |
| Patient | Tested Year (Years after CI) | In Quiet (%) | S/N20 (%) | S/N10 (%) |
|---|---|---|---|---|
| 4 | 5.2 | 45 | 20 | - |
| 5 | 1.3 | 95 | 95 | 58 |
| 3.9 | 100 | 95 | 78 | |
| 6 | 1.5 | 98 | 97 | 73 |
| 8 | 1.5 | 98 | 100 | 57 |
| 3 | 100 | 92 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanemoto, K.; Kashio, A.; Ogata, E.; Akamatsu, Y.; Koyama, H.; Uranaka, T.; Hoshi, Y.; Iwasaki, S.; Yamasoba, T. Cochlear Implantation in Patients with Mitochondrial Gene Mutation: Decline in Speech Perception in Retrospective Long-Term Follow-Up Study. Life 2022, 12, 482. https://doi.org/10.3390/life12040482
Kanemoto K, Kashio A, Ogata E, Akamatsu Y, Koyama H, Uranaka T, Hoshi Y, Iwasaki S, Yamasoba T. Cochlear Implantation in Patients with Mitochondrial Gene Mutation: Decline in Speech Perception in Retrospective Long-Term Follow-Up Study. Life. 2022; 12(4):482. https://doi.org/10.3390/life12040482
Chicago/Turabian StyleKanemoto, Kai, Akinori Kashio, Erika Ogata, Yusuke Akamatsu, Hajime Koyama, Tsukasa Uranaka, Yujiro Hoshi, Shinichi Iwasaki, and Tatsuya Yamasoba. 2022. "Cochlear Implantation in Patients with Mitochondrial Gene Mutation: Decline in Speech Perception in Retrospective Long-Term Follow-Up Study" Life 12, no. 4: 482. https://doi.org/10.3390/life12040482