
Ovarian Tissue Cryopreservation versus Other Fertility Techniques for Chemoradiation-Induced Premature Ovarian Insufficiency in Women: A Systematic Review and Future Directions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Eligibility Criteria
2.2. Identification and Selection of Studies
2.3. Data Collection and Study Appraisal
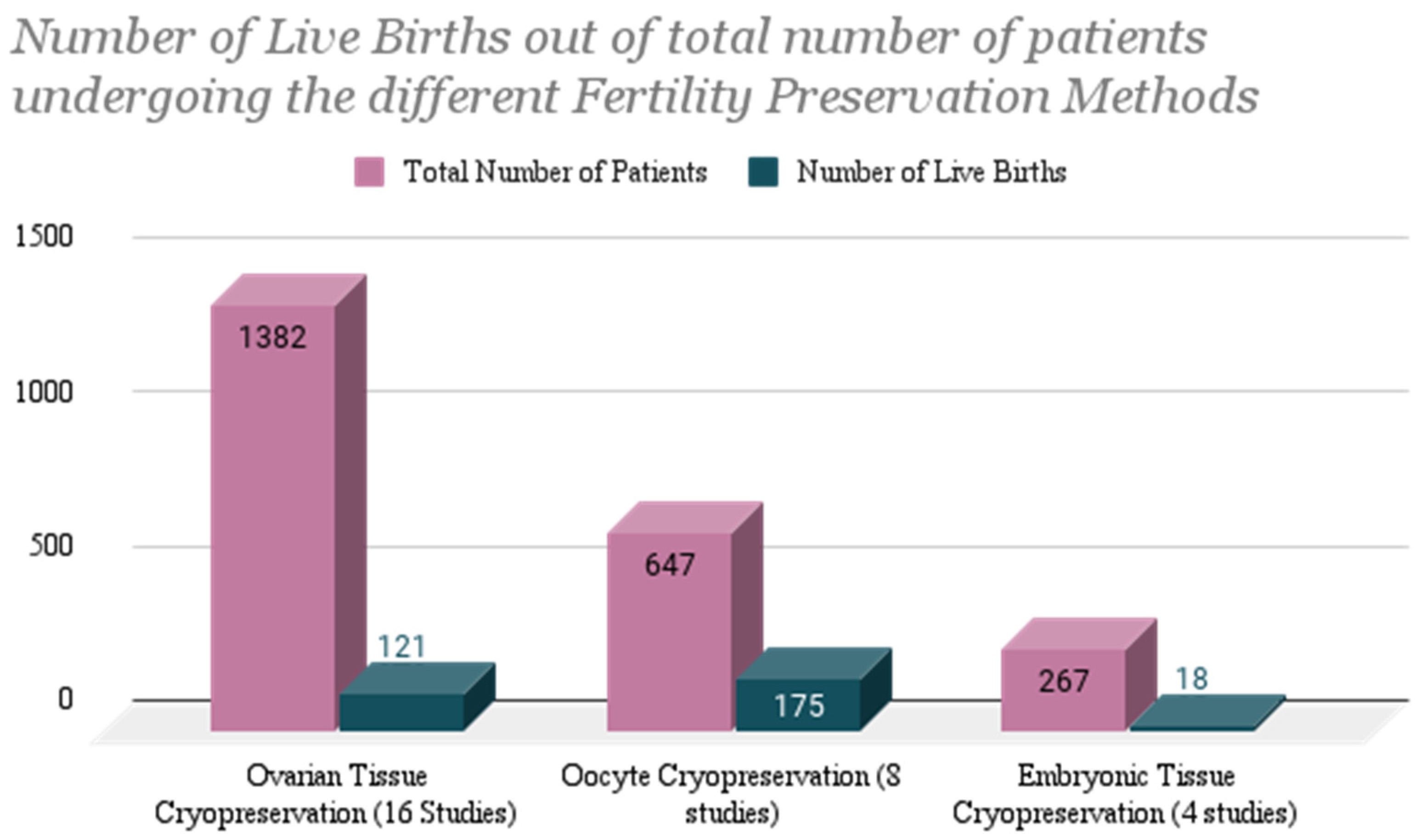
3. Results
3.1. Ovarian Tissue Cryopreservation (OTC)
3.2. Oocyte Cryopreservation (OC)
3.3. Embryonic Tissue Cryopreservation (ETC)
4. Discussion
- Comparative retrospective studies in the various methods of fertility preservation, i.e., embryo cryopreservation, oocyte cryopreservation, and ovarian tissue cryopreservation are needed to evaluate outcomes in a uniform population.
- Prospective information regarding markers of ovarian reserve before and after transplantation, as well as utilization of fertility preservation procedures, reasons why there is little uptake of fertility preservation, the utilization of assisted reproductive technology after transplantation, and understanding of the reasons why so few patients who do engage in fertility preservation before transplantation ever opt for using their cryopreserved tissues.
- Novel strategies to prevent or treat chemoradiation-induced ovarian insufficiency including primordial follicle maturation techniques and regenerative medicine (e.g., stromal cells, iPSC) as well as bioengineered ovaries should be tested in clinical trials.
- Though the risk of fertility loss is highest in young patients undergoing HSCT (where typically 12–14 cGys of ionizing total body irradiation is used along with massive chemotherapy), prospective studies in this population are extremely rare. Most of the data comes from case reports and retrospective studies. Thus, prospective trials in HSCT are critically needed.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedoschi, G.; Navarro, P.A.; Oktay, K. Chemotherapy-induced damage to ovary: Mechanisms and clinical impact. Future Oncol. 2016, 12, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Wallace, W.H.B.; Anderson, R.A.; Irvine, D.S. Fertility preservation for young patients with cancer: Who is at risk and what can be offered? Lancet Oncol. 2005, 6, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Azarbaijani, B.A.; Sheikhi, M.; Oskam, I.C.; Nurmio, M.; Laine, T.; Tinkanen, H.; Mäkinen, S.; Tanbo, T.G.; Hovatta, O.; Jahnukainen, K. Effect of Previous Chemotherapy on the Quality of Cryopreserved Human Ovarian Tissue In Vitro. PLoS ONE 2015, 10, e0133985. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Del Mastro, L.; Pescio, M.C.; Andersen, C.Y.; Azim, H.A.; Peccatori, F.A.; Costa, M.; Revelli, A.; Salvagno, F.; Gennari, A.; et al. Cancer and fertility preservation: International recommendations from an expert meeting. BMC Med. 2016, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy: A committee opinion. Fertil. Steril. 2019, 112, 1022–1033. [Google Scholar] [CrossRef] [PubMed]
- Loren, A.W.; Mangu, P.B.; Beck, L.N.; Brennan, L.; Magdalinski, A.J.; Partridge, A.H.; Quinn, G.; Wallace, W.H.; Oktay, K. Fertility Preservation for Patients with Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 2500–2510. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.; Baysal, Ö.; Nelen, W.L.D.M.; Braat, D.D.M.; Beerendonk, C.C.M.; Hermens, R.P.M.G. Professionals’ barriers in female oncofertility care and strategies for improvement. Hum. Reprod. 2019, 34, 1074–1082. [Google Scholar] [CrossRef]
- Salama, M.; Anazodo, A.; Woodruff, T.K. Preserving fertility in female patients with hematological malignancies: The key points. Expert Rev. Hematol. 2019, 12, 375–377. [Google Scholar] [CrossRef]
- Burns, K.C.; Hoefgen, H.; Strine, A.; Dasgupta, R. Fertility preservation options in pediatric and adolescent patients with cancer. Cancer 2018, 124, 1867–1876. [Google Scholar] [CrossRef]
- Behl, S.; Joshi, V.B.; Hussein, R.S.; Walker, D.L.; Lampat, K.L.; Krenik, A.G.; Barud, K.M.; Fredrickson, J.R.; Galanits, T.M.; Rian, K.J.; et al. Consult and procedure incidence outcomes following establishment of a fertility preservation program for children with cancer. J. Assist. Reprod. Genet. 2021, 38, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Montori, V.M.; Ioannidis, J.P.A.; Jaeschke, R.; Devereaux, P.J.; Prasad, K.; Neumann, I.; Carrasco-Labra, A.; Agoritsas, T.; Hatala, R.; et al. How to Read a Systematic Review and Meta-analysis and Apply the Results to Patient Care: Users’ Guides to the Medical Literature. JAMA 2014, 312, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.A.; Reed, D.A. Appraising the quality of medical education research methods: The Medical Education Research Study Quality Instrument and the Newcastle-Ottawa Scale-Education. Acad. Med. 2015, 90, 1067–1076. [Google Scholar] [CrossRef] [PubMed]
- Sigismondi, C.; Papaleo, E.; Vigano, P.; Vailati, S.; Candiani, M.; Ottolina, J.; Di Mattei, V.E.; Mangili, G. Fertility preservation in female cancer patients: A single center experience. Chin. J. Cancer 2015, 34, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Wallberg, K.A.; Marklund, A.; Lundberg, F.; Wikander, I.; Milenkovic, M.; Anastacio, A.; Sergouniotis, F.; Wånggren, K.; Ekengren, J.; Lind, T.; et al. A prospective study of women and girls undergoing fertility preservation due to oncologic and non-oncologic indications in Sweden-Trends in patients’ choices and benefit of the chosen methods after long-term follow up. Acta Obstet. Gynecol. Scand. 2019, 98, 604–615. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Goldrat, O.; Ferreira, A.; Dechene, J.; Jr, H.A.; Desir, J.; Delbaere, A.; de Roodenbeke, M.-D.T.; de Azambuja, E.; Ignatiadis, M.; et al. Reproductive potential and performance of fertility preservation strategies in BRCA-mutated breast cancer patients. Ann. Oncol. 2018, 29, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, C.E.; Brady, B.M.; McLaughlin, M.; Telfer, E.E.; White, J.; Cowie, F. Re-implantation of cryopreserved ovarian cortex resulting in restoration of ovarian function, natural conception and successful pregnancy after haematopoietic stem cell transplantation for Wilms tumor. J. Assist. Reprod. Genet. 2016, 33, 1615–1620. [Google Scholar] [CrossRef]
- Dittrich, R.; Hackl, J.; Lotz, L.; Hoffmann, I.; Beckmann, M.W. Pregnancies and live births after 20 transplantations of cryopreserved ovarian tissue in a single center. Fertil. Steril. 2015, 103, 462–468. [Google Scholar] [CrossRef]
- Oktay, K.; Bedoschi, G.; Pacheco, F.; Turan, V.; Emirdar, V. First pregnancies, live birth, and in vitro fertilization outcomes after transplantation of frozen-banked ovarian tissue with a human extracellular matrix scaffold using robot-assisted minimally invasive surgery. Am. J. Obstet. Gynecol. 2016, 214, 94.e1–94.e9. [Google Scholar] [CrossRef]
- Babayev, S.N.; Arslan, E.; Kogan, S.; Moy, F.; Oktay, K. Evaluation of ovarian and testicular tissue cryopreservation in children undergoing gonadotoxic therapies. J. Assist. Reprod. Genet. 2013, 30, 3–9. [Google Scholar] [CrossRef]
- Rodriguez-Wallberg, K.A.; Tanbo, T.; Tinkanen, H.; Thurin-Kjellberg, A.; Nedstrand, E.; Kitlinski, M.L.; Macklon, K.T.; Ernst, E.; Fedder, J.; Tiitinen, A.; et al. Ovarian tissue cryopreservation and transplantation among alternatives for fertility preservation in the Nordic countries—Compilation of 20 years of multicenter experience. Acta Obstet. Gynecol. Scand. 2016, 95, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Wallberg, K.A.; Karlström, P.; Rezapour, M.; Castellanos, E.; Hreinsson, J.; Rasmussen, C.; Sheikhi, M.; Ouvrier, B.; Bozóky, B.; Olofsson, J.I.; et al. Full-term newborn after repeated ovarian tissue transplants in a patient treated for Ewing sarcoma by sterilizing pelvic irradiation and chemotherapy. Acta Obstet. Gynecol. Scand. 2015, 94, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Poirot, C.; Brugieres, L.; Yakouben, K.; Prades-Borio, M.; Marzouk, F.; de Lambert, G.; Pacquement, H.; Bernaudin, F.; Neven, B.; Paye-Jaouen, A.; et al. Ovarian tissue cryopreservation for fertility preservation in 418 girls and adolescents up to 15 years of age facing highly gonadotoxic treatment—Twenty years of experience at a single center. Acta Obstet. Gynecol. Scand. 2019, 98, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Taylan, E.; Kawahara, T.; Cillo, G.M. Robot-assisted orthotopic and heterotopic ovarian tissue transplantation techniques: Surgical advances since our first success in 2000. Fertil. Steril. 2019, 111, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Peek, R.; Westphal, J.R.; van Dongen, A.J.C.M.; Loonen, J.J.; Braat, D.D.M.; Beerendonk, C.C.M. Fertility Preservation by Ovarian Tissue Cryopreservation after Limited Gonadotoxic Chemotherapy in a 10-Year-Old Ewing Sarcoma Patient. J. Adolesc. Young Adult Oncol. 2014, 3, 92–95. [Google Scholar] [CrossRef]
- Dorez, M.; Delotte, J.; Thibault, E.; Ciuca, S.; Mounier, N.; Bongain, A. Laparoscopic single-site ovariectomy: An indication of choice for ovarian cryopreservation. Grand. Rounds 2013, 13, 1–3. [Google Scholar] [CrossRef]
- Chambon, F.; Brugnon, F.; Grèze, V.; Grémeau, A.-S.; Pereira, B.; Déchelotte, P.; Kanold, J. Cryopreservation of ovarian tissue in pediatric patients undergoing sterilizing chemotherapy. Hum. Fertil. 2016, 19, 23–31. [Google Scholar] [CrossRef]
- Goeckenjan, M.; Rösner, S.; Toth, B.; Strowitzki, T.; Germeyer, A. Successful controlled ovarian stimulation despite elevated hCG levels after first-trimester abortion in the context of fertility preservation. Gynecol. Endocrinol. 2013, 29, 960–962. [Google Scholar] [CrossRef]
- Dolmans, M.M.; von Wolff, M.; Poirot, C.; Diaz-Garcia, C.; Cacciottola, L.; Boissel, N.; Liebenthron, J.; Pellicer, A.; Donnez, J.; Andersen, C.Y. Transplantation of cryopreserved ovarian tissue in a series of 285 women: A review of five leading European centers. Fertil. Steril. 2021, 115, 1102–1115. [Google Scholar] [CrossRef]
- Hashimoto, T.; Nakamura, Y.; Obata, R.; Doshida, M.; Toya, M.; Takeuchi, T.; Kyono, K. Effects of fertility preservation in patients with breast cancer: A retrospective two-centers study. Reprod. Med. Biol. 2017, 16, 374–379. [Google Scholar] [CrossRef]
- Perrin, J.; Saïas-Magnan, J.; Broussais, F.; Bouabdallah, R.; D’Ercole, C.; Courbiere, B. First French live-birth after oocyte vitrification performed before chemotherapy for fertility preservation. J. Assist. Reprod. Genet. 2016, 33, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, Z.; Zur, H.; Dann, E.J. Gonadotropin-Releasing Hormone Agonist Cotreatment during Chemotherapy May Increase Pregnancy Rate in Survivors. Oncologist 2015, 20, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, C.C.; Marinho, V.F.W.; Campos, A.L.M.; Guedes, J.D.S.; Xavier, .B.D.S.; Caetano, J.P.J.; Marinho, R.M. Oocyte cryopreservation for future fertility: Comparison of ovarian response between cancer and non-cancer patients. JBRA Assist. Reprod. 2019, 23, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Chien, A.J.; Chambers, J.; Mcauley, F.; Kaplan, T.; Letourneau, J.; Hwang, J.; Kim, M.-O.; Melisko, M.E.; Rugo, H.S.; Esserman, L.J.; et al. Fertility preservation with ovarian stimulation and time to treatment in women with stage II-III breast cancer receiving neoadjuvant therapy. Breast Cancer Res. Treat. 2017, 165, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Oktem, O.; Oktay, K. Preservation of Menstrual Function in Adolescent and Young Females. Ann. N. Y. Acad. Sci. 2008, 1135, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Peyser, A.; Bristow, S.L.; Hershlag, A. Two successful pregnancies following fertility preservation in a patient with anaplastic astrocytoma: A case report. BMC Cancer 2018, 18, 544. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.; Durant, J.F.; Camboni, A.; Gilliaux, S.; Amorim, C.A.; Van Langendonckt, A.; Irenge, L.M.; Gala, J.L.; Donnez, J.; Dolmans, M.M. Is transplantation of cryopreserved ovarian tissue from patients with advanced-stage breast cancer safe? A pilot study. J. Assist. Reprod. Genet. 2013, 30, 1289–1299. [Google Scholar] [CrossRef]
- Sklar, C.A.; Mertens, A.C.; Mitby, P.; Whitton, J.; Stovall, M.; Kasper, C.; Mulder, J.; Green, D.; Nicholson, H.S.; Yasui, Y.; et al. Premature menopause in survivors of childhood cancer: A report from the childhood cancer survivor study. J. Natl. Cancer Inst. 2006, 98, 890–896. [Google Scholar] [CrossRef]
- Mahajan, N. Fertility preservation in female cancer patients: An overview. J. Hum. Reprod. Sci. 2015, 8, 3–13. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M. Fertility Preservation in Women. N. Engl. J. Med. 2017, 377, 1657–1665. [Google Scholar] [CrossRef]
- Demeestere, I.; Simon, P.; Dedeken, L.; Moffa, F.; Tsépélidis, S.; Brachet, C.; Delbaere, A.; Devreker, F.; Ferster, A. Live birth after autograft of ovarian tissue cryopreserved during childhood. Hum. Reprod. 2015, 30, 2107–2109. [Google Scholar] [CrossRef] [PubMed]
- Matthews, S.J.; Picton, H.; Ernst, E.; Andersen, C.Y. Successful pregnancy in a woman previously suffering from β-thalassemia following transplantation of ovarian tissue cryopreserved before puberty. Minerva Ginecol. 2018, 70, 432–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Average Age at Cryopreservation Procedure | Whole Number Reported Successful Outcomes: Live Births (Percentage) | Whole Number Reported Unsuccessful Outcomes: Miscarriages and/or Unsuccessful Conceptions/Implantations | |
|---|---|---|---|
| Ovarian Tissue Cryopreservation | 23.6 | 8.76% | 45 (43 miscarriages, 2 unsuccessful IVF attempts) |
| Oocyte Cryopreservation | 31.2 | 27% | 16 (10 miscarriages, 6 unsuccessful conceptions) |
| Embryonic Tissue Cryopreservation | 31 | 6.74% | 13 (5 unsuccessful conceptions/implantations, 18 miscarriages) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhri, E.N.; Salman, A.; Awartani, K.; Khan, Z.; Hashmi, S.K. Ovarian Tissue Cryopreservation versus Other Fertility Techniques for Chemoradiation-Induced Premature Ovarian Insufficiency in Women: A Systematic Review and Future Directions. Life 2024, 14, 393. https://doi.org/10.3390/life14030393
Chaudhri EN, Salman A, Awartani K, Khan Z, Hashmi SK. Ovarian Tissue Cryopreservation versus Other Fertility Techniques for Chemoradiation-Induced Premature Ovarian Insufficiency in Women: A Systematic Review and Future Directions. Life. 2024; 14(3):393. https://doi.org/10.3390/life14030393
Chicago/Turabian StyleChaudhri, Eman N., Ayman Salman, Khalid Awartani, Zaraq Khan, and Shahrukh K. Hashmi. 2024. "Ovarian Tissue Cryopreservation versus Other Fertility Techniques for Chemoradiation-Induced Premature Ovarian Insufficiency in Women: A Systematic Review and Future Directions" Life 14, no. 3: 393. https://doi.org/10.3390/life14030393