Gene Expression of Glucose Transporter 1 (GLUT1), Hexokinase 1 and Hexokinase 2 in Gastroenteropancreatic Neuroendocrine Tumors: Correlation with F-18-fluorodeoxyglucose Positron Emission Tomography and Cellular Proliferation




Abstract
:1. Introduction
2. Experimental Section
2.1. Ethics Statement
2.2. Patients/Subjects
2.3. 18F-FDG-PET Imaging

{kind=link}
{kind=link}
| Tumor type | Site of sample collection a | Metastatic disease | Ki67 index, % |
|---|---|---|---|
| Ileal carcinoid | Retro-peritoneal LN (m) | Yes | <2 |
| Ileal carcinoid | Ileum (p) | Yes | <2 |
| Ileal carcinoid | Ileum (p) | Yes | <2 |
| Ileal carcinoid | Ileum (p) | Yes | <2 |
| Ileal carcinoid | Ovary (m) | Yes | 40 |
| Ileal carcinoid | Retro-peritoneal LN (m) | Yes | 5 |
| Ileal carcinoid | Ileum (p) | No | <2 |
| Ileal carcinoid | Muscle (m) | Yes | <2 |
| Ileal carcinoid | Ileum (p) | Yes | <2 |
| Ileal carcinoid | Ileum (p) | No | <2 |
| Ileal carcinoid | Ileum (p) | Yes | <2 |
| N-F pancreatic NET | Pancreas (p) | No | <2 |
| N-F pancreatic NET | Pancreas (p) | No | 5 |
| Functioning pancreatico-duodenal NETs | |||
| Gastrinoma | Retro-peritoneal LN (m) | Yes | 5 |
| Glucagonoma | Retro-peritoneal LN (m) | Yes | <2 |
| Glucagonoma | pancreas (p) | Yes | 5 |
| Glucagonoma | Pancreas (p) | Yes | 50 |
| Glucagonoma/Somatostatinoma | Pancreas (p) | No | <2 |
| Somatostatinoma | Pancreas (p) | Yes | <2 |
| Somatostatinoma | Papilla Vatery (p) | No | <2 |
| Pheochromocytoma | Adrenal medulla (p) | No | <2 |
| Pheochromocytoma | Adrenal medulla (p) | <2 | |
| Pheochromocytoma | Adrenal medulla (m) | Yes | <2 |
| Pheochromocytoma | Adrenal medulla (p) | No | 10 |
| Pheochromocytoma | Adrenal medulla (p) | <2 | |
| Pheochromocytoma | Adrenal medulla (p) | Yes | 5 |
| Pheochromocytoma | Adrenal medulla (p) | No | <2 |
| Pheochromocytoma | Adrenal medulla (p) | No | 25 |
| Paraganglioma | Retroperitoneum (p) | No | <2 |
| NE colon carcinoma | Colon (p) | Yes | 50 |
| NE colon carcinoma | Colon (p) | Yes | 85 |
| NE colon carcinoma | Colon (p) | Yes | <2 |
| NE colon carcinoma | Liver (m) | Yes | 5 |
| Gastric NET, type 3 | Corpus (p) | No | 5 |
2.4. RNA Extraction and Reverse Transcription
2.5. Quantitative Real-Time PCR
2.6. Immunohistochemical Evaluation of Ki67
2.7. Statistical Analysis
3. Results
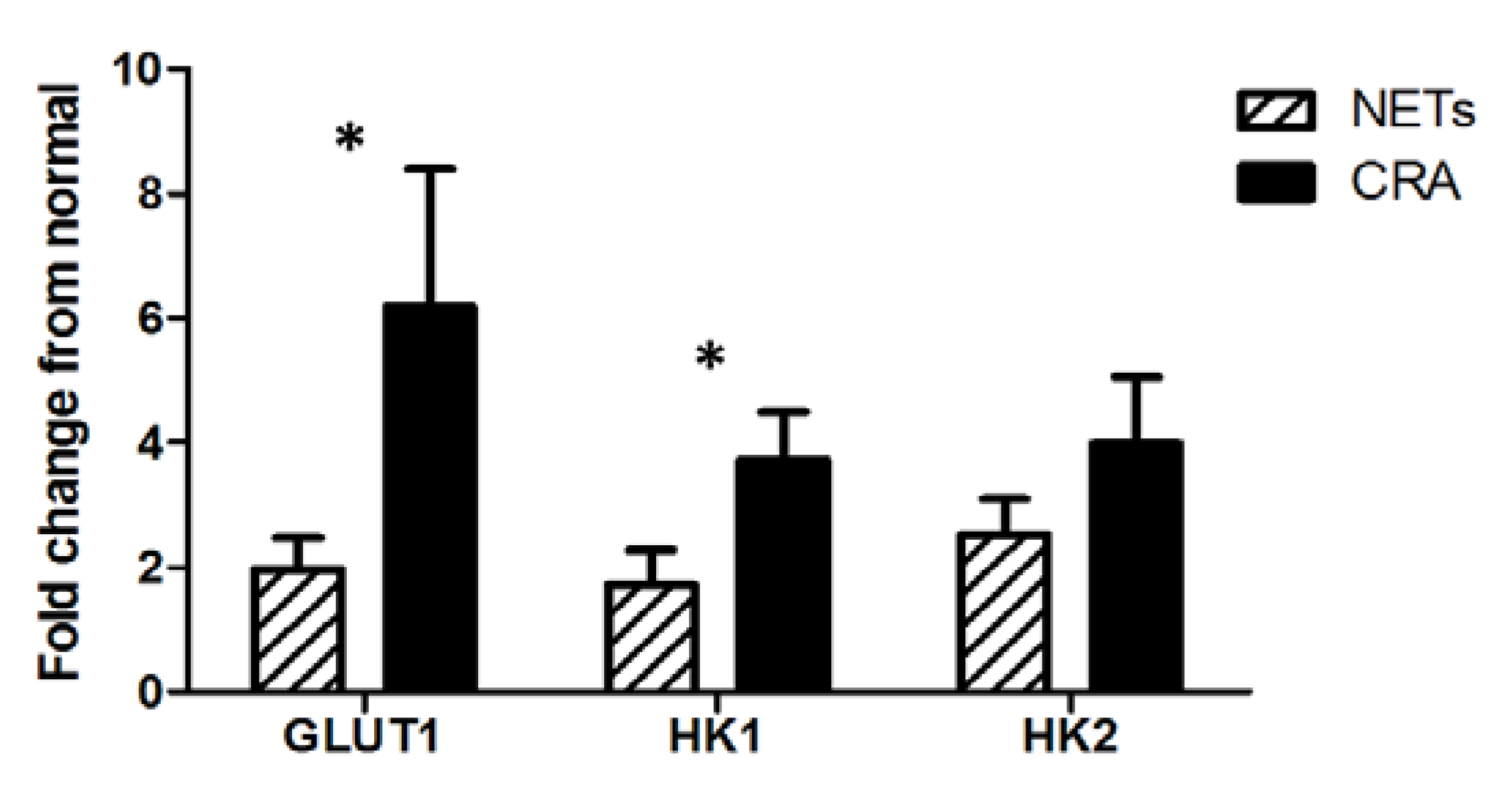
3.1. Gene Expression of GLUT, HK1 and HK2

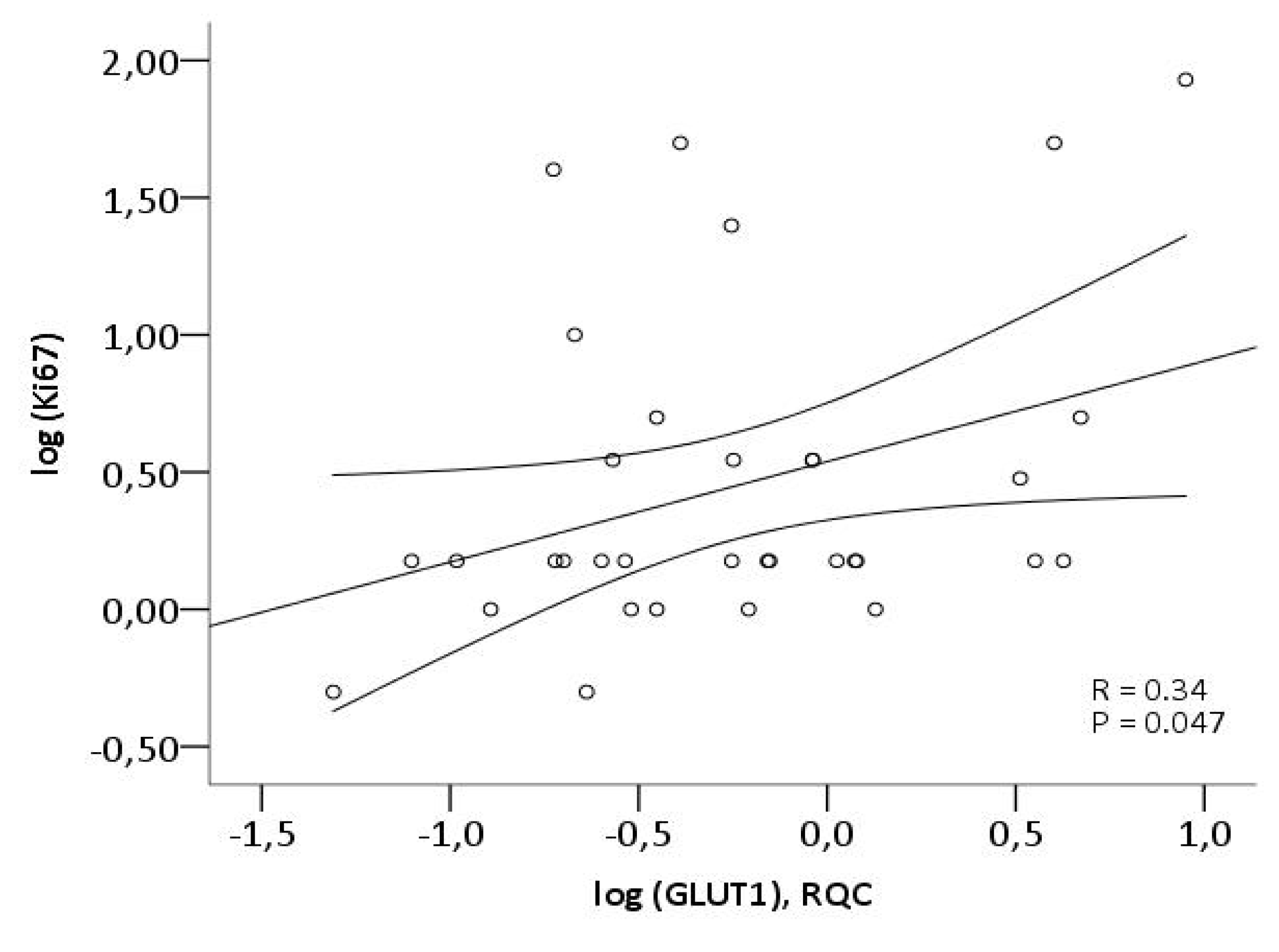
3.2. Ki67 and Correlation with Gene Expression of GLUT1, HK1 and HK2

3.3. FDG-PET and Gene Expression of GLUT1, HK1 and HK2
| FDG-PET result | GLUT1 gene expression | HK1 gene expression | HK2 gene expression | Ki67 index | |
|---|---|---|---|---|---|
| Ileal carcinoid | Neg | 5 | 1.1 | 1.1 | 5 |
| Ileal carcinoid | Neg | 4 | 3 | 1.8 | <2 |
| Ileal carcinoid | Neg | 1.3 | 0.4 | 1.5 | <2 |
| Ileal carcinoid | Neg | 1.1 | 0.8 | 1.6 | <2 |
| Pancreatico-duedenal NET (Somatostatinoma) | Neg | 0.4 | 1.5 | 4 | <2 |
| Pancreatico-duedenal NET (glucagonoma) | Pos | 0.9 | 0.1 | 1.5 | 2–5 |
| Pancreatico-duedenal NET (non-functioning) | Pos | 1.2 | 0.5 | 1.5 | <2 |
| NE colon carcinoma | Pos | 4 | 4 | 3 | 50 |
| NE colon carcinoma | Pos | 9 | 4 | 5 | 85 |
| NE colon carcinoma | Neg | 0.6 | 1.6 | 1.7 | 2–5 |
| NE colon carcinoma | Neg | 0.3 | 1.7 | 4 | <2 |
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Brown, R.S.; Leung, J.Y.; Kison, P.V.; Zasadny, K.R.; Flint, A.; Wahl, R.L. Glucose transporters and FDG uptake in untreated primary human non-small cell lung cancer. J. Nucl. Med. 1999, 40, 556–565. [Google Scholar] [PubMed]
- Kloppel, G.; Couvelard, A.; Perren, A.; Komminoth, P.; McNicol, A.M.; Nilsson, O.; Scarpa, A.; Scoazec, J.Y.; Wiedenmann, B.; Papotti, M.; Rindi, G.; Plockinger, U.; Mallorca Consensus Conference participants; European Neuroendocrine Tumor Society. ENETS Guidelines for the Standards of Care in Patients with Neuroendocrine Tumors: Towards a Standardized Approach to the Diagnosis of Gastroenteropancreatic Neuroendocrine Tumors and Their Prognostic Stratification. Neuroendocrinology 2008, 90, 162–166. [Google Scholar]
- Rindi, G.; Arnold, R.; Bosman, F.T.; Capella, C.; Klimstra, D.S.; Kloppel, G.; Komminoth, P.; Solcia, E. Nomenclature and Classification of Neuroendocrine Neoplasms of the Digestive System. In WHO Classification of Tumours of the Digestive System; IARC Press: Lyon, France, 2010. [Google Scholar]
- Binderup, T.; Knigge, U.; Loft, A.; Mortensen, J.; Pfeifer, A.; Federspiel, B.; Hansen, C.P.; Højgaard, L.; Kjaer, A. Functional imaging of neuroendocrine tumors: A head-to-head comparison of somatostatin receptor scintigraphy, 123I-MIBG scintigraphy, and 18F-FDG PET. J. Nucl. Med. 2010, 51, 704–712. [Google Scholar] [CrossRef]
- Ong, L.C.; Jin, Y.; Song, I.C.; Yu, S.; Zhang, K.; Chow, P.K. 2-[18F]-2-deoxy-D-glucose (FDG) uptake in human tumor cells is related to the expression of GLUT1 and hexokinase II. Acta Radiol. 2008, 49, 1145–1153. [Google Scholar] [CrossRef]
- Aloj, L.; Caracó, C.; Jagoda, E.; Eckelman, W.C.; Neumann, R.D. GLUT1 and hexokinase expression: Relationship with 2-fluoro-2-deoxy-D-glucose uptake in A431 and T47D cells in culture. Cancer Res. 1999, 59, 4709–4714. [Google Scholar] [PubMed]
- Higashi, K.; Ueda, Y.; Sakurai, A.; Wang, X.M.; Xu, L.; Murakami, M.; Seki, H.; Oguchi, M.; Taki, S.; Nambu, Y.; et al. Correlation of GLUT1 glucose transporter expression with [18F]FDG uptake in non-small cell lung cancer. Eur. J. Nucl. Med. 2000, 27, 1778–1785. [Google Scholar] [CrossRef]
- Mathupala, S.P.; Ko, Y.H.; Pedersen, P.L. Hexokinase II: Cancer’s double-edged sword acting as both facilitator and gatekeeper of malignancy when bound to mitochondria. Oncogene 2006, 25, 4777–4786. [Google Scholar] [CrossRef]
- Watson, A.J.; Lolohea, S.; Robertson, G.M.; Frizelle, F.A. The role of positron emission tomography in the management of recurrent colorectal cancer: A review. Dis. Colon Rectum 2007, 50, 102–114. [Google Scholar] [CrossRef]
- de Geus-Oei, L.F.; Ruers, T.J.M.; Punt, C.J.A.; Leer, J.W.; Corstens, F.H.M.; Oyen, W.J.G. FDG-PET in colorectal cancer. Cancer Imaging 2006, 6, S71–S81. [Google Scholar] [CrossRef]
- Gu, J.; Yamamoto, H.; Fukunaga, H.; Danno, K.; Takemasa, I.; Ikeda, M.; Tatsumi, M.; Sekimoto, M.; Hatazawa, J.; Nishimura, T.; Monden, M. Correlation of GLUT1 overexpression, tumor size, and depth of invasion with 18F-2-fluoro-2-deoxy-D: Glucose uptake by positron emission tomography in colorectal cancer. Digest Dis. Sci. 2006, 51, 2198–2205. [Google Scholar] [CrossRef]
- Song, Y.S.; Lee, W.W.; Chung, J.H.; Park, S.Y.; Kim, Y.K.; Kim, S.E. Correlation between FDG uptake and glucose transporter type 1 expression in neuroendocrine tumors of the lung. Lung Cancer 2008, 61, 54–60. [Google Scholar] [CrossRef]
- Hutchings, M.; Loft, A.; Hansen, M.; Ralfkiaer, E.; Spechit, L. Different histopathological subtypes of Hodgkin lymphoma show significantly different levels of FDG uptake. Hematol. Oncol. 2006, 24, 146–150. [Google Scholar] [CrossRef]
- Stratagene Laboratory Tools software. Available online: http://www.stratagene.com/qpcr/links.asp (accessed on 1 June 2005).
- Primer 3. Available online: http://primer3.sourceforge.net/ (accessed on 16 October 2013).
- Binderup, T.; Knigge, U.; Mellon, M.A.; Palnaes, H.C.; Kjaer, A. Quantitative gene expression of somatostatin receptors and noradrenaline transporter underlying scintigraphic results in patients with neuroendocrine tumors. Neuroendocrinology 2008, 87, 223–232. [Google Scholar] [CrossRef]
- Shebani, K.O.; Souba, W.W.; Finkelstein, D.M.; Stark, P.C.; Elgadi, K.M.; Tanabe, K.K.; Ott, M.J. Prognosis and survival in patients with gastrointestinal tract carcinoid tumors. Ann. Surg. 1999, 229, 815–821. [Google Scholar] [CrossRef]
- Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M.J. Cancer statistics. Ca—A Cancer J. Clin. 2007, 57, 43–66. [Google Scholar] [CrossRef]
- Panzuto, F.; Nasoni, S.; Falconi, M.; Corleto, M.M.; Capurso, G.; Cassetta, S.; di Fonzo, M.; Tornatore, V.; Milione, M.; Angeletti, S.; et al. Prognostic factors and survival in endocrine tumor patients: Comparison between gastrointestinal and pancreatic localization. Endocr. Relat. Cancer 2005, 12, 1083–1092. [Google Scholar] [CrossRef]
- Pape, U.F.; Berndt, U.; Müller-Nordhorn, J.; Bohmig, M.; Roll, S.; Koch, M.; Willich, S.N.; Wiedenmann, B. Prognostic factors of long-term outcome in gastroenteropancreatic neuroendocrine tumours. Endocr. Relat. Cancer 2008, 15, 1083–1097. [Google Scholar] [CrossRef]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahike, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant chemotherapy with gemcitabine vs. observation in patients undergoing curative-intent resection of pancreatic cancer: A randomized controlled trial. JAMA 2007, 297, 267–277. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef]
- Fischer, B.; Lassen, U.; Mortensen, J.; Larsen, S.; Loft, A.; Bertelsen, A.; Ravn, J.; Clementsen, P.; Høgholm, A.; Larsen, K.; et al. Preoperative staging of lung cancer with combined PET-CT. N. Engl. J. Med. 2009, 361, 32–39. [Google Scholar] [CrossRef]
- Hutchings, M.; Loft, A.; Hansen, M.; Pedersen, L.M.; Berthelsen, A.K.; Keiding, S.; D’Amore, F.; Boesen, A.M.; Roemer, L.; Specht, L. Position emission tomography with or without computed tomography in the primary staging of Hodgkin’s lymphoma. Haematologica 2006, 91, 482–489. [Google Scholar] [PubMed]
- Torizuka, T.; Tanizaki, Y.; Kanno, T.; Futatsubashi, M.; Naitou, K.; Ueda, Y.; Ouchi, Y. Prognostic value of 18F-FDG PET in patients with head and neck squamous cell cancer. AJR Am. J. Roentgenol. 2009, 192, W156–60. [Google Scholar] [CrossRef]
- Whiteford, M.H.; Whiteford, H.M.; Yee, L.F.; Ogunbiyi, O.A.; Dehdashti, F.; Siegel, B.A.; Birnbaum, E.H.; Fleshman, J.W.; Kodner, I.J.; Read, T.E. Usefulness of FDG-PET scan in the assessment of suspected metastatic or recurrent adenocarcinoma of the colon and rectum. Dis. Colon Rectum 2000, 43, 759–767. [Google Scholar] [CrossRef]
- Binderup, T.; Knigge, U.; Loft, A.; Federspiel, B.; Kjaer, A. 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin. Cancer Res. 2010, 16, 978–985. [Google Scholar] [CrossRef]
- Yen, T.C.; See, L.C.; Lai, C.H.; Yah-Huei, C.W.; Ng, K.K.; Ma, S.Y.; Lin, W.J.; Chen, J.T.; Chen, W.J.; Lai, C.R.; Hsueh, S. 18F-FDG uptake in squamous cell carcinoma of the cervix is correlated with glucose transporter 1 expression. J. Nucl. Med. 2004, 45, 22–29. [Google Scholar] [PubMed]
- Tohma, T.; Okazumi, S.; Makino, H.; Cho, A.; Mochiduki, R.; Shuto, K.; Kudo, H.; Matsubara, K.; Gunji, H.; Ochiai, T. Relationship between glucose transporter, hexokinase and FDG-PET in esophageal cancer. Hepatogastroenterology 2005, 52, 486–490. [Google Scholar] [PubMed]
- Zhao, S.; Kuge, Y.; Mochizuki, T.; Takahashi, T.; Nakada, K.; Sato, M.; Takei, T.; Tamaki, N. Biologic correlates of intratumoral heterogeneity in 18F-FDG distribution with regional expression of glucose transporters and hexokinase-II in experimental tumor. J. Nucl. Med. 2005, 46, 675–682. [Google Scholar] [PubMed]
- Lee, J.D.; Yang, W.I.; Park, Y.N.; Kim, K.S.; Choi, J.S.; Yun, M.; Ko, D.; Kim, T.S.; Cho, A.E.; Kim, H.M.; et al. Different glucose uptake and glycolytic mechanisms between hepatocellular carcinoma and intrahepatic mass-forming cholangiocarcinoma with increased 18F-FDG uptake. J. Nucl. Med. 2005, 46, 1753–1759. [Google Scholar] [PubMed]
- Kayani, I.; Bomanji, J.B.; Groves, A.; Conway, G.; Gacinovic, S.; Win, T.; Dickson, J.; Caplin, M.; Ell, P.J. Functional imaging of neuroendocrine tumors with combined PET/CT using 68Ga-DOTATATE (DOTA-DPhe1,Tyr3-octreotate) and 18F-FDG. Cancer 2008, 112, 2447–2455. [Google Scholar] [CrossRef]
- Oberg, K.; Astrup, L.; Eriksson, B.; Falkmer, S.E.; Falkmer, U.G.; Gustafsen, J.; Haglund, C.; Knigge, U.; Vatn, M.H.; Välimäki, M.; et al. Guidelines for the management of gastroenteropancreatic neuroendocrine tumours (including bronchopulmonary and thymic neoplasms). Part I—General overview. Acta Oncol. 2004, 43, 617–625. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Binderup, T.; Knigge, U.P.; Federspiel, B.; Sommer, P.; Hasselby, J.P.; Loft, A.; Kjaer, A. Gene Expression of Glucose Transporter 1 (GLUT1), Hexokinase 1 and Hexokinase 2 in Gastroenteropancreatic Neuroendocrine Tumors: Correlation with F-18-fluorodeoxyglucose Positron Emission Tomography and Cellular Proliferation. Diagnostics 2013, 3, 372-384. https://doi.org/10.3390/diagnostics3040372
Binderup T, Knigge UP, Federspiel B, Sommer P, Hasselby JP, Loft A, Kjaer A. Gene Expression of Glucose Transporter 1 (GLUT1), Hexokinase 1 and Hexokinase 2 in Gastroenteropancreatic Neuroendocrine Tumors: Correlation with F-18-fluorodeoxyglucose Positron Emission Tomography and Cellular Proliferation. Diagnostics. 2013; 3(4):372-384. https://doi.org/10.3390/diagnostics3040372
Chicago/Turabian StyleBinderup, Tina, Ulrich Peter Knigge, Birgitte Federspiel, Peter Sommer, Jane Preuss Hasselby, Annika Loft, and Andreas Kjaer. 2013. "Gene Expression of Glucose Transporter 1 (GLUT1), Hexokinase 1 and Hexokinase 2 in Gastroenteropancreatic Neuroendocrine Tumors: Correlation with F-18-fluorodeoxyglucose Positron Emission Tomography and Cellular Proliferation" Diagnostics 3, no. 4: 372-384. https://doi.org/10.3390/diagnostics3040372
APA StyleBinderup, T., Knigge, U. P., Federspiel, B., Sommer, P., Hasselby, J. P., Loft, A., & Kjaer, A. (2013). Gene Expression of Glucose Transporter 1 (GLUT1), Hexokinase 1 and Hexokinase 2 in Gastroenteropancreatic Neuroendocrine Tumors: Correlation with F-18-fluorodeoxyglucose Positron Emission Tomography and Cellular Proliferation. Diagnostics, 3(4), 372-384. https://doi.org/10.3390/diagnostics3040372