5. Discussion
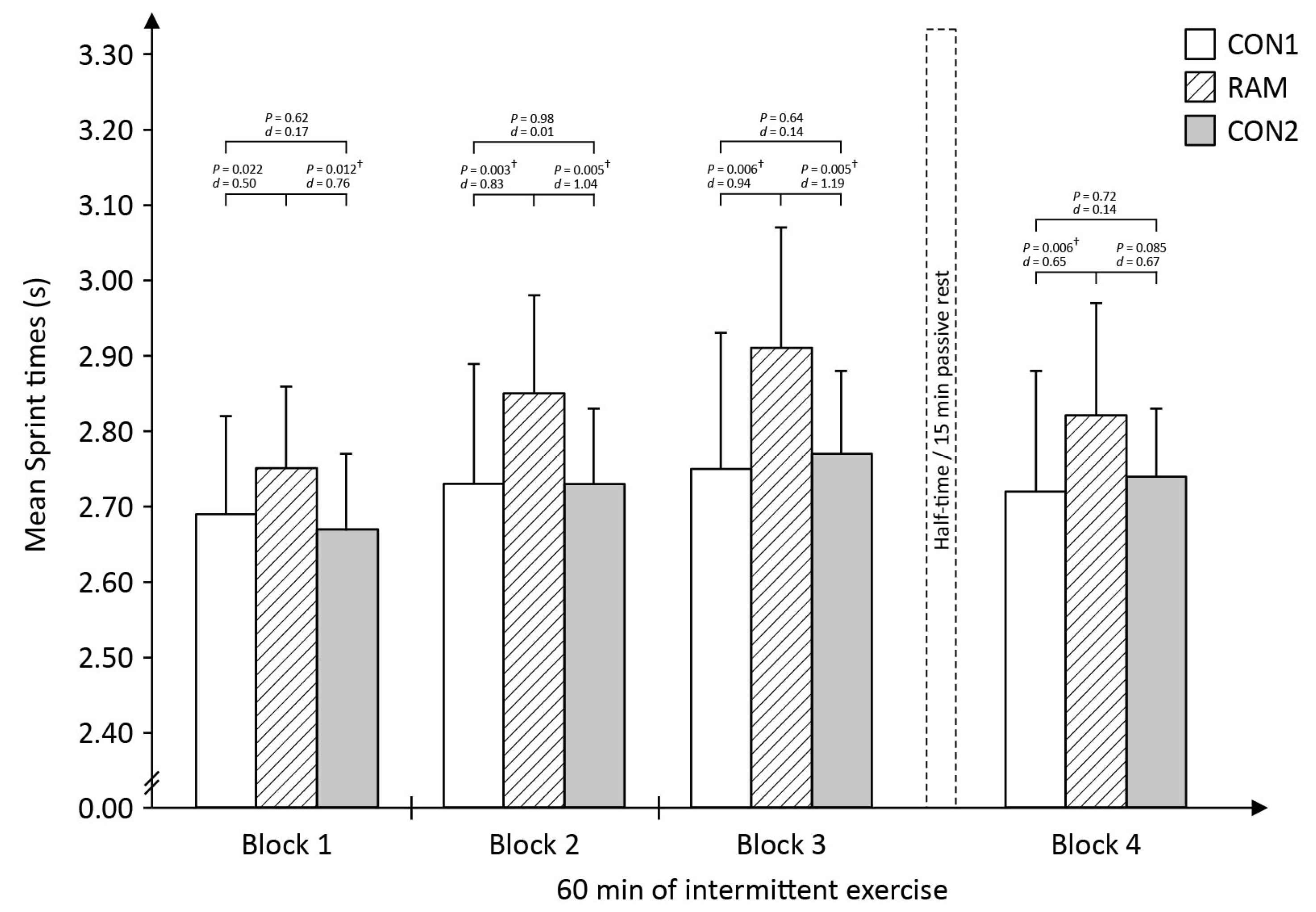
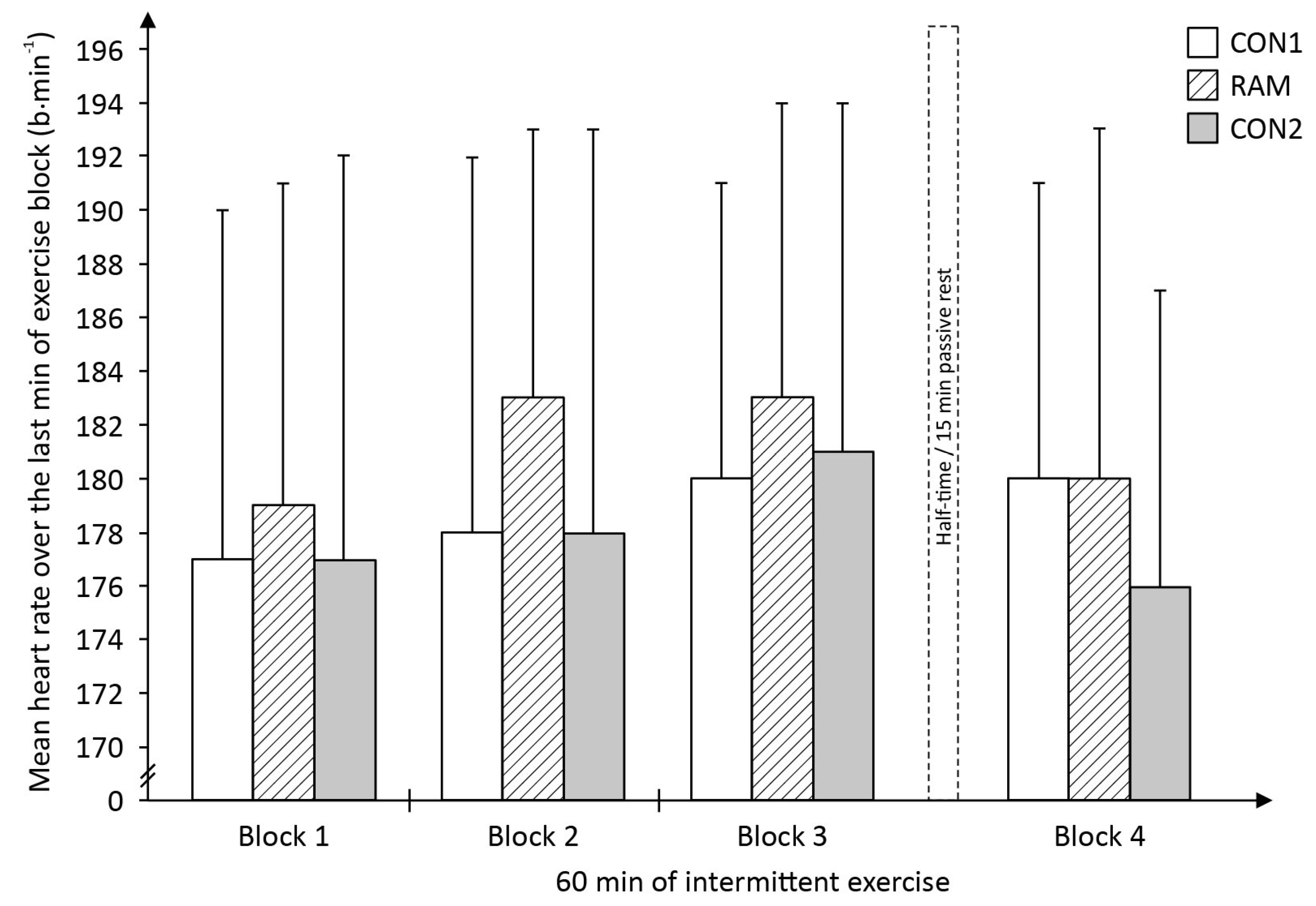
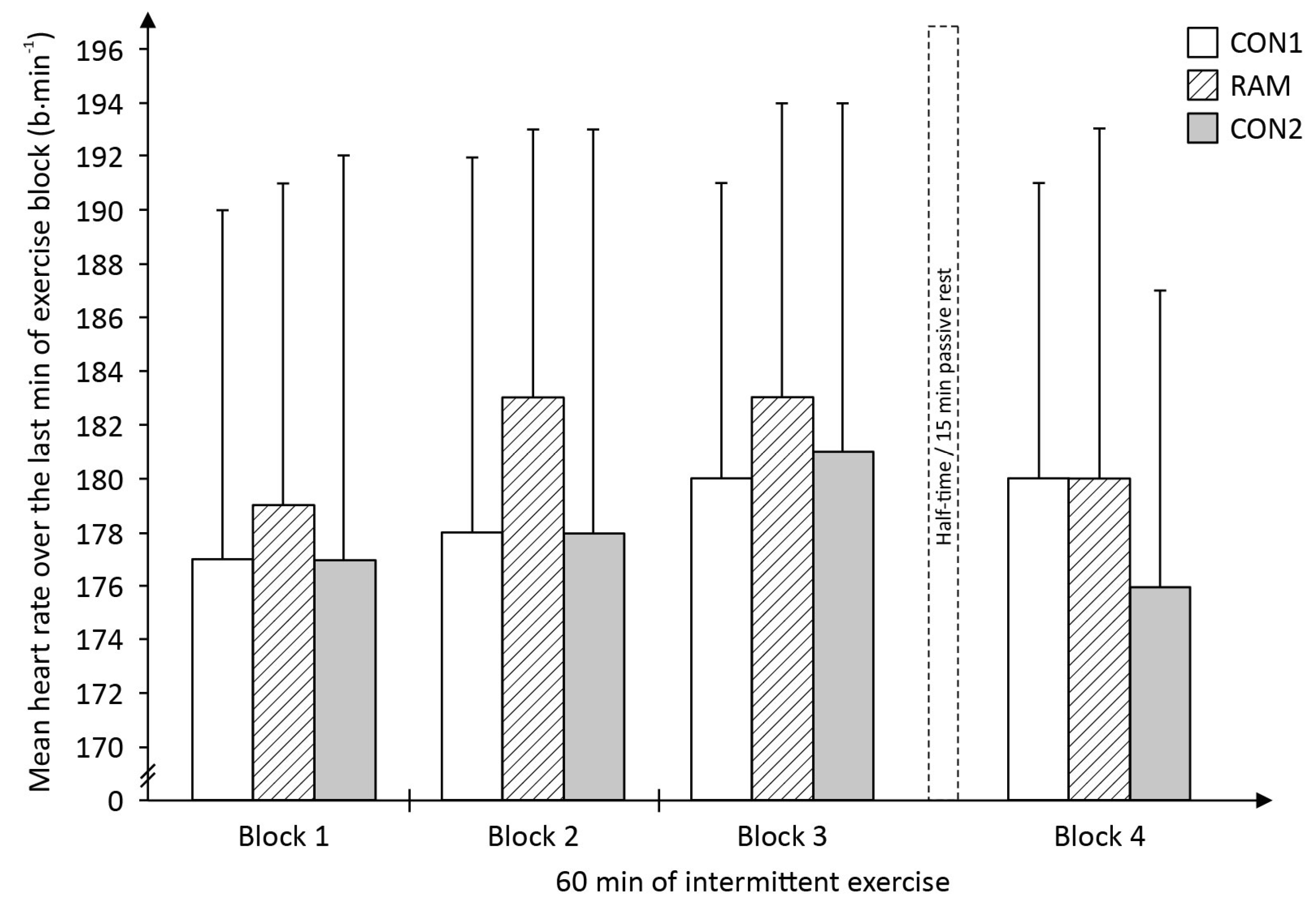
The present study endeavoured to closely control for the confounding factors that plagued previous Ramadan and exercise performance studies such as differences in the participants’ pre-exercise food and fluid intake, sleep pattern and training stimulus between Ramadan-fasted and non-fasted exercise trials. In the present study, all these factors were equivalent between the CON and RAM trials. Despite the similarities, the study’s major finding was that players’ sprint performance was shown to be poorer (i.e., slower mean sprint times) throughout the 60-min intermittent exercise during RAM trial as compared to their sprint performance in CON1 and CON2 trials. Further, it was shown that the poorer sprint performance in the Ramadan-fasted state was not associated with any substantial differences in the players’ metabolic measures such as blood glucose or blood lactate concentrations or physiological effort (as assessed via mean HR during exercise) between CON and RAM trials throughout the mLIST. In addition, the MVIC tests results of both the exercised and non-exercised muscles were equivalent between pre-exercise and during the mLIST in the RAM trial; which indicate there was minimal degree of fatigue within the working muscles (i.e., peripherally-related) and in the neural activation of the muscles (i.e., centrally-driven pathways) that can help to explain for the poorer sprint performance throughout the 60-min intermittent exercise in the RAM trial. Overall, these findings together with the observation of an early onset of the sprints performance decrements within the first 15-min of exercise, provided good evidence of the substantiated view that the negative impact of Ramadan fasting on exercise performance was largely due to negative placebo (or nocebo) effects of observing the religious fast.
Previous studies have indicated a lowering in the players’ submaximal intensity component to conserve their efforts for the more critical high-intensity efforts when athletes are exposed to heat or hypoxia [
29,
30]. In the present study, all submaximal locomotor activities of walking, jogging, and striding were dictated by pre-planned beeping sounds and players had “control” only over their maximal sprinting efforts. Thus by design, players in the present study were not able to pace their submaximal running speeds. Sprinting constitutes only ∼1% to ∼12% of the distance covered during a football match [
31] but this ability cannot be undermined since linear sprints are the most frequent action immediately preceding goal scoring opportunities in top-level matches [
18]. Therefore, the capacity to perform sprints at the player’s top velocity over an entire match is a critical reflection of a player’s football performance. Thus, in this regard, the present study’s results clearly indicate that Ramadan fasting has a negative impact on football performance, and possibly performance in other intermittent team-sports as well.
The present study’s findings clearly supported previous findings in which high-intensity running distance covered were significantly lower during a 90-min football match played in the Ramadan state as compared to a match played in the non-Ramadan state [
32]. In that study, performance decrement was similarly observed during the first 15-min of the 90 min match. This early “deterioration” in performance is unlikely to be due to the onset of physiologically-related fatigue as a result of factors such as total depletion of endogenous substrate, severe dehydration or metabolic disturbances within the muscles, but rather most probably be due to either a conscious or unconscious pacing strategy adopted by the players when in the fasted state. Perhaps, in the Ramadan-fasted state, players deliberately or were instinctively “compelled” via the Governor system [
33] to moderate their sprinting efforts (which is the most physically demanding activity of the mLIST) throughout the exercise in order to conserve their available resources to ensure that they would be able to successfully complete the other submaximal shuttle runs.
A previous study showed that Ramadan fasting led to a decline in 5000 m running performance in well-trained runners [
34]. The runners’ maximal strength via an isometric knee extension test performed in the Ramadan-fasted state was also negatively affected. The study’s investigators subsequently concluded that the decrease in leg strength could have led to the observed slower run times [
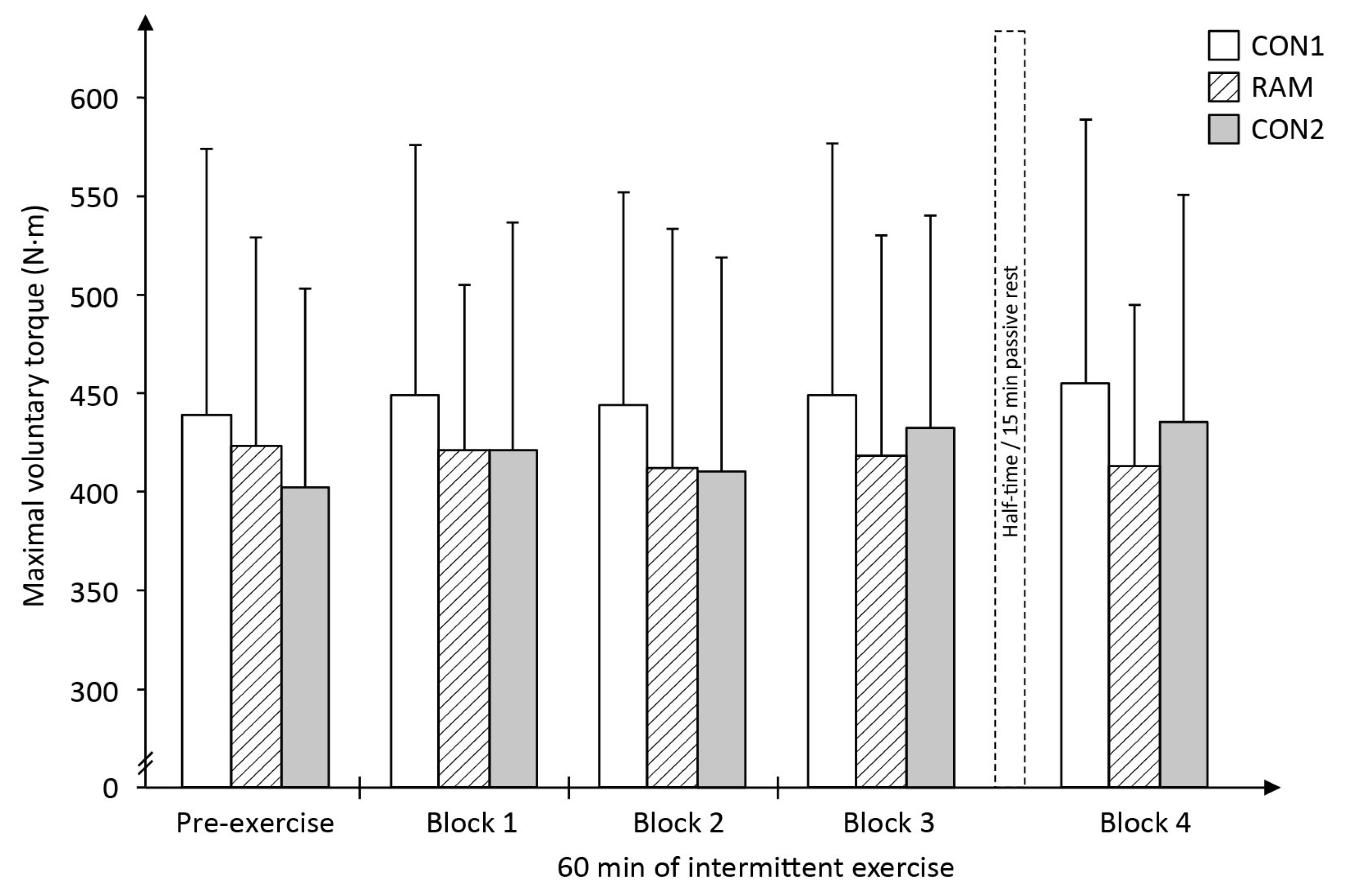
34]. However, a limitation in that study was that both the running performance and isometric strength tests were conducted as independent trials, i.e., on separate occasions, and thus it cannot be ascertained with confidence that the poorer endurance performance in Ramadan was directly due to the declined in isometric leg strength. In contrast, the present study ensured that players’ maximal muscle tests were conducted within the 60-min intermittent exercise. If impaired muscle functions (e.g., strength) and/or related adverse metabolic response within the contracting muscles were the key mechanism(s) to the poorer exercise performance in the Ramadan-fasted state, a greater decreased in the MVIC of the knee would also be expected in the RAM trial as compared to that in the CON trials. Rather surprising, the MVIC of the knee extensor indicated that muscle functional capability (i.e., the ability to generate high levels of contraction) was unaffected by Ramadan fast (
Figure 5) and is thus not a factor that could have led to the poorer sprinting performance in the RAM compared to that in the CON1 and CON2 trials.
Recently, Bouhlel and colleagues [
35] showed that repeated 6 s cycle sprints times were slower in the Ramadan-fasted relative to non-fasted state; but this decrement in performance was not associated with any changes in the muscles’ electromyographic measures taken immediately after the last sprint effort. Subsequently, the study’s investigators argued that the reduction in their sprint performance must originate from fatigue occurring within the central nervous system (CNS) rather than within the musculature [
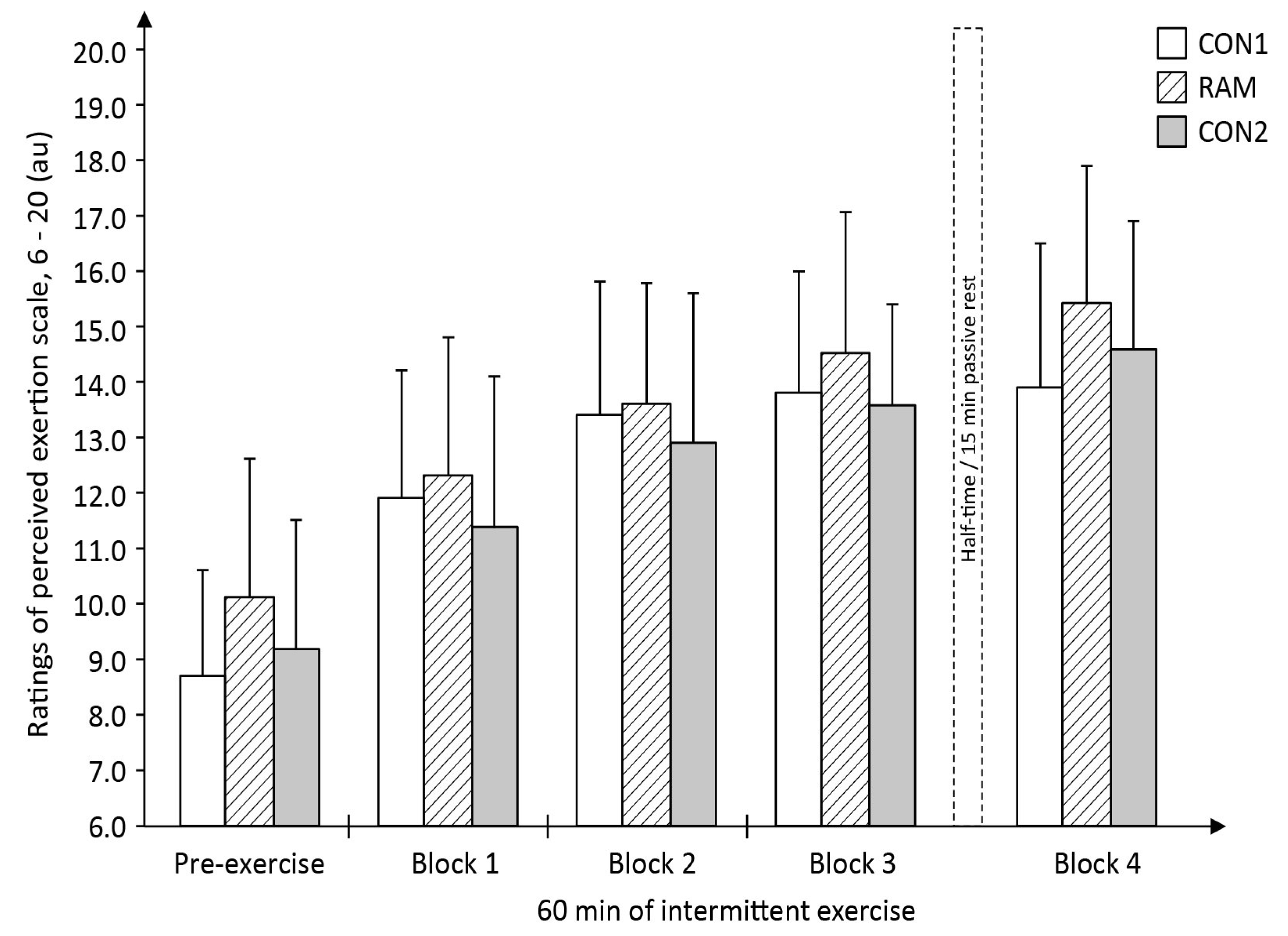
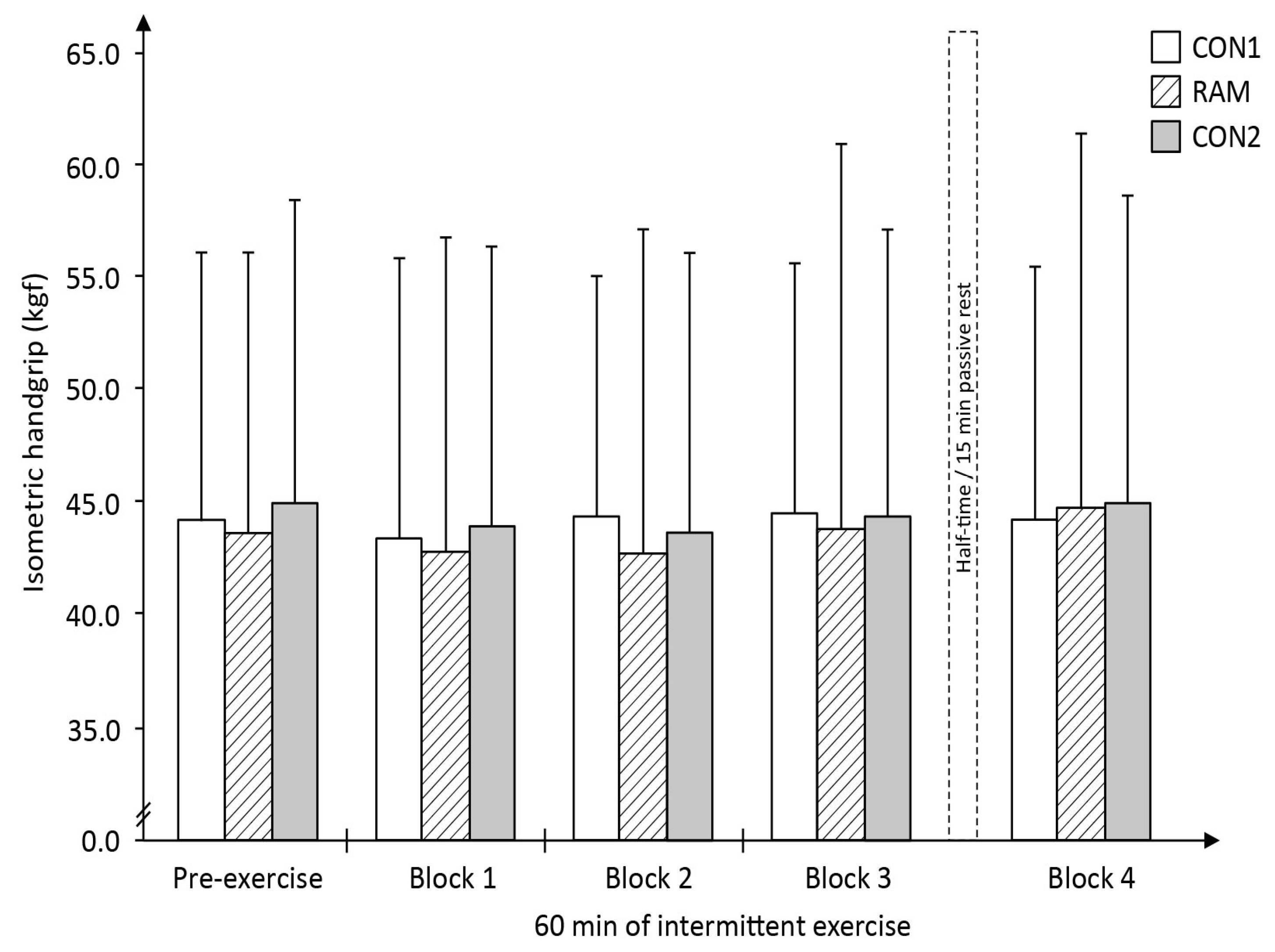
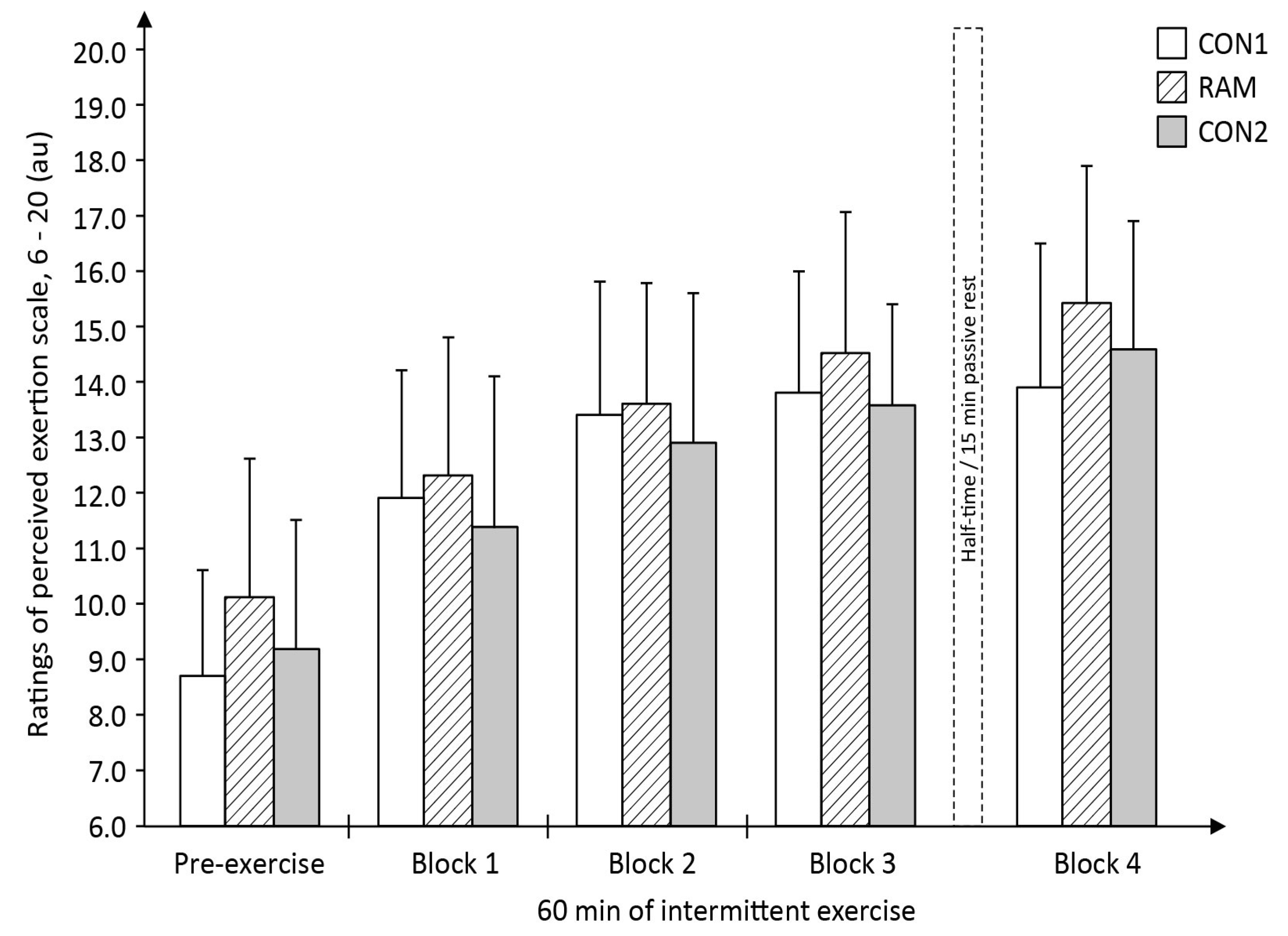
35]. Similarly, in the present study, the decline in sprint performance in the RAM trial could be that Ramadan fasting magnifies the perception of fatigue during the mLIST resulting in a decrease in central drive relative to that perceived in the non-fasted state and this subsequently, reduces the CNS ability to maximally recruit all the muscle fibres during the all-out sprint efforts. This interpretation is partially supported by the higher pre-exercise subjective ratings of tiredness (
Table 6) and overall higher levels of RPE throughout exercise (
Figure 8) in RAM trial. However, the lack of change in the objective measures of both the MVIC of the leg (exercised muscles) as well as the MVIC of the hand-grip (non-exercised muscles) across the entire 60 min duration within the RAM trial (
Figure 5 and
Figure 6, respectively) did not seem to support this theory of a higher level of CNS fatigue in the Ramadan-fasted state. If central-pathways fatigue was the primary cause of the poorer performance in sprints in RAM, there should be a decrease in the MVIC of the hand-grip as well, i.e., a ‘fatigued’ CNS should also lead to a decline in voluntary contraction of the non-exercised (i.e., the less fatiguing arm) muscle. This was not the case in the present study. Therefore, by the process of elimination, it can be deduced that the primary cause of the poorer performance in the sprints during RAM trial is not due to either peripheral- or CNS-mediated fatigue, but rather most likely to be due to the negative effects of placebo. This view has credence as neural activation from the CNS as the primary driver to single maximal or explosive effort during exercise, and coupled with the fact that the poorer sprint performance in RAM trials was observed as early as within the first 15 min (i.e., in exercise block 1) of the mLIST. In short, fasted individuals moderated their sprinting efforts early during the mLIST exercise, either consciously or subconsciously, as a way of coping with the challenging demands of completing the 60-min intermittent exercise in the Ramadan-fasted state without catastrophic consequences later in the mLIST [
36]. It may therefore be deduced that the decline in sprint performance during the RAM trial was not due to any physiological-induced mechanism from the act of Ramadan fast but rather due to the players pacing their efforts as a result of placebo effects, or in the present study’s situation, aptly termed nocebo consequences of observing the Ramadan fast [
37,
38].
Nonetheless, during prolonged exercise, it may be that the “fatigue” experienced by an athlete is perhaps, physiologically different during the early stage of exercise compared to the late stage of the exercise [
39,
40,
41]. In the present study, late in the RAM exercise trial, it might be that muscle glycogen concentration was reduced to critical levels leading to the poorer sprint performance. Krustrup and colleagues [
40] showed that despite ingesting breakfast, as well as a meal two hours prior to a football match, muscle glycogen decreased significantly, with about ~50% of muscle fibres being completely or almost depleted of muscle glycogen after the match, Further, they showed that reduced muscle glycogen stores were associated with a decline in physical exertions in the second half of the match [
40]. It should also be noted that the players in the present study was exercising in a hot, humid environment, which could have led to a greater rate of usage of endogenous muscle glycogen [
42] leading to its rapid depletion within specific muscle fibres, i.e., fast-twitch fibres [
43]. While this muscle glycogen limiting argument is reasonable, this might again, not be the case in the present study for several reasons. Firstly, it unlikely that the players in the Ramadan-fasted state were possessing lower levels endogenous muscle glycogen at pre-exercise relative to that in the CON trial. Although endogenous muscle glycogen was not directly measured, the players were optimally provided with sufficient carbohydrates (and total calories) in the 24 h period prior to the RAM trial and previous studies have indicated minimal impact of fasting on endogenous muscle glycogen levels in as long as no strenuous physical activity is engaged during the duration of the fast. Indeed, endogenous muscle glycogen depleted by a mere 25% as a result of fasting for a 24-h period [
44,
45]. Moreover, firstly the present study’s players fasted for only ~12 h and they did not engage in any strenuous physical activity prior to the exercise trial during the fasted period. Secondly, the mLIST exercise was only of 60 min rather than 90 min duration. A review on the effect of duration of exercise on muscle glycogen usage suggest that muscle glycogen tended to lower to critical levels only after >60 min of moderate to high-intensity exercise [
46]. Thirdly, blood lactate concentration, which has been considered as an indirect indicator of the substrate breakdown due to glycolysis [
47], was not significantly different between CON and RAM trials at the start and at the end of each four exercise blocks (
Table 3). All of these indicate that the muscle glycogen levels in the Ramadan-fasted state was not compromised throughout the mLIST exercise.
However, particularly towards the late part of the 60-min mLIST, dehydration may however adversely impact muscle function (i.e., on sprints performance) via a diminished ability of the CNS to recruit motor units efficiently. In particular, the loss of large amount of electrolytes through sweating can cause ionic imbalances [
48] resulting in the disruption of the neuromuscular function of the working muscles. Edwards and Noakes [
39] also suggested that dehydration may result in an unconscious effort to reduce subsequent physical exertions to try to maintain homeostasis and protect against intracellular disturbances. And when dehydration is accompanied with hyperthermia, as the case might be towards the end of the 60 min mLIST exercise, it can exert a more profound effect on muscular functions and this could have resulted in the greater slowed sprinting speeds in the RAM trial. However, the last 15 min of exercise (i.e., block 4) showed that sprinting times has reverted close to sprint times observed in block 1—further indicating that there was minimal accumulation of extreme physical fatigue in the Ramadan-fasted state.
A high body core temperature, instead of substrate availability, has been identified as a possible limiting factor to exercise performance in the heat [
49]. For example, the increased heat stress and high core temperatures from exercise have been reported to reduce the player’s ability to perform repeated high-intensity sprints [
50]. Players in the RAM trial did not consume fluid for at least ~12 h before exercise (resulting in hypohydration) and were not allowed to consume fluids during exercise (leading to dehydration), and hence it was expected that the thermoregulatory functions and/or processes of the players in the RAM trial would be compromised relative to the CON trials, which in turn could adversely influenced their subsequent exercise performance, vis-a-vis causing the fasted players to slow down in their sprinting speeds [
36]. Rather surprisingly, there were no significant differences in both mean
Tre and
Tsk in both the CON trials to that in the RAM trial (
Table 2). The
Tre data in all trials showed that none of the values surpassed the 40 °C mark, which is deemed to be the critical threshold point for internal core temperature [
49]. It should note however that the present
Tre are not peak values since
Tre was recorded only at the end of each 15 min exercise block and moreover in RAM trials, fasted players performed less intense work. It remains possible that there were instances during the mLIST where
Tre may have breached the 40 °C mark, which could have led to some altercations in the players’ exercise performance at that time point. Prolonged exercise in hot environmental conditions can lead to a rise in internal core temperature that can result not only in the decline in exercise performance, but in the worst case where the exercising individual succumbing to heat illness [
51]. Nonetheless, the present core and skin temperature data do suggest that fasted players can physiologically adjust their exertions and exercise safely in a hot humid environment. The present study to our knowledge, is the first to monitor the
Tre and
Tsk of Ramadan-fasted individuals throughout a prolonged exercise (>60 min) in the hot and humid environment, and given the present study’s mixed findings, further research in this area is warranted.
Yet another possible contributor to the reduction in performance is the elevation of negative mood states and suppression of positive feelings [
52]. These negative feelings can permeate via poor sleep quality and/or quantity and/or drastic shift in the body’s circadian rhythm during Ramadan [
9,
10]. Indeed, sleep loss during Ramadan has been reported to be closely associated with detrimental effects on mood and perception [
8,
9]. The present data however showed that sleep hours for the evening before the RAM experimental day, assessed objectively, was however equivalent to that in the two CON trials (
Table 5). During Ramadan, the players consumed their
sahur meal at ~05:30 and then went back to bed thereafter to continue with their sleep until late morning as was similarly observed in a group of professional football players [
53]. Detraining, as a result of reduced training load or stimulus due to a lowering of training frequency or intensity during the Ramadan month has also been highlighted as another possible cause of lowered performance in fasted Muslim athletes [
11,
12]. In the present study however, training load for the week before all three experimental trials, although was slightly lowered in RAM and CON2 trials when compared to CON1, was generally equivalent to each other (
Table 7).
In summary, the slower sprint times in RAM relative to CON trials were not due to physical fatigue from energy deficiency since blood glucose and blood lactate concentrations values throughout the exercise were generally similar between RAM and CON trials, or loss in muscular generating capabilities since no difference in the players’ MVIC of the knee extensor (exercised muscle) was observed between CON and RAM trials. The greater sprints decrement in RAM was also not likely to be due to greater fatigue within the CNS pathways since there was no drastic change in the hand-grip (non-exercised muscle) MVIC measure throughout the RAM trial. Given these observations and the fact that the decrement in sprints performance was already evident very early in the mLIST (which precludes the involvement of the peripheral limitations such as lack of endogenous substrate or excessive dehydration), it is thus reasoned that the negative effect of RAM on physical performance is primarily due to placebo (or nocebo effects) of performing the Ramadan fast per se. Nocebo is defined as the change arising from an individual’s negative perceptions about the likely outcome from receiving a (negative) treatment, vis-à-vis, observance of the Ramadan fast [
37,
38]. Players in the present study have been observing Ramadan fast annually for many years. The individual’s prior experience as to how he feels when exercising in the Ramadan-fasted state (presumably negative experience since exercise in the Ramadan-fasted state is physiologically challenging [
1,
2]) would have played a contributory role or even reinforced the nocebo response. Thus the players’ own expectations of a poorer performance is deemed as the primary cause of the relatively slower sprints in the RAM trial. Owing to the difficulty in defining the boundaries of consciousness, it is uncertain whether the fasted players were deliberately or unconsciously lowering their sprint efforts during the mLIST, in particular during the early stages of the mLIST. Interestingly, it was calculated that the percentage differences in the mean sprint times between RAM and both CON trials ranged between 2.9% to 5.5% across the four exercise blocks (
Figure 4), which were within the magnitude of the impact placebo, estimated to be 1% to 5% [
37].


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}