Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. High-Intensity Functional Training Intervention
2.4. Aerobic Capacity
2.5. Anaerobic Capacity
2.6. Maximal Strength
2.7. Work Capacity
2.8. Statistical Analyses
3. Results
3.1. Intervention Adherence
3.2. Baseline Relationships
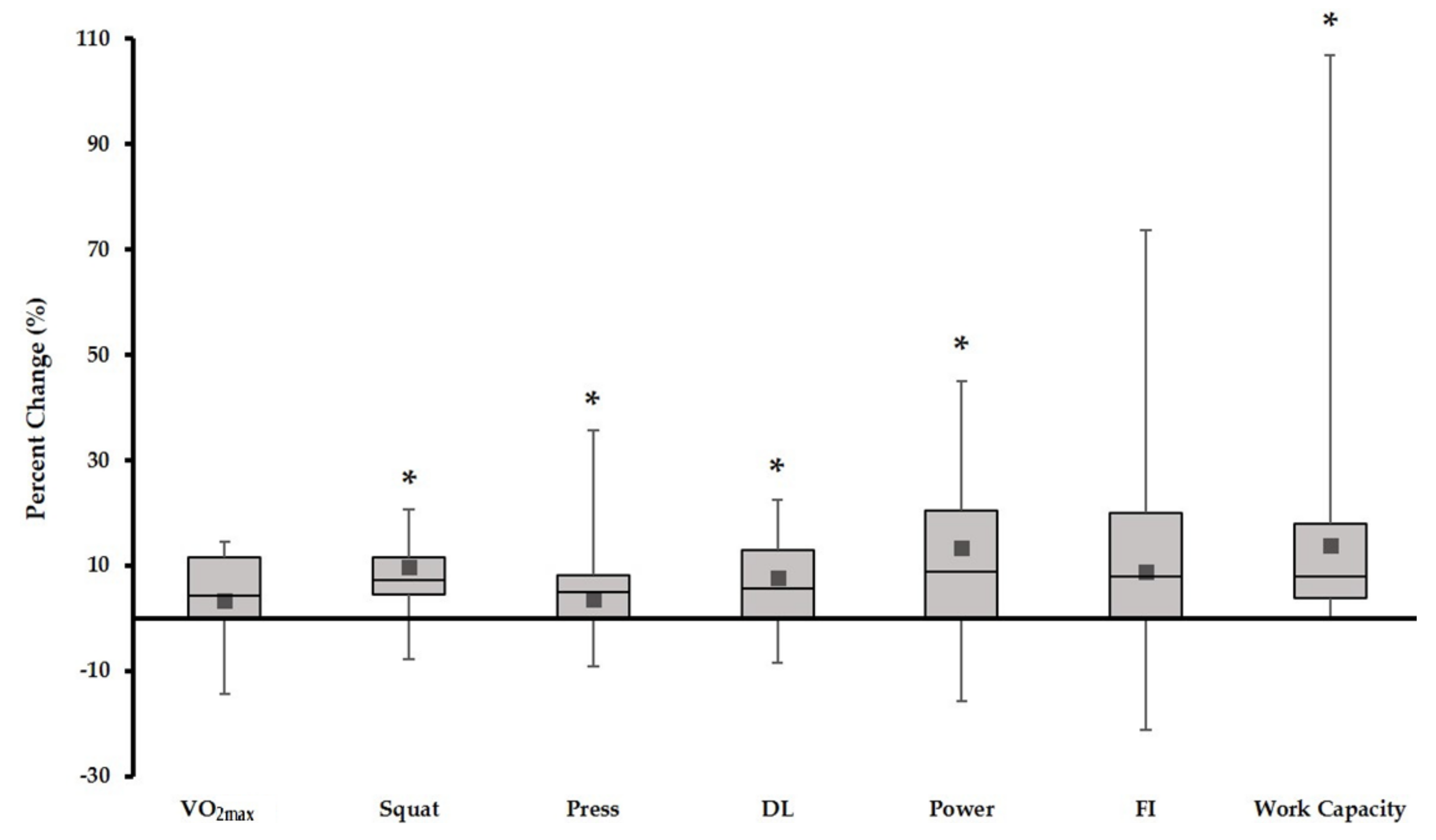
3.3. Effects on Physiologic Measures of Fitness
3.3.1. Aerobic Capacity
3.3.2. Anaerobic Capacity
3.3.3. Maximal Strength
3.3.4. Work Capacity
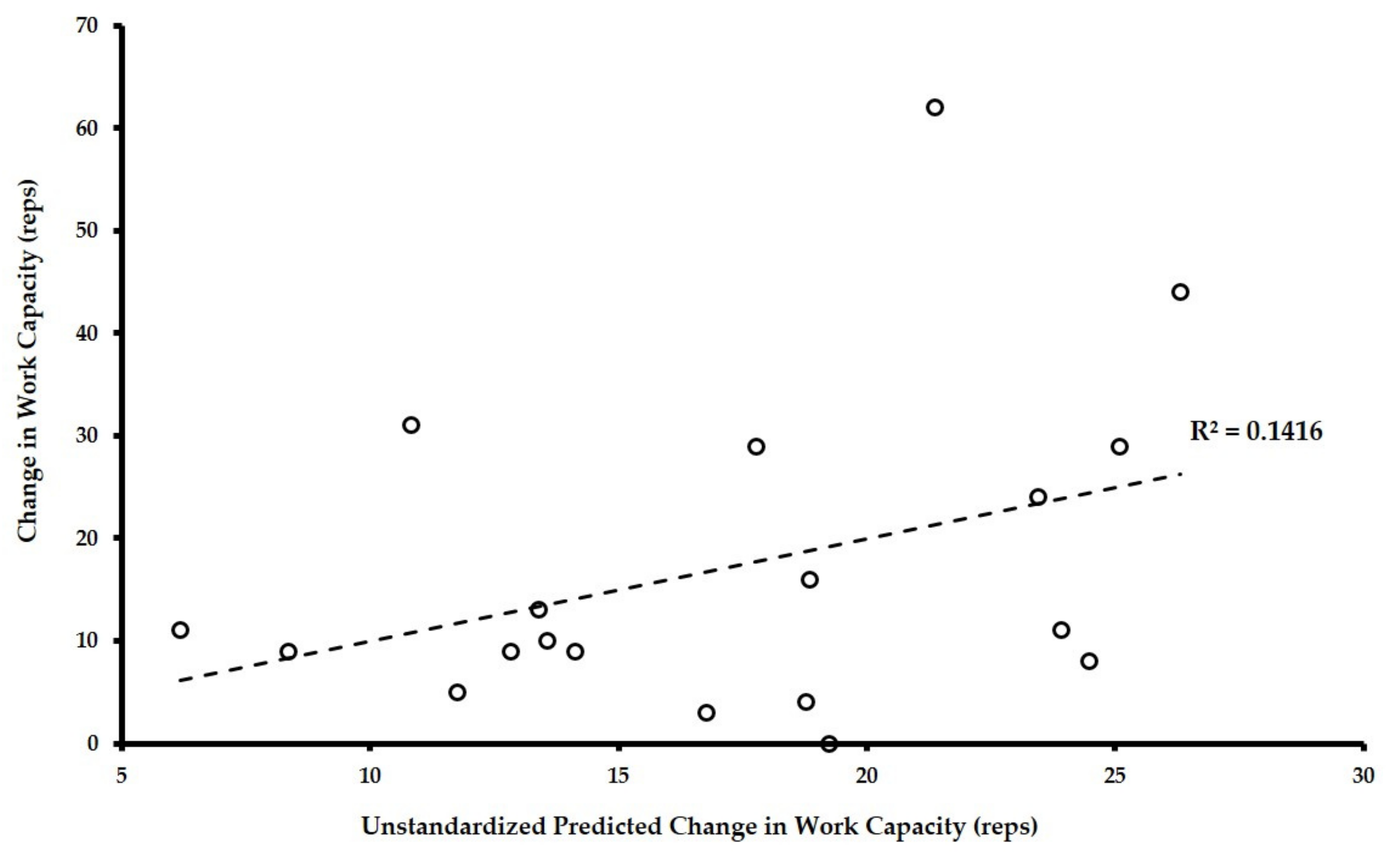
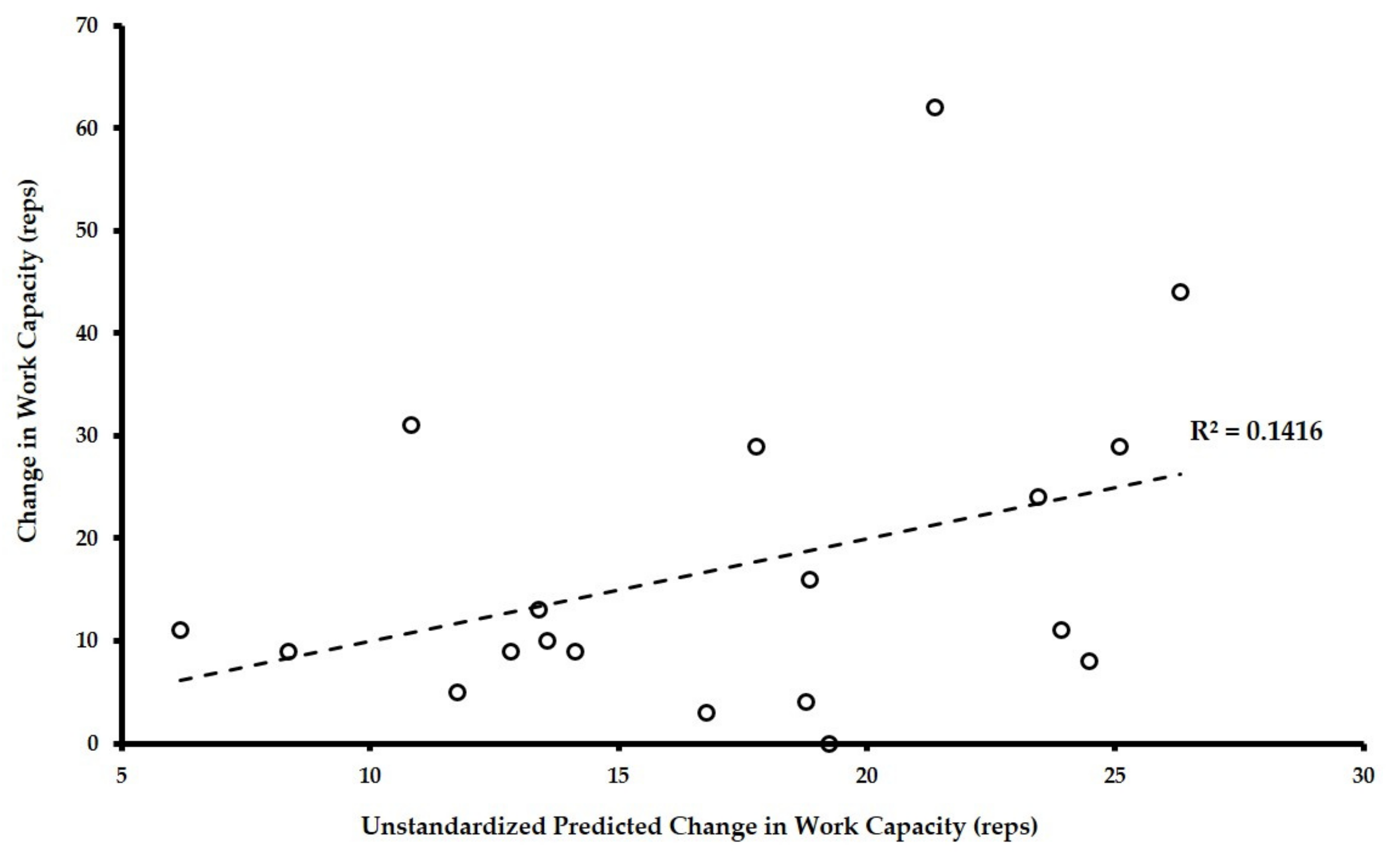
3.4. Relationship of Change in Physiologic Measures of Fitness and Change in Work Capacity
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Day | Structure | Workout of the Day * |
|---|---|---|
| 1 | M | Two mile Run (no time cap) |
| 2 | GW | (8 Push Press (135/95 lbs) + 8 Pull-Ups) × 5 rounds for time |
| 3 | MGW | (12 Goblet Squats (45/25 lbs) + 12 Burpees + 24 Calorie Row) AMRAP in 10 min |
| 4 | MG | (400 meter Run + 25 Box Jumps (18/12 inches)) × 3 rounds for time |
| 5 | W | Deadlift 5-5-5-5-5 working up to target 85% of 1RM |
| 6 | G | Kipping Pull-Up practice for 20 min |
| 7 | WM | (10 Thrusters (135/95 lbs) + 100 Double Unders) × 4 rounds for time |
| 8 | GWM | (6 Handstand Push-Ups + 12 Deadlifts (185/135 lbs) + 500 meter Row) AMRAP in 12 min |
| 9 | GW | (15 Ring Rows + 20 Wall Balls (20/14 lbs)) × 4 rounds for time |
| 10 | M | 8 km Partner Row (no time cap) |
| 11 | W | Front Squat 1-1-1-1-1-1-1-1-1-1 working up to target a 1RM |
| 12 | MG | (400 meter Run + 20 Push-Ups) × 5 rounds for time |
| 13 | WMG | (5 Cleans (135/95 lbs) + 10 Pull-Ups + 15 Double Unders) AMRAP in 15 min |
| 14 | WM | (10/20 − 8/16 − 6/12 − 4/8 − 2/4 repetitions of Power Clean/Calorie Row) for time |
| 15 | G | Handstand Push-Up Practice for 20 min |
| 16 | W | Squat 3-3-3-3-3-3-3 working up to target 90% 1RM |
| 17 | MG | (800 meter Run + 25 Sit-Ups) × 3 rounds for time |
| 18 | MGW | (50 Double Unders + 5 Box Jumps (18/12 inches) + 15 Ball Slams (20/14 lbs)) AMRAP in 15 min |
| 19 | GW | (6 Strict Pull-Ups + 6 Front Squats (50% Squat 1RM)) × 4 rounds for time |
| 20 | M | Two mile Run (no time cap) |
| 21 | M | Tabata Double Unders × 2 |
| 22 | GW | (Maximum repetitions Handstand Push-Ups + 6 Deadlifts (75% 1RM)) × 5 rounds for time |
| 23 | GWM | (20 Sit-Ups + 16 Dumbbell Clean and Jerk (45/20 lbs) + 20 Calorie Row) AMRAP in 15 min |
| 24 | WM | (30 Kettlebell Swings (45/20 lbs) + 400 meter Run) × 5 rounds for time |
| 25 | G | Strict Pull-Up Practice (Loaded) for 25 min |
| 26 | G | Muscle Up Practice for 25 min |
| 27 | WM | (6 Squats (50% 1RM) + 50 Double Unders) × 4 rounds for time |
| 28 | WMG | (12 Goblet Squats (45/25 lbs) + 12 Burpees + 24 Calorie Row) AMRAP in 10 min |
| 29 | MG | (400 meter Run + 10 Handstand Push-Ups) × 5 rounds for time |
| 30 | W | Clean 1-1-1-1-1-1-1-1-1-1 working up to target 1RM |
References
- Hak, P.T.; Hodzovic, E.H.; Hickey, B. The nature and prevalence of injury during CrossFit training. J. Strength Cond. Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Serafini, P.; Hoffstetter, W.; Mimms, H.; Smith, M.; Kliszczewicz, B.; Feito, Y. Body composition and strength changes following 16-weeks of high-intensity functional training. Med. Sci. Sports Exerc. 2016, 48, 1001. [Google Scholar] [CrossRef]
- Sobrero, G.L.; Inman, C.; Stone, W.; Zagdsuren, B.; Arnett, S.W.; Shafer, M.A.; Lyons, S.T.; Maples, J.; Crandall, J.; Callahan, Z. CrossFit vs. circuit-trained individuals: Effects of a ten-week training program on body composition and bone mineral density. Med. Sci. Sports Exerc. 2015, 47, 800. [Google Scholar] [CrossRef]
- Zagdsuren, B.; Sobrero, G.; Inman, C.; Arnett, S.; Schafer, M.; Lyons, S.; Maples, J.; Crandall, J.; Callahan, Z. CrossFit vs. circuit-training: Effects of a ten-week training program on aerobic, anaerobic, and flexibility indicators. Med. Sci. Sports Exerc. 2015, 47, 801. [Google Scholar] [CrossRef]
- McKenzie, M.J. CrossFit improves measures of muscular strength and power in active young females. Med. Sci. Sports Exerc. 2015, 47, 797. [Google Scholar] [CrossRef]
- Brown, J.T.; Sobrero, G.L.; Inman, C.; Stone, W.; Zagdsuren, B.; Arnett, S.W.; Schafer, M.A.; Maples, J.; Crandall, J.; Callahan, Z. CrossFit vs. circuit-trained individuals: Effects of a ten-week training program on muscular strength and endurance. Med. Sci. Sports Exerc. 2015, 47, 800. [Google Scholar] [CrossRef]
- Drake, N.B.; Smeed, J.; Carper, M.J.; Crawford, D.A. Effects of short-term CrossFit training: A magnitude-based approach. J. Exerc. Physiol. Online 2017, 20, 111–133. [Google Scholar]
- CrossFit Level 1 Training Guide; CrossFit Inc.: Washington, DC, USA, 2017.
- Haddock, C.K.; Poston, W.S.C.; Heinrich, K.M.; Jahnke, S.A.; Jitnarin, N. The benefits of high-intensity functional training fitness programs for military personnel. Mil. Med. 2016, 181, e1508–e1514. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, K.M.; Spencer, V.; Fehl, N.; Poston, W.S.C. Mission Essential Fitness: Comparison of Functional Circuit Training to Traditional Army Physical Training for Active-Duty Military. Mil. Med. 2012, 177, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, K.M.; Becker, C.; Carlisle, T.; Gilmore, K.; Hauser, J.; Frye, J.; Harms, C.A. High-intensity functional training improves functional movement and body composition among cancer survivors: A pilot study. Eur. J. Cancer Care 2015, 24, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.; Neydely, T.; Horvey, K.; Benko, C. Do physiological measures predict selected CrossFit benchmark performance? Open Access J. Sports Med. 2015, 6, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Dankel, S.J.; Buckner, S.L.; Jessee, M.B.; Mouser, J.G.; Mattocks, K.T.; Abe, T.; Loenneke, J.P. Correlations do not show cause and effect: Not even for changes in muscle size and strength. Sports Med. 2018, 48, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bruce, R.; Hosmer, D. Maximal oxygen intake and nomographic assessment of function aerobic impairment in cardiovascular disease. Am. Heart J. 1973, 85, 546–562. [Google Scholar] [CrossRef]
- Foster, C.; Jackson, A.S.; Pollack, M.L.; Taylor, M.M.; Hare, J.; Sennett, S.M.; Rod, J.L.; Sarwar, M.; Schmidt, D.H. Generalized equations for predicting functional capacity from treadmill performance. Am. Heart J. 1984, 107, 1229–1234. [Google Scholar] [CrossRef]
- Bar-Or, O. The Wingate Anaerobic Test an update on methodology, reliability and validity. Sports Med. 1987, 4, 381–394. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M. Principles of test selection and administration. In Essentials of Strength Training and Conditioning, 4th ed.; Haff, G.G., Triplett, N.T., Eds.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Beaver, W.L.; Lamarra, N.; Wasserman, K. Breath-by-breath measurement of true alveolar gas exchange. J. Appl. Physiol. 1981, 51, 1662–1675. [Google Scholar] [CrossRef] [PubMed]
- Serafini, P.R.; Feito, Y.; Mangine, G.T. Self-reported measures of strength and sport-specific skills distinguish ranking in an international online fitness competition. J. Strength Cond. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bellar, D.; Hatchett, A.; Judge, L.W.; Breaux, M.E.; Marcus, L. The relationship of aerobic capacity, anaerobic peak power and experience to performance in HIT exercise. Biol. Sport 2015, 32, 315–320. [Google Scholar] [CrossRef] [PubMed]
- La Scala Teixeira, C.V.; Evangelista, A.L.; Novaes, J.S.; Da Silva Grigoletto, M.E.; Behm, D.G. “You’re only as strong as your weakest link”: A current opinion about the concepts and characteristics of functional training. Front. Physiol. 2017, 8, 643. [Google Scholar] [CrossRef] [PubMed]

| Mn (SD) | WC | VO2 | Sq | P | DL | PP | FI | |
|---|---|---|---|---|---|---|---|---|
| Baseline Values (n = 25) | ||||||||
| 1. Work Capacity (reps) | 132.8 ± 32.4 | - | - | - | - | - | - | - |
| 2. VO2max (mL/kg−1/min−1) | 43.2 ± 6.9 | 0.598 ** | - | - | - | - | - | - |
| 3. Squat 1RM (kg) | 104.4 ± 44.8 | 0.653 ** | 0.352 | - | - | - | - | - |
| 4. Press 1RM (kg) | 46.7 ± 21.3 | 0.656 ** | 0.351 | 0.925 ** | - | - | - | - |
| 5. Deadlift 1RM (kg) | 118.8 ± 47.8 | 0.673 ** | 0.372 | 0.961 ** | 0.957 ** | - | - | - |
| 6. Peak Power (W) | 661.6 ± 258.4 | 0.571 ** | 0.407 * | 0.893 ** | 0.939 ** | 0.890 ** | - | - |
| 7. Fatigue Index (%) | 57.5 ± 9.6 | −0.016 | −0.050 | 0.122 | 0.336 | 0.207 | 0.397 * | - |
| Post-Intervention Values (n = 19) | ||||||||
| 1. Work Capacity (reps) | 153.5 ± 32.3 | - | - | - | - | - | - | - |
| 2. VO2max (mL/kg−1/min−1) | 44.6 ± 7.6 | 0.799 ** | - | - | - | - | - | - |
| 3. Squat 1RM (kg) | 109.3 ± 47.5 | 0.827 ** | 0.482 * | - | - | - | - | - |
| 4. Press 1RM (kg) | 48.0 ± 23.1 | 0.866 ** | 0.487 * | 0.945 ** | - | - | - | - |
| 5. Deadlift 1RM (kg) | 124.1 ± 53.1 | 0.892 ** | 0.552 * | 0.981 ** | 0.966 ** | - | - | - |
| 6. Peak Power (W) | 747.8 ± 284.3 | 0.736 ** | 0.330 | 0.905 ** | 0.846 ** | 0.872 ** | - | - |
| 7. Fatigue Index (%) | 59.9 ± 6.6 | 0.129 | −0.056 | 0.191 | 0.177 | 0.193 | 0.454 * | - |
| Variable | β-Coefficient | Standard Error | 95% CI of β | Significance |
|---|---|---|---|---|
| Overall Model | - | - | - | 0.908 |
| ΔVO2max (mL/kg−1/min−1) | 0.684 | 1.28 | −1.81, 3.18 | 0.605 |
| Δ Squat (kg) | −0.395 | 0.81 | −1.97, 1.18 | 0.638 |
| Δ Press (kg) | −1.068 | 1.16 | −3.33, 1.20 | 0.379 |
| Δ Deadlift (kg) | 0.326 | 0.52 | −0.68, 1.33 | 0.545 |
| Δ Peak Power (W) | −0.035 | 0.05 | −0.12, 0.12 | 0.518 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crawford, D.A.; Drake, N.B.; Carper, M.J.; DeBlauw, J.; Heinrich, K.M. Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures? Sports 2018, 6, 26. https://doi.org/10.3390/sports6020026
Crawford DA, Drake NB, Carper MJ, DeBlauw J, Heinrich KM. Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures? Sports. 2018; 6(2):26. https://doi.org/10.3390/sports6020026
Chicago/Turabian StyleCrawford, Derek A., Nicholas B. Drake, Michael J. Carper, Justin DeBlauw, and Katie M. Heinrich. 2018. "Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures?" Sports 6, no. 2: 26. https://doi.org/10.3390/sports6020026
APA StyleCrawford, D. A., Drake, N. B., Carper, M. J., DeBlauw, J., & Heinrich, K. M. (2018). Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures? Sports, 6(2), 26. https://doi.org/10.3390/sports6020026