The Combined Elevation Test (CET) in Adolescent School Children: A Pilot Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
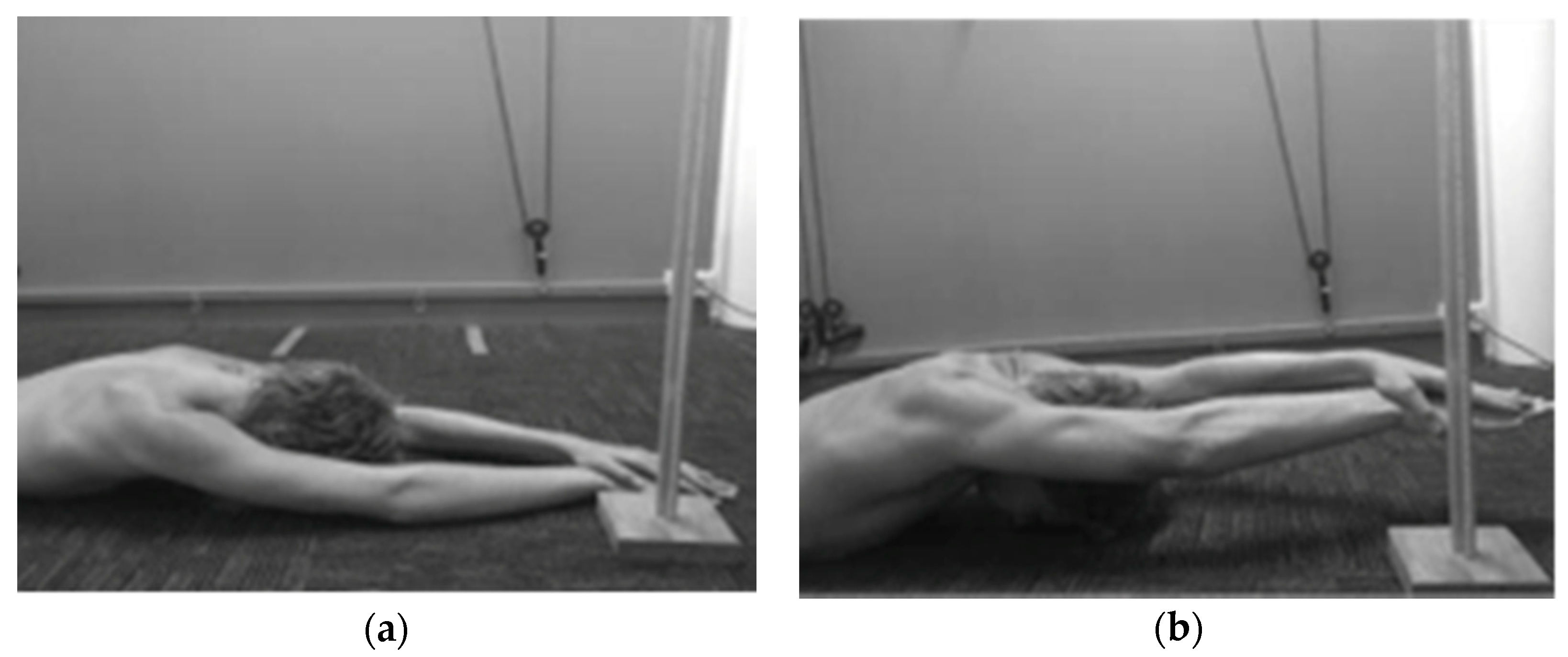
2.2. Equipment
2.3. Testing Procedure
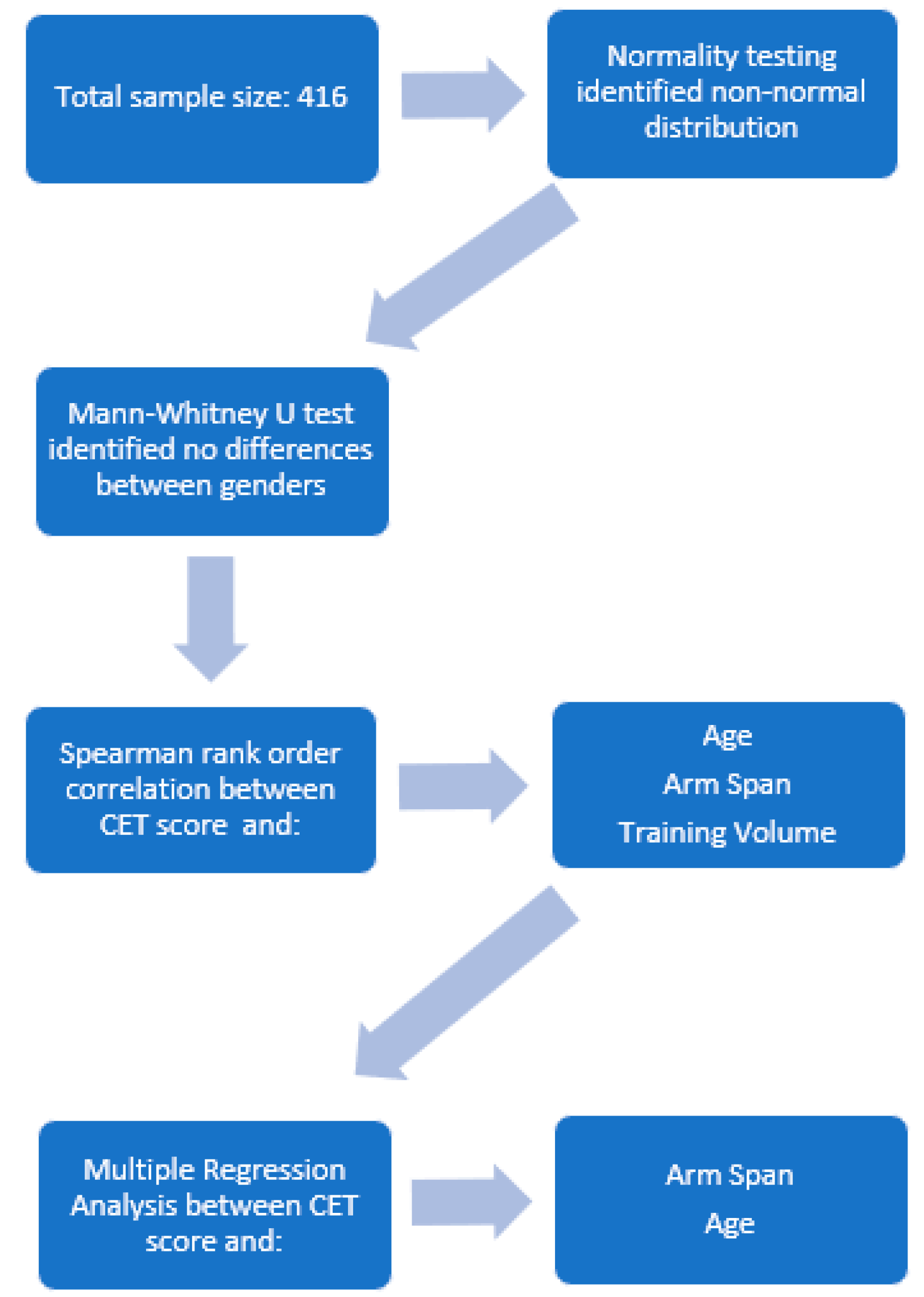
2.4. Data Analysis
3. Results
3.1. Reliability Analysis
3.2. Participant Demographics
3.3. Comparative Analysis for Males vs. Females
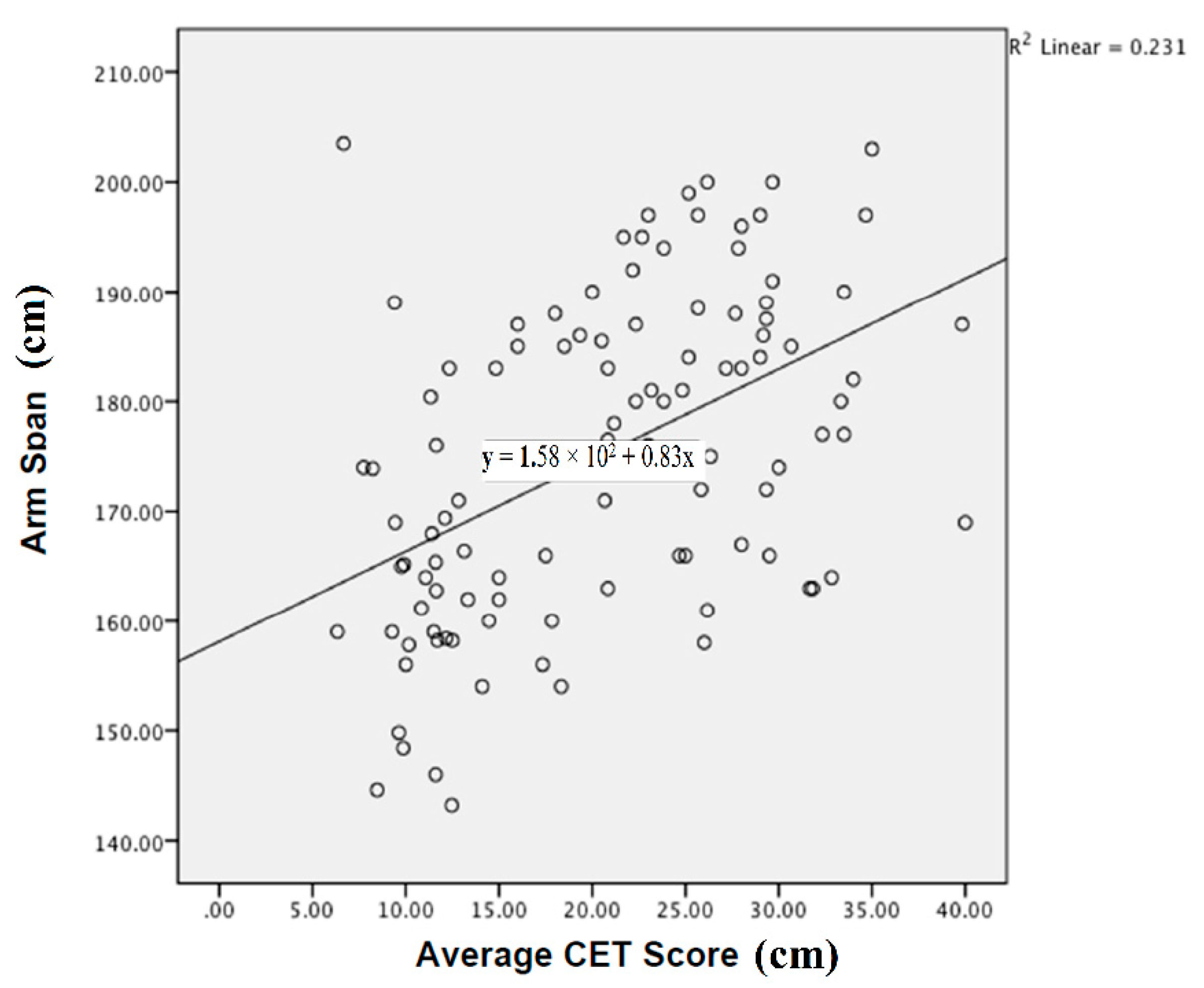
3.4. Correlations between CET Scores and Key Variables: Arm Span, Age, and Average Training Volume
3.5. Multiple Regression Analysis: Influence of Arm Span and Age on CET Scores
3.6. Standardized CET Scores Based on Age and Arm Span
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- DiFiori, J.P. Overuse injuries in children and adolescents. Physician Sports Med. 1999, 27, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Dennis, R.J.; Finch, C.F.; Elliott, B.C.; Farhart, P.J. The reliability of musculoskeletal screening tests used in cricket. Phys. Ther. Sport 2008, 9, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.; Collins, M.; Posthumus, M. Risk factors for shoulder pain and injury in swimmers: A critical systematic review. Phys. Sports Med. 2015, 43, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Sein, M.L.; Walton, J.; Linklater, J.; Appleyard, R.; Kirkbride, B.; Kuah, D.; Murrell, G.A.C. Shoulder pain in elite swimmers: Primarily due to swim-volume-induced supraspinatus tendinopathy. Br. J. Sports Med. 2010, 44, 105. [Google Scholar] [CrossRef] [PubMed]
- Blanch, P. Conserative management of shoulder pain in swimming. Phys. Ther. Sport 2004, 5, 109–124. [Google Scholar] [CrossRef]
- Johnson, K.D.; Kim, K.-M.; Yu, B.-K.; Saliba, S.A.; Grindstaff, T.L. Reliability of thoracic spine rotation range of motion measurements in healthy adults. J. Athl. Train. 2012, 47, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Furness, J.; Climstein, M.; Sheppard, J.M.; Abbott, A.; Hing, W. Clinical methods to quantify trunk mobility in an elite male surfing population. Phys. Ther. Sport 2016, 19, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Phillips, G.; McCaig, S. A biomechanical evaluation of the combined elevation test. Phys. Ther. Sport 2017, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dennis, R.J.; Finch, C.F.; McIntosh, A.S.; Elliott, B.C. Use of field-based tests to identify risk factors for injury to fast bowlers in cricket. Br. J. Sports Med. 2008, 42, 477. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Marshall, N.; Abbott, A. Shoulder pain and dysfunction in young surf lifesavers. Phys. Ther. Sport 2015, 16, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Bak, K.; Magnusson, S.P. Shoulder strength and range of motion in symptomatic and pain-free elite swimmers. Am. J. Sports Med. 1997, 25, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Beach, M.L.; Whitney, S.L.; Dickoff-Hoffman, S. Relationship of shoulder flexibility, strength, and endurance to shoulder pain in competitive swimmers. J. Orthop. Sports Phys. Ther. 1992, 16, 262–268. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J. Normative data: Their definition, interpretation, and importance for primary care physicians. Fam. Med. 1990, 22, 307–311. [Google Scholar] [PubMed]
- McGill, S.; Melanie, B.; Crosby, I.; Russell, C. Clinical tools to quantify torso flexion endurance: Normative data from student and firefighter populations. Occup. Ergon. 2010, 9, 55–61. [Google Scholar]
- Alaranta, H.; Hurri, H.; Heliovaara, M.; Soukka, A.; Harju, R. Flexibility of the spine—Normative values of goniometric and tape measurements. Scand. J. Med. Sci. Sports 1994, 26, 147–154. [Google Scholar]
- Lexell, J.E.; Downham, D.Y. How to assess the reliability of measurements in rehabilitation. Am. J. Phys. Med. Rehabil. 2005, 84, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Rikken-Bultman, D.G.A.; Wellink, L.; van Dongen, P.W.J. Hypermobility in two Dutch school poulations. Eur. J. Obstet. Gynecol. Reprod. Biol. 1997, 73, 189–192. [Google Scholar] [CrossRef]
- Saavedra, J.M.; Escalante, Y.; Rodriguez, F.A. A multivariate analysis of performance in young swimmers. Pediatr. Exerc. Sci. 2010, 22, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Moura, T.; Costa, M.; Oliveira, S.; Junior, M.B.; Ritti-Dias, R.; Santos, M. Height and body composition determine arm propulsive force in youth swimmers independent of a maturation stage. J. Hum. Kinet. 2014, 42, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Webber, C.E.; Barr, R.D. Age- and gender-dependent values of skeletal muscle mass in healthy children and adolescents. J. Cachexia Sarcopenia Muscle 2012, 3, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Geladas, N.D.; Nassis, G.P.; Pavlicevic, S. Somatic and physical traits affecting sprint swimming performance in young swimmers. Int. J. Sports Med. 2005, 26, 139–144. [Google Scholar] [CrossRef] [PubMed]
- McMaster, W.; Roberts, A.; Stoddard, T. A correlation between shoulder laxity and interfering pain in competitive swimmers. Am. J. Sports Med. 1998, 26, 83–86. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| n | Mean(SD) | n | Mean(SD) | n | Mean(SD) | |
| <10 | 2 | 18.83(0.94) | 0 | 0(0) | 2 | 18.83(0.94) |
| 11 | 6 | 20.36(6.90) | 9 | 17.11(6.09) | 15 | 18.4(6.40) |
| 12 | 33 | 18.47(8.23) | 27 | 19.05(6.80) | 60 | 18.73(7.56) |
| 13 | 36 | 16.34(6.09) | 47 | 18.39(6.82) | 83 | 17.5(6.56) |
| 14 | 37 | 16.97(6.42) | 29 | 16.52(8.56) | 66 | 16.78(7.38) |
| 15 | 66 | 19.84(8.55) | 38 | 24.0(8.54) | 104 | 21.35(8.74) |
| 16 | 39 | 22.21(5.73) | 20 | 23.8(5.68) | 59 | 22.75(5.71) |
| 17 | 14 | 24.24(6.79) | 10 | 20.23(7.20) | 24 | 22.57(7.10) |
| 18 | 1 | 33.00(0) | 2 | 28.08(14.02) | 3 | 29.72(10.31) |
| Total | 234 | 19.38(7.53) | 182 | 20.09(7.89) | 416 | 19.69(7.69) |
| Age (Years) | Arm Span (cm) | Average CET Score (cm) | CET Range (cm) |
|---|---|---|---|
| 10–12 (n = 27) | 140–154 | 12.5 ± 3.5 | 8.4–18.3 |
| 155–169 | 16.3 ± 7.5 | 6.3–29.5 | |
| 170–184 | 22.0 ± 6.4 | 12.8–27.1 | |
| 13–15 (n = 42) | 150–164 | 15.65 ± 7.7 | 9.3–31.8 |
| 165–179 | 19.7 ± 10.4 | 7.7–40.0 | |
| 180–194 | 24.2 ± 11.1 | 9.4–39.8 | |
| 16–18 (n = 36) | 160–174 | 27.2 ± 5.8 | 17.8–32.8 |
| 175–189 | 24.0 ± 5.5 | 14.5–33.5 | |
| 190–205 | 30.3 ± 4.4 | 26.2–35.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furness, J.; Schram, B.; Corea, D.; Turner, Z.; Cairns, H. The Combined Elevation Test (CET) in Adolescent School Children: A Pilot Study. Sports 2018, 6, 64. https://doi.org/10.3390/sports6030064
Furness J, Schram B, Corea D, Turner Z, Cairns H. The Combined Elevation Test (CET) in Adolescent School Children: A Pilot Study. Sports. 2018; 6(3):64. https://doi.org/10.3390/sports6030064
Chicago/Turabian StyleFurness, James, Ben Schram, Darren Corea, Zachary Turner, and Hannah Cairns. 2018. "The Combined Elevation Test (CET) in Adolescent School Children: A Pilot Study" Sports 6, no. 3: 64. https://doi.org/10.3390/sports6030064
APA StyleFurness, J., Schram, B., Corea, D., Turner, Z., & Cairns, H. (2018). The Combined Elevation Test (CET) in Adolescent School Children: A Pilot Study. Sports, 6(3), 64. https://doi.org/10.3390/sports6030064