Decision Making within the Built Environment as a Strategy for Mitigating the Risk of Malaria and Other Vector-Borne Diseases



Abstract
1. Introduction
2. Review of Closely Related Work
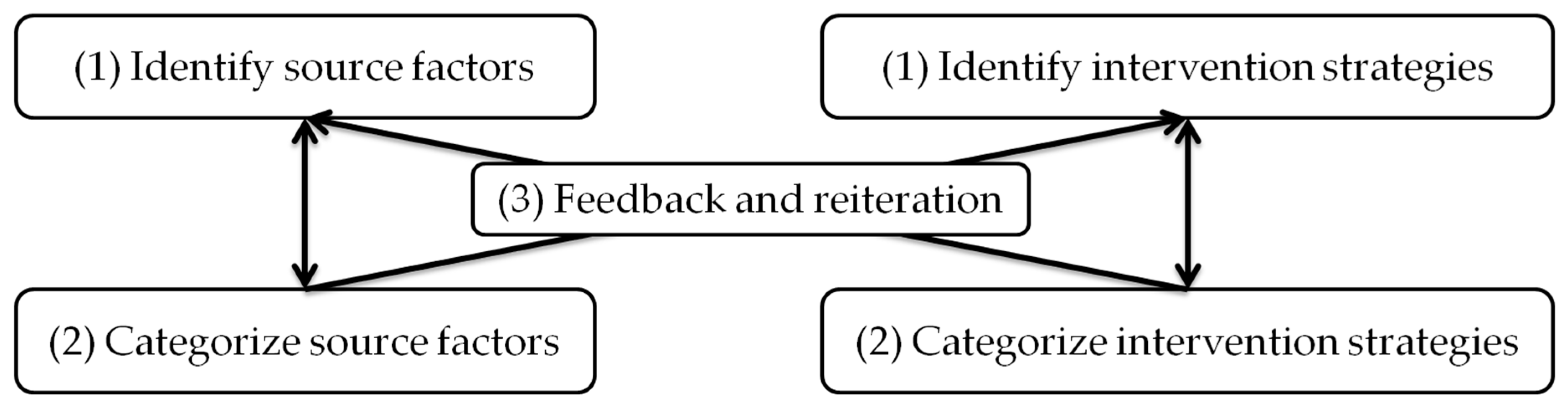
3. Methodology
4. Key Findings
4.1. Broader Cross-Disciplinary Synergies are Critical to Managing the Interdependencies and Complexities of Malaria Risk Factors
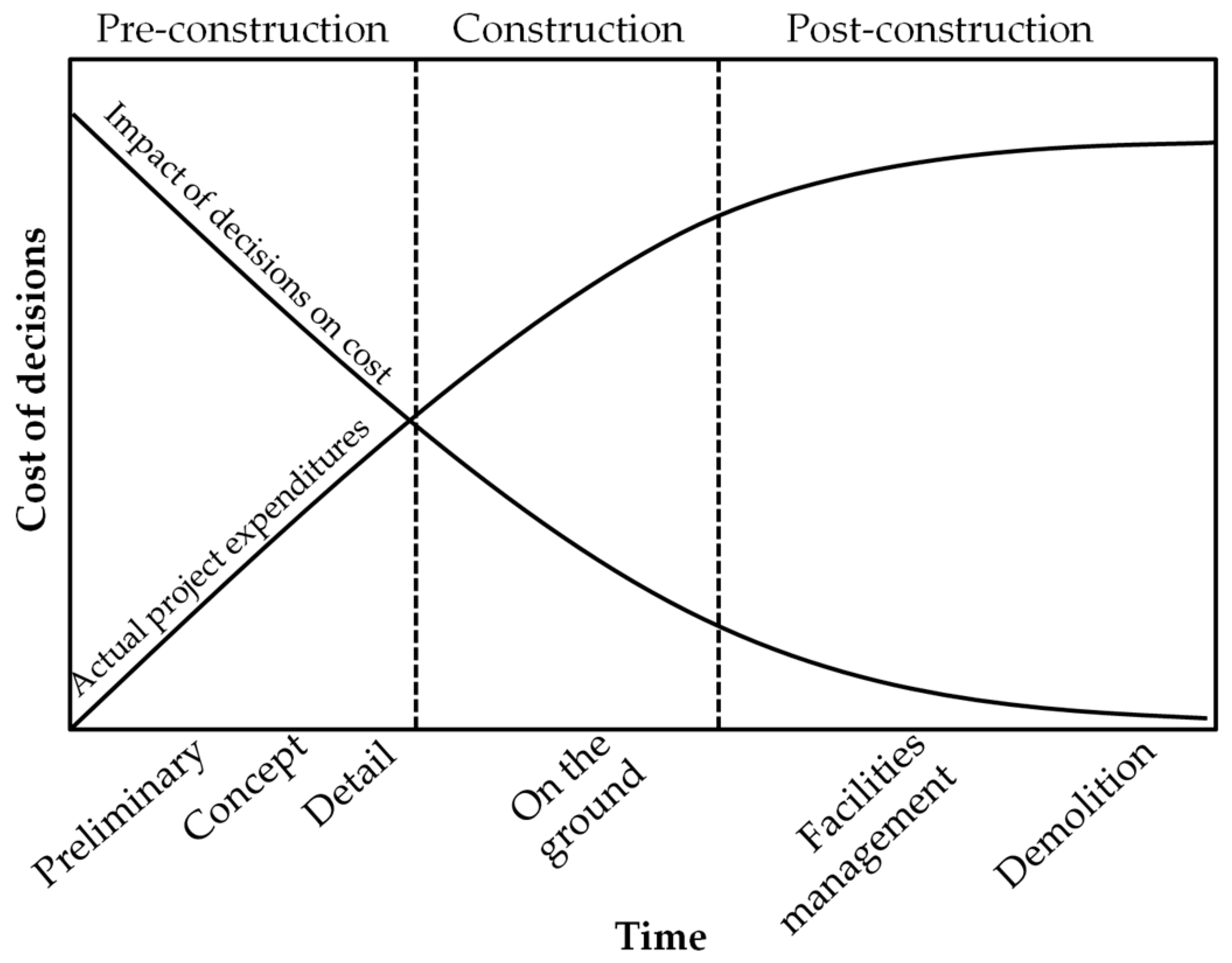
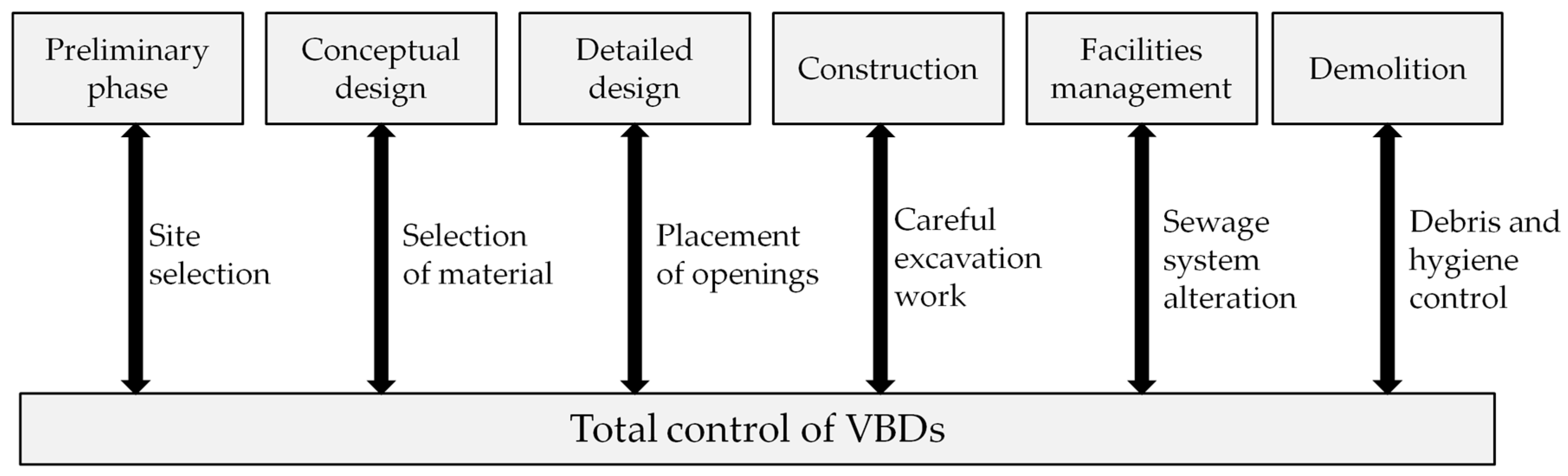
4.2. There Is an Opportunity to Catalyze Transformative Impact in the Mitigation of the Risk of Malaria through Leveraging the Life Cycle of Buildings
- (1)
- Preliminary Phase: Selection of a site near an open surface water body may increase the number of breeding sites for the malaria vector;
- (2)
- Conceptual Design: The placement and size of openings as well as the orientation of the building envelopes affects the vector accessibility both into and out of the building;
- (3)
- Detailed Design: Certain types of material on housing features, such as mud walls, thatched roofs, and earth, sand, dung, and stone flooring, increase vector attraction into the site [61];
- (4)
- Construction: Excavation work results in opportunities for several pools of stagnant water to form—such pools are ideal breeding grounds for mosquitoes;
- (5)
- Facilities Management: Drains and ditches are common habitats for mosquitoes to breed [62]; poorly installed pipes and drain blockage can lead to poor sanitation or reduced water flow. The accumulated stagnant water can become a favorable habitat, and;
- (6)
- End of Life/Disuse: Construction and demolition waste contributes to the environmental problem of landfills.
4.3. There Is a Need for a Decision Support System That Can Be Used by Built Environment Professionals to Manage the Interdependencies and Complexities of Malaria Risk Factors
5. Discussion and Further Work
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Fact Sheet about Malaria. Available online: https://www.who.int/malaria/en/ (accessed on 30 September 2017).
- HIV/AIDS Data and Statistics. Available online: https://www.who.int/hiv/data/en/ (accessed on 30 September 2017).
- World Health Organization. Global Tuberculosis Report. Available online: https://www.who.int/tb/publications/global_report/MainReport_18Sept2018.pdf (accessed on 30 September 2018).
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 30 September 2018).
- World Health Organization. Global Leprosy Programme. Available online: http://www.searo.who.int/entity/global_leprosy_programme/en/ (accessed on 30 September 2018).
- World Health Organization. Ebola Virus Disease. Available online: https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease (accessed on 30 September 2018).
- World Health Organization. Global Technical Strategy for Malaria 2016–2030. Available online: https://www.who.int/malaria/areas/global_technical_strategy/en/ (accessed on 30 September 2018).
- World Health Organization. World Malaria Report 2016. Available online: https://www.who.int/malaria/publications/world-malaria-report-2016/report/en/ (accessed on 2 November 2018).
- Roser, M.; Ritchie, H. Malaria. Available online: https://ourworldindata.org/malaria (accessed on 30 September 2018).
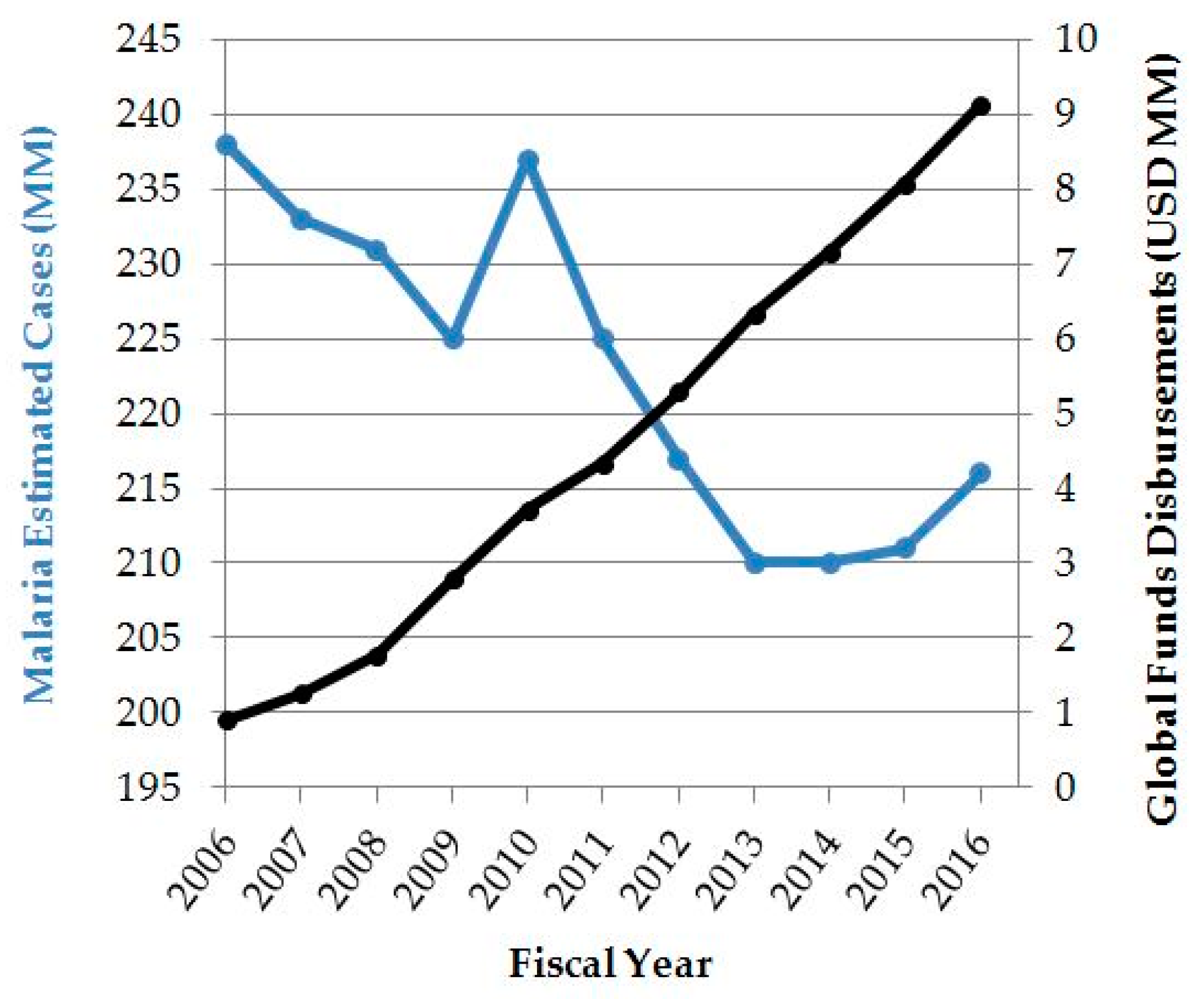
- The Global Fund. Financials. Available online: https://www.theglobalfund.org/en/financials/ (accessed on 14 April 2018).
- World Health Organization. World Malaria Report 2017. Available online: https://www.who.int/malaria/publications/world-malaria-report-2017/en/ (accessed on 2 November 2018).
- World Health Organization. World Malaria Report 2010. Available online: https://www.who.int/malaria/world_malaria_report_2010/en/ (accessed on 2 November 2018).
- Sustainable Development Goals Knowledge Platform. Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 1 November 2018).
- World Health Organization. Sustainable Cities: Health at the Heart of Urban Development. Available online: https://www.who.int/sustainable-development/cities/Factsheet-Cities-sustainable-health.pdf (accessed on 30 October 2018).
- United Nations General Assembly. Draft outcome document of the United Nations Conference on Housing and Sustainable Urban. Development (Habitat III). In Proceedings of the Habitat III Conference, Quito, Ecuador, 17–20 October 2016. [Google Scholar]
- Tusting, L.S.; Ippolito, M.M.; Willey, B.A.; Kleinschmidt, I.; Dorsey, G.; Gosling, R.D.; Lindsay, S.W. The evidence for improving housing to reduce malaria: A systematic review and meta-analysis. Malar. J. 2015, 14, 209. [Google Scholar] [CrossRef] [PubMed]
- Menger, D.J.; Otieno, B.; de Rijk, M.; Mukabana, W.R.; van Loon, J.J.; Takken, W. A push-pull system to reduce house entry of malaria mosquitoes. Malar. J. 2014, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.; Marshall, J. Factors Contributing to Urban. Malaria Transmission in Sub-Saharan Africa: A Systematic Review. J. Trop. Med. 2012, 2012, 10. [Google Scholar] [CrossRef] [PubMed]
- Gamage-Mendis, A.C.; Carter, R.; Mendis, C.; De Zoysa, A.P.; Herath, P.R.; Mendis, K.N. Clustering of malaria infections within an endemic population: Risk of malaria associated with the type of housing construction. Am. J. Trop. Med. Hyg. 1991, 45, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Malaria. Available online: https://www.cdc.gov/malaria/about/history/panama_canal.html# (accessed on 10 October 2017).
- Ogoma, S.B.; Kannady, K.; Sikulu, M.; Chaki, P.P.; Govella, N.J.; Mukabana, W.R.; Killeen, G.F. Window screening, ceilings and closed eaves as sustainable ways to control malaria in Dar es Salaam, Tanzania. Malar. J. 2009, 8, 221. [Google Scholar] [CrossRef] [PubMed]
- Tizifa, T.A.; Kabaghe, A.N.; McCann, R.S.; van den Berg, H.; Van Vugt, M.; Phiri, K.S. Prevention Efforts for Malaria. Curr. Trop. Med. Rep. 2018, 5, 41–50. [Google Scholar] [CrossRef]
- Mitsakakis, K.; Hin, S.; Müller, P.; Wipf, N.; Thomsen, E.; Coleman, M.; Zengerle, R.; Vontas, J.; Mavridis, K. Converging Human and Malaria Vector Diagnostics with Data Management towards an Integrated Holistic One Health Approach. Int. J. Environ. Res. Public Health 2018, 15, 259. [Google Scholar] [CrossRef]
- Mgone, C.S. Strengthening of the clinical research capacity for malaria: A shared responsibility. Malar. J. 2010, 9, S5. [Google Scholar] [CrossRef]
- Marshall, J.M.; Touré, M.B.; Traore, M.M.; Famenini, S.; Taylor, C.E. Perspectives of people in Mali toward genetically-modified mosquitoes for malaria control. Malar. J. 2010, 9, 128. [Google Scholar] [CrossRef]
- Atkinson, J.A.; Vallely, A.; Fitzgerald, L.; Whittaker, M.; Tanner, M. The architecture and effect of participation: A systematic review of community participation for communicable disease control and elimination. Implications for malaria elimination. Malar. J. 2011, 10, 225. [Google Scholar] [CrossRef]
- Wang, S.J.; Lengeler, C.; Smith, T.A.; Vounatsou, P.; Cissé, G.; Tanner, M. Rapid Urban Malaria Appraisal (RUMA) III: Epidemiology of urban malaria in the municipality of Yopougon (Abidjan). Malar. J. 2006, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Guerra, C.A.; Moyes, C.L.; Elyazar, I.A.F.; Gething, P.W.; Hay, S.I.; Tatem, A.J. The effects of urbanization on global Plasmodium vivax malaria transmission. Malar. J. 2012, 11, 403. [Google Scholar] [CrossRef]
- Vajda, E.A.; Webb, C.E. Assessing the Risk Factors Associated with Malaria in the Highlands of Ethiopia: What Do We Need to Know? Trop. Med. Infect. Dis. 2017, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Hausmann-Muela, S.; Eckl, J. Re-imagining malaria—A platform for reflections to widen horizons in malaria control. Malar. J. 2015, 14, 180. [Google Scholar] [CrossRef] [PubMed]
- Ocampo, A.J.; Chunara, R.; Brownstein, J.S. Using search queries for malaria surveillance, Thailand. Malar. J. 2013, 12, 390. [Google Scholar] [CrossRef] [PubMed]
- Tatem, A.J.; Huang, Z.; Narib, C.; Kumar, U.; Kandula, D.; Pindolia, D.K.; Smith, D.L.; Cohen, J.M.; Graupe, B.; Uusiku, P.; et al. Integrating rapid risk mapping and mobile phone call record data for strategic malaria elimination planning. Malar. J. 2014, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C. Prototype Early Warning Systems for Vector-Borne Diseases in Europe. Int. J. Environ. Res. Public Health 2015, 12, 6333–6351. [Google Scholar] [CrossRef] [PubMed]
- Ninphanomchai, S.; Chansang, C.; Hii, Y.L.; Rocklöv, J.; Kittayapong, P. Predictiveness of Disease Risk in a Global Outreach Tourist Setting in Thailand Using Meteorological Data and Vector-Borne Disease Incidences. Int. J. Environ. Res. Public Health 2014, 11, 10694–10709. [Google Scholar] [CrossRef]
- Reiter, P. Global Warming and Malaria: Knowing the Horse before Hitching the Cart. Malar. J. 2008, 7, S3. [Google Scholar] [CrossRef]
- Klinkenberg, E.; McCall, P.J.; Wilson, M.D.; Amerasinghe, F.P.; Donnelly, M.J. Impact of urban agriculture on malaria vectors in Accra, Ghana. Malar. J. 2008, 7, 151. [Google Scholar] [CrossRef]
- Hay, S.I.; Cox, J.; Rogers, D.J.; Randolph, S.E.; Stern, D.I.; Shanks, G.D.; Myers, M.F.; Snow, R.W. Climate change and the resurgence of malaria in the East African highlands. Nature 2002, 415, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Adefemi, K.; Awolaran, O.; Wuraola, C. Social and environmental determinants of malaria in under five children in Nigeria: A review. Int. J. Commun. Med. Public Health 2015, 2, 345–350. [Google Scholar] [CrossRef]
- Negev, M.; Paz, S.; Clermont, A.; Pri-Or, N.G.; Shalom, U.; Yeger, T.; Green, M.S. Impacts of Climate Change on Vector Borne Diseases in the Mediterranean Basin—Implications for Preparedness and Adaptation Policy. Int. J. Environ. Res. Public Health 2015, 12, 6745–6770. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Afrane, Y.A.; Vardo-Zalik, A.M.; Atieli, H.; Zhong, D.; Wamae, P.; Himeidan, Y.E.; Minakawa, N.; Githeko, A.K.; Yan, G. Changing Patterns of Malaria Epidemiology between 2002 and 2010 in Western Kenya: The Fall and Rise of Malaria. PLoS ONE 2011, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Lindblade, K.A.; Walker, E.D.; Onapa, A.W.; Katungu, J.; Wilson, M.L. Land use change alters malaria transmission parameters by modifying temperature in a highland area of Uganda. Trop. Med. Int. Health 2000, 5, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Tonnang, H.E.; Kangalawe, R.Y.; Yanda, P.Z. Predicting and mapping malaria under climate change scenarios: The potential redistribution of malaria vectors in Africa. Malar. J. 2010, 9, 111. [Google Scholar] [CrossRef] [PubMed]
- Edlund, S.; Davis, M.; Douglas, J.V.; Kershenbaum, A.; Waraporn, N.; Lessler, J.; Kaufman, J.H. A global model of malaria climate sensitivity: Comparing malaria response to historic climate data based on simulation and officially reported malaria incidence. Malar. J. 2012, 11, 331. [Google Scholar] [CrossRef]
- Walls, K.L.; Boulic, M.; Boddy, J.W.D. The Built Environment—A Missing Cause of the Causes of Non-Communicable Diseases. Int. J. Environ. Res. Public Health 2016, 13, 956. [Google Scholar] [CrossRef]
- Lindsay, S.W.; Emerson, P.M.; Charlwood, J.D. Reducing malaria by mosquito-proofing houses. Trends Parasitol. 2002, 18, 510–514. [Google Scholar] [CrossRef]
- Lindsay, S.W.; Jawara, M.; Paine, K.; Pinder, M.; Walraven, G.E.L.; Emerson, P.M. Changes in house design reduce exposure to malaria mosquitoes. Trop. Med. Int. Health 2003, 8, 512–517. [Google Scholar] [CrossRef]
- Allen, L.K.; Hetherington, E.; Manyama, M.; Hatfield, J.M.; van Marle, G. Using the social entrepreneurship approach to generate innovative and sustainable malaria diagnosis interventions in Tanzania: a case study. Malar. J. 2010, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Tusting, L.S.; Willey, B.; Lines, J. Building malaria out: Improving health in the home. Malar. J. 2016, 15, 320. [Google Scholar] [CrossRef] [PubMed]
- Atieli, H.; Menya, D.; Githeko, A.; Scott, T. House design modifications reduce indoor resting malaria vector densities in rice irrigation scheme area in western Kenya. Malar. J. 2009, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Njau, R.J.; de Savigny, D.; Gilson, L.; Mwageni, E.; Mosha, F.W. Implementation of an insecticide-treated net subsidy scheme under a public-private partnership for malaria control in Tanzania—Challenges in implementation. Malar. J. 2009, 8, 201. [Google Scholar] [CrossRef] [PubMed]
- Waite, J.L.; Lynch, P.A.; Thomas, M.B. Eave tubes for malaria control in Africa: A modelling assessment of potential impact on transmission. Malar. J. 2016, 15, 449. [Google Scholar] [CrossRef] [PubMed]
- Tusting, L.S.; Bottomley, C.; Gibson, H.; Kleinschmidt, I.; Tatem, A.J.; Lindsay, S.W.; Gething, P.W. Housing Improvements and Malaria Risk in Sub-Saharan Africa: A Multi-Country Analysis of Survey Data. PLoS Med. 2017, 14, e1002234. [Google Scholar] [CrossRef]
- Okumu, F. The paradigm of eave tubes: Scaling up house improvement and optimizing insecticide delivery against disease-transmitting mosquitoes. Malar. J. 2017, 16, 207. [Google Scholar] [CrossRef]
- Climate Risk and Spread of Vector-Borne Diseases. Available online: https://climatenexus.org/climate-issues/health/climate-change-and-vector-borne-diseases/ (accessed on 22 September 2016).
- Nabi, S.A.; Qader, S.S. Is Global Warming likely to cause an increased incidence of Malaria? Libyan J. Med. 2009, 4, 9–16. [Google Scholar] [CrossRef]
- United Nations. Goal 11: Make Cities Inclusive, Safe, Resilient and Sustainable. Available online: https://www.un.org/sustainabledevelopment/cities/ (accessed on 14 April 2018).
- Donnelly, M.J.; McCall, P.J.; Lengeler, C.; Bates, I.; D’Alessandro, U.; Barnish, G.; Konradesn, F.; Klinkenberg, E.; Townson, H.; Trape, J.F.; et al. Malaria and urbanization in sub-Saharan Africa. Malar. J. 2005, 4, 12. [Google Scholar] [CrossRef]
- The World Bank. Population, Total. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 14 April 2018).
- Barnes, R. Tanzania’s Housing Deficit at Three Million Units. Available online: https://constructionreviewonline.com/2015/05/tanzanias-housing-deficit-at-three-million-units/ (accessed on 2 October 2018).
- Patz, J.A.; Daszak, P.; Tabor, G.M.; Aguirre, A.A.; Pearl, M.; Epstein, J.; Wolfe, N.D.; Kilpatrick, A.M.; Foufopoulos, J.; Molyneux, D.; et al. Unhealthy landscapes: Policy recommendations on land use change and infectious disease emergence. Environ. Health Perspect. 2004, 112, 1092–1098. [Google Scholar] [CrossRef]
- Wanzirah, H.; Tusting, L.S.; Arinaitwe, E.; Katureebe, A.; Maxwell, K.; Rek, J.; Bottomley, C.; Staedke, S.G.; Kamya, M.; Dorsey, G.; et al. Mind the Gap: House Structure and the Risk of Malaria in Uganda. PLoS ONE 2015, 10, e0117396. [Google Scholar] [CrossRef] [PubMed]
- Mattah, P.A.; Futagbi, G.; Amekudzi, L.K.; Mattah, M.M.; de Souza, D.K.; Kartey-Attipoe, W.D.; Bimi, L.; Wilson, M.D. Diversity in breeding sites and distribution of Anopheles mosquitoes in selected urban areas of southern Ghana. Parasites Vectors 2017, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Why Steel. Available online: https://www.aisc.org/why-steel/resources/project-delivery-methods/ (accessed on 14 April 2018).
- Lipscomb, H.J.; Glazner, J.E.; Bondy, J.; Guarini, K.; Lezotte, D. Injuries from slips and trips in construction. Appl. Ergon. 2006, 37, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, Y.; Haile, M.; Ghebreyesus, T.A.; Witten, K.A.; Getachew, A.; Byass, P.; Lindsay, S.W. Can source reduction of mosquito larval habitat reduce malaria transmission in Tigray, Ethiopia? Trop. Med. Int. Health. 2005, 10, 12. [Google Scholar] [CrossRef]
- Sternberg, E.D.; Ng’habi, K.R.; Lyimo, I.N.; Kessy, S.T.; Farenhorst, M.; Thomas, M.B.; Knols, B.G.J.; Mnyone, L.L. Eave tubes for malaria control in Africa: Initial development and semi-field evaluations in Tanzania. Malar. J. 2016, 15, 447. [Google Scholar] [CrossRef] [PubMed]
- Huizenga, C.; Abbaszadeh, S.; Zagreus, L.; Arens, E.A. Air quality and thermal comfort in office buildings: Results of a large indoor environmental quality survey. Indoor Environmental Quality (IEQ). Proc. Healthy Build. 2006, 3, 393–397. [Google Scholar]
- Ezzati, M.; Kammen, D.M. The Health Impacts of Exposure to Indoor Air Pollution from Solid Fuels in Developing Countries: Knowledge, Gaps, and Data Needs. Environ. Health Perspect. 2002, 110, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Health as the Pulse of the New Urban Agenda: United Nations Conference on Housing and Sustainable Urban Development; WHO: Quito, Ecuador, 2016. [Google Scholar]
- Dodge Data and Analytics. The Drive Towards Healthier Buildings 2016. Available online: https://www.worldgbc.org/sites/default/files/Drive%20Toward%20Healthier%20Buildings%202016_ffff.pdf (accessed on 2 October 2018).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tropical Disease | Number of People Infected in 2016 |
|---|---|
| Malaria | 216 million |
| HIV/AIDS | 36.7 million |
| Tuberculosis | 10.4 million |
| Dengue | 3.2 million |
| Leprosy | 200,000 |
| Ebola | 28,600 |
| Research Focus | ||
|---|---|---|
| Motivation | Outcomes Assessment and Impact Evaluation | Spatial Analysis of the Spread of Malaria |
| Promoting public health from a global perspective | Mitsakakis et al., 2018; Mgone, 2010; Marshall et al., 2010; Atkinson, 2011; Wang et al., 2006; Marshall and De Silva, 2012; Qi, 2012; Tizifa, et al., 2018 | Vajda and Webb, 2017; Hausmann-Muela and Eckl, 2015; Ocampo et al., 2013; Tatem, 2014 |
| The link between climate change and the occurrence of malaria | Semenza, 2015; Ninphanomchai et al., 2014; Reiter, 2008; Klinkenberg et al., 2008; Hay et al., 2002; Adefemi et al., 2015. | Negev et al., 2015; Zhou et al., 2007; Lindblade, 2000; Tonnang, 2010; Edlund et al., 2012 |
| Opportunities for built environment-related mitigation | Walls et al., 2016; Lindsay et al., 2002; Menger et al., 2014; Gamage-Mendis, 1991; Lindsay et al., 2003, Harrysone et al., 2009; Tusting et al., 2015; Tusting et al., 2016; Marshall and De Silva, 2012; Atieli et al., 2009; Njau et al., 2009. | Marshall and De Silva, 2012; Waite, et al., 2016; Tusting et al., 2017 |
| Malaria Source Factors |
|---|
| 1. Antibiotic resistance |
| 2. Artificial breeding sites |
| 3. Building envelope modifications (modifying size/placement of openings) |
| 4. Changes in global wind pattern |
| 5. Deforestation from land use |
| 6. Desertification and drought |
| 7. Higher relative humidity |
| 8. Increased rainfall (precipitation) |
| 9. Increased temperature |
| 10. Inlets/outlets for air transfer and ventilation |
| 11. Insufficient government/NGO funding |
| 12. Lack of health education (e.g., hygiene practices, blood transfusion) |
| 13. Low standard of living (e.g., socioeconomic status) |
| 14. More excavated areas (open surface water bodies) |
| 15. Urban agriculture practices |
| 16. Poor housing material |
| 17. Urban agriculture practices |
| 18. Urbanization |
| Built Environment | Global Health | Climate Change |
|---|---|---|
| 1. Artificial Breeding Sites | 1. Antibiotic resistance | 1. Changes in global wind pattern |
| 2. Building envelope modifications (modifying size/placement of openings) | 2. Geographic residence (e.g., urban, peri-urban, rural, river, coast, altitude) | 2. Deforestation from land use |
| 3. Inlets/outlets for air transfer and ventilation | 3. Insufficient GOV/NGO funding | 3. Desertification and drought |
| 4. More excavated areas causing open surface water bodies | 4. Lack of health education (e.g., hygiene practices, blood transfusion) | 4. Higher relative humidity |
| 5. Poor housing material | 5. Lack of synergy among institutions/organizations | 5. Increased rainfall (precipitation) |
| 6. Urbanization | 6. Urban agriculture practices | 6. Increased temperature |
| 7. Low standard of living (e.g., socioeconomic status) | 7. Pollution (poor indoor air quality) |
| Built Environment Intervention Strategy | Global Health Intervention Strategy | ||
|---|---|---|---|
| 1. Screened eave tubes (SET) | 2. Artemisinin-based combination therapy (ACT) | ||
| Built environment source factors | 1. Artificial breeding sites | The mechanism of a SET requires a wall that separates an interior from an exterior. Although these tubes may not be used for breeding sites, like drains, gutters, swimming pools, or tire tracks [18], placing a treated screen on these types of areas can open new, innovative solutions to preventing malaria in those sites, such as electrostatic coating [53]. | More larvae development results in greater mosquito population density, resulting in uneven distribution of therapy needed and a greater number of individuals at risk for disease. |
| 2. Urbanization | Due to the scalability of eaves tubes, there must be a focus on high-risk groups that serve as priority, before the intervention technologies are scaled to the entire community [53]. | Increased population results in greater demand for this product. | |
| Global health source factors | 1. Low standard of living (e.g., socioeconomic status) | Low socioeconomic status (SES) to the extent of homelessness within poverty may occur in urban regions. Poverty is the greatest risk factor towards malaria. Poverty reduces opportunities to a formal education, which reduces chances to get a good job, recycling into increased poverty [40]. | Because there are problems related to affordability and accessibility of this drug, those of low SES who already suffer the financial burden of disease treatment are further at risk. |
| 2. Geographic residence (e.g., urban) | Malaria is transmitted by different Anopheles species, which can vary by geographic environment. Some vectors are more dominant than others. Therefore, more SETs should be implemented in regions with higher prevalence. | Those in regions where the species of Anopheles is more prevalent will increase the demand, resulting in a greater need for affordable and accessible therapy drugs. | |
| Climate change source factors | 1. Deforestation from land use | Deforestation increases prevalence of the malaria vector. Because buildings are made by initial deforestation, the increase in homes requiring SETs mirrors the increase in the deforestation. | Dispersal of the vector to different geographic regions results in a greater need to outsource the drug to new communities, which causes difficulty for those unable to afford or access the drug. |
| 2. Increased rainfall (precipitation) | Increased prevalence of the Anopheles vector will result, causing greater need for SETs. | More favorable habitat for reproduction allows more generations to develop. This can result in antibiotic resistance. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obonyo, E.; Pareek, S.; Woldu, D.O. Decision Making within the Built Environment as a Strategy for Mitigating the Risk of Malaria and Other Vector-Borne Diseases. Buildings 2019, 9, 2. https://doi.org/10.3390/buildings9010002
Obonyo E, Pareek S, Woldu DO. Decision Making within the Built Environment as a Strategy for Mitigating the Risk of Malaria and Other Vector-Borne Diseases. Buildings. 2019; 9(1):2. https://doi.org/10.3390/buildings9010002
Chicago/Turabian StyleObonyo, Esther, Sumit Pareek, and Dawit Okubatsion Woldu. 2019. "Decision Making within the Built Environment as a Strategy for Mitigating the Risk of Malaria and Other Vector-Borne Diseases" Buildings 9, no. 1: 2. https://doi.org/10.3390/buildings9010002
APA StyleObonyo, E., Pareek, S., & Woldu, D. O. (2019). Decision Making within the Built Environment as a Strategy for Mitigating the Risk of Malaria and Other Vector-Borne Diseases. Buildings, 9(1), 2. https://doi.org/10.3390/buildings9010002