
Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bacteriological Analysis, Patients’ Demographics, and Antimicrobial Susceptibility Testing
2.2. Microbiological Analysis
2.3. Classifications as Multi-, Extremely- and Pan-Drug Resistant Bacteria (MDR, XDR, and PDR)
2.4. Direct Multi-Gene Molecular Detection of S. aureus Lineages by GeneXpert System
2.5. Statistical Analysis
3. Results
3.1. Age-Specific Frequencies of S. aureus Lineages in ICU and Non-ICU
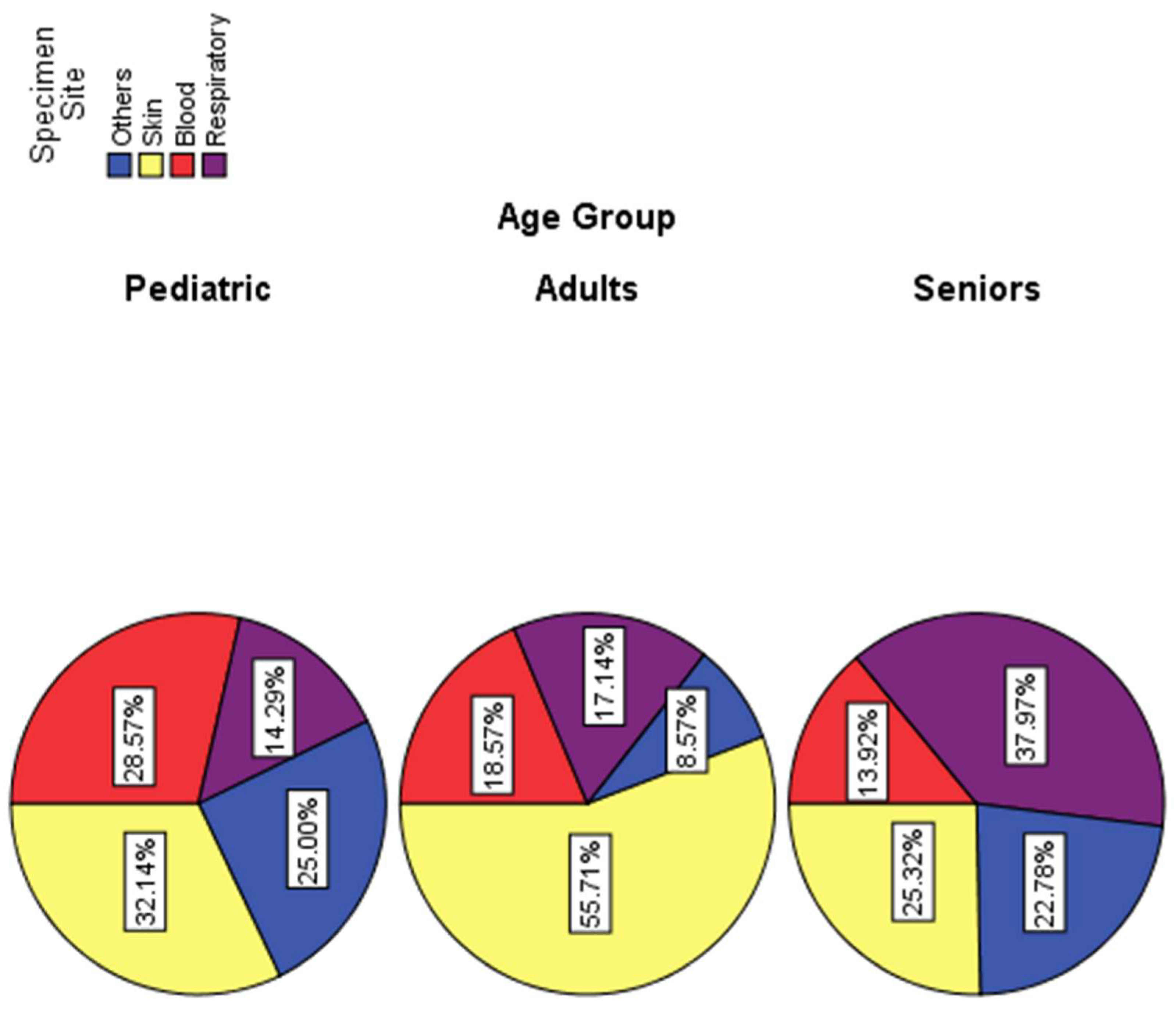
3.2. Organ-Specific Distribution of Clinical S. aureus Infections among Different Age Groups
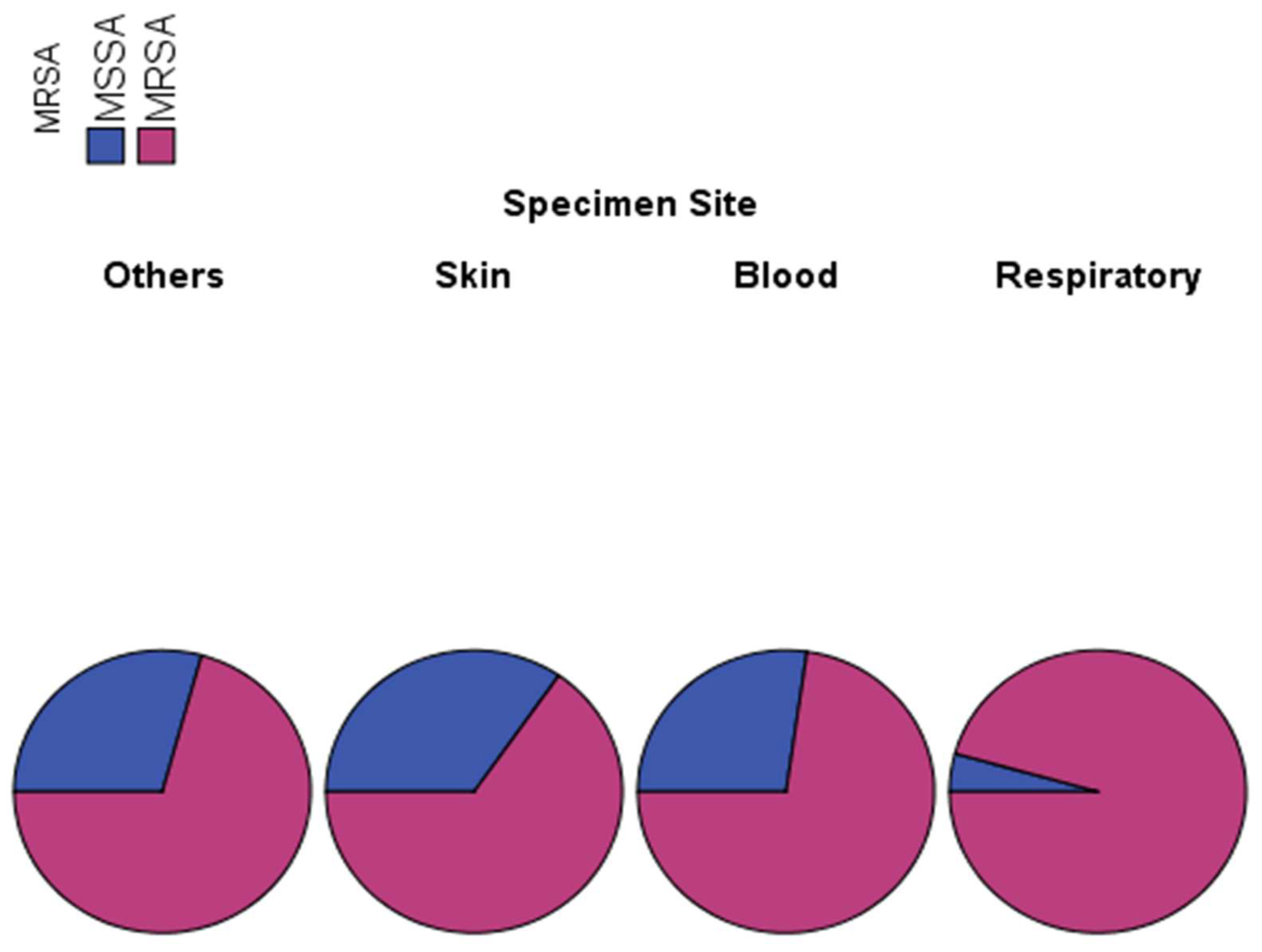
3.3. Association between Site of Infection and S. aureus Lineage
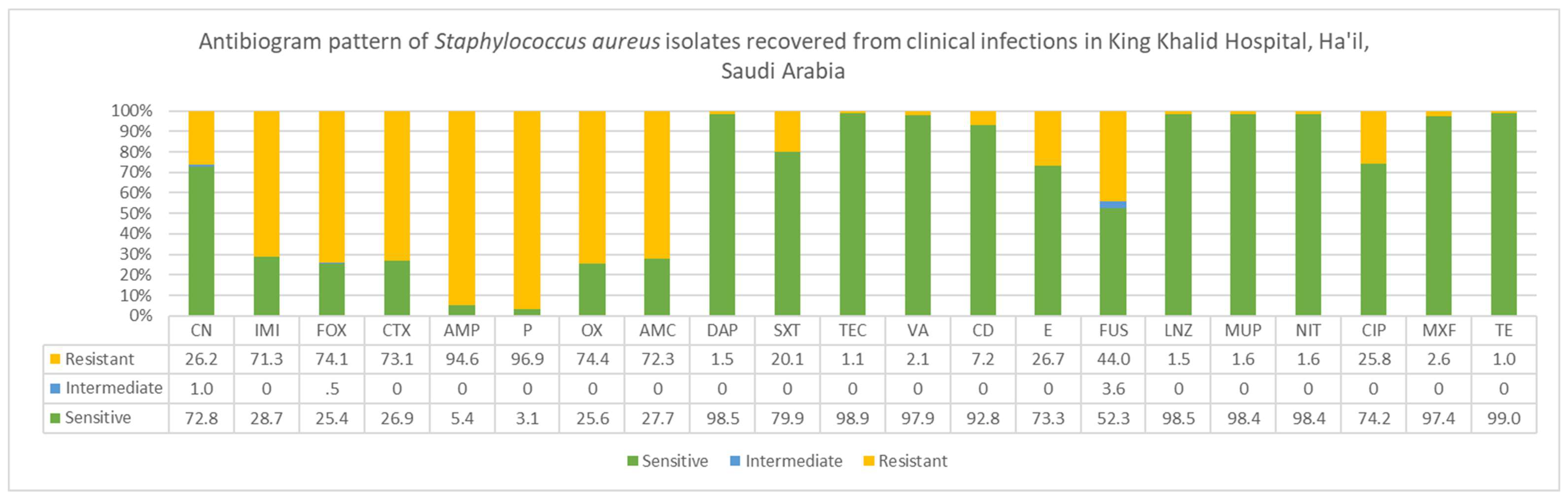
3.4. Molecular Characterization and Antimicrobial Susceptibility Testing (AST) of Clinical S. aureus Lineages
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Sato, E.; Yamamoto, H.; Honda, T.; Koyama, S.; Kubo, K.; Sediguchi, M. Acute Respiratory Distress Syndrome Due to Methicillin-Resistant Staphylococcus Aureus Sepsis in Hyper-IgE Syndrome. Eur. Respir. J. 1996, 9, 386–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardakas, K.Z.; Matthaiou, D.K.; Falagas, M.E. Comparison of Community-Acquired Pneumonia Due to Methicillin-Resistant and Methicillin-Susceptible Staphylococcus Aureus Producing the Panton-Valentine Leukocidin. Int. J. Tuberc. Lung Dis. 2009, 13, 1476–1485. [Google Scholar] [PubMed]
- Boucher, H.W.; Corey, G.R. Epidemiology of Methicillin-Resistant Staphylococcus Aureus. Clin. Infect. Dis. 2008, 46 (Suppl. S5), S344–S349. [Google Scholar] [CrossRef] [Green Version]
- Kuehnert, M.J.; Hill, H.A.; Kupronis, B.A.; Tokars, J.I.; Solomon, S.L.; Jernigan, D.B. Methicillin-Resistant–Staphylococcus Aureus Hospitalizations, United States. Emerg. Infect. Dis. 2005, 11, 868. [Google Scholar] [CrossRef]
- Klevens, R.M.; Morrison, M.A.; Nadle, J.; Petit, S.; Gershman, K.; Ray, S.; Harrison, L.H.; Lynfield, R.; Dumyati, G.; Townes, J.M.; et al. Invasive Methicillin-Resistant Staphylococcus Aureus Infections in the United States. JAMA 2007, 298, 1763–1771. [Google Scholar] [CrossRef] [Green Version]
- Louise Gerberding, J.; Director, M.; Cohen, M.; Ronald Valdiserri, P.O.; Acting Director, M.; Janssen, R.S. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2004-vol-16.pdf (accessed on 1 January 2023).
- FastStats-Viral Hepatitis. Available online: https://www.cdc.gov/nchs/fastats/hepatitis.htm (accessed on 19 March 2022).
- Table 1|Reported TB in the US 2020|Data & Statistics|TB|CDC. Available online: https://www.cdc.gov/tb/statistics/reports/2020/table1.htm (accessed on 19 March 2022).
- Fowler, V.G.; Miro, J.M.; Hoen, B.; Cabell, C.H.; Abrutyn, E.; Rubinstein, E.; Corey, G.R.; Spelman, D.; Bradley, S.F.; Barsic, B.; et al. Staphylococcus Aureus Endocarditis: A Consequence of Medical Progress. JAMA 2005, 293, 3012–3021. [Google Scholar] [CrossRef] [Green Version]
- Bancroft, E.A. Antimicrobial Resistance: It’s Not Just for Hospitals. JAMA 2007, 298, 1803–1804. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Reyes, L.F.; Aliberti, S.; Restrepo, M.I. Empirical Coverage of Methicillin-Resistant Staphylococcus Aureus in Community-Acquired Pneumonia: Those Who Do Not Remember the Past Are Doomed to Repeat It. Clin. Infect. Dis. 2016, 63, 1145–1146. [Google Scholar] [CrossRef] [Green Version]
- Hassoun, A.; Linden, P.K.; Friedman, B. Incidence, Prevalence, and Management of MRSA Bacteremia across Patient Populations-a Review of Recent Developments in MRSA Management and Treatment. Crit. Care 2017, 21, 211. [Google Scholar] [CrossRef]
- Köck, R.; Becker, K.; Cookson, B.; van Gemert-Pijnen, J.E.; Harbarth, S.; Kluytmans, J.; Mielke, M.; Peters, G.; Skov, R.L.; Struelens, M.J.; et al. Methicillin-Resistant Staphylococcus Aureus (MRSA): Burden of Disease and Control Challenges in Europe. Euro. Surveill. 2010, 15, 19688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio. Medica. Atenei. Parm. 2020, 91, 157. [Google Scholar] [CrossRef]
- Güner, R.; Hasanoğlu, İ.; Aktaş, F. COVID-19: Prevention and Control Measures in Community. Turk. J. Med. Sci. 2020, 50, 571. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Upadhyay, P.; Reddy, J.; Granger, J. SARS-CoV-2 Respiratory Co-Infections: Incidence of Viral and Bacterial Co-Pathogens. Int. J. Infect. Dis. 2021, 105, 617. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Ej Golzari, S. Evaluation of Bacterial Co-Infections of the Respiratory Tract in COVID-19 Patients Admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.G.; Smoot, B.E.; Thompson, B.T. Critical Illness from 2009 Pandemic Influenza A (H1N1) Virus and Bacterial Co-Infection in the United States. Crit. Care Med. 2012, 40, 1487. [Google Scholar] [CrossRef] [Green Version]
- Joseph, C.; Togawa, Y.; Shindo, N. Bacterial and Viral Infections Associated with Influenza. Influenza Other Respir Viruses 2013, 7 (Suppl. S2), 105. [Google Scholar] [CrossRef] [Green Version]
- Giancola, S.E.; Nguyen, A.T.; Le, B.; Ahmed, O.; Higgins, C.; Sizemore, J.A.; Orwig, K.W. Clinical Utility of a Nasal Swab Methicillin-Resistant Staphylococcus Aureus Polymerase Chain Reaction Test in Intensive and Intermediate Care Unit Patients with Pneumonia. Diagn. Microbiol. Infect. Dis. 2016, 86, 307–310. [Google Scholar] [CrossRef]
- Smith, M.N.; Erdman, M.J.; Ferreira, J.A.; Aldridge, P.; Jankowski, C.A. Clinical Utility of Methicillin-Resistant Staphylococcus Aureus Nasal Polymerase Chain Reaction Assay in Critically Ill Patients with Nosocomial Pneumonia. J. Crit. Care 2017, 38, 168–171. [Google Scholar] [CrossRef]
- Chan, J.D.; Dellit, T.H.; Choudhuri, J.A.; McNamara, E.; Melius, E.J.; Evans, H.L.; Cuschieri, J.; Arbabi, S.; Lynch, J.B. Active Surveillance Cultures of Methicillin-Resistant Staphylococcus Aureus as a Tool to Predict Methicillin-Resistant S. Aureus Ventilator-Associated Pneumonia. Crit. Care Med. 2012, 40, 1437–1442. [Google Scholar] [CrossRef]
- Langsjoen, J.; Brady, C.; Obenauf, E.; Kellie, S. Nasal Screening Is Useful in Excluding Methicillin-Resistant Staphylococcus Aureus in Ventilator-Associated Pneumonia. Am. J. Infect Control 2014, 42, 1014–1015. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Wunderink, R.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Balk, R.A.; Fakhran, S.S.; Chappell, J.D.; Casimir, G.; Courtney, D.M.; et al. Staphylococcus Aureus Community-Acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clin. Infect Dis. 2016, 63, 300–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyrani, P.; Mandell, L.; Torres, A.; Tillotson, G.S. The Burden of Community-Acquired Bacterial Pneumonia in the Era of Antibiotic Resistance. Expert. Rev. Respir. Med. 2019, 13, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Letsiou, E.; Wang, H.; Belvitch, P.; Meliton, L.N.; Brown, M.E.; Bandela, M.; Chen, J.; Garcia, J.G.N.; Dudek, S.M. MRSA-Induced Endothelial Permeability and Acute Lung Injury Are Attenuated by FTY720 S-Phosphonate. Am. J. Physiol. Lung Cell Mol. Physiol. 2022, 322, L149–L161. [Google Scholar] [CrossRef]
- Dugani, S.; Veillard, J.; Kissoon, N. Reducing the Global Burden of Sepsis. CMAJ 2017, 189, E2–E3. [Google Scholar] [CrossRef] [Green Version]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Abbasoglu Ozgoren, A.; Abdalla, S.; Abd-Allah, F.; et al. Global, Regional, and National Age-Sex Specific All-Cause and Cause-Specific Mortality for 240 Causes of Death, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, J.M.; Johnson, M.H.; Kagan, S.A.; Baer, S.L. Clinical and Economic Burden of Community-Acquired Pneumonia in the Veterans Health Administration, 2011: A Retrospective Cohort Study. Infection 2015, 43, 671–680. [Google Scholar] [CrossRef] [Green Version]
- Fernando, S.M.; Rochwerg, B.; Seely, A.J.E. Clinical Implications of the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). CMAJ 2018, 190, E1058–E1059. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Qian, Y.; Miao, Z.; Zheng, P.; Shi, T.; Jiang, X.; Pan, L.; Qian, F.; Yang, G.; An, H.; et al. Xuebijing Injection Alleviates Pam3CSK4-Induced Inflammatory Response and Protects Mice From Sepsis Caused by Methicillin-Resistant Staphylococcus Aureus. Front. Pharmacol. 2020, 11, 104. [Google Scholar] [CrossRef]
- Kourtis, A.P.; Hatfield, K.; Baggs, J.; Mu, Y.; See, I.; Epson, E.; Nadle, J.; Kainer, M.A.; Dumyati, G.; Petit, S.; et al. Vital Signs: Epidemiology and Recent Trends in Methicillin-Resistant and in Methicillin-Susceptible Staphylococcus Aureus Bloodstream Infections - United States. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Doudoulakakis, A.G.; Bouras, D.; Drougka, E.; Kazantzi, M.; Michos, A.; Charisiadou, A.; Spiliopoulou, I.; Lebessi, E.; Tsolia, M. Community-Associated Staphylococcus Aureus Pneumonia among Greek Children: Epidemiology, Molecular Characteristics, Treatment, and Outcome. Eur. J. Clin. Microbiol. Infect Dis. 2016, 35, 1177–1185. [Google Scholar] [CrossRef]
- Ghahremani, M.; Jazani, N.H.; Sharifi, Y. Emergence of Vancomycin-Intermediate and -Resistant Staphylococcus Aureus among Methicillin-Resistant S. Aureus Isolated from Clinical Specimens in the Northwest of Iran. J. Glob. Antimicrob. Resist. 2018, 14, 4–9. [Google Scholar] [CrossRef]
- Boswihi, S.S.; Udo, E.E.; Monecke, S.; Mathew, B.; Noronha, B.; Verghese, T.; Tappa, S.B. Emerging Variants of Methicillin-Resistant Staphylococcus Aureus Genotypes in Kuwait Hospitals. PLoS ONE 2018, 13, e0195933. [Google Scholar] [CrossRef] [Green Version]
- Senok, A.; Ehricht, R.; Monecke, S.; Al-Saedan, R.; Somily, A. Molecular Characterization of Methicillin-Resistant Staphylococcus Aureus in Nosocomial Infections in a Tertiary-Care Facility: Emergence of New Clonal Complexes in Saudi Arabia. New Microbes New Infect. 2016, 14, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Senok, A.; Somily, A.M.; Nassar, R.; Garaween, G.; Sing, G.K.; Müller, E.; Reissig, A.; Gawlik, D.; Ehricht, R.; Monecke, S. Emergence of Novel Methicillin-Resistant Staphylococcus Aureus Strains in a Tertiary Care Facility in Riyadh, Saudi Arabia. Infect. Drug Resist. 2019, 12, 2739–2746. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Chen, C.J.; Su, L.H.; Hu, S.; Yu, J.; Chiu, C.H. Evolution and Pathogenesis of Staphylococcus Aureus: Lessons Learned from Genotyping and Comparative Genomics. FEMS Microbiol. Rev. 2008, 32, 23–37. [Google Scholar] [CrossRef] [Green Version]
- van Leeuwen, W.B.; Melles, D.C.; Alaidan, A.; Al-Ahdal, M.; Ne, H.; Boelens, A.M.; Snijders, S.V.; Wertheim, H.; van Duijkeren, E.; Peeters, J.K.; et al. Host-and Tissue-Specific Pathogenic Traits of Staphylococcus Aureus. J. Bacteriol. 2005, 187, 4584–4591. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, G.; Francioli, P.; Blanc, D.S. Evidence for Clonal Evolution among Highly Polymorphic Genes in Methicillin-Resistant Staphylococcus Aureus. J. Bacteriol. 2006, 188, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Feil, E.J.; Cooper, J.E.; Grundmann, H.; Robinson, D.A.; Enright, M.C.; Berendt, T.; Peacock, S.J.; Smith, J.M.; Murphy, M.; Spratt, B.G.; et al. How Clonal Is Staphylococcus Aureus? J. Bacteriol. 2003, 185, 3307–3316. [Google Scholar] [CrossRef]
- Said, K.B.; Al-Jarbou, A.N.; Alrouji, M.; Al-Harbi, H.O. Surveillance of Antimicrobial Resistance among Clinical Isolates Recovered from a Tertiary Care Hospital in Al Qassim, Saudi Arabia. Int. J. Health Sci. 2014, 8, 3. [Google Scholar] [CrossRef]
- Said, K.B.; Zhu, G.; Zhao, X. Organ- and Host-Specific Clonal Groups of Staphylococcus Aureus from Human Infections and Bovine Mastitis Revealed by the Clumping Factor A Gene. Foodborne Pathog. Dis. 2010, 7, 111–119. [Google Scholar] [CrossRef]
- Said, K.B.; Ramotar, K.; Zhu, G.; Zhao, X. Repeat-Based Subtyping and Grouping of Staphylococcus Aureus from Human Infections and Bovine Mastitis Using the R-Domain of the Clumping Factor A Gene. Diagn. Microbiol. Infect. Dis. 2009, 63, 24–37. [Google Scholar] [CrossRef]
- Tabaja, H.; Hindy, J.R.; Kanj, S.S. Epidemiology of Methicillin-Resistant Staphylococcus Aureus in Arab Countries of the Middle East and North African (MENA) Region. Mediterr. J. Hematol. Infect. Dis. 2021, 13, 2021050. [Google Scholar] [CrossRef]
- Global Laboratory Standards for a Healthier World. 26th Edition. CLSI Document MS100. Available online: www.clsi.org/ (accessed on 22 December 2022).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Manzur, A.; Gavalda, L.; Ruiz De Gopegui, E.; Mariscal, D.; Dominguez, M.A.; Perez, J.L.; Segura, F.; Pujol, M. Prevalence of Methicillin-Resistant Staphylococcus Aureus and Factors Associated with Colonization among Residents in Community Long-Term-Care Facilities in Spain. Clin. Microbiol. Infect. 2008, 14, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Stone, N.D.; Lewis, D.R.; Johnson, T.M.; Hartney, T.; Chandler, D.; Byrd-Sellers, J.; McGowan, J.E.; Tenover, F.C.; Jernigan, J.A.; Gaynes, R.P. Methicillin-Resistant Staphylococcus Aureus (MRSA) Nasal Carriage in Residents of Veterans Affairs Long-Term Care Facilities: Role of Antimicrobial Exposure and MRSA Acquisition. Infect. Control Hosp. Epidemiol. 2012, 33, 551–557. [Google Scholar] [CrossRef]
- Sasahara, T.; Ae, R.; Yoshimura, A.; Kosami, K.; Sasaki, K.; Kimura, Y.; Akine, D.; Ogawa, M.; Hamabata, K.; Hatakeyama, S.; et al. Association between Length of Residence and Prevalence of MRSA Colonization among Residents in Geriatric Long-Term Care Facilities. BMC Geriatr. 2020, 20, 481. [Google Scholar] [CrossRef]
- Rodríguez-Villodres, Á.; Martín-Gandul, C.; Peñalva, G.; Guisado-Gil, A.B.; Crespo-Rivas, J.C.; Pachón-Ibáñez, M.E.; Lepe, J.A.; Cisneros, J.M. Prevalence and Risk Factors for Multidrug-Resistant Organisms Colonization in Long-Term Care Facilities around the World: A Review. Antibiotics 2021, 10, 680. [Google Scholar] [CrossRef]
- Lee, Y.J.; Chen, J.Z.; Lin, H.C.; Liu, H.Y.; Lin, S.Y.; Lin, H.H.; Fang, C.T.; Hsueh, P.R. Impact of Active Screening for Methicillin-Resistant Staphylococcus Aureus (MRSA) and Decolonization on MRSA Infections, Mortality and Medical Cost: A Quasi-Experimental Study in Surgical Intensive Care Unit. Crit. Care 2015, 19, 143. [Google Scholar] [CrossRef]
- Edgeworth, J.D.; Batra, R.; Wulff, J.; Harrison, D. Reductions in Methicillin-Resistant Staphylococcus Aureus, Clostridium Difficile Infection and Intensive Care Unit–Acquired Bloodstream Infection Across the United Kingdom Following Implementation of a National Infection Control Campaign. Clin. Infect. Dis. 2020, 70, 2530. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.Y.; Hayden, M.K.; Lyles, R.D.; Lolans, K.; Fogg, L.F.; Kallen, A.J.; Weber, S.G.; Weinstein, R.A.; Trick, W.E. Regional Epidemiology of Methicillin-Resistant Staphylococcus Aureus Among Adult Intensive Care Unit Patients Following State-Mandated Active Surveillance. Clin. Infect. Dis. 2018, 66, 1535. [Google Scholar] [CrossRef] [PubMed]
- Qiao, F.; Huang, W.; Cai, L.; Zong, Z.; Yin, W. Methicillin-Resistant Staphylococcus Aureus Nasal and Infection in an Intensive Care Unit of a University Hospital In. J. Int. Med. Res. 2018, 46, 3698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, Y.K.; Lee, M.J.; Ju, Y.; Lee, S.E.; Yang, K.S.; Sohn, J.W.; Kim, M.J. Determining the Clinical Significance of Co-Colonization of Vancomycin-Resistant Enterococci and Methicillin-Resistant Staphylococcus Aureus in the Intestinal Tracts of Patients in Intensive Care Units: A Case–Control Study. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, Y.; Hegde, A.; Pande, R.; Zirpe, K.G.; Gupta, V.; Ahdal, J.; Qamra, A.; Motlekar, S.; Jain, R. Methicillin-Resistant Staphylococcus Aureus in Intensive Care Unit Setting of India: A Review of Clinical Burden, Patterns of Prevalence, Preventive Measures, and Future Strategies. Indian J. Crit. Care Med. 2020, 24, 55. [Google Scholar] [CrossRef]
- Ali, M.A.; Rajab, A.M.; Al-Khani, A.M.; Ayash, S.Q.; Chamsi Basha, A.; Abdelgadir, A.; Rajab, T.M.; Enabi, S.; Saquib, N. Methicillin-Resistant Staphylococcus Aureus Development in Intensive Care Patients A Case-Control Study OPEN ACCESS. Saudi Med. J. 2020, 41, 1181–1186. [Google Scholar] [CrossRef]
- Angvik, M.; Olsen, R.S.; Olsen, K.; Simonsen, G.S.; Furberg, A.-S.; Ericson Sollid, J.U. Age-and Gender-Associated Staphylococcus Aureus Spa Types Found among Nasal Carriers in a General Population: The Tromsø Staph and Skin Study. J. Clin. Microbiol. 2011, 49, 4213–4218. [Google Scholar] [CrossRef] [Green Version]
- Bayles, K.W.; Wesson, C.A.; Liou, L.E.; Fox, L.K.; Bohach, G.A.; Trumble, A.W.R. Intracellular Staphylococcus Aureus Escapes the Endosome and Induces Apoptosis in Epithelial Cells. Infect. Immun. 1998, 66, 336–342. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Staphylococcus aureus Isolates | Age Groups | ||||
|---|---|---|---|---|---|
| <20 | 20–50 | >50 | |||
| MSSA | Setting | ICU | 5 | 2 | 9 |
| Non-ICU | 5 | 10 | 25 | ||
| Total | 10 | 12 | 34 | ||
| MRSA | Setting | ICU | 6 | 8 | 34 |
| Non-ICU | 12 | 43 | 99 | ||
| Total | 18 | 51 | 133 | ||
| Total | Setting | ICU | 11 | 10 | 43 |
| Non-ICU | 17 | 53 | 124 | ||
| Total | 28 | 63 | 167 | ||
| SPECIMEN SITE | Total | ||||||
|---|---|---|---|---|---|---|---|
| Others | Skin | Blood | Respiratory | ||||
| Age | <20 | Count | 7 | 9 | 8 | 4 | 28 |
| Percentage | 25.0% | 32.1% | 28.6% | 14.3% | 100.0% | ||
| 20–50 | Count | 6 | 39 | 13 | 12 | 70 | |
| Percentage | 8.6% | 55.7% | 18.6% | 17.1% | 100.0% | ||
| >50 | Count | 18 | 20 | 11 | 30 | 79 | |
| Percentage | 22.8% | 25.3% | 13.9% | 38.0% | 100.0% | ||
| Total | Count | 31 | 68 | 32 | 46 | 177 | |
| Percentage | 17.5% | 38.4% | 18.1% | 26.0% | 100.0% | ||
| Value | df | Asymptotic Significance (2-sided) | |||||
| Pearson Chi-Square | 25.032 | 6 | 0.000 | ||||
| Likelihood Ratio | 25.237 | 6 | 0.000 | ||||
| Linear-by-Linear Association | 2.848 | 1 | 0.051 | ||||
| N of Valid Cases | 177 | ||||||
| Specimen Site by | Staphylococcus aureus Isolates | Total | |||
|---|---|---|---|---|---|
| MSSA | MRSA | ||||
| Specimen Site | Others | Count | 12 | 29 | 41 |
| Percentage | 29.3% | 70.7% | 100.0% | ||
| Skin | Count | 26 | 49 | 75 | |
| Percentage | 34.7% | 65.3% | 100.0% | ||
| Blood | Count | 9 | 24 | 33 | |
| Percentage | 27.3% | 72.7% | 100.0% | ||
| Respiratory | Count | 2 | 44 | 46 | |
| Percentage | 4.3% | 95.7% | 100.0% | ||
| Total | Count | 49 | 146 | 195 | |
| Percentage | 25.1% | 74.9% | 100.0% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, K.B.; Alghasab, N.S.; Alharbi, M.S.M.; Alsolami, A.; Saleem, M.; Alhallabi, S.A.; Alafnan, S.F.; Khaja, A.S.S.; Taha, T.E.; on behalf of the Ha’il COM Research Unit Group. Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics. Microorganisms 2023, 11, 149. https://doi.org/10.3390/microorganisms11010149
Said KB, Alghasab NS, Alharbi MSM, Alsolami A, Saleem M, Alhallabi SA, Alafnan SF, Khaja ASS, Taha TE, on behalf of the Ha’il COM Research Unit Group. Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics. Microorganisms. 2023; 11(1):149. https://doi.org/10.3390/microorganisms11010149
Chicago/Turabian StyleSaid, Kamaleldin B., Naif Saad Alghasab, Mohammed S. M. Alharbi, Ahmed Alsolami, Mohd Saleem, Sulaf A. Alhallabi, Shahad F. Alafnan, Azharuddin Sajid Syed Khaja, Taha E. Taha, and on behalf of the Ha’il COM Research Unit Group. 2023. "Molecular and Source-Specific Profiling of Hospital Staphylococcus aureus Reveal Dominance of Skin Infection and Age-Specific Selections in Pediatrics and Geriatrics" Microorganisms 11, no. 1: 149. https://doi.org/10.3390/microorganisms11010149