

Systemic Inflammatory Molecules Are Associated with Advanced Fibrosis in Patients from Brazil Infected with Hepatitis Delta Virus Genotype 3 (HDV-3)
 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Cohort
2.2. Samples and Laboratory Assays
2.3. Viral Quantification and Genotyping
2.4. Soluble Inflammatory Mediators (SIMs) Measurements
2.5. Statistical Analyses
3. Results
3.1. Clinical Characteristics of Study Subjects
3.2. Soluble Inflammatory Mediators in Non-Cirrhotic vs. Cirrhotic Patients
3.3. Clinical Markers of Fibrosis in HDV-Infected Patients
3.4. ROC Curve SIMs Considerations
4. Discussion
4.1. SIMs Associated Fibrosis
4.2. Established Fibrosis Scores
4.3. Alternative Fibrosis Scores Based on SIMs
4.4. Influencing Factors—DNA HBV and RNA HDV
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Braga, W.S.; Castilho, M.d.C.; Borges, F.G.; Leão, J.R.; Martinho, A.C.; Rodrigues, I.S.; Azevedo, E.P.; Barros Júnior, G.M.; Paraná, R. Hepatitis D virus infection in the Western Brazilian Amazon—Far from a vanishing disease. Rev. Soc. Bras. Med. Trop. 2012, 45, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Wedemeyer, H.; Manns, M.P. Epidemiology, pathogenesis and management of hepatitis D: Update and challenges ahead. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Lunemann, S.; Malone, D.F.; Grabowski, J.; Port, K.; Béziat, V.; Bremer, B.; Malmberg, K.J.; Manns, M.P.; Sandberg, J.K.; Cornberg, M.; et al. Effects of HDV infection and pegylated interferon α treatment on the natural killer cell compartment in chronically infected individuals. Gut 2015, 64, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Wranke, A.; Pinheiro Borzacov, L.M.; Parana, R.; Lobato, C.; Hamid, S.; Ceausu, E.; Dalekos, G.N.; Rizzetto, M.; Turcanu, A.; Niro, G.A.; et al. Hepatitis Delta International Network. Clinical and virological heterogeneity of hepatitis delta in different regions world-wide: The Hepatitis Delta International Network (HDIN). Liver Int. 2018, 38, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Dény, P. Hepatitis delta virus genetic variability: From genotypes I, II, III to eight major clades? Curr. Top. Microbiol. Immunol. 2006, 307, 151–171. [Google Scholar] [CrossRef]
- Gomes-Gouvêa, M.S.; Soares, M.C.P.; Bensabath, G.; de Carvalho-Mello, I.M.V.G.; Brito, E.M.F.; Souza, O.S.C.; Queiroz, A.T.L.; Carrilho, F.J.; Pinho, J.R.R. Hepatitis B virus and hepatitis delta virus genotypes in outbreaks of fulminant hepatitis (Labrea black fever) in the western Brazilian Amazon region. J. Gen. Virol. 2009, 90 Pt 11, 2638–2643. [Google Scholar] [CrossRef]
- Kay, A.; Melo da Silva, E.; Pedreira, H.; Negreiros, S.; Lobato, C.; Braga, W.; Muwonge, R.; Dény, P.; Reis, M.; Zoulim, F.; et al. HBV/HDV co-infection in the Western Brazilian Amazonia: An intriguing mutation among HDV genotype 3 carriers. J. Viral Hepat. 2014, 21, 921–924. [Google Scholar] [CrossRef]
- Paraná, R.; Kay, A.; Molinet, F.; Viana, S.; Silva, L.K.; Salcedo, J.M.; Tavares-Neto, J.; Lobato, C.; Rios-Leite, M.; Matteoni, L.; et al. HDV genotypes in the Western Brazilian Amazon region: A preliminary report. Am. J. Trop. Med. Hyg. 2006, 75, 475–479. [Google Scholar] [CrossRef]
- Grabowski, J.; Yurdaydìn, C.; Zachou, K.; Buggisch, P.; Hofmann, W.P.; Jaroszewicz, J.; Schlaphoff, V.; Manns, M.P.; Cornberg, M.; Wedemeyer, H.; et al. Hepatitis D virus-specific cytokine responses in patients with chronic hepatitis delta before and during interferon alfa-treatment. Liver Int. 2011, 31, 1395–1405. [Google Scholar] [CrossRef]
- Schirdewahn, T.; Grabowski, J.; Owusu Sekyere, S.; Bremer, B.; Wranke, A.; Lunemann, S.; Schlaphoff, V.; Kirschner, J.; Hardtke, S.; Manns, M.P.; et al. The Third Signal Cytokine Interleukin 12 Rather Than Immune Checkpoint Inhibitors Contributes to the Functional Restoration of Hepatitis D Virus-Specific T Cells. J. Infect. Dis. 2017, 215, 139–149. [Google Scholar] [CrossRef]
- Borzacov, L.M.; de Figueiredo Nicolete, L.D.; Souza, L.F.; Dos Santos, A.O.; Vieira, D.S.; Salcedo, J.M. Treatment of hepatitis delta virus genotype 3 infection with peg-interferon and entecavir. Int. J. Infect. Dis. 2016, 46, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Lutterkort, G.L.; Wranke, A.; Yurdaydin, C.; Budde, E.; Westphal, M.; Lichtinghagen, R.; Stift, J.; Bremer, B.; Hardtke, S.; Keskin, O.; et al. Non-invasive fibrosis score for hepatitis delta. Liver Int. 2017, 37, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Takyar, V.; Etzion, O.; Heller, T.; Kleiner, D.E.; Rotman, Y.; Ghany, M.G.; Fryzek, N.; Williams, V.H.; Rivera, E.; Auh, S.; et al. Complications of percutaneous liver biopsy with Klatskin needles: A 36-year single-centre experience. Aliment. Pharmacol. Ther. 2017, 45, 744–753. [Google Scholar] [CrossRef]
- Casey, J.L.; Niro, G.A.; Engle, R.E.; Vega, A.; Gomez, H.; McCarthy, M.; Watts, D.M.; Hyams, K.C.; Gerin, J.L. Hepatitis B virus (HBV)/hepatitis D virus (HDV) coinfection in outbreaks of acute hepatitis in the Peruvian Amazon basin: The roles of HDV genotype III and HBV genotype F. J. Infect. Dis. 1996, 174, 920–926. [Google Scholar] [CrossRef]
- Lareyre, F.; Moratal, C.; Chikande, J.; Jean-Baptiste, E.; Hassen-Khodja, R.; Neels, J.; Chinetti, G.; Raffort, J. Investigation of Plasma Inflammatory Profile in Diabetic Patients with Abdominal Aortic Aneurysm: A Pilot Study. Vasc. Endovascular. Surg. 2018, 52, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Viana, S.; Paraná, R.; Moreira, R.C.; Compri, A.P.; Macedo, V. High prevalence of hepatitis B virus and hepatitis D virus in the western Brazilian Amazon. Am. J. Trop. Med. Hyg. 2005, 73, 808–814. [Google Scholar] [CrossRef]
- Rizzetto, M.; Ciancio, A. Epidemiology of hepatitis D. Semin. Liver Dis. 2012, 32, 211–219. [Google Scholar] [CrossRef]
- Mendes-Correa, M.C.; Gomes-Gouvêa, M.S.; Alvarado-Mora, M.V.; Da Silva, M.H.; Lázari, C.; Cavalcanti, N.C.; Alonso, F.K.; Carpinelli, C.C.; Uip, D.E.; Pinho, J.R. Hepatitis delta in HIV/HBV co-infected patients in Brazil: Is it important? Int. J. Infect. Dis. 2011, 15, e828–e832. [Google Scholar] [CrossRef]
- Yurdaydin, C.; Bozkaya, H.; Karaaslan, H.; Onder, F.O.; Erkan, O.E.; Yalçin, K.; Değertekin, H.; Bozdayi, A.M.; Uzunalimoğlu, O. A pilot study of 2 years of interferon treatment in patients with chronic delta hepatitis. J. Viral. Hepat. 2007, 14, 812–816. [Google Scholar] [CrossRef]
- Braga, W.S.M.; Brasil, L.M.; de Souza, R.A.B.; da Costa Castilho, M.; da Fonseca, J.C. Ocorrência da infecçãopelovírus da hepatite B (VHB) e delta (VHD) emsetegruposindígenas do Estado do Amazonas. Rev. Soc. Bras. Med. Trop. 2001, 34, 349–355. [Google Scholar] [CrossRef]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. Elife 2014, 3, e00049, Erratum in Elife 2014, 3, e05570. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Lai, M.M. Hepatitis delta virus RNA replication. Viruses 2009, 1, 818–831. [Google Scholar] [CrossRef]
- Kiesslich, D.; Crispim, M.A.; Santos, C.; Ferreira Fde, L.; Fraiji, N.A.; Komninakis, S.V.; Diaz, R.S. Influence of hepatitis B virus (HBV) genotype on the clinical course of disease in patients coinfected with HBV and hepatitis delta virus. J. Infect. Dis. 2009, 199, 1608–1611. [Google Scholar] [CrossRef] [PubMed]
- Kalayci, O.; Sonna, L.A.; Woodruff, P.G.; Camargo CAJr Luster, A.D.; Lilly, C.M. Monocyte chemotactic protein-4 (MCP-4; CCL-13): A biomarker of asthma. J. Asthma. 2004, 41, 27–33. [Google Scholar] [CrossRef]
- Scandella, E.; Men, Y.; Legler, D.F.; Gillessen, S.; Prikler, L.; Ludewig, B.; Groettrup, M. CCL19/CCL21-triggered signal transduction and migration of dendritic cells requires prostaglandin E2. Blood 2004, 103, 1595–1601. [Google Scholar] [CrossRef]
- Hasegawa, T.; Kosaki, A.; Kimura, T.; Matsubara, H.; Mori, Y.; Okigaki, M.; Masaki, H.; Toyoda, N.; Inoue-Shibata, M.; Kimura, Y.; et al. The regulation of EN-RAGE (S100A12) gene expression in human THP-1 macrophages. Atherosclerosis 2003, 171, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, A.; Sturm, G.J.; Ofner, M.; Sturm, E.M.; Weller, C.; Peskar, B.A.; Hartnell, A. Stem cell factor stimulates the chemotaxis, integrin upregulation, and survival of human basophils. J. Allergy Clin. Immunol. 2005, 116, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Chakraborti, A.; Das, A.; Dhiman, R.K.; Chawla, Y. Elevation of interleukin-18 in chronic hepatitis C: Implications for hepatitis C virus pathogenesis. Immunology 2009, 128 (Suppl. 1), e514–e522. [Google Scholar] [CrossRef] [PubMed]
- Wedemeyer, H.; Yurdaydìn, C.; Dalekos, G.N.; Erhardt, A.; Çakaloğlu, Y.; Değertekin, H.; Gürel, S.; Zeuzem, S.; Zachou, K.; Bozkaya, H.; et al. HIDIT Study Group. Peginterferon plus adefovir versus either drug alone for hepatitis delta. N. Engl. J. Med. 2011, 364, 322–331. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 61) | Non-Cirrhotic (n = 44) | Advanced Fibrosis (n = 17) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Female | 22 (36.1%) | 17 (38.6%) | 5 (29.4%) | |
| Male | 39 (63.9%) | 27 (61.4%) | 12 (70.6%) | |
| Age Median=(interval=) | 41 (18–59) | 39 (18–57) | 44 (18–59) | 0.1056 |
| Use of alcohol | ||||
| No | 45 (73.8%) | 32 (72.7%) | 13 (76.5%) | |
| Yes | 16 (26.2%) | 12 (27.3%) | 4 (23.5%) | |
| ALT Level (U/L) Median=(interval=) | 19.0 (11.0–29.0) | 17.0 (10.0–26.2) | 28.0 (17.0–36.0) | 0.024 |
| AST Level (U/L) Median=(interval=) | 20.0 (12.0–26.0) | 17.0 (10.8–23.0) | 28.0 (13.0–32.0) | 0.020 |
| GGT Level (U/L) Median=(interval=) | 21.0 (13.0–31.0) | 20.5 (14.8–30.0) | 26.0 (9.0–35.0) | 0.929 |
| TB* (mmol/L) Median=(interval=) | 13.0 (10.0–21.0) | 13.0 (10.5–19.0) | 21.0 (10.0–24.0) | 0.083 |
| AFP** (ng/mL) Median=(interval=) | 25.0 (13.0–39.0) | 30.5 (16.8–39.2) | 21.0 (5.0–25.0) | 0.012 |
| Platelets (109/L) Median=(interval=) | 21.0 (9.0–34.0) | 22.5 (9.8–34.2) | 18.0 (9.0–34.0) | 0.778 |
| ALB Median=(interval=) | 17.0 (10.0–23.0) | 17.0 (12.8–24.2) | 11.0 (8.0–18.0) | 0.085 |
| PT Median=(interval=) | 12.0 (8.0–20.0) | 14.0 (8.0–20.5) | 9.0 (7.0–16.0) | 0.143 |
| HBV DNA Median=(interval=) | 348,786.257 (0.0–18,700,000) | 101,425.0 (0.0–2,295,572) | 113 (0.0–745) | 0.3468 |
| SIMs | Total (n = 61) | Non-Cirrhotic (n = 44) | Advanced Fibrosis (n = 17) | p-Value |
|---|---|---|---|---|
| SCF | 9.4 (8.8–9.8) | 9.6 (9.1–9.9) | 8.4 (8.0–9.5) | 0.01 |
| EN.RAGE | 5.5 (4.2–5.9) | 5.8 (5.2–5.9) | 4.8 (4.2–5.1) | 0.014 |
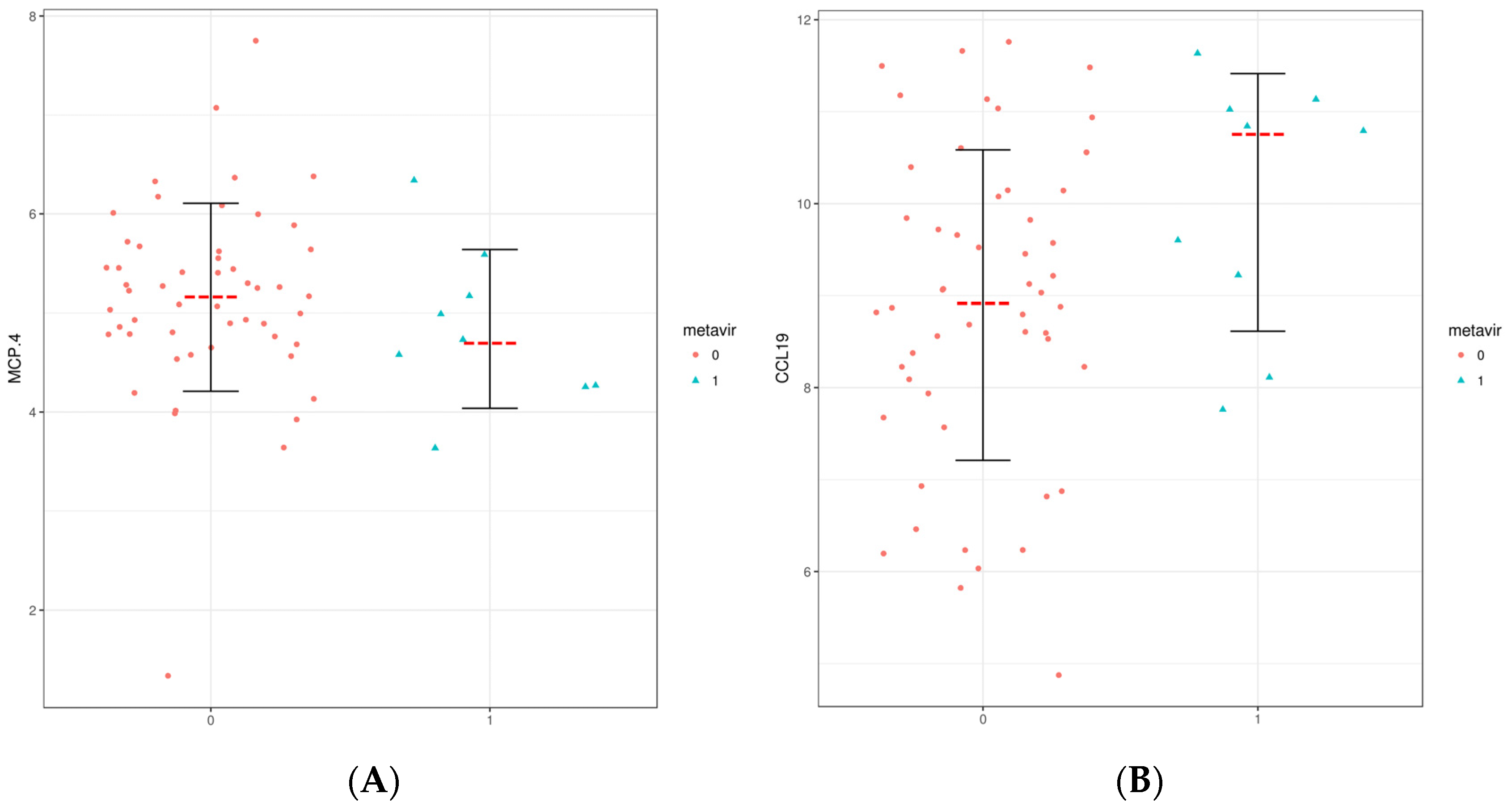
| CCL19 | 9.1 (8.1–10.4) | 8.8 (7.9–9.8) | 10.1 (9.0–11.0) | 0.024 |
| MCP.4 | 5.1 (4.7–5.6) | 5.3 (4.8–5.7) | 4.7 (4.3–5.2) | 0.032 |
| IL18 | 8.5 (8.0–9.0) | 8.4 (7.9–8.9) | 8.8 (8.5–9.3) | 0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza Campos, M.; Villalobos-Salcedo, J.M.; Vieira Dallacqua, D.S.; Lopes Borges Andrade, C.; Meyer Nascimento, R.J.; Menezes Freire, S.; Paraná, R.; Schinoni, M.I. Systemic Inflammatory Molecules Are Associated with Advanced Fibrosis in Patients from Brazil Infected with Hepatitis Delta Virus Genotype 3 (HDV-3). Microorganisms 2023, 11, 1270. https://doi.org/10.3390/microorganisms11051270
Souza Campos M, Villalobos-Salcedo JM, Vieira Dallacqua DS, Lopes Borges Andrade C, Meyer Nascimento RJ, Menezes Freire S, Paraná R, Schinoni MI. Systemic Inflammatory Molecules Are Associated with Advanced Fibrosis in Patients from Brazil Infected with Hepatitis Delta Virus Genotype 3 (HDV-3). Microorganisms. 2023; 11(5):1270. https://doi.org/10.3390/microorganisms11051270
Chicago/Turabian StyleSouza Campos, Mauricio, Juan Miguel Villalobos-Salcedo, Deusilene Souza Vieira Dallacqua, Caio Lopes Borges Andrade, Roberto José Meyer Nascimento, Songeli Menezes Freire, Raymundo Paraná, and Maria Isabel Schinoni. 2023. "Systemic Inflammatory Molecules Are Associated with Advanced Fibrosis in Patients from Brazil Infected with Hepatitis Delta Virus Genotype 3 (HDV-3)" Microorganisms 11, no. 5: 1270. https://doi.org/10.3390/microorganisms11051270