Acupuncture Points of the Horse’s Distal Thoracic Limb: A Neuroanatomic Approach to the Transposition of Traditional Points

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
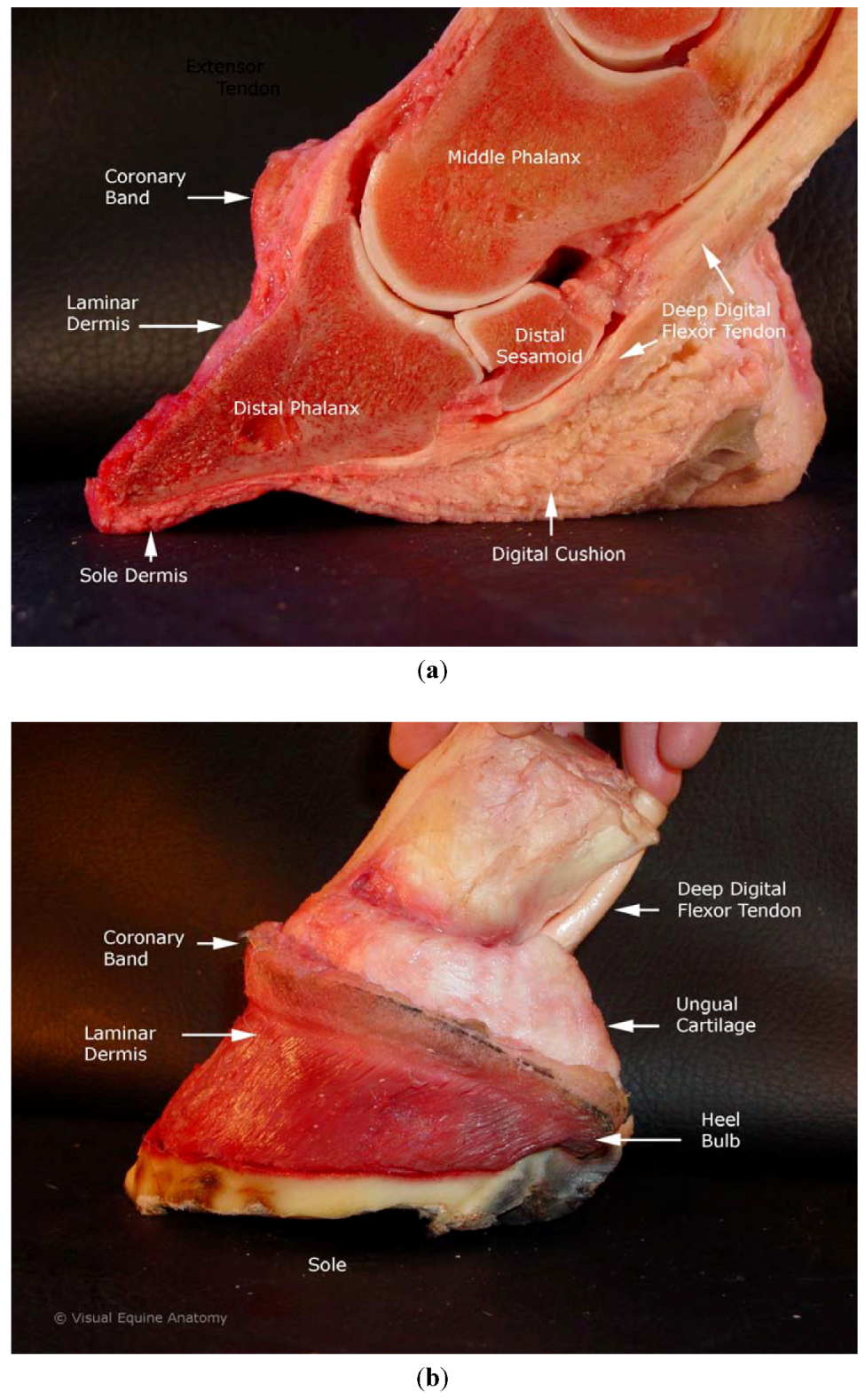
2. Equine Foot Anatomy and Physiology

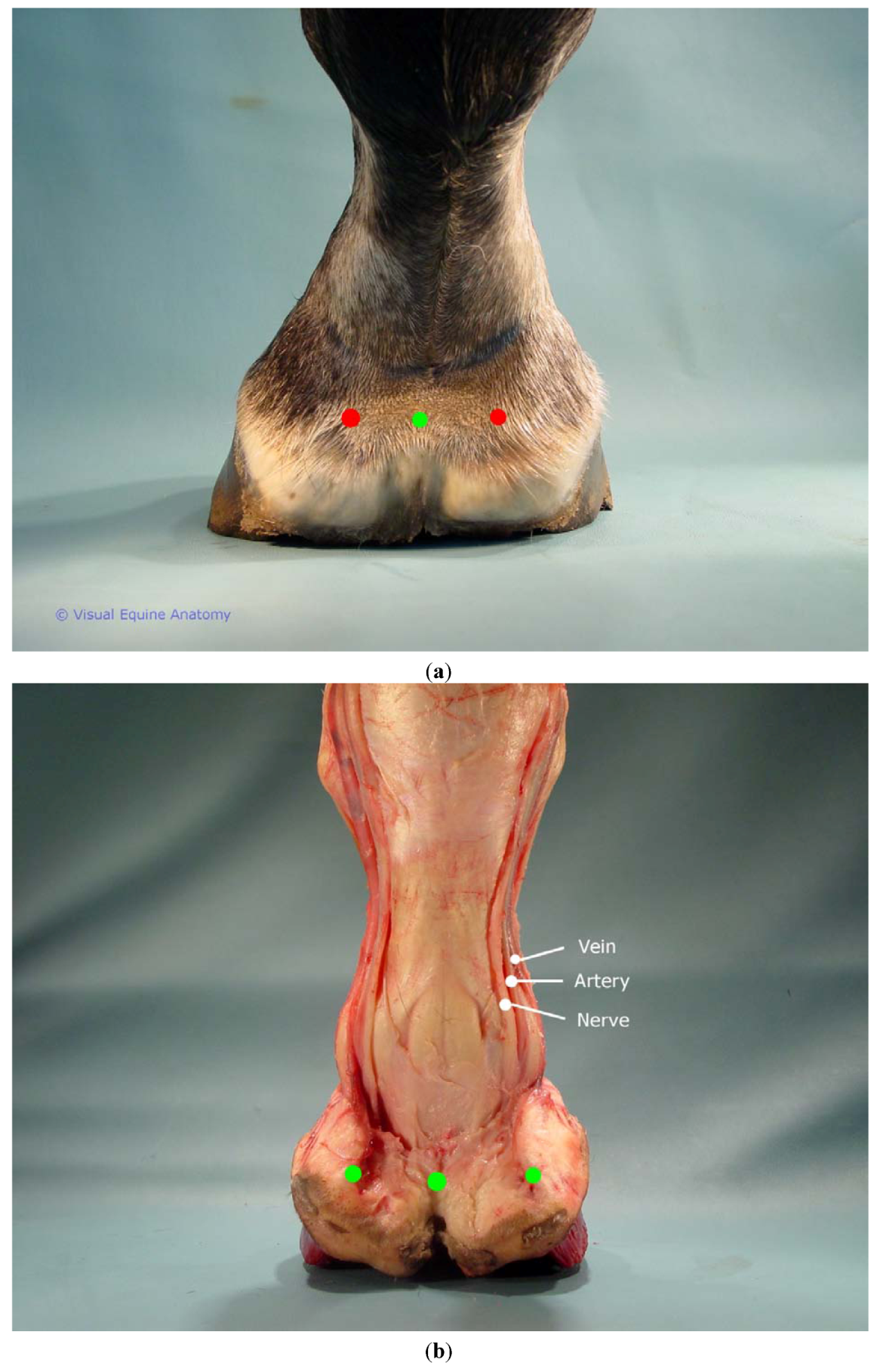
2.1. Vasculature
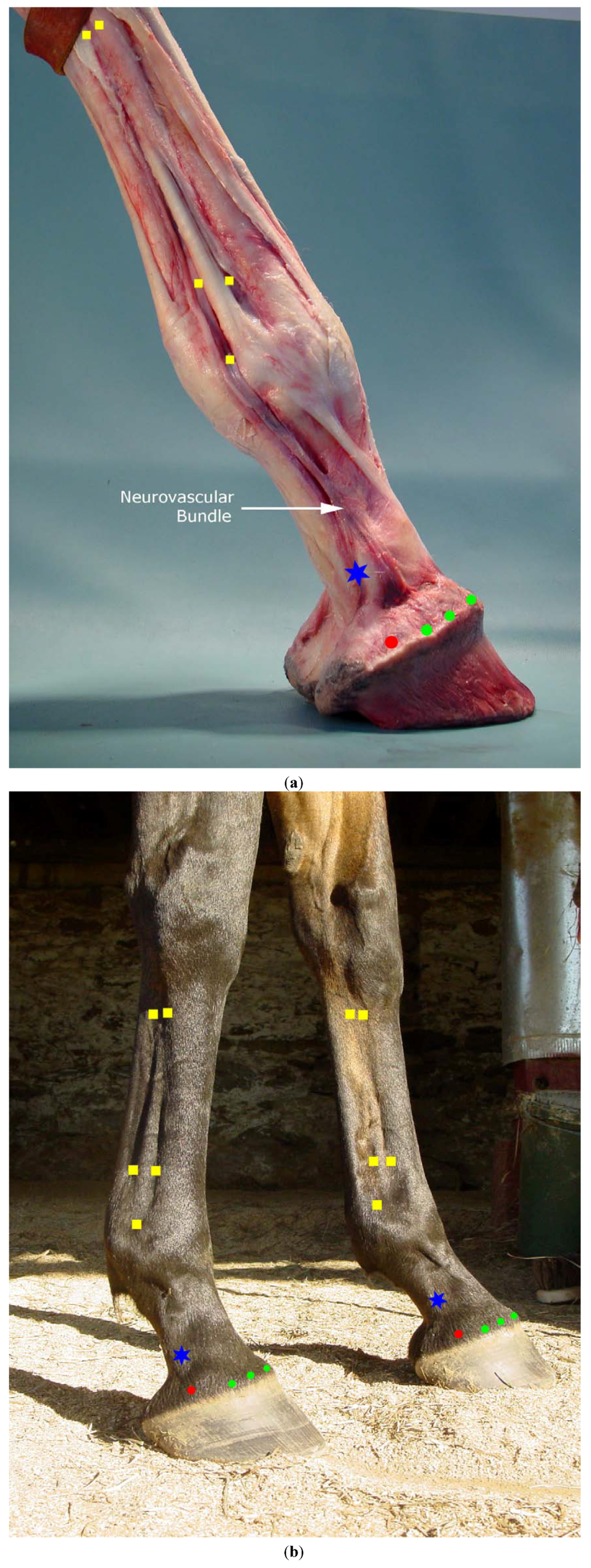
2.2. Innervation
2.3. Nerve Fiber Types and Neuropeptides
2.4. Mechanoreceptors
3. Modified and Newly Proposed Acupuncture Points
3.1. Transpositional Ting Points and Coronet Points

3.2. Proposed Additional New Points: Nerve Block Points
3.2.1. Proposed Modification to Traditional Points Large Intestine 4 (LI4) and Small Intestine 3 (SI3)

3.2.2. Small Intestine 3 (SI3)
3.3. Possible Neurophysiology of Newly Proposed Points
4. Clinical Suggestions for Laminitis Treatment
5. Conclusions
Acknowledgments
Conflict of Interest
References and Notes
- Schoen, A. Veterinary Acupuncture: Ancient Art to Modern Medicine, 2nd ed.; Mosby: St. Louis, MO, USA, 2001. [Google Scholar]
- Pollitt, C.C. Microscopic anatomy and physiology of the hoof. In Equine Podiatry; Floyd, A.E., Mansmann, R.A., Eds.; Saunders: St. Louis, MO, USA, 2007; pp. 90–101. [Google Scholar]
- Molyneux, G.S.; Haller, C.J.; Mogg, K.; Pollitt, C.C. The structure, innervation and location of arteriovenous anastomoses in the equine foot. Equine Vet. J. 1994, 26, 305–312. [Google Scholar] [CrossRef]
- Sack, W.O. Nerve distribution in the metacarpus and front digit of the horse. J. Am. Vet. Med. Assoc. 1975, 167, 298–305. [Google Scholar]
- Bowker, R.M. Innervation of the equine foot: Its importance to the horse and to the clinician. In Equine Podiatry; Floyd, A.E., Mansmann, R.A., Eds.; Saunders: St. Louis, MO, USA, 2007; pp. 74–89. [Google Scholar]
- Bowker, R.M.; Brewer, A.M.; Vex, K.B.; Guida, L.A.; Linder, K.E.; Sonea, I.M.; Stinson, A.W. Sensory receptors in the equine foot. Am. J. Vet. Res. 1993, 54, 1840–1844. [Google Scholar]
- Fleming, P. Transpositional equine acupuncture atlas. In Veterinary Acupuncture: Ancient Art to Modern Medicine, 2nd ed.; Schoen, A., Ed.; Mosby: St. Louis, MO, USA, 2001; pp. 393–431. [Google Scholar]
- Moyer, W.; Schumacher, J.; Schumacher, J. A Guide to Equine Joint Injection and Regional Anesthesia; Veterinary Learning Systems: Yardley, PA, USA, 2007. [Google Scholar]
- Fleming, P. Diagnostic acupuncture palpation examination in the horse. In Veterinary Acupuncture: Ancient Art to Modern Medicine, 2nd ed.; Schoen, A., Ed.; Mosby: St. Louis, MO, USA, 2001; pp. 433–441. [Google Scholar]
- May, K.J. Equine Traditional, Transpositional and Non-Meridian Points. In Proceedings of the Annual Conference of the American Holistic Veterinary Medical Association, Tulsa, OK, USA, 6-9 October 2007; pp. 242–249.
- Hui, K.K.; Liu, J.; Makris, N.; Gollub, R.L.; Chen, A.J.; Moore, C.I.; Kennedy, D.N.; Rosen, B.R.; Kwong, K.K. Acupuncture modulates the limbic system and subcortical gray structures of the human brain: Evidence from fmri studies in normal subjects. Hum. Brain Map. 2000, 9, 13–25. [Google Scholar] [CrossRef]
- Kong, J.; Ma, L.; Gollub, R.L.; Wei, J.; Yang, X.; Li, D.; Weng, X.; Jia, F.; Wang, C.; Li, F.; et al. A pilot study of functional magnetic resonance imaging of the brain during manual and electroacupuncture stimulation of acupuncture point (li-4 hegu) in normal subjects reveals differential brain activation between methods. J. Altern. Complement. Med. 2002, 8, 411–419. [Google Scholar] [CrossRef]
- Kendall, D.E. A scientific model for acupuncture, part I. Am. J. Acupunct. 1989, 17, 251–268. [Google Scholar]
- Kendall, D.E. A scientific model for acupuncture, part II. Am. J. Acupunct. 1989, 17, 343–360. [Google Scholar]
- Robinson, N.G. Neuroanatomic structure and function of acupuncture points around the eye. Am. J. Trad. Chin. Vet. Med. 2007, 2, 33–44. [Google Scholar]
- Steiss, J.E. The neurophysiologic basis of acupuncture. In Veterinary Acupuncture: Ancient Art to Modern Medicine, 2nd ed.; Schoen, A., Ed.; Mosby: St. Louis, MO, USA, 2001; pp. 27–45. [Google Scholar]
- Blythe, L.; Kitchell, R. Electrophysiologic studies of the thoracic limb of the horse. Am. J. Vet. Res. 1982, 43, 1511–1524. [Google Scholar]
- Hood, D.M.; Grosenbaugh, D.A.; Mostafa, M.B.; Morgan, S.J.; Thomas, B.C. The role of vascular mechanisms in the development of acute equine laminitis. J. Vet. Intern. Med. 1993, 7, 228–234. [Google Scholar] [CrossRef]
- Pollitt, C.C.; Davies, C.T. Equine laminitis: Its development coincides with increased sublamellar blood flow. Equine Vet. J. Suppl. 1998, 26 (Suppl), 125–132. [Google Scholar]
- Peroni, J.F.; Moore, J.N.; Noschka, E.; Grafton, M.E.; Aceves-Avila, M.; Lewis, S.J.; Robertson, T.P. Predisposition for venoconstriction in the equine laminar dermis: Implications in equine laminitis. J. Appl. Physiol. 2006, 100, 759–763. [Google Scholar]
- Uchida, S.; Hotta, H. Acupuncture affects regional blood flow in various organs. Evid. Based Complement. Alternat. Med. 2008, 5, 145–151. [Google Scholar] [CrossRef]
- Macgregor, J.; Graf von Schweinitz, D. Needle electromyographic activity of myofascial trigger points and control sites in equine cleidobrachialis muscle-An observational study. Acupunct. Med. 2006, 24, 61–70. [Google Scholar] [CrossRef]
- Langevin, H.M.; Yandow, J.A. Relationship of acupuncture points and meridians to connective tissue planes. Anat. Rec. 2002, 269, 257–265. [Google Scholar] [CrossRef]
- Yamamoto, H.; Kawada, T.; Kamiya, A.; Miyazaki, S.; Sugimachi, M. Involvement of the mechanoreceptors in the sensory mechanisms of manual and electrical acupuncture. Auton. Neurosci. 2011, 160, 27–31. [Google Scholar] [CrossRef]
- Zhao, Z.Q. Neural mechanism underlying acupuncture analgesia. Prog. Neurobiol. 2008, 85, 355–375. [Google Scholar] [CrossRef]
- Feng, K.R. A method of electro-acupuncture treatment for equine intestinal impaction. Am. J. Chin. Med. 1981, 9, 174–180. [Google Scholar] [CrossRef]
- Tangitjaroen, W.; Rice, B.; Xie, H.; Colahan, P. Effects of Electroacupuncture on Pulmonary Function and Immune Function in Horses. In Proceedings of the 56th Annual Convention of the American Association of Equine Practitioners, Baltimore, MD, USA, 4-8 December2010; pp. 413–421.
- Schofield, W.A. Use of acupuncture in equine reproduction. Theriogenology 2008, 70, 430–434. [Google Scholar] [CrossRef]
- Skarda, R.T.; Muir, W.W., 3rd. Comparison of electroacupuncture and butorphanol on respiratory and cardiovascular effects and rectal pain threshold after controlled rectal distention in mares. Am. J. Vet. Res. 2003, 64, 137–144. [Google Scholar] [CrossRef]
- Hackett, G.E.; Spitzfaden, D.M.; May, K.J.; Savoldi, M.; Dodd, M. Acupuncture: Is it Effective for Alleviating Pain in the Horse? In Proceedings of the 43rd Annual Convention of the American Association of Equine Practitioners, Phoenix, AZ, USA, 7-10 December 1997; 43, pp. 333–335.
- Xie, H.; Ott, E.; Colahan, P. Influence of Acupuncture on Experimental Lameness in Horses. In Proceedings of the 47th Annual Convention of the American Association of Equine Practitioners, San Diego, CA, USA, 24-28 November 2001; 47, pp. 347–357.
- Klide, A.M. Acupuncture for treatment of chronic back pain in the horse. Acupunct. Electrother. Res 1984, 9, 57–70. [Google Scholar]
- Xie, H.; Colahan, P.; Ott, E.A. Evaluation of electroacupuncture treatment of horses with signs of chronic thoracolumbar pain. J. Am. Vet. Med. Assoc. 2005, 227, 281–286. [Google Scholar] [CrossRef]
- Pollitt, C.C. The anatomy and physiology of the suspensory apparatus of the distal phalanx. Vet. Clin. North. Am. Equine Pract. 2010, 26, 29–49. [Google Scholar] [CrossRef]
- Heymering, H.W. 80 causes, predispositions, and pathways of laminitis. Vet. Clin. North Am. Equine Pract. 2010, 26, 13–19. [Google Scholar] [CrossRef]
- Johnson, P.J.; Wiedmeyer, C.E.; LaCarrubba, A.; Ganjam, V.K.; Messer, N.T., IV. Laminitis and the equine metabolic syndrome. Vet. Clin. North. Am. Equine Pract. 2010, 26, 239–255. [Google Scholar] [CrossRef]
- McGowan, C.M. Endocrinopathic laminitis. Vet. Clin. North Am. Equine Pract. 2010, 26, 233–237. [Google Scholar] [CrossRef]
- van Eps, A.; Collins, S.N.; Pollitt, C.C. Supporting limb laminitis. Vet. Clin. North Am. Equine Pract. 2010, 26, 287–302. [Google Scholar] [CrossRef]
- Eades, S.C. Overview of current laminitis research. Vet. Clin. North Am. Equine Pract. 2010, 26, 51–63. [Google Scholar] [CrossRef]
- Hood, D.M.; Amoss, M.S.; Grosenbaugh, D.A. Equine laminitis: A potential model of Raynaud’s phenomenon. Angiology 1990, 41, 270–277. [Google Scholar] [CrossRef]
- Belknap, J.K. The pharmacologic basis for the treatment of developmental and acute laminitis. Vet. Clin. North Am. Equine Pract. 2010, 26, 115–124. [Google Scholar] [CrossRef]
- Jones, E.; Vinuela-Fernandez, I.; Eager, R.A.; Delaney, A.; Anderson, H.; Patel, A.; Robertson, D.C.; Allchorne, A.; Sirinathsinghji, E.C.; Milne, E.M.; et al. Neuropathic changes in equine laminitis pain. Pain 2007, 132, 321–331. [Google Scholar] [CrossRef]
- Driessen, B.; Bauquier, S.H.; Zarucco, L. Neuropathic pain management in chronic laminitis. Vet. Clin. North Am. Equine Pract. 2010, 26, 315–337. [Google Scholar] [CrossRef]
- Collins, S.N.; Pollitt, C.; Wylie, C.E.; Matiasek, K. Laminitic pain: Parallels with pain states in humans and other species. Vet. Clin. North Am. Equine Pract. 2010, 26, 643–671. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lancaster, L.S.; Bowker, R.M. Acupuncture Points of the Horse’s Distal Thoracic Limb: A Neuroanatomic Approach to the Transposition of Traditional Points. Animals 2012, 2, 455-471. https://doi.org/10.3390/ani2030455
Lancaster LS, Bowker RM. Acupuncture Points of the Horse’s Distal Thoracic Limb: A Neuroanatomic Approach to the Transposition of Traditional Points. Animals. 2012; 2(3):455-471. https://doi.org/10.3390/ani2030455
Chicago/Turabian StyleLancaster, Lisa S., and Robert M. Bowker. 2012. "Acupuncture Points of the Horse’s Distal Thoracic Limb: A Neuroanatomic Approach to the Transposition of Traditional Points" Animals 2, no. 3: 455-471. https://doi.org/10.3390/ani2030455