1. Introduction
Organized dogfighting is rampant in many parts of the United States even though it is a felony offense in all 50 States. The American Pit Bull Terrier is the breed most commonly associated with organized dogfighting in this country [
1,
2,
3].
Dogs that have been pitted against other dogs typically display scars due to the wounds caused by the teeth of their opponent. The scarring associated with organized dog fights is primarily concentrated on the front legs, head, and muzzle. This is a different pattern of injury than that sustained in spontaneous, non-organized fights between dogs, as documented in an earlier study [
4] and supported by the current study. This is because dogs in organized fights face each other while fighting. In fact, the instruction given by the referee in such fights is “face your dog,” initiating the mutual attack. In addition, while fighting dogs are selected and trained to cause injury to their opponent, non-organized fighting amongst dogs is more likely to consist of ritualized displays and non-injurious biting [
5]. Any injuries that do occur in a spontaneous fights among dogs of the same sex and of similar size are primarily located on the pinnae (ears), dorsal and lateral neck, and front legs—although to a lesser extent than in an organized fight [
4].
In our experience, heavily scarred pit bull-type dogs are often assumed to be highly dog aggressive as the result of a history of fighting. However, we have found that not all dogs seized from dogfighting investigations, including some bearing scars, are aggressive to other dogs. This may be because the dog is in the early stages of its training as a fighting dog and may still retain non-aggressive, social behavior toward other dogs. On the other hand, we have identified some dogs with no or few scars that exhibit significant dog-aggressive tendencies. These dogs are likely young, inexperienced dogs who have not yet been fought, or are dogs that have only been “rolled” (a training fight) once or twice, or breeding dogs who were not used for fighting but possess a strong genetic propensity for aggressive behavior.
It is our experience that some organizations responsible for placing dogs seized from dogfighting investigations do not have the resources to conduct thorough behavior evaluations on the dogs and therefore may rely on extent of scarring to form their decisions on the disposition of the dogs. Highly scarred dogs are usually assumed to be dog-aggressive, although there is currently no commonly accepted threshold for the number of scars on which to base this determination. Other organizations who do conduct behavior evaluations may utilize the extent of scarring as a secondary piece of information, to supplement their disposition decisions, especially with respect to dogs that do not show aggression toward other dogs but also do not engage in friendly behavior. Having information concerning the validity of utilizing the extent of scarring as a proxy for dog aggression would assist these organizations in making more informed decisions, and potentially reduce the euthanasia of non-dog aggressive pit bull-type dogs.
To our knowledge, no analysis has been conducted to determine the relationship between the presence and extent of wounds or scarring and dog aggression among dogs seized from dogfighters. We analyzed this relationship with the following objectives:
Describe the extent and distribution of scarring among dogs seized from organized dogfighting investigations;
Describe the extent of aggression towards other dogs exhibited by dogs in this population;
Analyze the relationship between extent of scarring and aggression towards dogs;
Investigate whether the sex of the dog affects the relationship between scarring and dog aggression;
Determine whether level of scarring is a useful screening test/proxy for aggression towards dogs and, if so, what threshold of scarring is appropriate for identifying dogs at high risk for dog aggression?
2. Materials and Methods
The American Society for the Prevention of Cruelty to Animals (ASPCA) Anti-Cruelty Behavior Team and Forensics Sciences departments deploy nationally to large scale cases of animal cruelty, including dogfighting. Data were collected as part of our routine documentation of dogfighting evidence. We collected data from 279 pit bull-type dogs seized as evidence in four organized dogfighting investigations conducted from 2012 through 2015. The dogs originated from 13 different owners residing in six States in the Southeast and Midwest United States.
In order to be included in the analyses, dogs must have had complete forensic behavioral and medical data available. Dogs included in the study were estimated by veterinary examination to be young adults (six months to three years) or adults (at least three years), based on eruption of all permanent teeth and the degree of dental wear. Puppies less than six months old were excluded from analyses because such dogs are not used in organized fights and do not display scarring consistent with organized dogfighting activities.
Behavioral data were collected during the course of standardized evaluations conducted by teams of forensic animal behavior professionals who were Certified Professional Dog Trainers (CPDT) or Certified Applied Animal Behaviorists (CAAB). These evaluations took place at ASPCA temporary shelters where the dogs were housed and cared for until disposition was granted to the ASPCA by the courts. After they were transferred from their point of origin, the dogs were given at least three days to settle into their new environments before their behavior was assessed. Dogs who were ill, debilitated, or in late pregnancy were not behaviorally evaluated until their physical condition stabilized, as determined by the ASPCA’s veterinary medical team.
In the evaluation, dogs were exposed to a variety of situations that simulated what they would experience in a typical shelter or home environment, including being petted and handled, having food and a rawhide chew taken away, being scolded, meeting a toddler-sized doll, and greeting a friendly dog.
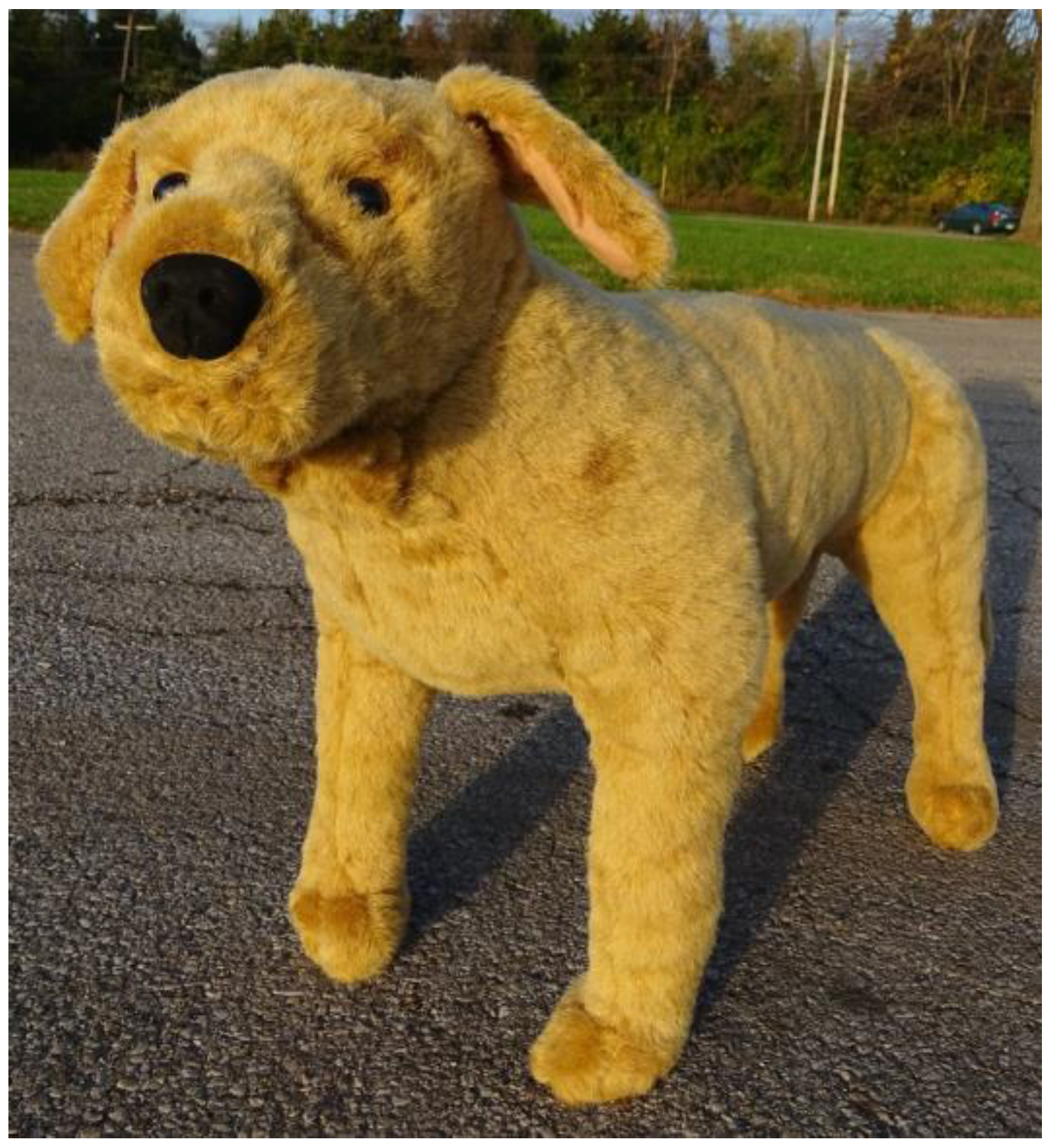
A previous study demonstrated that, for 81% of dogs from dogfighting cases, an aggressive reaction to a life-size model of a Labrador retriever dog matches their reaction to a real dog [
6]. (See
Figure A1 in
Appendix A for a photograph of the model dog). For safety reasons, a similar model dog was used in our behavior assessments to determine whether to introduce the test dog to a friendly stimulus dog. A display of classic dogfighting behavior to the model dog (see
Table 1) was sufficient to halt further testing, precluding an introduction to the stimulus dog. If the test dog exhibited any other reaction to the model dog however, we proceeded to introduce it to the stimulus dog.
The stimulus dog was chosen for its tendency for social, non-aggressive behavior towards other dogs. For logistical reasons, and to increase the generalizability of results, multiple stimulus dogs were used throughout this study, but each test dog met only one stimulus dog. The stimulus dog was always the same sex as the test dog. The stimulus dog was first paused outside the gate of the evaluation area so the dogs could meet initially through a fence. The stimulus dog was then brought into the pen, with both dogs on leash, to assess the test dog’s reaction from a distance for a few seconds. Lastly, the test dog was permitted to meet the stimulus dog nose-to-nose on leash, wearing a muzzle if caution dictated. Aggression on the part of the test dog at any point was sufficient to halt further testing. If no aggression was observed, the two dogs were permitted to interact on leash for 1–3 min. Behaviors recorded during the model and stimulus dog tests utilized in this study are defined in
Table 1. When aggressive as well as non-aggressive behavior was displayed, such as arousal followed by offensive aggression to the stimulus dog, we categorized the interaction according to the aggressive behavior.
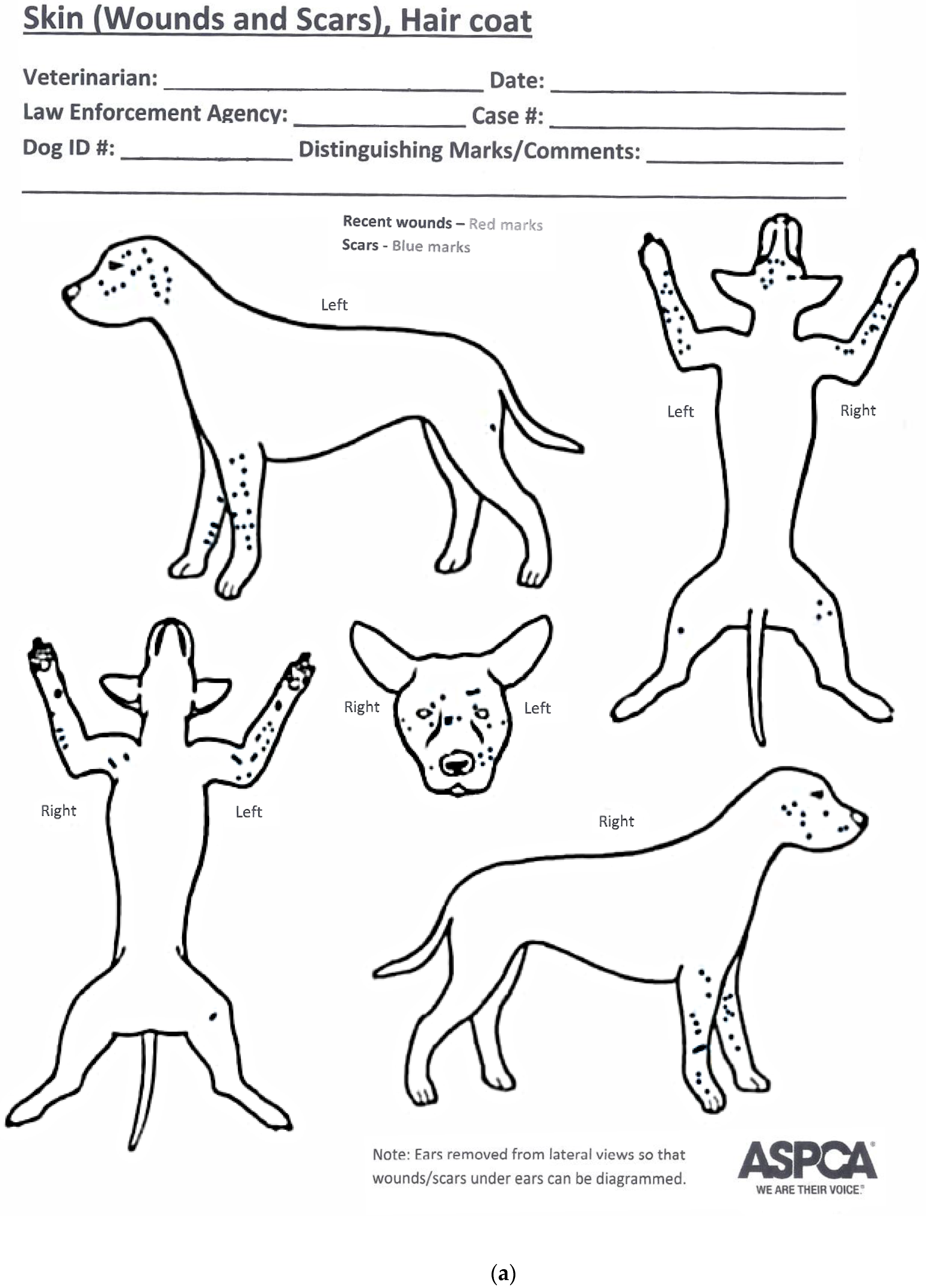
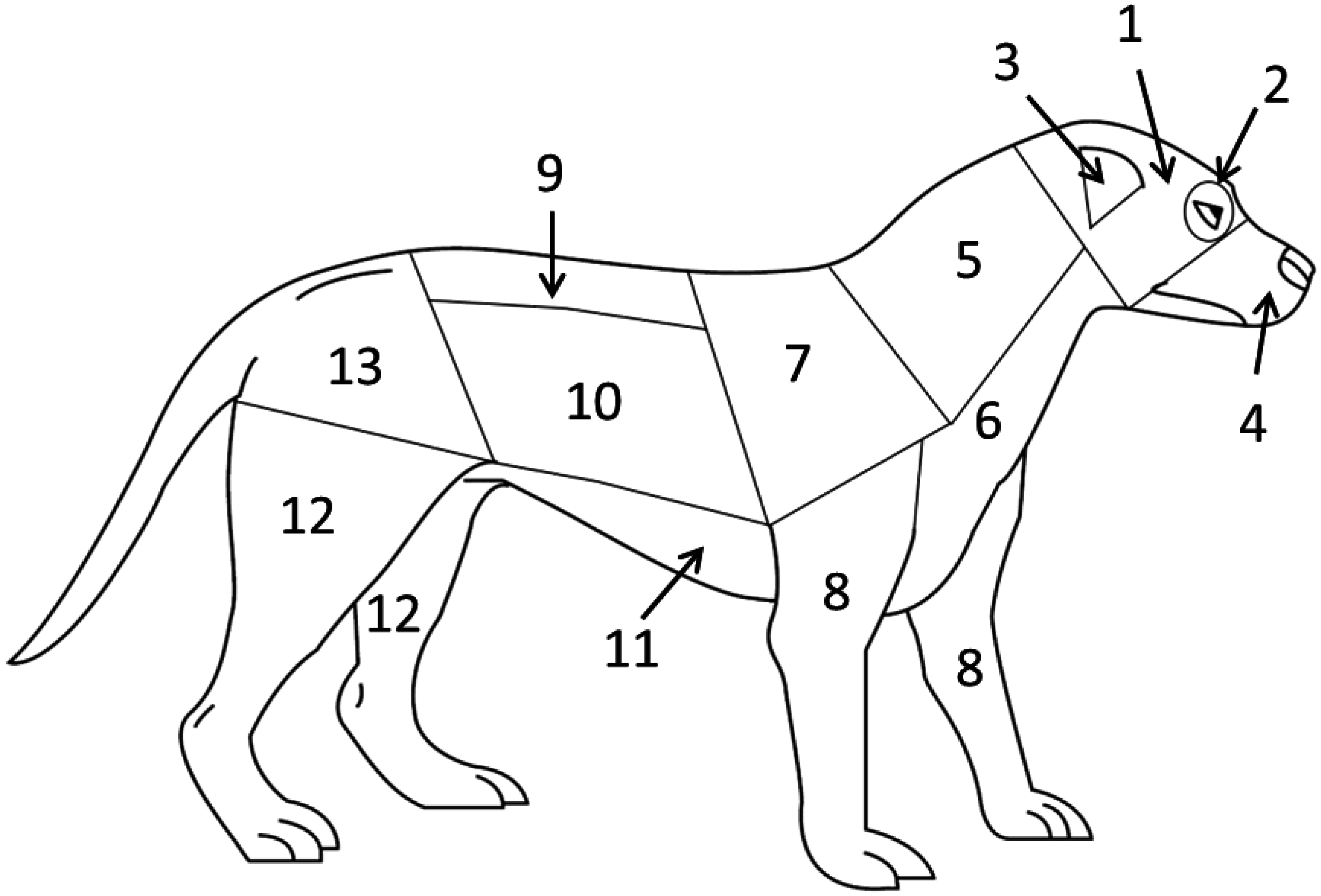
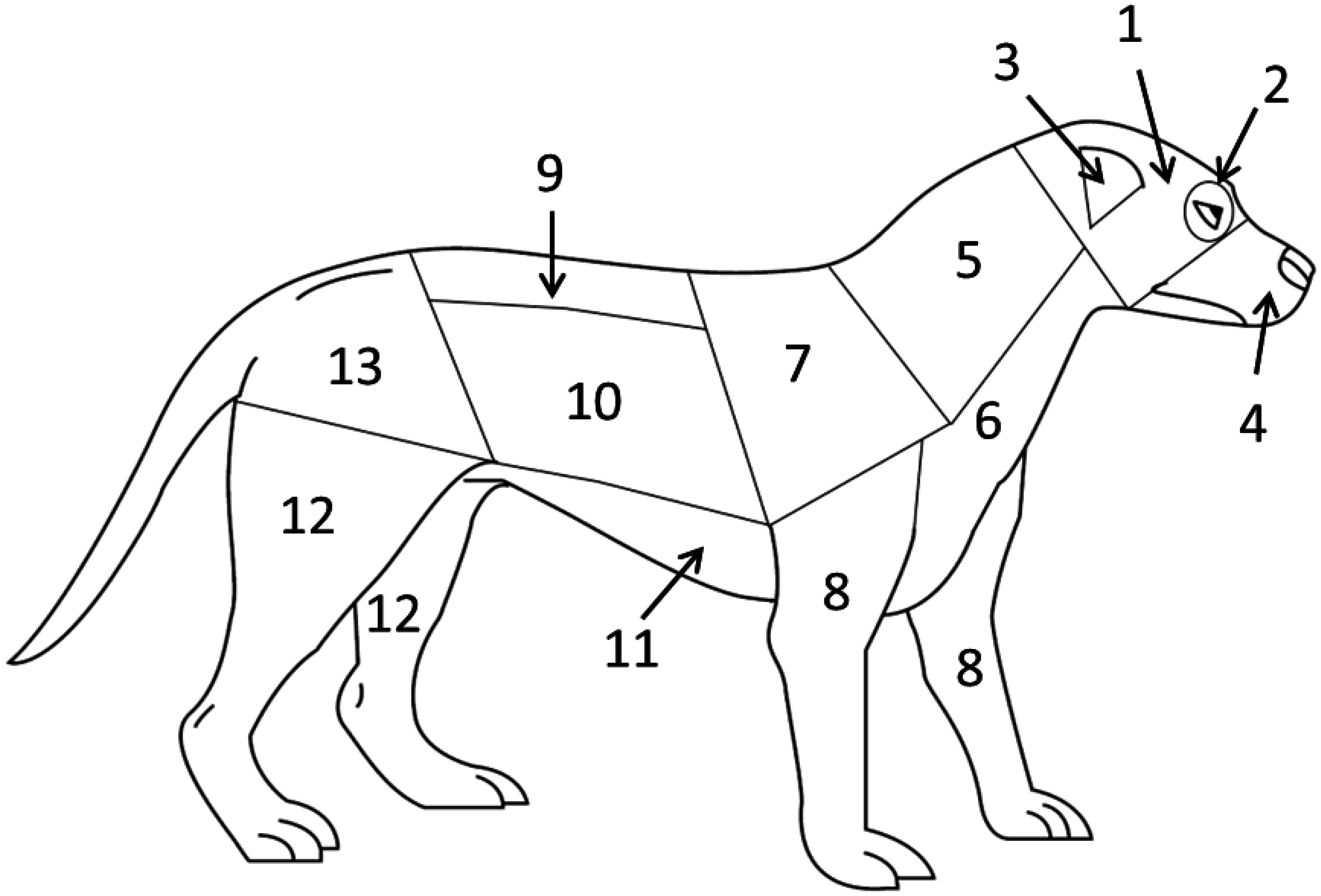
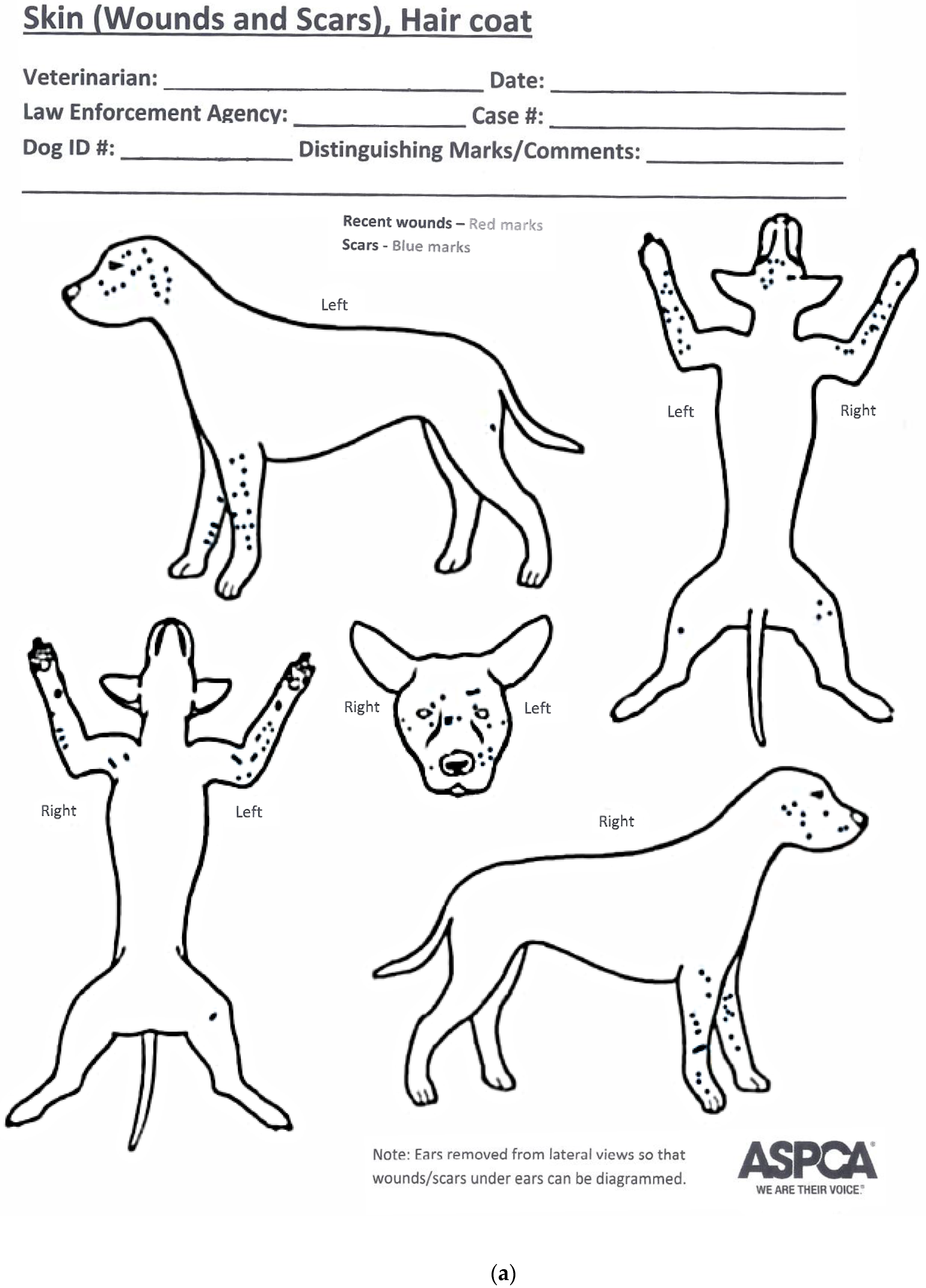
Medical data were collected during the course of standardized forensic medical exams conducted by veterinarians in the ASPCA’s Forensic Sciences department. Exams were initiated upon the dogs’ arrival at the ASPCA’s temporary shelters. We categorized the extent of each dog’s injuries by location in 13 different zones on the body (see
Figure 1) using a standard data collection sheet, commonly called a “scar chart” (see
Figure B1 in
Appendix B). Such categorization was based on results from a previous study, which established that the distribution and extent of scarring on dogs involved in organized dogfighting are significantly different than that of dogs involved in naturally occurring fights [
4]. Dogs involved in organized dogfighting sustain a higher prevalence of injuries on the front legs, dorsal and lateral head, and the muzzle and oral mucosa. Therefore, we summed the number of injuries, including both scars and recent wounds, in these three body zones as well as the total number present on the body. All visible indications of wounds and scars were counted, including older scars that were sufficiently healed such that they appeared as an area of alopecia or depigmented hair coat (white hair regrowth).
The primary behavioral outcome for analysis was dog-directed aggression, defined by demonstrating classic dogfighting behavior to the model dog or offensive aggression to the stimulus dog. For each dog, the total number of scars (including recent wounds) in the three body zones was categorized as: no scars, 1–9 scars, 10–39 scars, or ≥40 scars. These thresholds were selected to ensure that each category had a sufficient number of dogs for meaningful statistical analyses and also for ease of interpretation. The scar-count category was treated as a nominal variable (not ordinal) for analytic purposes. This choice is more conservative statistically and was appropriate in the event of subgroups for which there was not a consistent trend in the relationship between scarring category and dog aggression.
We calculated exact 95% confidence intervals for the proportion of dogs with each behavioral response using the Clopper-Pearson method [
7]. In order to assess whether the relationship between scarring and behavior may differ by sex, the proportion of dogs with each behavioral outcome was also stratified by sex. The overall association between level of scarring and behavior was measured using Fisher’s exact test.
Receiver operator characteristic (ROC) curves [
8] were created to determine which thresholds of scar count (summed from the three selected body zones) are most useful as a screening test for classifying dogs as high risk for dog aggression, in the absence of a full behavioral assessment. The area under the curve (AUC) was used as a measure of overall accuracy of using scar data, and it was calculated separately for male and female dogs. For the threshold that appeared to offer discrimination, we calculated sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) stratified by sex. Where relevant, 95% confidence intervals were calculated using the Clopper–Pearson method. All analyses were conducted in Stata 13.1 (StataCorp LP, College Station, TX, USA).
3. Results
Of the 279 dogs from which data were collected, 24 were excluded from analysis because they did not receive a complete behavioral assessment and 3 were excluded because they were under 6 months old. Among the remaining 252 dogs that qualified for analysis, 54% were female and the majority (60%) were estimated to be adults at least three years of age (
Table 2). 180 dogs (71%) had one or more scars. Among these, the median number of scars (including wounds) was 36.5 (range: 1 to 256). The remaining 29% of dogs had no scars at all. Overall, 14% of dogs had a total scar count between 1 and 9, 23% between 10 and 39, and 34% had 40 or more scars (
Table 3). The majority of dogs had one or more scars in the three zones commonly scarred during dogfighting: front legs (63%), dorsal and lateral head (57%), and muzzle and oral mucosa (51%). Only 26 dogs (10%) had both healed scars and recent wounds in these three body zones, and no dogs had only recent wounds without any scars. All further results rely on the sum of scar data, including both scars and recent wounds, tallied from these three body zones.
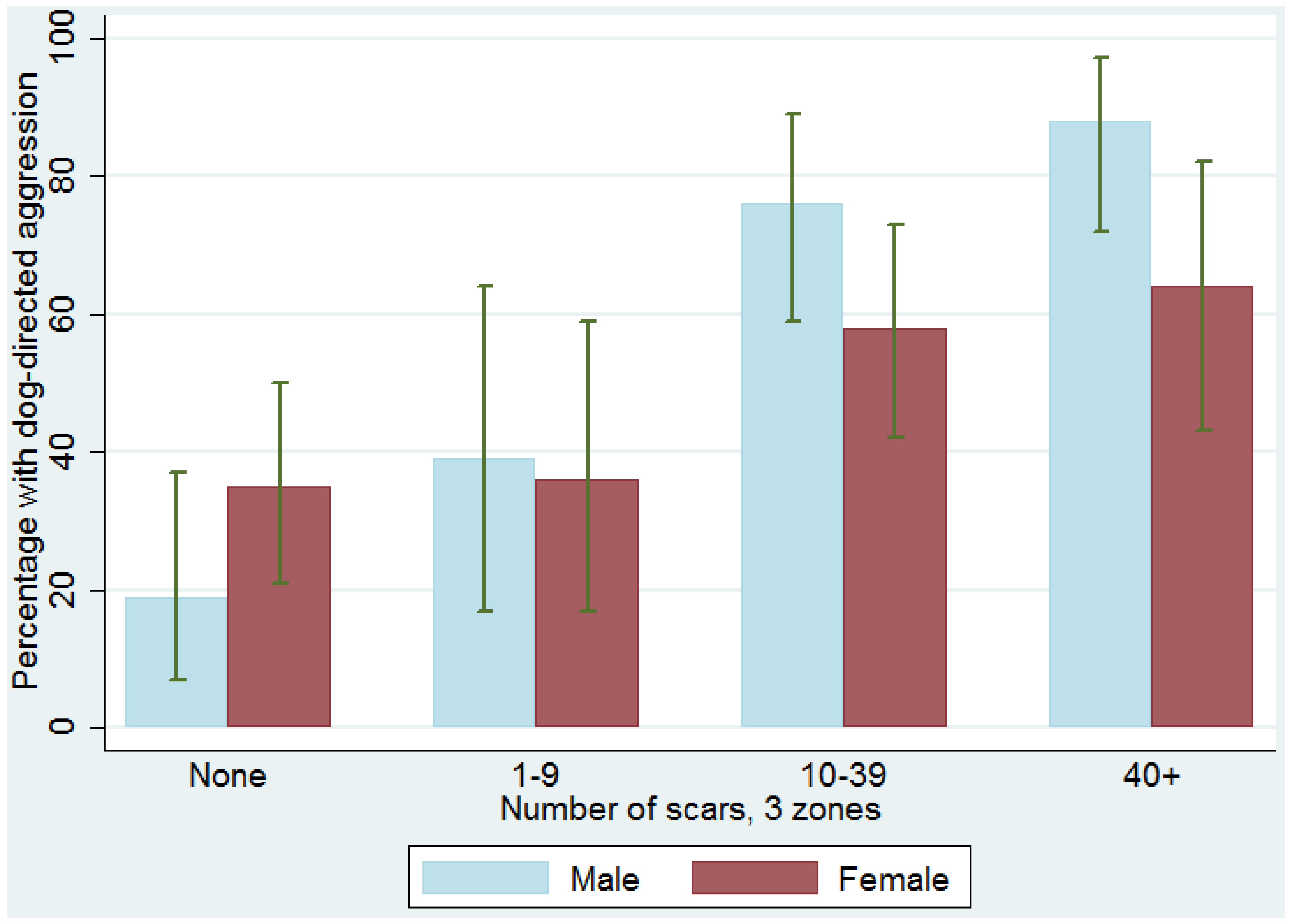
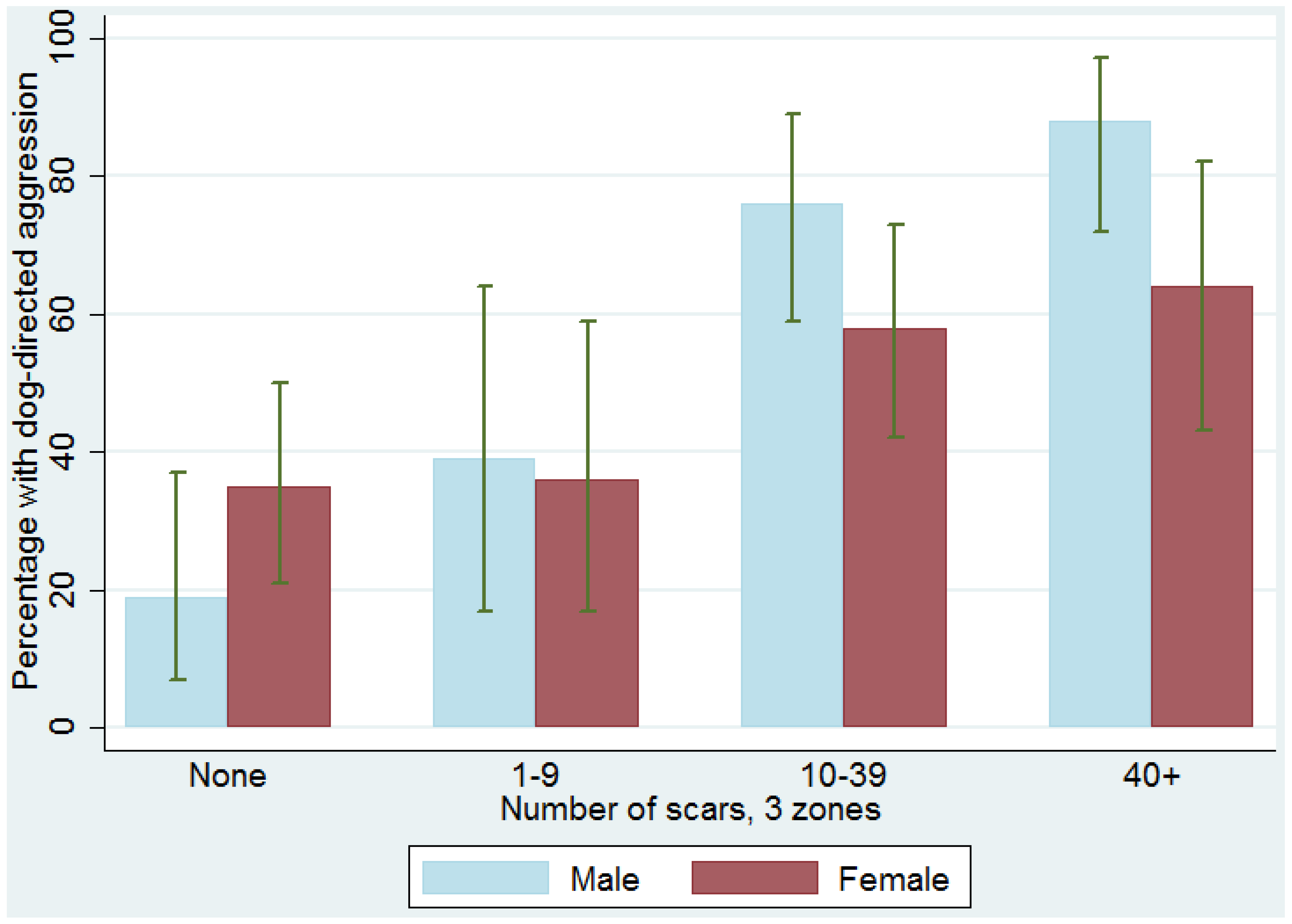
We found a linear relationship between the level of scarring and frequency of dog-directed aggression, with a stronger relationship among males (Fisher’s Exact
p < 0.001) than females (Fisher’s Exact
p = 0.05). Among males, the proportion showing dog-directed aggression ranged from 19% among those with no scars to 88% among those with ≥40 scars. (
Table 4 and
Figure 2). Among females, the proportion showing dog-directed aggression ranged from 35% among those with no scars to 64% among those with ≥40 scars. The presence of both wounds and healed scars on a dog may be considered an indication of participation in multiple dog fighting episodes. When classifying recent wounds separately from healed scars in these body zones, we found the proportion showing dog-directed aggression ranged from 29% among those dogs with neither wounds nor scars, to 62% for those with only healed scars, to 69% for those showing both wounds and healed scars. Because analyzing scar and wound data separately did not provide better prediction of dog aggression than using the sum of both wounds and healed scars, we chose to use the sum of both wounds and healed scars in all analyses.
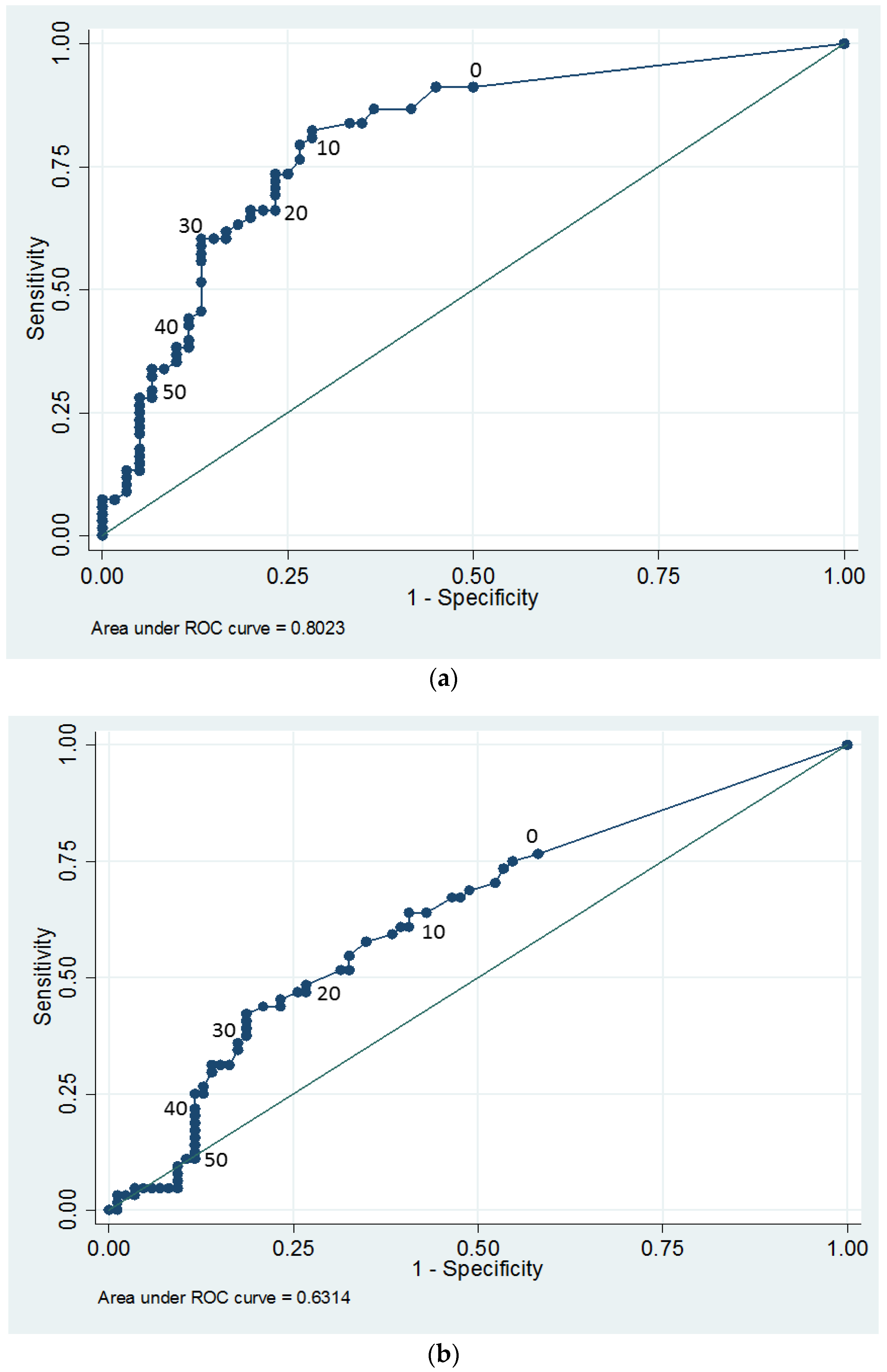
Based on the ROC curves (See
Figure C1 in
Appendix C), summed scar data from the 3 body zones were more reliable as a predictor of dog aggression among males (AUC = 0.82, 95% CI: 0.74–0.90) than females (AUC = 0.63, 95% CI: 0.54–0.73). We reviewed the ROC curves to determine if there was a single threshold of scarring in the 3 body zones that could be useful as an indicator of high risk of dog aggression. Several thresholds between 10 and 20 scars provided similar overall accuracy for classifying dogs as high risk. We chose to further evaluate the threshold of 10 scars for two reasons: logistically, it is easier to count fewer scars accurately, and statistically, a lower threshold reduces the likelihood of a false negative determination (i.e., truly dog-aggressive dogs are less likely to be misclassified as low risk in the screening process).
Table 5 contains the sensitivity, specificity, PPV, and NPV when using the threshold of 10 scars as a screening threshold for dog aggression. The PPV was 82% among males and 60% among females. This means that, among dogs with 10 or more scars in the three body zones, 82% of males and 60% of females could be expected to show dog aggression. The NPV was 74% for males and 65% for females indicating that, among dogs with nine or fewer scars in the three selected body zones, 74% of males and 65% of females would not show dog aggression. Because NPV and PPV are sensitive to the frequency of dog aggression in the population being analyzed, these NPV and PPV results should be generalized only to populations of dogs expected to be at similarly high risk for dog aggression. Therefore, these findings should only be applied to pit bull-type dogs seized from organized dog fighting investigations, and should not be applied to the general population of shelter dogs or to the general population of pit bull-type dogs.
4. Discussion
Among dogs seized in organized dogfighting investigations, a higher percentage of dogs with 10 or more scars on the front legs, dorsal and lateral head, and muzzle and oral mucosa were aggressive to dogs in their behavior evaluation than dogs with fewer than 10 or no scars. This finding suggests that extent of scarring on the three body zones is a fairly accurate tool that may be used in identification of dog aggressive dogs among populations seized in organized dogfighting investigations. However, the accuracy of this tool is imperfect. Some heavily scarred dogs were not dog aggressive and some unscarred or lightly scarred dogs were. Therefore, while 10 or more scars in the three body zones, especially on male dogs, could be useful in triage situations to quickly estimate risk of dog aggression, we recommend also gathering behavioral information about each dog before making disposition decisions.
The extent of scarring in this study ranged widely, from no scars to over 250. In our experience, this is representative of populations seized from dogfighting investigations. The majority of scarring was concentrated on the front legs, dorsal and lateral head, and muzzle and oral mucosa, consistent with findings that these zones are associated with organized dogfighting as opposed to spontaneous, non-organized fights between dogs [
4].
Aggressiveness to dogs also varied widely, from non-aggressive, friendly behavior to highly directed, intense aggression. Overall in this population, which did not include puppies, 53% of dogs displayed either classic dogfighting behavior to the model dog or aggression to the real dog. Again, in our experience this is representative of the range of behavior found in dogs from organized dogfighting populations, based on results of the standardized behavior evaluation described herein.
There was a clear association between extent of scarring and aggression to dogs, with a steady increase in proportion that were aggressive as scar count increased. However, it is critical to note that 28% of dogs with no scars were aggressive to dogs, whereas 22% of dogs bearing 40 or more scars were not. Therefore, while scar count may be an aid in identifying dog aggressive and non-dog aggressive dogs from fighting cases, it is prone to both false negatives and false positives. Therefore, a scar count should not be utilized in isolation when making disposition decisions but in combination with observation of behavior towards dogs including handler and kennel staff reports and careful interactions with other dogs, as in the standardized behavior assessment described above.
The lowest proportion of dog-aggressive dogs was found among unscarred males, followed by unscarred females. These dogs may have been used for breeding purposes and therefore not fought extensively, if at all. Alternatively, they may have been dogs who were not yet rolled in a training fight, or they may have been kept by the owners as status or pet dogs and not for fighting. Many heavily scarred dogs of both sexes were also not aggressive to other dogs, however. These dogs may have been used to train other dogs or they might have been poor fighters but kept for breeding purposes due to their bloodline or fecundity. Conversely, many unscarred or lightly scarred dogs were dog aggressive. Some of these dogs may have been particularly good fighters who were able to disable their opponents quickly while sustaining few injuries. Others may not have been fought much yet, if at all. Still others may have been kept for breeding, or as pet or status dogs and not fought despite their dog aggression.
While it is possible that some older injuries had healed sufficiently such that they may be difficult to visualize upon examination, the severity of wounds associated with dogfighting likely result in scarring that remains visible over time, either as an area of alopecia or depigmented hair coat (white hair regrowth). All visible indications of scars and wounds were counted in this study, thereby utilizing a method available to any veterinarian performing such an examination.
We also must consider that any behavior evaluation protocol is not perfectly accurate at identifying dog aggressive dogs. It is likely that some dogs who were truly dog aggressive did not appear so in their behavior evaluation. Potential reasons for false negatives include dogs fearing the evaluation situation or the evaluators, masking their “normal” behavior. We often see very fearful dogs in fighting dog populations, likely because they spend much of their lives chained in a yard with little experience of the outside world. In addition, the evaluation context may have lacked the necessary stimuli to trigger aggressive behavior in some dogs (e.g., an active, aggressive opponent; a fighting pit). Using a model dog may have limited responses to aroused or precursory dogfighting behavior because the model does not give the dog appropriate feedback that may lead to display of classic dogfighting behavior. Similarly, the stimulus dog test was a controlled situation conducted on leash for just a few minutes with a stimulus dog that was generally rather tolerant and not dog-aggressive. There may have been more aggressive responses from the test dogs had we let the interaction continue longer, or not controlled the dogs on leash, or had the stimulus dog been more dog-reactive. Some fighting dogs may need such feedback from the other dog to initiate aggression, while others do not.
Relatively few dogs were categorized as aroused in this study, and of those, no clear association with scarring was evident (see
Table S1). Aroused was a rather difficult behavior to categorize. Assertive, aroused mounting behavior, and sexually-motivated mounting behavior can be difficult to discern without allowing the dogs to potentially consummate a sexual act. We did observe some sexual mounting behavior directed towards the stimulus dogs even though the test dog and stimulus dog were always of the same sex. This is not unusual among dogs. For ethical reasons, we did not permit the male dogs to attempt sexual behavior toward the stimulus dogs in order to discern arousal from sexual mounting, which we categorized as not aggressive. Of dogs that displayed precursory dogfighting behavior to the model dog, as defined above, there was some association with amount of scarring, but not a clear trend (see
Table S1). All dogs that displayed precursory fighting behavior to the model dog in this study were then introduced to a stimulus dog, and behavior with the stimulus dog took precedence in the analysis. We recommend cautious introductions to real dogs for more information when precursory fighting behavior is observed with a model dog.
In order to obtain a scar count, we recommend that veterinarians involved in dogfighting cases complete a canine skin wound and scar body diagram, otherwise known as a “scar chart”, as part of a complete forensic medical examination (see
Figure S1). A scar count can then be obtained in the three body zones identified as being most consistent with organized dogfighting, based on the completed chart. Particular attention should be paid to whether there are 10 or more scars present in these three body zones. Ten scars was not only a statistically valid threshold in the data in this study, but is also a reasonable number for veterinarians to count accurately.
In a situation where risk of dog aggression must be estimated quickly, dogs with 10 or more scars in the three body zones, especially males, may be considered at high risk. However, because scar count appears to be a useful but imperfect predictor of dog aggression, we recommend gathering behavioral information in multiple contexts and with a variety of stimulus dogs to supplement scar count whenever possible, particularly before making disposition decisions. In addition to handler and kennel staff reports and a standardized behavior evaluation as described above, we recommend that dogs who do not display aggression or who display ambiguous behavior with the stimulus dog should be observed in controlled interactions with a variety of other dogs of both sexes. Interactions should include meeting on a leash and carefully refereed socialization sessions (on muzzle as conditions warrant) in order to ascertain whether a lack of aggression in the evaluation was an effect of the particular stimulus dog chosen, the effect of the evaluation context, or is a behavioral trait of the dog itself.
5. Conclusions
Among pit bull-type dogs seized in investigations of organized dogfighting, there was a significant but imperfect relationship between extent of scarring on the front legs, dorsal and lateral head, and muzzle and oral mucosa with dog aggression exhibited in a standardized behavior evaluation. Dogs with 10 or more scars in these body zones were more likely to display dog aggression than dogs with fewer or no scars. However, about one-quarter of unscarred dogs were dog aggressive and about one-fifth of dogs with 40 or more scars were not. Therefore, we recommend that behavioral information be collected in addition to scar count when making disposition decisions in order to make more accurate predictions and informed decisions. We must emphasize that our findings only apply to dogs with confirmed dogfighting origins, and should not be applied to dogs who do not originate from dogfighting cases.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}