
Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark

 , ,
, ,
Abstract
:
1. Introduction
1.1. Sources of I, Li, and Sr in Ground- and Drinking Water
1.2. Public Health and I, Li, and Sr in Drinking Water
1.2.1. Iodine
1.2.2. Lithium
1.2.3. Strontium
1.3. Study Objectives
2. Experimental Section
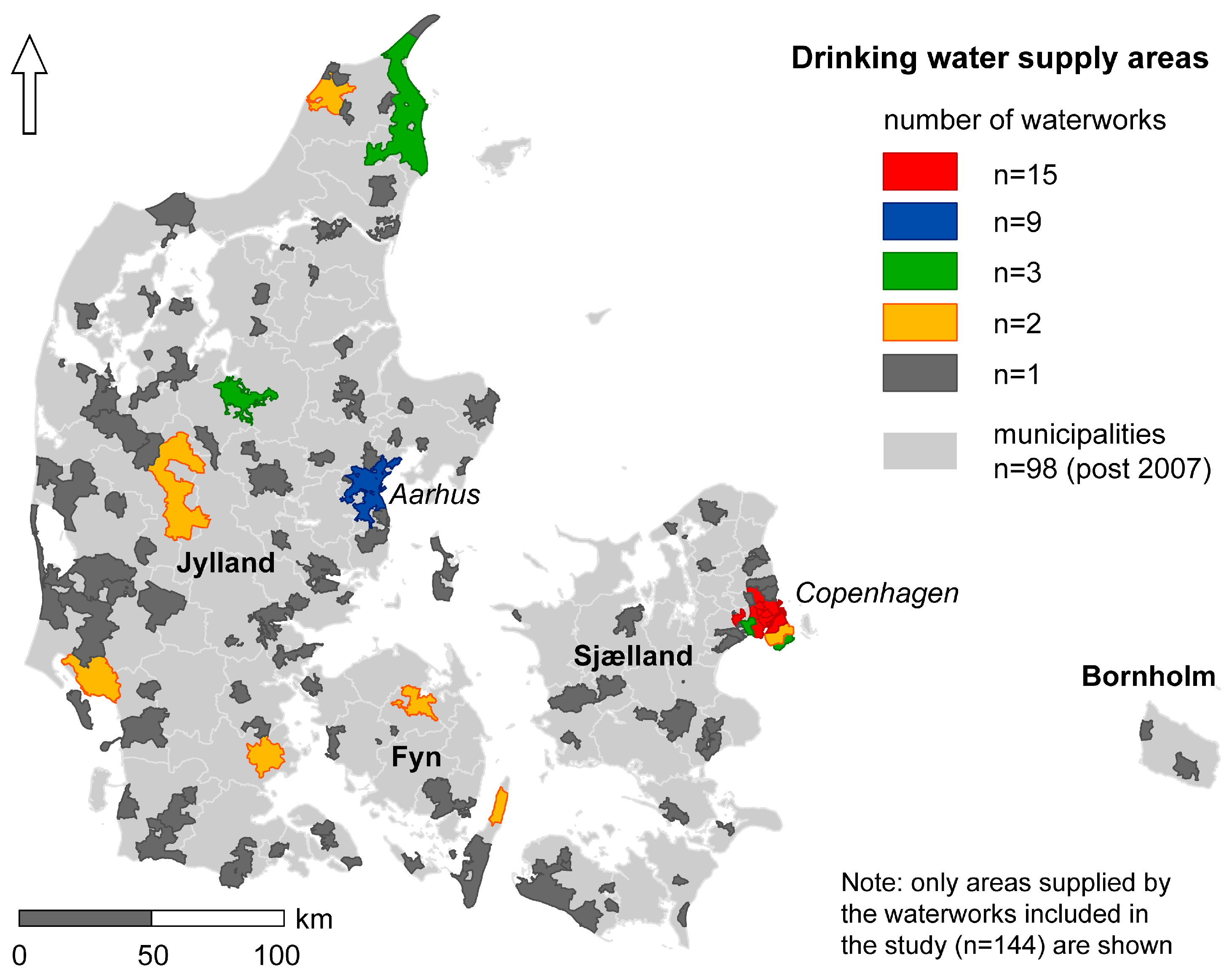
2.1. Danish Public Drinking Water Supply
2.2. Water Chemistry Data (I, Li, and Sr)
2.3. Water Supply Areas

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Title | Iodine (I) | Lithium (Li) | Strontium (Sr) |
|---|---|---|---|
| Unit | μg/L | μg/L | mg/L |
| Lab method | ICP-MS * | ICP-MS | ICP-MS |
| Count (n) | 144 * | 139 | 139 |
| Detection limit (d.l.) | 0.2 | 5 | 0.005 |
| <d.l. (%) | 6.25 | 18.7 | 0 |
| Substitution (0.5*d.l.) | 0.1 | 2.5 | - |
| Min. concentration | 0.1 | 2.5 | 0.07 |
| Max. concentration | 126 | 30.7 | 14.45 |
| Mean concentration | 13.97 * | 11.04 | 1.31 |
| Median concentration | 11.25 * | 10.30 | 0.59 |

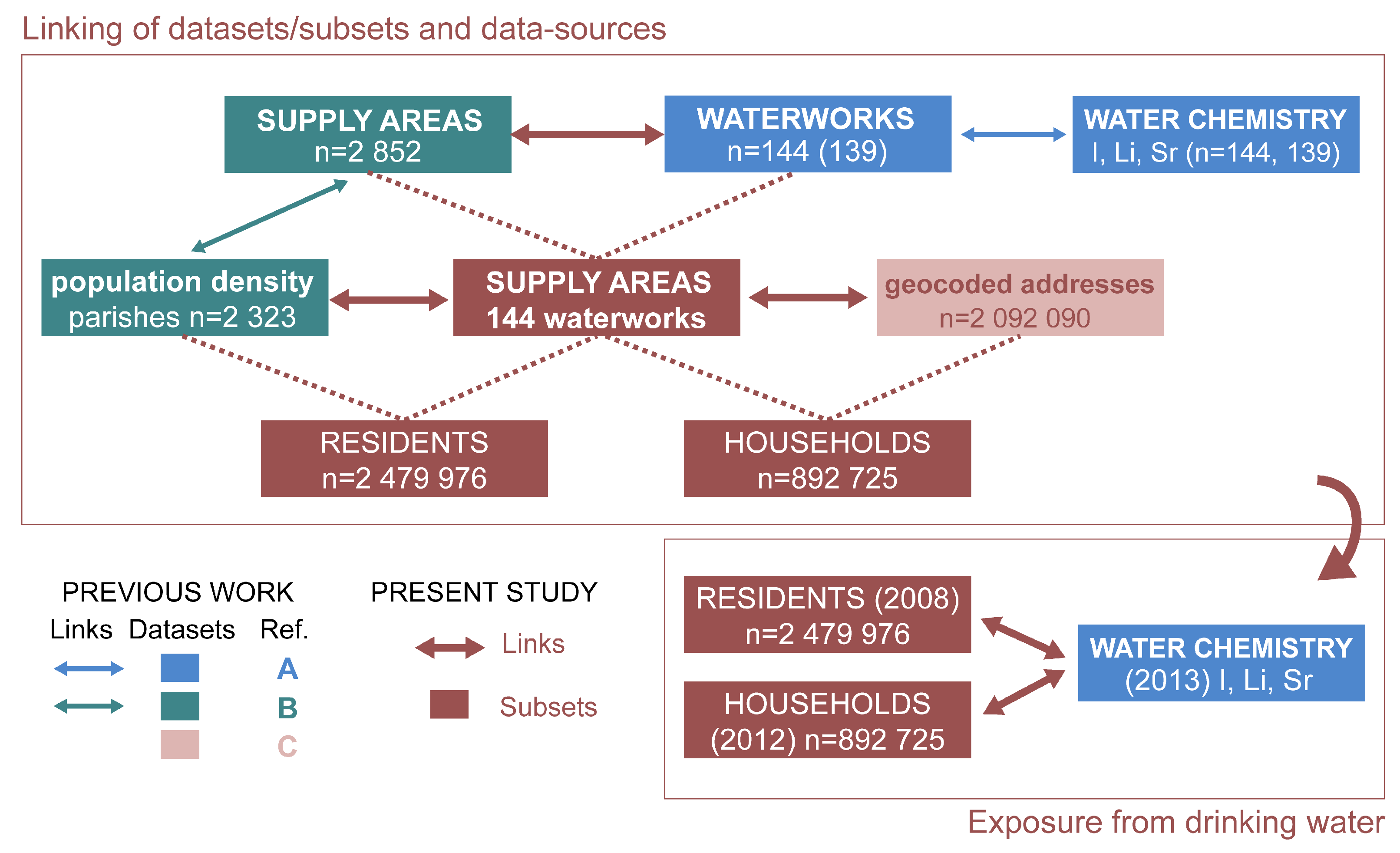
2.4. Estimation of the Population Living in the Selected Water Supply Areas
- 1st dataset: a population density map based on the population counts in the smallest census unit (parishes) for 2008 (further details can be found in [57]). This method yields “number of residents” in the selected supply areas.
- 2nd dataset: a database including geocoded addresses with at least one registered resident from the Danish Civil Registration System (DCRS), provided by the Centre for Integrated Register-Based Research at Aarhus University (CIRRAU). This database contains one record for each specific address (municipality, road, house number, and, if relevant, door number) used as a residence in DCRS [58]. The DCRS was established in 1968 and has since recorded current and historical information not only on the place of residence, but also on vital status, gender, place and date of birth, parents, spouses, and siblings and twins for all persons living in Denmark [59]. This information is regarded as being of very high quality and yields an important and rare asset which can be used for epidemiological research [59]. A subset of this database has been used here. It consists of the geocoded addresses for 2012 only (n = 2,092,090), which are further referred to as “households”.
2.5. Inverse Distance Weighted Interpolation and Cluster Analysis
2.5.1. Data Pretreatment
2.5.2. Inverse distance weighted interpolation
2.5.3. Cluster Analysis
2.6. Exposure Analysis

3. Results and Discussion
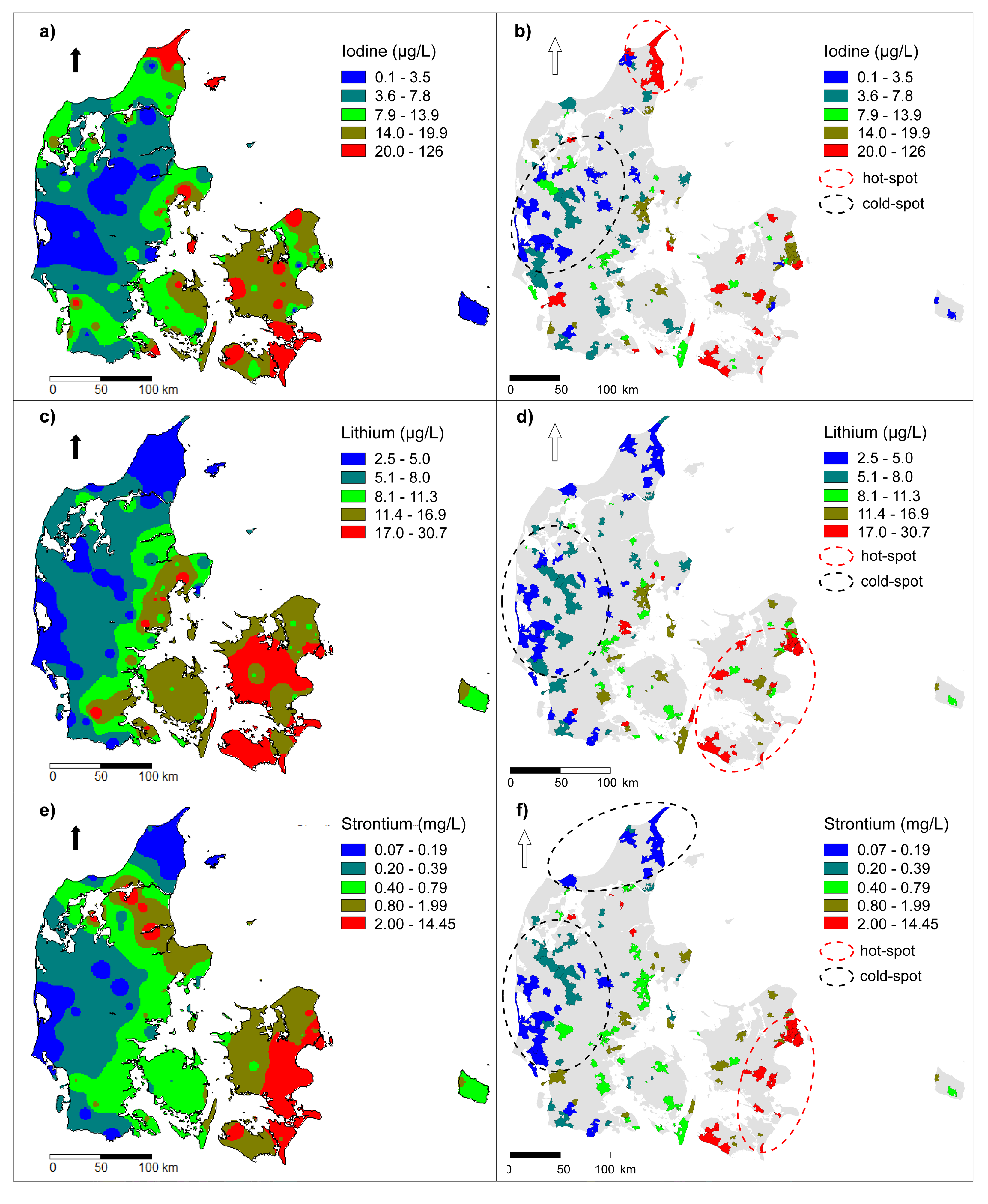
3.1. Spatial Distribution of Drinking Water I, Li and Sr

| Element | Type of Cluster | Nmeasurements Inside Cluster | Mean Concentration | p-value | |
|---|---|---|---|---|---|
| Inside Cluster | Outside Cluster | ||||
| Iodine (μg/L) | Hot spot | 4 | 77.09 | 9.92 | 0.001 |
| Cold spot | 26 | 2.37 | 13.69 | 0.003 | |
| Lithium (μg/L) | Hot spot | 27 | 19.08 | 9.10 | 0.001 |
| Cold spot | 27 | 4.56 | 21.60 | 0.002 | |
| Strontium (mg/L) | Hot spot | 27 | 2.66 | 0.45 | 0.001 |
| Cold spot | 27 | 0.21 | 0.84 | 0.001 | |
| Cold spot | 10 | 0.15 | 0.72 | 0.049 | |
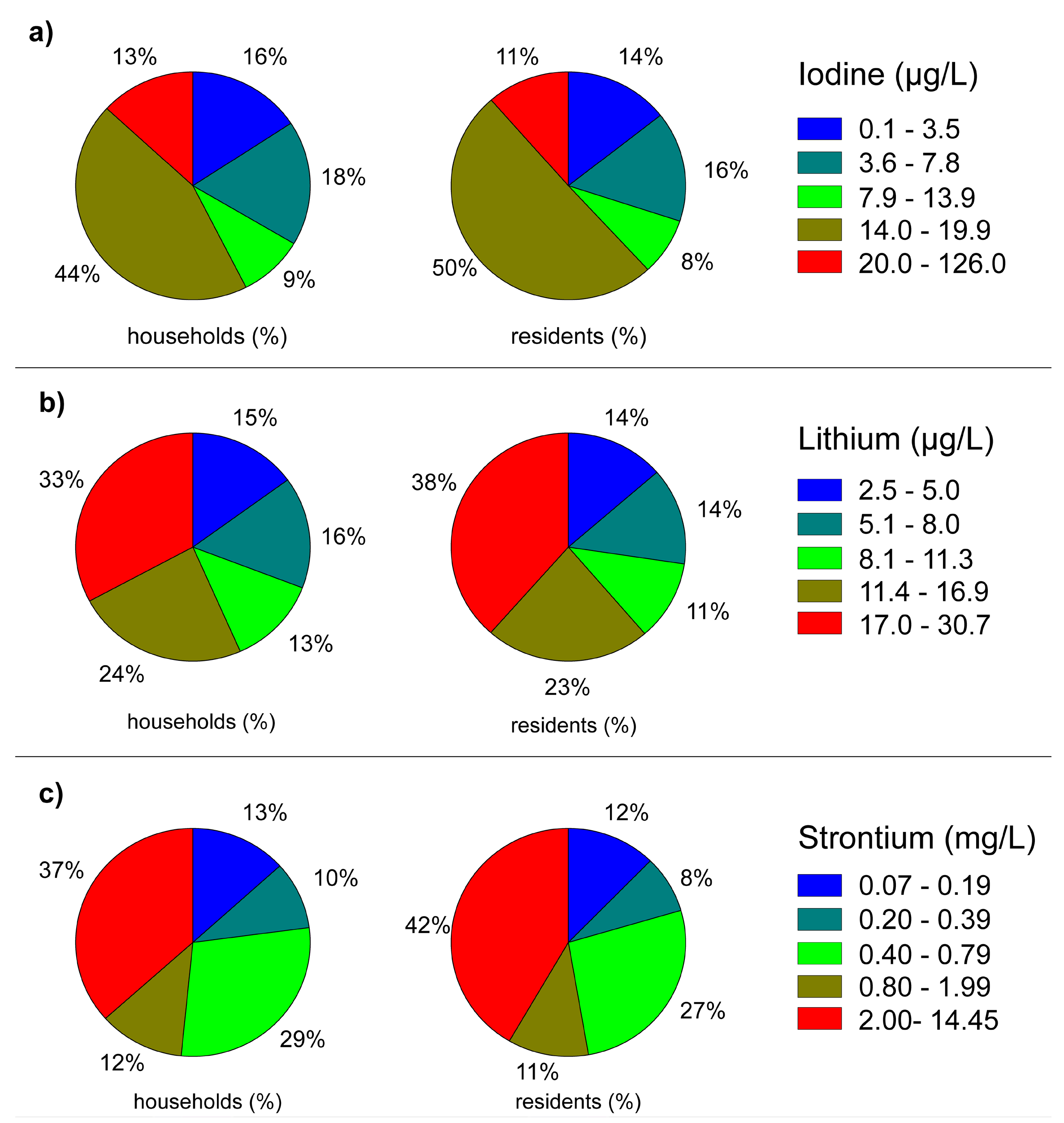
3.2. Exposure to I, Li, and Sr via Drinking Water

| Element | Concentration | Households | Residents | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Iodine | <3.6 μg/L | 140,593 | 15.7 | 356,533 | 14.4 |
| 3.6 to 7.8 μg/L | 158,213 | 17.7 | 388,008 | 15.6 | |
| 7.9 to 13.9 μg/L | 80,677 | 9.0 | 201,478 | 8.1 | |
| 14.0 to 19.9 μg/L | 396,070 | 44.4 | 1,250,457 | 50.4 | |
| 20.0 to 126.0 μg/L | 117,172 | 13.1 | 283,500 | 11.4 | |
| Total | 892,725 | 100 | 2,479,976 | 100 | |
| Lithium | <5.1 μg/L | 130,954 | 15.0 | 332,613 | 13.6 |
| 5.1 to 8.0 μg/L | 138,441 | 15.8 | 335,875 | 13.8 | |
| 8.1 to 11.3 μg/L | 109,879 | 12.6 | 277,078 | 11.3 | |
| 11.4 to 16.9 μg/L | 207,907 | 23.8 | 556,759 | 22.8 | |
| 17.0 to 30.7 μg/L | 287,194 | 32.8 | 940,380 | 38.5 | |
| Total | 874,375 | 100 | 2,442,705 | 100 | |
| Strontium | <0.2 mg/L | 116,284 | 13.3 | 300,856 | 12.3 |
| 0.20 to 0.39 mg/L | 84,145 | 9.6 | 199,114 | 8.2 | |
| 0.40 to 0.79 mg/L | 250,705 | 28.7 | 654,183 | 26.8 | |
| 0.80 to 1.99 mg/L | 103,087 | 11.8 | 272,128 | 11.1 | |
| 2.00 to 14.45 mg/L | 320,154 | 36.6 | 1,016,424 | 41.6 | |
| Total | 874,375 | 100 | 2,442,705 | 100 | |
3.3. Discussion

4. Conclusions
Acknowledgments
Author Contributions
Supplementary Materials
Conflicts of Interest
References and Notes
- Villanueva, C.M.; Kogevinas, M.; Cordier, S.; Templeton, M.R.; Vermeulen, R.; Nuckols, J.R.; Nieuwenhuijsen, M.J.; Levallois, P. Assessing exposure and health consequences of chemicals in drinking water: Current state of knowledge and research needs. Environ. Health Perspect. 2014, 122, 213–221. [Google Scholar] [PubMed]
- Reimann, C.; Birke, M. Geochemistry of European Bottled Water; Borntraeger Science Publishers: Stuttgart, Germany, 2010. [Google Scholar]
- Voutchkova, D.D.; Ernstsen, V.; Hansen, B.; Sørensen, B.L.; Zhang, C.; Kristiansen, S.M. Assessment of spatial variation in drinking water iodine and its implications for dietary intake: A new conceptual model for Denmark. Sci. Total Environ. 2014, 493, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Voutchkova, D.D.; Kristiansen, S.M.; Hansen, B.; Ernstsen, V.; Sørensen, B.L.; Esbensen, K.H. Iodine concentrations in Danish groundwater: Historical data assessment 1933–2011. Environ. Geochem. Health 2014, 36, 1151–1164. [Google Scholar] [CrossRef] [PubMed]
- Voutchkova, D.D.; Hansen, B.; Ernstsen, V.; Kristiansen, S.M. Hydro-geochemical characterisation of Danish groundwaters in relation to iodine. Paper III in PhD thesis [70].
- Kesler, S.E.; Gruber, P.W.; Medina, P.A.; Keoleian, G.A.; Everson, M.P.; Wallington, T.J. Global lithium resources: Relative importance of pegmatite, brine and other deposits. Ore Geol. Rev. 2012, 48, 55–69. [Google Scholar] [CrossRef]
- Hinsby, K.; Rasmussen, E.S.; Henriksen, H.J. European Reference Aquifers: The Miocene Sand Aquifers of Western Denmark. In Report for the EU Research Project (‘BASELINE’): Natural Baseline Quality of European Groundwater: A basis for Aquifer Management; Geological Survey of Denmark and Greenland (GEUS): Copenhagen, Denmark, 2003; pp. 1–18. [Google Scholar]
- Bonnesen, E.P.; Larsen, F.; Sonnenborg, T.O.; Klitten, K.; Stemmerik, L. Deep saltwater in Chalk of North-West Europe: Origin, interface characteristics and development over geological time. Hydrogeol. J. 2009, 17, 1643–1663. [Google Scholar] [CrossRef]
- Ramsay, L. Strontium i Grundvand & Drikkevand i Roskilde Amt; Roskilde Amt: Roskilde, Denmark, 2005. (In Danish) [Google Scholar]
- Danish Ministry of the Environment (DME). Bekendtgørelse om Vandkvalitet og Tilsyn Med Vandforsyningsanlæg BEK nr 292 af 26/03/2014; Miljøministeriet: Copenhagen, Denmark, 2014. (In Danish) [Google Scholar]
- World Health Organization (WHO). Iodine Deficiency in Europe: A Continuing Public Health Problem; World Health Organization, United Nations Children’s Fund: Geneva, Switzerland, 2007; pp. 1–86. [Google Scholar]
- World Health Organization (WHO). Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers, 3rd ed.; World Health Organization: Geneva, Switzerland, 2007; pp. 1–97. [Google Scholar]
- Soldin, O.P. Iodine Status Reflected by Urinary Concentrations: Comparison with the USA and Other Countries. In Comprehensive Handbook of Iodine: Nutritional, Biochemical, Pathological and Therapeutic Aspects; Preedy, V.R., Burrow, G.N., Watson, R., Eds.; Elsevier: Amsterdam, The Netherlands, 2009; pp. 1129–1137. [Google Scholar]
- Zimmermann, M.B. Iodine deficiency in industrialized countries. Clin. Endocrinol. 2011, 75, 287–288. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Andersson, M. Update on iodine status worldwide. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Andersson, M.; Zimmermann, M.B. Global iodine nutrition: Where do we stand in 2013? Thyroid 2013, 23, 523–528. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Salt Reduction and Iodine Fortification Strategies in Public Health: Report of a Joint Technical Meeting; World Health Organization: Geneva, Switzerland, 2014; pp. 1–34. [Google Scholar]
- Speeckaert, M.M.; Speeckaert, R.; Wierckx, K.; Delanghe, J.R.; Kaufman, J.M. Value and pitfalls in iodine fortification and supplementation in the 21st century. Br. J. Nutr. 2011, 106, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.; Dary, O.; Cappuccio, F.P.; Neufeld, L.M.; Harding, K.B.; Zimmermanne, M.B. Collaboration to optimize dietary intakes of salt and iodine: A critical but overlooked public health issue. Bull. World Health Organ. 2012, 90, 73–74. [Google Scholar] [CrossRef] [PubMed]
- Fuge, R. Soils and Iodine Deficiency. In Essentials of Medical Geology: Impacts of the Natural Environment on Public Health; Selinus, O., Alloway, B.J., Centeno, J.A., Finkelman, R.B., Fuge, R., Lindh, U., Smedley, P., Eds.; Elsevier: Amsterdam, The Netherlands, 2005; pp. 417–433. [Google Scholar]
- Laurberg, P.; Jørgensen, T.; Perrild, H.; Ovesen, L.; Knudsen, N.; Pedersen, I.B.; Rasmussen, L.B.; Carlé, A.; Vejbjerg, P. The Danish investigation on iodine intake and thyroid disease, DanThyr: Status and perspectives. Eur. J. Endocrinol. 2006, 155, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.N.; Fagt, S.; Groth, M.V.; Christensen, T.; Biltoft-Jensen, A.; Matthiessen, J.; Andersen, N.L.; Kørup, K.; Hartkopp, H.; Ygil, K.H.; Hinsch, H.J.; Saxholt, E.; Trolle, E. Danskernes Kostvaner 2003–2008; National Food Institute, Technical University of Denmark (DTU Fødevareinstituttet): Kongens Lyngby, Denmark, 2010; pp. 1–200. (In Danish) [Google Scholar]
- Rasmussen, L.B.; Larsen, E.H.; Ovesen, L. Iodine content in drinking water and other beverages in Denmark. Eur. J. Clin. Nutr. 2000, 54, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.B.; Ovesen, L.; Bülow, I.; Jørgensen, T.; Knudsen, N.; Laurberg, P.; Perrild, H. Dietary iodine intake and urinary iodine excretion in a Danish population: Effect of geography, supplements and food choice. Br. J. Nutr. 2002, 87, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.M.; Laurberg, P.; Nøhr, S.; Jørgensen, A.; Andersen, S. Iodine in drinking water varies by more than 100-fold in Denmark. Importance for iodine content of infant formulas. Eur. J. Endocrinol. 1999, 140, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.M.; Liu, S.J.; Sun, D.J.; Zhang, S.B.; Su, X.H.; Shen, Y.F.; Han, H.P. Geographical distribution of drinking-water with high iodine level and association between high iodine level in drinking-water and goitre: A Chinese national investigation. Br. J. Nutr. 2011, 106, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Lv, S.; Wang, Y.; Xu, D.; Rutherford, S.; Chong, Z.; Du, Y.; Jia, L.; Zhao, J. Drinking water contributes to excessive iodine intake among children in Hebei, China. Eur. J. Clin. Nutr. 2013, 67, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Del Grande, C.; Muti, M.; Musetti, L.; Corsi, M.; Pergentini, I.; Turri, M.; Corsini, G.U.; Dell’Osso, L. Lithium and valproate in manic and mixed states: A naturalistic prospective study. J. Psychopathol. 2014, 20, 6–10. [Google Scholar]
- Grunze, H.; Vieta, E.; Goodwin, G.M.; Bowden, C.; Licht, R.W.; Möller, H.J.; Kasper, S. The world federation of societies of biological psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders: Update 2012 on the long-term treatment of bipolar disorder. World J. Biol. Psychiatry 2013, 14, 154–219. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Pretty, H.; Hawton, K.; Geddes, J.R. Lithium in the prevention of suicidal behavior and all-cause mortality in patients with mood disorders: A systematic review of randomized trials. Am. J. Psychiatry 2005, 162, 1805–1819. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J.; Tondo, L.; Davis, P.; Pompili, M.; Goodwin, F.K.; Hennen, J. Decreased risk of suicides and attempts during long-term lithium treatment: A meta-analytic review. Bipolar Disord. 2006, 8, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Schrauzer, G.N.; Shrestha, K.P. Lithium in drinking water and the incidences of crimes, suicides, and arrests related to drug addictions. Biol. Trace Elem. Res. 1990, 25, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Ohgami, H.; Terao, T.; Shiotsuki, I.; Ishii, N.; Iwata, N. Lithium levels in drinking water and risk of suicide. Br. J. Psychiatry 2009, 194, 464–465. [Google Scholar] [CrossRef] [PubMed]
- Blüml, V.; Regier, M.D.; Hlavin, G.; Rockett, I.R.H.; König, F.; Vyssoki, B.; Bschor, T.; Kapusta, N.D. Lithium in the public water supply and suicide mortality in Texas. J. Psychiatr. Res. 2013, 47, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Helbich, M.; Leitner, M.; Kapusta, N.D. Geospatial examination of lithium in drinking water and suicide mortality. Int. J. Health Geogr. 2012, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kapusta, N.D.; Mossaheb, N.; Etzersdorfer, E.; Hlavin, G.; Thau, K.; Willeit, M.; Praschak-Rieder, N.; Sonneck, G.; Leithner-Dziubas, K. Lithium in drinking water and suicide mortality. Br. J. Psychiatry 2011, 198, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Kabacs, N.; Memon, A.; Obinwa, T.; Stochl, J.; Perez, J. Lithium in drinking water and suicide rates across the East of England. Br. J. Psychiatry 2011, 198, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Kovacsics, C.E.; Gottesman, I.I.; Gould, T.D. Lithium’s Antisuicidal Efficacy: Elucidation of Neurobiological Targets Using Endophenotype Strategies. Annu. Rev. Pharmacol. Toxicol. 2009, 49, 175–198. [Google Scholar] [CrossRef] [PubMed]
- Hernlund, E.; Svedbom, A.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8. [Google Scholar] [CrossRef]
- Svedbom, A.; Hernlund, E.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: A compendium of country-specific reports. Arch. Osteoporos. 2013, 8. [Google Scholar] [CrossRef]
- Skoryna, S.C. Effects of oral supplementation with stable strontium. Can. Med. Assoc. J. 1981, 125, 703–712. [Google Scholar] [PubMed]
- Dahl, S.G.; Allain, P.; Marie, P.J.; Mauras, Y.; Boivin, G.; Ammann, P.; Tsouderos, Y.; Delmas, P.D.; Christiansen, C. Incorporation and distribution of strontium in bone. Bone 2001, 28, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Watts, P.; Howe, P. Strontium and Strontium Compounds (Concise International Chemical Assessment Document, No 77); World Health Organization (WHO): Geneva, Switzerland, 2010; pp. 1–67. [Google Scholar]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Strontium; Agency for Toxic Substances and Disease Registry, Division of Toxicology/Toxicology Information Branch: Atlanta, GA, USA, 2004. [Google Scholar]
- Shahnazari, M.; Sharkey, N.A.; Fosmire, G.J.; Leach, R.M. Effects of strontium on bone strength, density, volume, and microarchitecture in laying hens. J. Bone Miner. Res. 2006, 21, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Dawson, E.B.; Frey, M.J.; Moore, T.D.; McGanity, W.J. Relationship of metal metabolism to vascular disease mortality rates in Texas. Am. J. Clin. Nutr. 1978, 31, 1188–1197. [Google Scholar] [PubMed]
- Polyakova, E.V. Strontium in water-supply sources of arkhangelsk region and its impact on human health. Hum. Ecol. 2012, 2, 9–14. [Google Scholar]
- Curzon, M.E. The relation between caries prevalence and strontium concentrations in drinking water, plaque, and surface enamel. J. Dent. Res. 1985, 64, 1386–1388. [Google Scholar] [CrossRef] [PubMed]
- Rygaard, M.; Albrechtsen, H.-J. Redegørelse om Sundhedseffekter af Blødgøring i København Specielt Med Fokus på Caries; Technical University of Denmark (DTU): Kongens Lyngby, Denmark, 2012. (In Danish) [Google Scholar]
- Geological Survey of Denmark and Greenland (GEUS). JUPITER—Danmarks geologiske & hydrologiske database 2011. Available online: http://www.geus.dk/DK/data-maps/jupiter/Sider/default.aspx (accessed on 6 December 2012).
- Danish Nature Agency (DNA). Kvaliteten af Det Danske Drikkevand for Perioden 2008–2010. Available online: http://naturstyrelsen.dk/media/nst/Attachments/Indberetningsrapportdrikkevand20082010.pdf (accessed on 17 February 2015).
- Sørensen, B.L.; Møller, R.R. Evaluation of total groundwater abstraction from public waterworks in Denmark using principal component analysis. Geol. Surv. Den. Greenl. Bull. 2013, 28, 37–40. [Google Scholar]
- Union of European Soft Drinks Associations (UNESDA). Sales Volume Statistics by Industry Analyst “Canadean”. Available online: http://www.unesda.eu/products-ingredients/consumption/ (accessed on 17 February 2015).
- Marcussen, H.; Holm, P.E.; Hansen, H.C.B. Composition, Flavor, Chemical Foodsafety, and Consumer Preferences of Bottled Water. Compr. Rev. Food Sci. Food Saf. 2013, 12, 333–352. [Google Scholar] [CrossRef]
- Danish Nature Agency (DNA). Videregående Vandbehandling; Danish Nature Agency (Naturstyrelsen), Ministry of the Environment (Miljøministeriet): Copenhagen, Denmark, 2012; pp. 1–65. (In Danish) [Google Scholar]
- Voutchkova, D.D.; Hansen, B.; Ernstsen, V.; Kristiansen, S.M. Design of a nationwide drinking-water sampling campaign for assessment of dietary iodine intake and human health outcomes. Technical Note I in PhD thesis [70].
- Schullehner, J.; Hansen, B. Nitrate exposure from drinking water in Denmark over the last 35 years. Environ. Res. Lett. 2014, 9, 095001. [Google Scholar] [CrossRef]
- Thygesen, M. Geocoding of All Danish Addresses from the Residence Database (Version 2). Available online: http://cirrau.au.dk/data-resources/data-documentation/ (accessed on 17 February 2015).
- Pedersen, C.B. The Danish civil registration system. Scand. J. Public Health 2011, 39, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Bivand, R.S.; Pebesma, E.J.; Gómez-Rubio, V. Applied Spatial Data Analysis with R; Springer: Berlin, Germany, 2008. [Google Scholar]
- Waller, L.A.; Gotway, C.A. Applied Spatial Statistics for Public Health Data; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Pfeiffer, D.; Robinson, T.; Stevenson, M.; Stevens, K.B.; Rogers, D.J.; Clements, A.C. Spatial Analysis in Epidemiology; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Kulldorff, M.; Huang, L.; Konty, K. A scan statistic for continuous data based on the normal probability model. Int. J. Health Geogr. 2009, 8. [Google Scholar] [CrossRef]
- Andersen, S.; Lauberg, P. The Nature of Iodine in Drinking Water. In Comprehensive Handbook of Iodine Nutritional, Biochemical, Pathological and Therapeutic Aspects; Preedy, V.R., Burrow, G.N., Watson, R., Eds.; Academic Press: London, UK, 2009; pp. 125–134. [Google Scholar]
- Thygesen, L.C.; Daasnes, C.; Thaulow, I.; Brønnum-Hansen, H. Introduction to Danish (nationwide) registers on health and social issues: Structure, access, legislation, and archiving. Scand. J. Public Health 2011, 39, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Dahl, C.; Søgaard, A.J.; Tell, G.S.; Flaten, T.P.; Hongve, D.; Omsland, T.K.; Holvik, K.; Meyer, H.E.; Aamodt, G. Nationwide data on municipal drinking water and hip fracture: Could calcium and magnesium be protective? A NOREPOS study. Bone 2013, 57, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kirkeskov, L.; Kristiansen, E.; Bøggild, H.; Von Platen-Hallermund, F.; Sckerl, H.; Carlsen, A.; Larsen, M.J.; Poulsen, S. The association between fluoride in drinking water and dental caries in Danish children. Linking data from health registers, environmental registers and administrative registers. Community Dent. Oral Epidemiol. 2010, 38, 206–212. [Google Scholar] [CrossRef] [PubMed]
- GEUS. Interactive Map on Water Hardness as an Average per Municipality. Available online: http://www.geus.dk/DK/data-maps/Sider/haardhedskort-dk.aspx (accessed on 17 February 2015).
- Voutchkova, D.D. Iodine in Danish Groundwater and Drinking Water. Ph.D. Thesis, Aarhus University, Aarhus, Denmark, 2014. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voutchkova, D.D.; Schullehner, J.; Knudsen, N.N.; Jørgensen, L.F.; Ersbøll, A.K.; Kristiansen, S.M.; Hansen, B. Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark. Geosciences 2015, 5, 45-66. https://doi.org/10.3390/geosciences5010045
Voutchkova DD, Schullehner J, Knudsen NN, Jørgensen LF, Ersbøll AK, Kristiansen SM, Hansen B. Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark. Geosciences. 2015; 5(1):45-66. https://doi.org/10.3390/geosciences5010045
Chicago/Turabian StyleVoutchkova, Denitza Dimitrova, Jörg Schullehner, Nikoline Nygård Knudsen, Lisbeth Flindt Jørgensen, Annette Kjær Ersbøll, Søren Munch Kristiansen, and Birgitte Hansen. 2015. "Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark" Geosciences 5, no. 1: 45-66. https://doi.org/10.3390/geosciences5010045
APA StyleVoutchkova, D. D., Schullehner, J., Knudsen, N. N., Jørgensen, L. F., Ersbøll, A. K., Kristiansen, S. M., & Hansen, B. (2015). Exposure to Selected Geogenic Trace Elements (I, Li, and Sr) from Drinking Water in Denmark. Geosciences, 5(1), 45-66. https://doi.org/10.3390/geosciences5010045