
New Insights on the Toxicity on Heart and Vessels of Breast Cancer Therapies

 ,
,
Abstract
:1. Background
1.1. Chemotherapy
1.2. Hormonal Therapy
1.3. Targeted Therapy
2. Methods
3. Chemotherapy Induced Cardiotoxicity
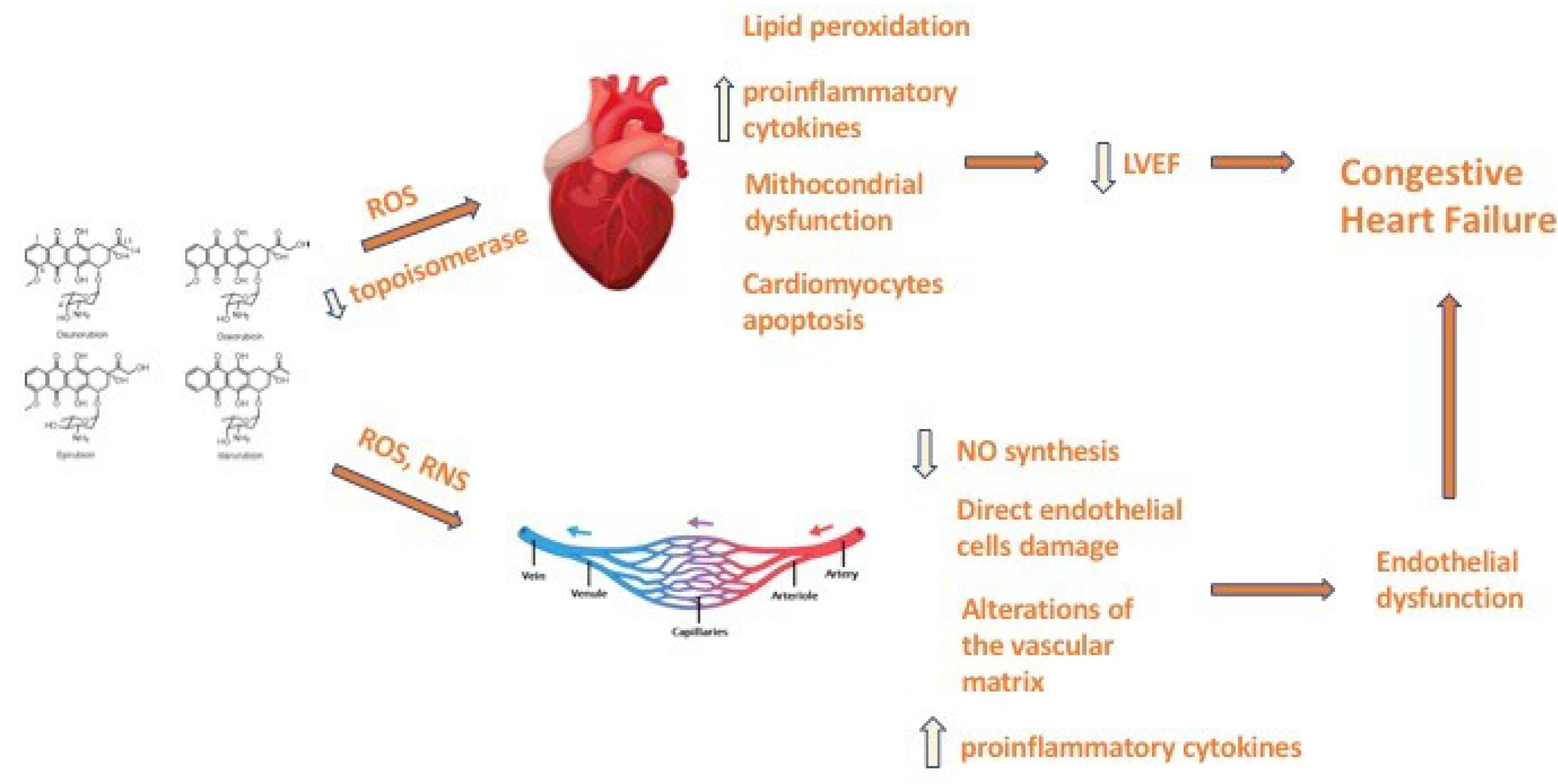
3.1. Anthracyclines
3.2. Taxanes
3.3. Cyclophosphamide
3.4. 5-Fluorouracil
4. Hormonal Therapy
Estrogen Receptor modulators and Aromatase Inhibitors
5. Targeted Therapy
5.1. Immune Checkpoint Inhibitors (ICI)
5.2. HER2 Targeted Therapy
5.3. Cyclin Dependent Kinase 4/6 (CDK 4/6) Inhibitors
6. Radiotherapy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer 2019, 11, 151–164. [Google Scholar] [CrossRef] [Green Version]
- DeSantis, C.E.; Bray, F.; Ferlay, J.; Lortet-Tieulent, J.; Anderson, B.O.; Jemal, A. International Variation in Female Breast Cancer Incidence and Mortality Rates. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1495–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 14 February 2022).
- Rojas, K.; Stuckey, A. Breast Cancer Epidemiology and Risk Factors. Clin. Obstet. Gynecol. 2016, 59, 651–672. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Collins, W.J.; Audeh, M.W.; Shiao, S.L.; Gottlieb, R.A.; Goodman, M.T.; Merz, C.; Mehta, P.K. Breast Cancer Survivorship and Cardiovascular Disease: Emerging Approaches in Cardio-Oncology. Curr. Treat. Options Cardiovasc. Med. 2015, 17, 60. [Google Scholar] [CrossRef]
- Moo, T.A.; Sanford, R.; Dang, C.; Morrow, M. Overview of Breast Cancer Therapy. PET Clin. 2018, 13, 339–354. [Google Scholar] [CrossRef]
- Dunnwald, L.K.; Rossing, M.A.; Li, C.I. Hormone receptor status, tumor characteristics, and prognosis: A prospective cohort of breast cancer patients. Breast Cancer Res. 2007, 9, R6. [Google Scholar] [CrossRef]
- Drăgănescu, M.; Carmocan, C. Hormone Therapy in Breast Cancer. Chirurgia 2017, 112, 413–417. [Google Scholar] [CrossRef]
- Dumbrava, I.; Raghav, K.; Balaji, K.; Bhatt, M.; Murthy, R.K.; Rodon, J.; Sarina, A.; Bernstam, F.M.; Johnson, A.M.; Ecaterina, E.; et al. Advances in HER2-Targeted Therapy: Novel Agents and Opportunities Beyond Breast and Gastric Cancer. Clin. Cancer Res. 2019, 25, 2033–2204. [Google Scholar]
- Spring, L.M.; Wander, S.A.; Zangardi, M.; Bardia, A. CDK 4/6 Inhibitors in Breast Cancer: Current Controversies and Future Directions. Curr. Oncol. Rep. 2019, 21, 25. [Google Scholar] [CrossRef] [PubMed]
- Florescu, D.R.; Nistor, D.E. Therapy-induced cardiotoxicity in breast cancer patients: A well-known yet unresolved problem. Discoveries 2019, 7, e89. [Google Scholar] [CrossRef]
- Alexander, J.; Dainiak, N.; Berger, H.J.; Goldman, L.; Johnstone, D.; Reduto, L.; Duffy, T.; Schwartz, P.; Gottschalk, A.; Zaret, B.L.; et al. Serial assessment of doxorubicin cardiotoxicity with quantitative radionuclide angiocardiography. N. Engl. J. Med. 1979, 300, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Munoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, T.S.; DeCara, J.M. Risk factors for chemotherapy-related cardiac toxicity. Curr. Opin. Cardiol. 2019, 34, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Litvak, A.; Batukbhai, B.; Russell, S.D.; Tsai, H.L.; Rosner, G.L.; Jeter, S.C.; Armstrong, D.; Emens, L.A.; Fetting, J.; Wolff, A.C.; et al. Racial disparities in the rate of cardiotoxicity of HER2-targeted therapies among women with early breast cancer. Cancer 2018, 124, 1904–1911. [Google Scholar] [CrossRef]
- Chang, V.Y.; Wang, J.J. Pharmacogenetics of Chemotherapy-Induced Cardiotoxicity. Curr. Oncol. Rep. 2018, 20, 52. [Google Scholar] [CrossRef]
- Schwartz, R.G.; McKenzie, W.B.; Alexander, J.; Sager, P.; D’Souza, A.; Manatunga, A.; Schwartz, P.E.; Berger, H.J.; Setaro, J.; Surkin, L.; et al. Congestive heart failure and left ventricular dysfunction complicating doxorubicin therapy. Seven-year experience using serial radionuclide angiocardiography. Am. J. Med. 1987, 82, 1109–1118. [Google Scholar] [CrossRef]
- Seidman, A.; Hudis, C.; Pierri, M.K.; Shak, S.; Paton, V.; Ashby, M.; Murphy, M.; Stewart, S.J.; Keefe, D. Cardiac dysfunction in the trastuzumab clinical trials experience. J. Clin. Oncol. 2002, 20, 1215–1221. [Google Scholar] [CrossRef]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. and ESMO Guidelines Committee. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail 2020, 22, 1945–1960. [Google Scholar]
- Fujiwara, A.; Hoshino, T.; Westley, J. Anthracycline Antibiotics. Crit. Rev. Biotechnol. 2008, 3, 133–157. [Google Scholar] [CrossRef]
- Giordano, S.H.; Lin, Y.L.; Kuo, Y.F.; Hortobagyi, G.N.; Goodwin, J.S. Decline in the use of anthracyclines for breast cancer. J. Clin. Oncol. 2012, 30, 2232–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doroshow, J.H. Effect of anthracycline antibiotics on oxygen radical formation in rat heart. Cancer Res. 1983, 43, 460–472. [Google Scholar] [PubMed]
- Menna, P.; Salvatorelli, E.; Giampietro, R.; Liberi, G.; Teodori, G.; Calafiore, A.M.; Minotti, G. Doxorubicin-dependent reduction of ferrylmyoglobin and inhibition of lipid peroxidation: Implications for cardiotoxicity of anticancer anthracyclines. Chem. Res. Toxicol. 2002, 15, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- Nebigil, C.G.; Désaubry, L. Updates in Anthracycline-Mediated Cardiotoxicity. Front Pharm. 2018, 9, 1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.A. Doxorubicin/taxane combinations: Cardiac toxicity and pharmacokinetics. Semin. Oncol. 1999, 26, 14–19. [Google Scholar]
- Mao, Z.; Shen, K.; Zhu, L.; Xu, M.; Yu, F.; Xue, D.; Li, H.; Xue, C. Comparisons of Cardiotoxicity and Efficacy of Anthracycline-Based Therapies in Breast Cancer: A Network Meta-Analysis of Randomized Clinical Trials. Oncol. Res. Treat. 2019, 42, 405–413. [Google Scholar] [CrossRef]
- Schettini, F.; Giuliano, M.; Lambertini, M.; Bartsch, R.; Pinato, D.J.; Onesti, C.E.; Harbeck, N.; Lüftner, D.; Rottey, S.; van Dam, P.A.; et al. Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer. Cancers 2021, 13, 4421. [Google Scholar] [CrossRef]
- Novo, G.; Di Lisi, D.; Manganaro, R.; Manno, G.; Lazzara, S.; Immordino, F.A.; Madaudo, C.; Carerj, S.; Russo, A.; Incorvaia, L.; et al. Arterial Stiffness: Effects of Anticancer Drugs Used for Breast Cancer Women. Front. Physiol. 2021, 12, 661464. [Google Scholar] [CrossRef]
- Duquaine, D.; Hirsch, G.A.; Chakrabarti, A.; Han, Z.; Kehrer, C.; Brook, R.; Joseph, J.; Schott, A.; Kalyanaraman, B.; Vasquez-Vivar, J.; et al. Rapid-onset endothelial dysfunction with adriamycin: Evidence for a dysfunctional nitric oxide synthase. Vasc. Med. 2003, 8, 101–107. [Google Scholar] [CrossRef]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Salvatorelli, E.; Menna, P.; Cascegna, S.; Liberi, G.; Calafiore, A.M.; Gianni, L.; Minotti, G. Paclitaxel and docetaxel stimulation of doxorubicinol formation in the human heart: Implications for cardiotoxicity of doxorubicin-taxane chemotherapies. J. Pharmacol. Exp. Ther. 2006, 318, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Shimoyama, M.; Murata, Y.; Sumi, K.; Hamazoe, R.; Komuro, I. Docetaxel induced cardiotoxicity. Heart 2001, 86, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florescu, M.; Mihalcea, D.; Enescu, O.A.; Radu, E.; Chirca, A.; Acasandrei, A.M.; Magda, L.S.; Rimbas, R.C.; Cirstoiu, C.; Vinereanu, D. Taxanes-induced cardiotoxicity is related to increased arterial stiffness and oxidative stress. Eur. Heart J. 2013, 34, P3006. [Google Scholar] [CrossRef] [Green Version]
- Arbuck, S.G.; Strauss, H.; Rowinsky, E.; Christian, M.; Suffness, M.; Adams, J.; Oakes, M.; McGuire, W.; Reed, E.; Gibbs, H.; et al. A reassessment of cardiac toxicity associated with Taxol. J. Natl. Cancer Inst. Monogr. 1993, 15, 117–130. [Google Scholar]
- Kim, K.J.; Chan, C.J. Cyclophosphamide in dermatology. Australas. J. Dermatol. 2017, 58, 5–17. [Google Scholar] [CrossRef]
- Goldberg, G.M.A.; Antin, A.J.H.; Guinan, G.E.C.; Rappeport, R.J.M. Cyclophosphamide cardiotoxicity: An analysis of dosing as a risk factor. Blood 1986, 68, 1114–1118. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, T.I. Clinical significance of cyclophosphamide-induced cardiotoxicity. Intern. Med. 2005, 44, 89–90. [Google Scholar] [CrossRef] [Green Version]
- Kurauchi, K.K.; Nishikawa, N.T.; Miyahara, M.E.; Okamoto, O.Y.; Kawano, K.Y. Role of metabolites of cyclophosphamide in cardiotoxicity. BMC Res. 2017, 10, 406. [Google Scholar] [CrossRef] [Green Version]
- Kupari, K.M.; Volin, V.L.; Suokas, A.; Timonen, T.; Hekali, P.; Ruutu, T. Cardiac involvement in bone marrow transplantation: Electrocardiographic changes, arrhythmias, heart failure and autopsy findings. Bone Marrow Transpl. 1990, 5, 91–98. [Google Scholar]
- Morandi, M.P.; Ruffini, R.P.A.; Benvenuto, B.G.M.; La Vecchia, L.V.A.; Mezzena, M.G.; Raimondi, R.R. Serum cardiac troponin I levels and ECG/ echo monitoring in breast cancer patients undergoing high- dose (7 g/m2) cyclophosphamide. Bone Marrow Transpl. 2001, 28, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huyan, H.X.; Lin, L.Y.P.; Gao, G.T.; Chen, C.R.Y.; Fan, F.Y.M. Immunosuppressive effect of cyclophosphamide on white blood cells and lymphocyte subpopulations from peripheral blood of Balb/c mice. Int. Immunopharmacol. 2011, 11, 1293–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhesi, D.S.; Chu, C.M.P.; Blevins, B.G.; Paterson, P.I.; Larratt, L.L.; Oudit, O.G.Y.; Kim, K.D.H. Cyclophosphamide-Induced Cardiomyopathy: A Case Report, Review, and Recommendations for Management. J. Investig. Med. High Impact Case Rep. 2013, 1, 2324709613480346. [Google Scholar] [CrossRef] [PubMed]
- Basselin, B.C.; Fontanges, F.T.; Descotes, D.J.; Chevalier, C.P.; Bui-Xuan, B.X.; Feinard, F.G.; Timour, T.Q. 5-Fluorouracil-induced Tako-Tsubo-like syndrome. Pharmacotherapy 2011, 31, 226. [Google Scholar] [CrossRef]
- Polk, P.A.; Vaage-Nilsen, V.N.; Vistisen, V.M.; Nielsen, N.K. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: A systematic review of incidence, manifestations and predisposing factors. Cancer Treat. 2013, 39, 974–984. [Google Scholar] [CrossRef]
- Gradishar, G.W.J.; Vokes, V.E. 5-Fluorouracil cardiotoxicity: A critical review. Ann. Oncol. 1990, 1, 409–414. [Google Scholar] [CrossRef]
- Luwaert, L.R.J.; Descamps, D.O.; Majois, M.F.; Chaudron, C.J.M.; Beauduin, B.M. Coronary artery spasm induced by 5-fluorouracil. Eur. Heart J. 1991, 12, 468–470. [Google Scholar] [CrossRef]
- Stewart, S.T.; Pavlakis, P.N.; Ward, W.N. Cardiotoxicity with 5-fluorouracil and capecitabine: More than just vasospastic angina. Intern. Med. J. 2010, 40, 303–307. [Google Scholar] [CrossRef]
- Çalık, C.A.N.; Çeliker, C.E.; Velibey, V.Y.; Çağdaş, C.M.; Güzelburç, G.O. Initial dose effect of 5-fluorouracil: Rapidly improving severe, acute toxic myopericarditis. Am. J. Emerg. Med. 2012, 30, e1–e3. [Google Scholar] [CrossRef]
- Robben, R.N.C.; Pippas, P.A.W.; Moore, M.J.O. The syndrome of 5-fluorouracil cardiotoxicity. An elusive cardiopathy. Cancer 1993, 71, 493–509. [Google Scholar] [CrossRef]
- Burstein, H.J.; Griggs, J.J.; Prestrud, A.A.; Temin, S. American Society of Clinical Oncology clinical practice guideline: Update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. J. Clin. Oncol. 2010, 28, 3784–3796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, B.; Dignam, J.; Wolmark, N. Five versus more than five years of tamoxifen for lymph node-negative breast cancer: Updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J. Natl. Cancer Inst. 2001, 93, 684–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frasor, J.; Stossi, F.; Danes, J.M.; Komm, B.; Lyttle, C.R.; Katzenellenbogen, B.S. Selective estrogen receptor modulators: Discrimination of agonistic versus antagonistic activities by gene expression profiling in breast cancer cells. Cancer Res. 2004, 64, 1522–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteva, F.J.; Hortobagyi, G.N. Comparative assessment of lipid effects of endocrine therapy for breast cancer: Implications for cardiovascular disease prevention in postmenopausal women. Breast 2006, 15, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Babyshkina, N.; Dronova, T.; Erdyneeva, D.; Gervas, P.; Cherdyntseva, N. Role of TGF-β signaling in the mechanism of tamoxifen resistance. Cyt. Growth Fac. Rev. 2021, 62, 62–69. [Google Scholar] [CrossRef]
- Mosquera, L.; Colón, J.M.; Santiago, J.M.; Torrado, A.I.; Meléndez, M.; Segarra, A.C.; Rodríguez-Orengo, J.F.; Miranda, J.D. Tamoxifen and estradiol improved locomotor function and increased spared tissue in rats after spinal cord injury: Their antioxidant effect and role of estrogen receptor alpha. Brain Res. 2014, 1561, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, H. Tamoxifen as an antioxidant and cardioprotectant. Biochem. Soc. Symp. 1995, 61, 209–219. [Google Scholar]
- Matthews, A.; Stanway, S.; Farmer, R.E.; Strongman, H.; Thomas, S.; Lyon, A.R.; Smeeth, L.; Bhaskaran, K. Long term adjuvant endocrine therapy and risk of cardiovascular disease in female breast cancer survivors: Systematic review. BMJ 2018, 363, k3845. [Google Scholar] [CrossRef] [Green Version]
- Saphner, T.; Tormey, D.C.; Gray, R. Venous and arterial thrombosis in patients who received adjuvant therapy for breast cancer. J. Clin. Oncol. 1991, 9, 286–294. [Google Scholar] [CrossRef]
- Amir, E.; Seruga, B.; Niraula, S.; Carlsson, L.; Ocaña, A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2011, 103, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Grouthier, V.; Lebrun-Vignes, B.; Glazer, A.M.; Touraine, P.; Funck-Brentano, C.; Pariente, A.; Courtillot, C.; Bachelot, A.; Roden, D.M.; Moslehi, J.J.; et al. Increased long QT and torsade de pointes reporting on tamoxifen compared with aromatase inhibitors. Heart 2018, 104, 1859–1863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabian, C.J. The what, why and how of aromatase inhibitors: Hormonal agents for treatment and prevention of breast cancer. Int. J. Clin. Pract. 2007, 61, 2051–2063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khosrow-Khavar, F.; Bouganim, N.; Filion, K.B.; Suissa, S.; Azoulay, L. Cardiotoxicity of Use of Sequential Aromatase Inhibitors in Women with Breast Cancer. Am J Epidemiol. 2020, 189, 1086–1095. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.F.; Cuzick, J.; Buzdar, A.; Howell, A.; Tobias, J.S.; Baum, M. Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trialists’ Group. Effect of anastrozole and tamoxifen as adjuvant treatment for early- stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol. 2008, 9, 45–53. [Google Scholar] [PubMed]
- Coates, A.S.; Keshaviah, A.; Thürlimann, B.; Mouridsen, H.; Mauriac, L.; Forbes, J.F.; Paridaens, R.; Castiglione-Gertsch, M.; Gelber, R.D.; Colleoni, M. Five years of letrozole compared with tamoxifen as initial adjuvant therapy for postmeno- pausal women with endocrine-responsive early breast cancer: Update of study BIG 1-98. J. Clin. Oncol. 2007, 25, 486–492. [Google Scholar] [CrossRef]
- Khosrow-Khavar, F.; Filion, K.B.; Bouganim, N.; Suissa, S.; Azoulay, L. Aromatase Inhibitors and the Risk of Cardiovascular Outcomes in Women with Breast Cancer: A Population-Based Cohort Study. Circulation 2020, 141, 549–559. [Google Scholar] [CrossRef]
- Khosrow-Khavar, F.; Filion, K.B.; Al-Qurashi, S.; Torabi, N.; Bouganim, N.; Suissa, S.; Azoulay, L. Cardiotoxicity of aromatase inhibitors and tamoxifen in postmenopausal women with breast cancer: A systematic review and meta-analysis of randomized controlled trials. Ann. Oncol. 2017, 28, 487–496. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Amir, E.; Fischer, H.D.; Fu, L.; Austin, P.C.; Harvey, P.J.; Rochon, P.A.; Lee, D.S.; Anderson, G.M. The risk of myocardial infarction with aromatase inhibitors relative to tamoxifen in post-menopausal women with early stage breast cancer. Eur. J. Cancer 2016, 68, 11–21. [Google Scholar] [CrossRef]
- Tsai, H.F.; Hsu, P.N. Cancer immunotherapy by targeting immune checkpoints: Mechanism of T cell dysfunction in cancer immunity and new therapeutic targets. J. Biomed. Sci. 2017, 24, 35. [Google Scholar] [CrossRef]
- Kwapisz, D. Pembrolizumab and atezolizumab in triple-negative breast cancer. Cancer Immunol. Immunother. 2021, 70, 607–617. [Google Scholar] [CrossRef]
- Schütz, F.; Stefanovic, S.; Mayer, L.; von Au, A.; Domschke, C.; Sohn, C. PD-1/PD-L1 Pathway in Breast Cancer. Oncol. Res. Treat. 2017, 40, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.E.; Tolaney, S.M. Role of Immunotherapy in Triple-Negative Breast Cancer. J. Natl. Compr. Canc. Netw. 2020, 18, 479–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, S.; Ghosh, R.K.; Wongsaengsak, S.; Bandyopadhyay, D.; Ghosh, G.C.; Aronow, W.S.; Fonarow, G.C.; Lenihan, D.J.; Bhatt, D.L. Cardiovascular Toxicities of Immune Checkpoint Inhibitors: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1714–1727. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.; Cronin, K.A. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl. Cancer Inst. 2014, 106, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Pegram, M.D.; Lipton, A.; Hayes, D.F.; Weber, B.L.; Baselga, J.M.; Tripathy, D.; Baly, D.; Baughman, S.A.; Twaddell, T.; Glaspy, J.A.; et al. Phase II study of receptor-enhanced chemosensitivity using recombinant humanized anti-p185HER2/neu monoclonal antibody plus cisplatin in patients with HER2/neu-overexpressing metastatic breast cancer refractory to chemotherapy treatment. J. Clin. Oncol. 1998, 16, 2659–2671. [Google Scholar] [CrossRef]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Maadi, H.; Soheilifar, M.H.; Choi, W.S.; Moshtaghian, A.; Wang, Z. Trastuzumab Mechanism of Action; 20 Years of Research to Unravel a Dilemma. Cancers 2021, 13, 3540. [Google Scholar] [CrossRef]
- Yu, X.; Wang, L.; Shen, Y.; Wang, C.; Zhang, Y.; Meng, Y.; Yang, Y.; Liang, B.; Zhou, B.; Wang, H.; et al. Targeting EGFR/HER2 heterodimerization with a novel anti-HER2 domain II/III antibody. Mol. Immunol 2017, 87, 300–307. [Google Scholar] [CrossRef]
- Korzeniecki, C.; Priefer, R. Targeting KRAS mutant cancers by preventing signaling transduction in the MAPK pathway. Eur. J. Med. Chem 2021, 211, 113006. [Google Scholar] [CrossRef]
- Ruiz-Saenz, A.; Dreyer, C.; Campbell, M.R.; Steri, V.; Gulizia, N.; Moasser, M.M. HER2 Amplification in Tumors Activates PI3K/Akt Signaling Independent of HER3. Cancer Res. 2018, 78, 3645–3658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, X.F.; Claret, F.X.; Lammayot, A.; Tian, L.; Deshpande, D.; LaPushin, R.; Tari, A.M.; Bast, R.C. The Role of Cyclin-dependent Kinase Inhibitor p27Kip1 in Anti-HER2 Antibody-induced G1 Cell Cycle Arrest and Tumor Growth Inhibition. J. Biol. Chem. 2003, 278, 23441–23450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijsen, M.; King, P.; Perera, T.; Parker, P.J.; Harris, A.L.; Larijani, B.; Kong, A. HER2 Phosphorylation Is Maintained by a PKB Negative Feedback Loop in Response to Anti-HER2 Herceptin in Breast Cancer. PLoS Biol. 2010, 8, e1000563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Song, J.; Park, S.; Ham, S.; Paek, K.; Kang, M.; Chae, Y.; Seo, H.; Kim, H.C.; Flores, M. Drifts in ADCC-related quality attributes of Herceptin®: Impact on development of a trastuzumab biosimilar. MAbs 2017, 9, 704–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suter, T.M.; Procter, M.; van Veldhuisen, D.J.; Muscholl, M.; Bergh, J.; Carlomagno, C.; Perren, T.; Passalacqua, R.; Bighin, C.; Klijn, J.G.; et al. Trastuzumab-associated cardiac adverse effects in the Herceptin adjuvant trial. J. Clin. Oncol. 2007, 25, 3859–3865. [Google Scholar] [CrossRef] [PubMed]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef] [Green Version]
- Chavez-MacGregor, M.; Zhang, N.; Buchholz, T.A.; Zhang, Y.; Niu, J.; Elting, L.; Smith, B.D.; Hortobagyi, G.N.; Giordano, S.H. Trastuzumab-related cardiotoxicity among older patients with breast cancer. J. Clin. Oncol. 2013, 31, 4222–4228. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Romond, E.H.; Jeong, J.H.; Rastogi, P.; Swain, S.M.; Geyer, C.E.; Ewer, M.S., Jr.; Rathi, V.; Fehrenbacher, L.; Brufsky, A.; Azar, C.A.; et al. Seven-year follow-up assessment of cardiac function in NSABP B-31, a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel (ACP) with ACP plus trastuzumab as adjuvant therapy for patients with node-positive, human epidermal growth factor receptor 2-positive breast cancer. J. Clin. Onc. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 3792–3799. [Google Scholar]
- Yu, A.F.; Moskowitz, C.S.; Chuy, K.L.; Yang, J.; Dang, C.T.; Liu, J.E.; Oeffinger, K.C.; Steingart, R.M. Cardiotoxicity Surveillance and Risk of Heart Failure During HER2 Targeted Therapy. JACC Cardio. Oncol. 2020, 2, 166–175. [Google Scholar] [CrossRef]
- Battisti, N.; Andres, M.S.; Lee, K.A.; Ramalingam, S.; Nash, T.; Mappouridou, S.; Senthivel, N.; Asavisanu, K.; Obeid, M.; Tripodaki, E.S.; et al. Incidence of cardiotoxicity and validation of the Heart Failure Association-International Cardio-Oncology Society risk stratification tool in patients treated with trastuzumab for HER2-positive early breast cancer. Breast Cancer Res. Treat. 2021, 18, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, B.T.; Varga, Z.V.; Wu, W.J.; Pacher, P. Trastuzumab cardiotoxicity: From clinical trials to experimental studies. Br. J. Pharmacol. 2017, 174, 3727–3748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, V.S.; Lenihan, D.J.; Ky, B. Cancer therapy-induced cardiotoxicity: Basic mechanisms and potential cardioprotective therapies. J. Am. Heart Assoc. 2014, 3, e000665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portera, C.C.; Walshe, J.M.; Rosing, D.R.; Denduluri, N.; Berman, A.W.; Vatas, U.; Velarde, M.; Chow, C.K.; Steinberg, S.M.; Nguyen, D. Cardiac toxicity and efficacy of trastuzumab combined with pertuzumab in patients with [corrected] human epidermal growth factor receptor 2-positive metastatic breast cancer. Clin. Cancer. Res. 2008, 14, 2710–2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, V.U.; Reeves, D.J.; Chugh, A.R.; O’Quinn, R.; Fradley, M.G.; Raghavendra, M.; Dent, S.; Barac, A.; Lenihan, D. Clinical Approach to Cardiovascular Toxicity of Oral Antineoplastic Agents: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 2693–2716. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Torrisi, R.; Sandri, M.T.; Civelli, M.; Salvatici, M.; Lamantia, G.; Colombo, N.; Cortinovis, S.; Dessanai, M.A. Trastuzumab-induced cardiotoxicity: Clinical and prognostic implications of troponin I evaluation. J. Clin. Oncol. 2010, 28, 3910–3916. [Google Scholar] [CrossRef]
- Dobson, R.; Ghosh, A.K.; Ky, B.; Marwick, T.; Stout, M.; Harkness, A.; Steeds, R.; Robinson, S.; Oxborough, D.; Adlam, D.; et al. British Society of Echocardiography (BSE) and the British Society of Cardio-Oncology (BCOS) (2021). BSE and BCOS Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab. JACC. Cardio. Oncol. 2021, 3, 1–16. [Google Scholar] [CrossRef]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail 2020, 22, 1504–1524. [Google Scholar]
- Pituskin, E.; Mackey, J.R.; Koshman, S.; Jassal, D.; Pitz, M.; Haykowsky, M.J.; Pagano, J.J.; Chow, K.; Thompson, R.B.; Vos, L.J. Multidisciplinary Approach to Novel Therapies in Cardio-Oncology Research (MANTICORE 101-Breast): A Randomized Trial for the Prevention of Trastuzumab-Associated Cardiotoxicity. J. Clin. Oncol. 2017, 35, 870–877. [Google Scholar] [CrossRef]
- Guglin, M.; Krischer, J.; Tamura, R.; Fink, A.; Bello-Matricaria, L.; McCaskill-Stevens, W.; Munster, P.N. Randomized Trial of Lisinopril Versus Carvedilol to Prevent Trastuzumab Cardiotoxicity in Patients with Breast Cancer. J. Am. Coll. Cardiol. 2019, 73, 2859–2868. [Google Scholar] [CrossRef]
- Lynce, F.; Barac, A.; Geng, X.; Dang, C.; Yu, A.F.; Smith, K.L.; Gallagher, C.; Pohlmann, P.R.; Nunes, R.; Herbolsheimer, P.; et al. Prospective evaluation of the cardiac safety of HER2-targeted therapies in patients with HER2-positive breast cancer and compromised heart function: The SAFE-HEaRt study. Breast Cancer Res. Treat. 2019, 175, 595–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewer, M.S.; Vooletich, M.T.; Durand, J.B.; Woods, M.L.; Davis, J.R.; Valero, V.; Lenihan, D.J. Reversibility of trastuzumab-related cardiotoxicity: New in- sights based on clinical course and response to medical treatment. J. Clin. Oncol. 2005, 23, 7820–7826. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.E.; Kim, S.B.; Martin, A.G.; LoRusso, P.M.; Ferrero, J.M.; Badovinac-Crnjevic, T.; Hoersch, S.; Smitt, M.; Wildiers, H. Trastuzumab emtansine versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): Final overall survival results from a randomised open-label phase 3 trial. Lancet Oncol. 2017, 18, 743–754. [Google Scholar] [CrossRef]
- Perez, E.A.; Barrios, C.; Eiermann, W.; Toi, M.; Im, Y.H.; Conte, P.; Martin, M.; Pienkowski, T.; Pivot, X.B.; Burris, H.A.; et al. Trastuzumab emtansine with or without pertuzumab versus trastuzumab with taxane for human epidermal growth factor receptor 2-positive advanced breast cancer: Final results from MARIANNE. Cancer 2019, 125, 3974–3984. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Eng. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- Swain, S.M.; Baselga, J.; Kim, S.B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Heeson, S.; et al. CLEOPATRA Study Group. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Eng. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef] [Green Version]
- von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E.; et al. APHINITY Steering Committee and Investigators Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer. N. Eng. J. Med. 2017, 377, 122–131. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.; Holmes, E.; Baselga, J.; de Azambuja, E.; Dueck, A.C.; Viale, G.; Zujewski, J.A.; Goldhirsch, A.; Armour, A.; Pritchard, K.I.; et al. Adjuvant Lapatinib and Trastuzumab for Early Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer: Results from the Randomized Phase III Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1034–1042. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.; Delaloge, S.; Holmes, F.A.; Moy, B.; Iwata, H.; Harvey, V.J.; Robert, N.J.; Silovski, T.; Gokmen, E.; von Minckwitz, G.; et al. Neratinib after trastuzumab-based adju- vant therapy in patients with HER2-positive breast cancer (ExteNET): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016, 17, 367–377. [Google Scholar] [CrossRef]
- Choi, Y.J.; Anders, L. Signaling through cyclin D-dependent kinases. Oncogene 2014, 33, 1890–1903. [Google Scholar] [CrossRef] [Green Version]
- Dickson, M.A. Molecular pathways: CDK4 inhibitors for cancer therapy. Clin. Cancer Res. 2014, 20, 3379–3383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spring, L.M.; Zangardi, M.L.; Moy, B.; Bardia, A. Clinical Management of Potential Toxicities and Drug Interactions Related to Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: Practical Considerations and Recommendations. Oncol. 2017, 22, 1039–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, N.C.; Ro, J.; André, F.; Loi, S.; Verma, S.; Iwata, H.; Harbeck, N.; Loibl, S.; Huang Bartlett, C.; Zhang, K. PALOMA3 Study Group Palbociclib in hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 2015, 373, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sledge, G.W.; Toi, M., Jr.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. MONARCH 2: Abemaciclib in combination with fulvestrant in patients with HR1/HER2- advanced breast cancer who progressed on endocrine therapy. J. Clin. Oncol. 2017, 35, 1000. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Jerusalem, G.; De Laurentiis, M.; Im, S.; Petrakova, K.; Valeria Bianchi, G.; Martín, M.; Nusch, A.; et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: Updated overall survival. Ann. Oncol. Eur. Soc. Med. Oncol. 2021, 32, 1015–1024. [Google Scholar] [CrossRef]
- Vidula, N.; Rugo, H.S. Cyclin-dependent kinase 4/6 inhibitors for the treatment of breast cancer: A review of preclinical and clinical data. Clin. Breast Cancer 2016, 16, 8–17. [Google Scholar] [CrossRef]
- Beachler, D.C.; de Luise, C.; Jamal-Allial, A.; Yin, R.; Taylor, D.H.; Suzuki, A.; Lewis, J.H.; Freston, J.W.; Lanes, S. Real-world safety of palbociclib in breast cancer patients in the United States: A new user cohort study. BMC Cancer 2021, 21, 97. [Google Scholar] [CrossRef]
- Infante, J.R.; Cassier, P.A.; Gerecitano, J.F.; Witteveen, P.O.; Chugh, R.; Ribrag, V.; Chakraborty, A.; Matano, A.; Dobson, J.R.; Crystal, A.S.; et al. A Phase I Study of the Cyclin-Dependent Kinase 4/6 Inhibitor Ribociclib (LEE011) in Patients with Advanced Solid Tumors and Lymphomas. Clin. Cancer Res. Off. J. Am. Ass Cancer Res 2016, 22, 5696–5705. [Google Scholar] [CrossRef] [Green Version]
- Barroso-Sousa, R.; Shapiro, G.I.; Tolaney, S.M. Clinical Development of the CDK4/6 Inhibitors Ribociclib and Abemaciclib in Breast Cancer. Breast Care 2016, 11, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Bellet, M.; Ahmad, F.; Villanueva, R.; Valdivia, C.; Palomino-Doza, J.; Ruiz, A.; Gonzàlez, X.; Adrover, E.; Azaro, A.; Valls-Margarit, M.; et al. Palbociclib and ribociclib in breast cancer: Consensus workshop on the management of concomitant medication. Ther. Adv. Med. Oncol. 2019, 11, 1758835919833867. [Google Scholar] [CrossRef]
- Lewis, G.D.; Farach, A. Cardiovascular Toxicities of Radiation Therapy. Methodist. Debakey Cardiovasc. J. 2019, 15, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Holley, A.K.; Miao, L.; St. Clair, D.K.; St. Clair, W.H. Redox-modulated phenomena and radiation therapy: The central role of superoxide dismutases. Antioxid. Redox Signal. 2014, 20, 1567–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvester, C.B.; Abe, J.I.; Patel, Z.S.; Grande-Allen, K.J. Radiation- induced cardiovascular disease: Mechanisms and importance of linear energy transfer. Front. Cardiovasc. Med. 2018, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.M.; Nagalla, S. Hypercoagulable workup in thrombotic cardiovascular diseases. Circulation 2018, 138, 229–231. [Google Scholar] [CrossRef]
- Aronson, D.; Brenner, B. Arterial thrombosis and cancer. Thromb. Res. 2018, 164, S23–S28. [Google Scholar] [CrossRef]
- Pelliccia, F.; Pasceri, V.; Tanzilli, G.; Speciale, G.; Camici, P.G.; Gaudio, C. Malignancy in patients with myocardial infarction and non-obstructive coronary arteries: A systematic review and meta-regression. Eur. J. Intern. Med. 2020, 81, 38–43. [Google Scholar] [CrossRef]


{kind=link}
| Definition | Modality of Evaluation | Chemotherapy Agents | |
|---|---|---|---|
| Alexander et al. [12] | Mild: decline in LVEF > 10%. Moderate: decline in LVEF > 15% to final LVEF < 45% Severe: symptoms of congestive HF | MUGA scan | Anthracycline |
| Schwartz et al. [17] | Decline in LVEF > 10% to final LVEF < 50% | MUGA scan | Anthracycline |
| Seidman et al. [18] | 1. Cardiomyopathy characterized by a decrease in LVEF globally or more severe in the septum 2. Sign and symptoms of HF 3. Decline of LVEF ≥ 5% to final EF < 55% with symptoms of congestive HF 4. Asymptomatic decline of LVEF ≥ 10% to final EF < 55% | Echocardiogram and MUGA scan | Trastuzumab +/− Anthracycline |
| Zamorano et al. [13] | 1. Decline in LVEF >10% to a value < 50% 2. GLS > 15% relative percentage reduction | Two-dimensional (2D) and three-dimensional (3D) contrast echocardiography, cardiac magnetic resonance imaging, MUGA scan | N/A |
| Curigliano, G et al. [19] | Reduction in LVEF of 10%, especially if the number is below LVEF < 50% | Two-dimensional (2D) and three-dimensional (3D) contrast echocardiography, cardiac magnetic resonance imaging, MUGA scan | N/A |
| Risk Factors | Risk Level |
|---|---|
| Congestive heart failure | Very High |
| Ischemic cardiomyopathy | High |
| LVEF reduction | High |
| Elevated baseline troponin | High |
| Previous anthracycline treatment | High |
| Prior radiotherapy to left chest or mediastinum | High |
| Elevated baseline BNP or NT-proBNP | High |
| Age ≥ 80 years | High |
| Age 65–79 years | Medium |
| Baseline LVEF 50–54% | Medium |
| Hypertension | Medium |
| Diabetes | Medium |
| Chronic kidney disease | Medium |
| Previous nonanthracycline-based chemotherapy | Medium |
| Current smoker or smoking history | Medium |
| Obesity | Medium |
| Anti-HER2 Agents/Tyrosine Kinase Inhibitor | Risk Factors |
|---|---|
| Age (>65 years) BMI > 30 kg/m2 Arterial Hypertension Left Ventricular Dysfunction (LVEF < 50%) Previous or roncomitant anthracycline treatment Previous Radiation Therapy (Left chest or Mediastinum) Heart Failure or Cardiomyopathy History of CAD (previous MI, CABG or coronary revascularization) Valvular Heart Disease Arrhythmia Elevated Cardiac Biomarkers (NT-pro-BNP, BNP, Troponin) |
| Anthracycline | Incidence of LV Dysfunction (%) |
|---|---|
| Doxorubicin 400 mg/m2 | 3–5 |
| Doxorubicin 550 mg/m2 | 7–26 |
| Doxorubicin 700 mg/m2 | 18–48 |
| Epirubicin > 900 mg/m2 | 0.9–11.4 |
| Liposomal anthracyclines > 900 mg/m2 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanza, O.; Ferrera, A.; Reale, S.; Solfanelli, G.; Petrungaro, M.; Tini Melato, G.; Volpe, M.; Battistoni, A. New Insights on the Toxicity on Heart and Vessels of Breast Cancer Therapies. Med. Sci. 2022, 10, 27. https://doi.org/10.3390/medsci10020027
Lanza O, Ferrera A, Reale S, Solfanelli G, Petrungaro M, Tini Melato G, Volpe M, Battistoni A. New Insights on the Toxicity on Heart and Vessels of Breast Cancer Therapies. Medical Sciences. 2022; 10(2):27. https://doi.org/10.3390/medsci10020027
Chicago/Turabian StyleLanza, Oreste, Armando Ferrera, Simone Reale, Giorgio Solfanelli, Mattia Petrungaro, Giacomo Tini Melato, Massimo Volpe, and Allegra Battistoni. 2022. "New Insights on the Toxicity on Heart and Vessels of Breast Cancer Therapies" Medical Sciences 10, no. 2: 27. https://doi.org/10.3390/medsci10020027