
Association of Mediterranean Diet Adherence with Disease Progression Characteristics, Lifestyle Factors and Overall Survival in Gastric Cancer Patients

 ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Questionnaire and Lifestyle Factor Evaluations
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Study Population
3.2. Associations of Mediterranean Diet (MD) Compliance with Disease Progression and Lifestyle Factors of Gastric Patients’ Characteristics
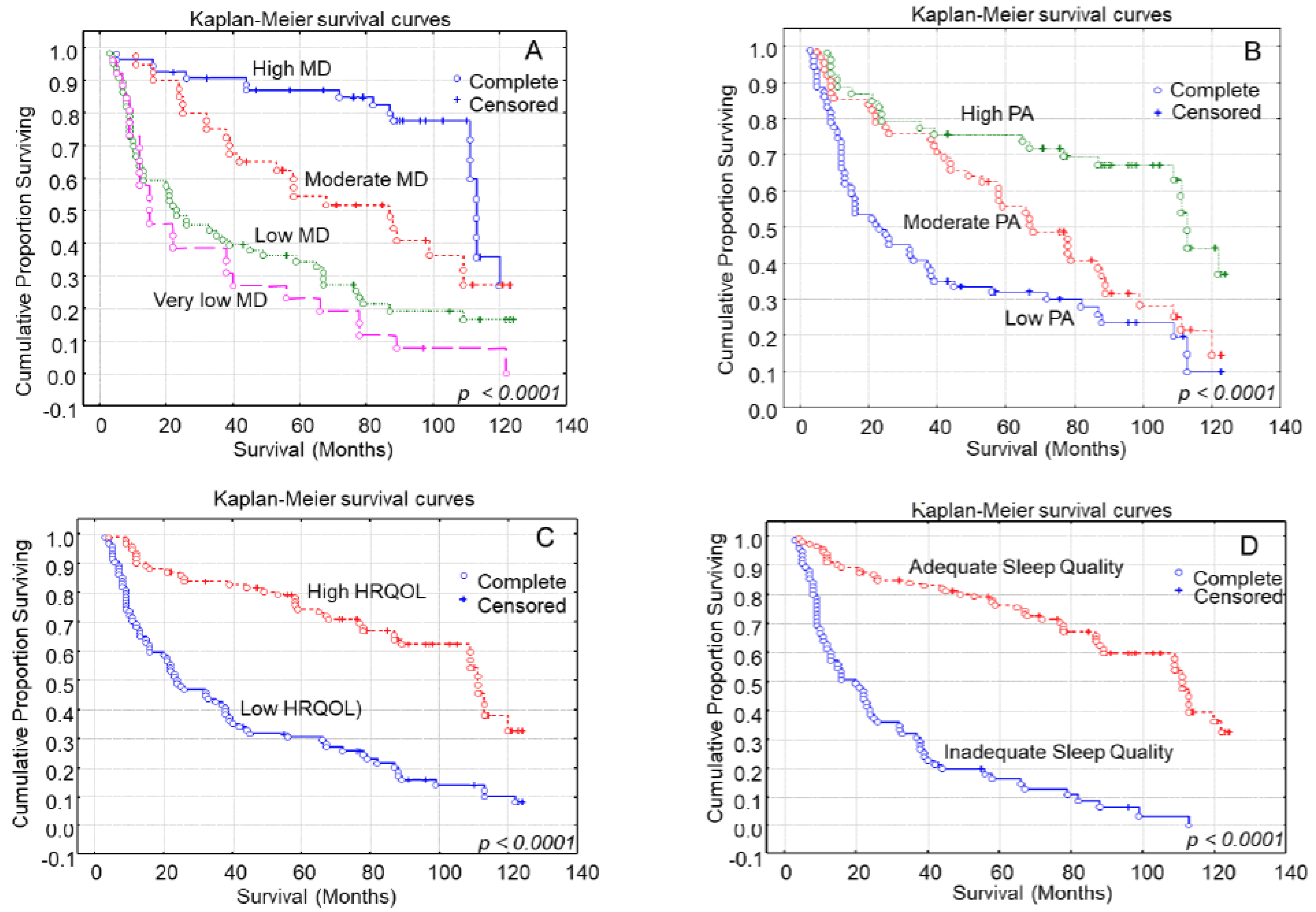
3.3. Kaplan–Meier Analysis for Patients’ Overall Survival
3.4. Multivariate Analysis of MD Adherence with Patients’ Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Álvarez, L.; Vitelli-Storelli, F.; Rubín-García, M.; Aragonés, N.; Ardanaz, E.; Castaño-Vinyals, G.; Obón-Santacana, M.; Dierssen-Sotos, T.; Salas-Trejo, D.; Tardón, A.; et al. Relationship between the Risk of Gastric Cancer and Adherence to the Mediterranean Diet According to Different Estimators. MCC—Spain Study. Cancers 2021, 13, 5281. [Google Scholar] [CrossRef] [PubMed]
- Barekzai, A.M.; Aminianfar, A.; Mousavi, S.M.; Esmaillzadeh, A. The Association between Dietary Inflammatory Potential and Gastric Cancer: A Case Control Study. Nutr. Cancer 2022, 74, 463–471. [Google Scholar] [CrossRef]
- Poorolajal, J.; Moradi, L.; Mohammadi, Y.; Cheraghi, Z.; Gohari-Ensaf, F. Risk factors for stomach cancer: A systematic review and meta-analysis. Epidemiol. Health 2020, 42, e2020004. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Alfano, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Burger, R.A.; Chlebowski, R.T.; Fabian, C.J.; Gucalp, A.; Hershman, D.L.; Hudson, M.M.; et al. American Society of Clinical Oncology position statement on obesity and cancer. J. Clin. Oncol. 2014, 32, 3568–3574. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef]
- Hu, B.; El Hajj, N.; Sittler, S.; Lammert, N.; Barnes, R.; Meloni-Ehrig, A. Gastric cancer: Classification, histology and application of molecular pathology. J. Gastrointest Oncol. 2012, 3, 251–261. [Google Scholar] [CrossRef]
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Bouras, E.; Tsilidis, K.K.; Triggi, M.; Siargkas, A.; Chourdakis, M.; Haidich, A.B. Diet and Risk of Gastric Cancer: An Umbrella Review. Nutrients 2022, 14, 1764. [Google Scholar] [CrossRef]
- Castelló, A.; Fernández de Larrea, N.; Martín, V.; Dávila-Batista, V.; Boldo, E.; Guevara, M.; Moreno, V.; Castaño-Vinyals, G.; Gómez-Acebo, I.; Fernández-Tardón, G.; et al. High adherence to the Western, Prudent, and Mediterranean dietary patterns and risk of gastric adenocarcinoma: MCC-Spain study. Gastric Cancer 2018, 21, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Qu, J.; Liang, X.; Wang, M.; Yin, J.; Qu, J.; Liang, X.; Wang, M. Prognostic significance of controlling nutritional status score for patients with gastric cancer: A systematic review and meta-analysis. Exp. Ther. Med. 2023, 25, 202. [Google Scholar] [CrossRef] [PubMed]
- Tayyem, R.; Al-Awwad, N.; Allehdan, S.; Ajeen, R.; Al-Jaberi, T.; Rayyan, Y.; Bawadi, H.; Hushki, A. Mediterranean Dietary Pattern is Associated with Lower Odds of Gastric Cancer: A Case-Control Study. Cancer Manag. Res. 2022, 14, 2017–2029. [Google Scholar] [CrossRef] [PubMed]
- Yusefi, A.R.; Lankarani, K.Β.; Bastani, P.; Radinmanesh, M.; Kavosi, Z. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Rosania, R.; Chiapponi, C.; Malfertheiner, P.; Venerito, M. Nutrition in Patients with Gastric Cancer: An Update. Gastrointest. Tumors 2016, 2, 178–187. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, Nutrients, and Dietary Patterns: Interconnections and Implications for Dietary Guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, Q.; Guo, H.; Wang, N.; Fan, X.; Zhang, B.; Zhang, W.; Wang, W.; Fang, Z.; Wu, J. Dietary patterns and risk for gastric cancer: A case-control study in residents of the Huaihe River Basin, China. Front. Nutr. 2023, 10, 1118113. [Google Scholar] [CrossRef]
- Rinninella, E.; Mele, M.C.; Cintoni, M.; Raoul, P.; Ianiro, G.; Salerno, L.; Pozzo, C.; Bria, E.; Muscaritoli, M.; Molfino, A.; et al. The Facts about Food after Cancer Diagnosis: A Systematic Review of Prospective Cohort Studies. Nutrients 2020, 12, 2345. [Google Scholar] [CrossRef]
- Maddineni, G.; Xie, J.J.; Brahmbhatt, B.; Mutha, P. Diet and carcinogenesis of gastric cancer. Curr. Opin. Gastroenterol. 2022, 38, 588–591. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef]
- Amiry, F.; Mousavi, S.M.; Barekzai, A.M.; Esmaillzadeh, A. Adherence to the Mediterranean Diet in Relation to Gastric Cancer in Afghanistan. Front. Nutr. 2022, 9, 830646. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef] [PubMed]
- Barile, J.P.; Horner-Johnson, W.; Krahn, G.; Zack, M.; Miranda, D.; De Michele, K.; Ford, D.; Thompson, W.W. Measurement characteristics for two health-related quality of life measures in older adults: The SF-36 and the CDC Healthy Days items. Disabil. Health J. 2016, 9, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Salahuddin, M.; Maru, T.T.; Kumalo, A.; Pandi-Perumal, S.R.; Bahammam, A.S.; Manzar, M.D. Validation of the Pittsburgh sleep quality index in community dwelling Ethiopian adults. Health Qual. Life Outcomes 2017, 15, 58. [Google Scholar] [CrossRef]
- Wang, Y.-P.; Gorenstein, C. Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Rev. Bras. Psiquiatr. 2013, 35, 416–431. [Google Scholar] [CrossRef]
- Tluczek, A.; Henriques, J.B.; Brown, R.L. Support for the reliability and validity of a six-item state anxiety scale derived from the State-Trait Anxiety Inventory. J. Nurs. Meas. 2009, 17, 19–28. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef]
- Mantzorou, M.; Tolia, M.; Poultsidi, A.; Vasios, G.K.; Papandreou, D.; Theocharis, S.; Kavantzas, N.; Troumbis, A.Y.; Giaginis, C. Adherence to Mediterranean Diet and Nutritional Status in Women with Breast Cancer: What Is Their Impact on Disease Progression and Recurrence-Free Patients’ Survival? Curr. Oncol. 2022, 2, 7482–7497. [Google Scholar] [CrossRef]
- Mizukami, T.; Piao, Y. Role of nutritional care and general guidance for patients with advanced or metastatic gastric cancer. Future Oncol. 2021, 17, 3101–3109. [Google Scholar] [CrossRef]
- Xu, R.; Chen, X.D.; Ding, Z. Perioperative nutrition management for gastric cancer. Nutrition 2022, 93, 111492. [Google Scholar] [CrossRef] [PubMed]
- Praud, D.; Bertuccio, P.; Bosetti, C.; Turati, F.; Ferraroni, M.; La Vecchia, C. Adherence to the Mediterranean diet and gastric cancer risk in Italy. Int. J. Cancer 2014, 134, 2935–2941. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.N.; Sageena, G. Dietary factors associated with gastric cancer—A review. Transl. Med. Commun. 2022, 7, 7. [Google Scholar] [CrossRef]
- Van den Brandt, P.A. The impact of a healthy lifestyle on the risk of esophageal and gastric cancer subtypes. Eur. J. Epidemiol. 2022, 3, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.; Zhou, Y.X.; Jin, Y.; Wang, Z.X.; Wei, X.L.; Han, H.Y.; Ye, W.F.; Zhou, Z.W.; Zhang, D.S.; Wang, F.H.; et al. Nutrition support can bring survival benefit to high nutrition risk gastric cancer patients who received chemotherapy. Support Care Cancer 2015, 23, 1933–1939. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of me-ta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 7, 30–43. [Google Scholar] [CrossRef]
- Kyriacou, A.; Evans, J.M.; Economides, N.; Kyriacou, A. Adherence to the Mediterranean diet by the Greek and Cypriot population: A systematic review. Eur. J. Public Health 2015, 25, 1012–1018. [Google Scholar] [CrossRef]
- Castro-Espin, C.; Agudo, A. The Role of Diet in Prognosis among Cancer Survivors: A Systematic Review and Meta-Analysis of Dietary Patterns and Diet Interventions. Nutrients 2022, 14, 348. [Google Scholar] [CrossRef]
- Steck, S.E.; Murphy, E.A. Dietary patterns and cancer risk. Nat. Rev. Cancer 2020, 20, 125–138. [Google Scholar] [CrossRef]
- Shin, J.; Shin, D.W.; Lee, J.; Hwang, J.; Lee, J.E.; Cho, B.; Song, Y.M. Exploring socio-demographic, physical, psychological, and quality of life-related factors related with fear of cancer recurrence in stomach cancer survivors: A cross-sectional study. BMC Cancer 2022, 2, 414. [Google Scholar] [CrossRef]
- Vajdi, M.; Farhangi, M.A. A systematic review of the association between dietary patterns and health-related quality of life. Health Qual. Life Outcomes 2020, 18, 337. [Google Scholar] [CrossRef] [PubMed]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1151–1176. [Google Scholar] [CrossRef] [PubMed]
- Sachlova, M.; Majek, O.; Tucek, S. Prognostic value of scores based on malnutrition or systemic inflammatory response in patients with metastatic or recurrent gastric cancer. Nutr. Cancer 2014, 66, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Eo, W.K.; Chang, H.J.; Suh, J.; Ahn, J.; Shin, J.; Hur, J.Y.; Kim, G.Y.; Lee, S.; Park, S.; Lee, S. The Prognostic Nutritional Index Predicts Survival and Identifies Aggressiveness of Gastric Cancer. Nutr. Cancer 2015, 67, 1260–1267. [Google Scholar] [CrossRef]
- Pano, O.; Gamba, M.; Bullón-Vela, V.; Aguilera-Buenosvinos, I.; Roa-Díaz, Z.M.; Minder, B.; Kopp-Heim, D.; Laine, J.E.; Martínez-González, M.Á.; Martinez, A.; et al. Eating behaviors and health-related quality of life: A scoping review. Maturitas 2022, 165, 58–71. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Behbahani, H.B.; Borazjani, F.; Sheikhi, L.; Amiri, R.; Angali, K.A.; Nejad, S.B.; Samadani, M. The Association between Diet Quality Scores with Sleep Quality among Employees: A Cross-Sectional Study. Ethiop. J. Health Sci. 2022, 32, 145–154. [Google Scholar]
- Scoditti, E.; Tumolo, M.R.; Garbarino, S. Mediterranean Diet on Sleep: A Health Alliance. Nutrients 2022, 14, 2998. [Google Scholar] [CrossRef]
- Bamia, C. Dietary patterns in association to cancer incidence and survival: Concept, current evidence, and suggestions for future research. Eur. J. Clin. Nutr. 2018, 72, 818–825. [Google Scholar] [CrossRef]
- Kwon, S.; Kim, J.; Kim, T.; Jeong, W.; Park, E.C. Association between gastric cancer and the risk of depression among South Korean adults. BMC Psychiatry 2022, 22, 207. [Google Scholar] [CrossRef]
- Yu, H.; Wang, Y.; Ge, X.; Wu, X.; Mao, X. Depression and survival in Chinese patients with gastric cancer: A prospective study. Asian Pac. J. Cancer Prev. 2012, 13, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Wu, J.; Zheng, S.; Sun, H.; Fang, Y.; Huang, Z.; Shi, M.; Liang, L.; Bin, J.; Liao, Y.; et al. Depression accelerates gastric cancer invasion and metastasis by inducing a neuroendocrine phenotype via the catecholamine/β2 -AR/MACC1 axis. Cancer Commun. 2021, 41, 1049–1070. [Google Scholar] [CrossRef] [PubMed]
- Han, L. Prevalence, risk factors and prognostic role of anxiety and depression in surgical gastric cancer patients. Transl. Cancer Res. 2020, 9, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, J.; Pan, Y.; Cai, Y.; Ge, C.; Chu, H.; Xia, C.; Song, Y.; Chen, Y.; Wu, B.; et al. The effects of video based nursing education on perioperative anxiety and depression in patients with gastric cancer. Psychol. Health Med. 2021, 26, 867–876. [Google Scholar] [CrossRef]
- Rui, A.; Xu, Q.; Yang, X. Effect of multidisciplinary cooperative continuous nursing on the depression, anxiety and quality of life in gastric cancer patients. Am. J. Transl. Res. 2021, 13, 3316–3322. [Google Scholar]
- Wu, X.; Zhang, W. Reminiscence therapy-based care program alleviates anxiety and depression, as well as improves the quality of life in recurrent gastric cancer patients. Front. Psychol. 2023, 14, 1133470. [Google Scholar] [CrossRef]
- Ni, H.; Sun, Y.; Meng, Y.; Zhang, J.; Yang, Y. Effects of Psychiatric Issues and Early Enteral Nutrition Therapy on Anxiety and Quality-of-Life of Patients with Gastric Cancer. Am. J. Health Behav. 2022, 46, 595–599. [Google Scholar] [CrossRef]
- Liu, P.; Wang, Z. Postoperative anxiety and depression in surgical gastric cancer patients: Their longitudinal change, risk factors, and correlation with survival. Medicine 2022, 101, e28765. [Google Scholar] [CrossRef]
- Bryniarski, P.; Bryniarska, M.; Jezioro, M.; Andrysiak, D.; Filipczak-Bryniarska, I. Factors connected with anxiety and other neuropsychiatric symptoms in advanced gastric cancer. Acta Neuropsychiatr. 2022, 34, 10–14. [Google Scholar] [CrossRef]
- Zhang, L. Anxiety and depression in recurrent gastric cancer: Their prevalence and independent risk factors analyses. Medicine 2021, 100, e28358. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter, n = 186 | Descriptive Statistics |
|---|---|
| Mean age (years ± SD *) | 67.6 ± 8.9 |
| Gender (n, %) | |
| Male | 124 (66.7%) |
| Female | 62 (33.3%) |
| Smoking (n, %) | |
| Regular smoker | 122 (60.2%) |
| Never smoker | 74 (39.8%) |
| Mean BMI (kg/m2, SD *) | 24.1 ± 5.4 |
| BMI status (n, %) | |
| Underweight | 47 (25.3%) |
| Normal weight | 63 (33.9%) |
| Overweight | 46 (24.7%) |
| Obese | 30 (16.1%) |
| Histopathological type (n, %) | |
| Intestinal gastric carcinoma | 88 (47.3%) |
| Diffuse gastric carcinoma | 99 (52.7%) |
| Tumor grade of differentiation (n, %) | |
| Low | 10 (5.4%) |
| Moderate | 84 (45.1%) |
| High | 92 (49.5%) |
| Tumor stage (n, %) | |
| Stage I | 54 (29.0%) |
| Stage II | 40 (21.5%) |
| Stage III | 66 (35.5%) |
| Stage IV | 26 (14.0%) |
| Tumor size (n, %) | |
| pT1 | 22 (11.8%) |
| pT2 | 60 (32.3%) |
| pT3 | 84 (45.2%) |
| pT4 | 20 (10.7%) |
| Lymph node metastasis (n, %) | |
| pN0 | 66 (35.5%) |
| pN1 | 110 (59.1%) |
| pN2 | 10 (5.4%) |
| Distant metastasis (n, %) | |
| pM0 | 164 (88.2%) |
| pM1 | 22 (11.8%) |
| International Physical Activity Questionnaire (IPAQ) level (n, %) | |
| Low | 71 (38.2%) |
| Moderate | 62 (33.3%) |
| High | 53 (28.5%) |
| Health-Related Quality of Life (HRQOL) (n, %) | |
| Low | 94 (50.5%) |
| High | 92 (49.5%) |
| Pittsburgh Sleep Quality Index (PSQI) (n, %) | |
| Inadequate | 75 (40.3%) |
| Adequate | 111 (59.7%) |
| Depression (n, %) | |
| No | 106 (57.0%) |
| Yes | 80 (43.0%) |
| Anxiety (n, %) | |
| No | 113 (60.7%) |
| Yes | 73 (32.3%) |
| Median Mediterranean diet score (IQR **) | 26 (IQR: 24–29) |
| Mediterranean diet quartile (n, %) | |
| Very low | 48 (25.8%) |
| Low | 47 (25.3%) |
| Moderate | 46 (24.7%) |
| High | 45 (24.2%) |
| Patients’ overall survival (months, IQR **) | 57 (IQR: 16–90) |
| Characteristic, n = 186 | Mediterranean Diet (MD) Adherence | ||||
|---|---|---|---|---|---|
| Very Low | Low | Moderate | High | p-Value | |
| Age (years, mean ± SD *) | 71 ± 9.5 | 67.6 ± 7.9 | 65.9 ± 10.3 | 65.5 ± 6.5 | p = 0.0106 |
| Gender (n, %) | p = 0.1378 | ||||
| Male | 29 (60.4%) | 28 (59.6%) | 31 (67.4%) | 36 (80.0%) | |
| Female | 19 (39.6%) | 19 (40.4%) | 15 (32.6%) | 9 (20.0%) | |
| Smoking status (n, %) | p < 0.0001 | ||||
| Never smoker | 17 (35.4%) | 22 (46.8%) | 37 (80.4%) | 36 (80.0%) | |
| Regular smoker | 31 (64.6%) | 25 (53.2%) | 9 (19.6%) | 9 (20.0%) | |
| Mean BMI (kg/m2 ± SD *) | 26.6 ± 8.6 | 25.7 ± 7.2 | 24.9 ± 6.5 | 24.2 ± 6.8 | p = 0.0023 |
| BMI class (n, %) | p < 0.0001 | ||||
| Underweight | 26 (54.2%) | 14 (29.8%) | 3 (6.5%) | 4 (8.9%) | |
| Normal weight | 7 (14.6%) | 15 (31.9%) | 18 (39.1%) | 23 (51.1%) | |
| Overweight | 2 (4.2%) | 9 (19.2%) | 20 (43.5%) | 15 (33.3%) | |
| Obese | 13 (27.1%) | 9 (19.2%) | 5 (10.9%) | 3 (6.7%) | |
| Histopathological type (n, %) | p = 0.0111 | ||||
| Intestinal gastric carcinoma | 15 (31.3%) | 20 (42.6%) | 24 (52.2%) | 29 (64.4%) | |
| Diffuse gastric carcinoma | 33 (68.7%) | 27 (57.4%) | 22 (47.8%) | 16 (35.6%) | |
| Tumor differentiation grade (n, %) | p < 0.0001 | ||||
| Low | 36 (75.0%) | 32 (68.1%) | 19 (41.3%) | 5 (11.1%) | |
| Moderate | 12 (25.0%) | 14 (29.8%) | 23 (50.0%) | 35 (77.8%) | |
| High | 0 (0.0%) | 1 (2.1%) | 4 (8.7%) | 5 (11.1%) | |
| Tumor stage (n, %) | p < 0.0001 | ||||
| Stage I | 6 (12.5%) | 7 (14.9%) | 24 (52.2%) | 17 (37.8%) | |
| Stage II | 4 (8.3%) | 14 (29.8%) | 8 (17.4%) | 14 (31.1%) | |
| Stage III | 27 (56.3%) | 17 (36.2%) | 11 (23.9%) | 11 (24.4%) | |
| Stage IV | 11 (22.9%) | 9 (19.1%) | 3 (6.5%) | 3 (6.7%) | |
| Tumor size (n, %) | p = 0.0003 | ||||
| pT1 | 2 (4.2%) | 3 (6.4%) | 10 (21.7%) | 7 (15.6%) | |
| pT2 | 8 (16.7%) | 14 (29.8%) | 20 (43.5%) | 18 (40.0%) | |
| pT3 | 25 (52.1%) | 26 (55.3%) | 13 (28.3%) | 20 (44.4%) | |
| pT4 | 13 (27.1%) | 4 (8.5%) | 3 (6.5%) | 0 (0.0%) | |
| Presence of lymph node metastasis (n, %) | p = 0.0201 | ||||
| No | 12 (25.0%) | 12 (25.5%) | 19 (41.3%) | 23 (51.1%) | |
| Yes | 36 (75.0%) | 35 (74.5%) | 27 (58.7%) | 22 (48.9%) | |
| Presence of distant metastasis (n, %) | p = 0.1964 | ||||
| No | 40 (83.3%) | 39 (83.0%) | 43 (93.5%) | 42 (93.3%) | |
| Yes | 8 (16.7%) | 8 (17.0%) | 3 (6.5%) | 3 (6.7%) | |
| Physical activity (n, %) | p < 0.0001 | ||||
| Low | 28 (58.4%) | 21 (44.7%) | 15 (32.6%) | 7 (15.6%) | |
| Moderate | 10 (20.8%) | 22 (46.8%) | 13 (28.3%) | 17 (37.7%) | |
| High | 10 (20.8%) | 4 (8.5%) | 18 (39.1%) | 21 (46.7%) | |
| HRQOL (n, %) | p < 0.0001 | ||||
| Low (Below mean value) | 37 (77.1%) | 28 (59.6%) | 17 (37.0%) | 12 (26.7%) | |
| High (Over mean value) | 11 (22.9%) | 19 (39.4%) | 29 (63.0%) | 33 (73.3%) | |
| PSQI (n, %) | p < 0.0001 | ||||
| Inadequate | 36 (75.0%) | 31 (66.0%) | 6 (13.0%) | 2 (4.4%) | |
| Adequate | 12 (25.0%) | 16 (44.0%) | 40 (87.0%) | 43 (95.6%) | |
| Depression (n, %) | p = 0.0003 | ||||
| No | 17 (35.4%) | 21 (44.7%) | 34 (73.9%) | 34 (75.6%) | |
| Yes | 31 (64.6%) | 26 (55.3%) | 12 (26.1%) | 11 (24.4%) | |
| Anxiety (n, %) | p = 0.0006 | ||||
| No | 18 (37.5%) | 25 (53.2%) | 34 (73.9%) | 36 (80%) | |
| Yes | 30 (62.5%) | 22 (46.8%) | 12 (26.1%) | 9 (20.0%) | |
| Patients’ overall survival (months, median, IQR **) | 17 (7–29) | 34 (21–52) | 79 (61–95) | 102 (88–116) | p < 0.0001 |
| Characteristic | Overall Survival | |
|---|---|---|
| HR * (95% CI **) | p-Value | |
| Age (Below/Over mean value) | 1.02 (0.63–1.58) | p = 0.0922 |
| Gender (Male/Female) | 1.15 (0.39–1.92) | p = 0.3478 |
| Smoking habit (Never smoker/Regular smoker) | 1.53 (1.25–1.88) | p = 0.0036 |
| BMI (Normal weight and overweight/Underweight and obese) | 1.35 (1.04–1.62) | p = 0.0015 |
| Histological type (Intestinal/Diffuse) | 1.22 (0.70–1.81) | p = 0.2237 |
| Histological grade (High/Moderate/Low) | 1.82 (1.54–2.13) | p = 0.0127 |
| Tumor size (pT1 + pT2/pT3 + pT4) | 1.43 (1.11–1.79) | p = 0.0029 |
| Lymph node metastasis (No/Yes) | 1.21 (0.71–1.83) | p = 0.1822 |
| Distant metastases (No/Yes) | 1.05 (0.29–1.81) | p = 0.4893 |
| Physical activity (High/Moderate/Low) | 2.24 (1.98–2.49) | p = 0.0008 |
| Health-Related Quality of Life (Over/Below mean value) | 2.41 (2.18–2.64) | p = 0.0023 |
| Pittsburg Sleep Quality of Life (Adequate/Inadequate) | 2.02 (1.79–2.29) | p = 0.0012 |
| Depression (No/Yes) | 2.68 (2.47–2.90) | p = 0.0025 |
| Anxiety (No/Yes) | 2.54 (2.29–2.81) | p = 0.0046 |
| MD adherence | p = 0.0001 | |
| Very low (Reference) | 1.00 | |
| Low | 1.27 (0.97–1.55) | |
| Moderate | 1.82 (1.58–2.19) | |
| High | 2.01 (1.81–2.23) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlidou, E.; Papadopoulou, S.K.; Tolia, M.; Mentzelou, M.; Tsoukalas, N.; Alexatou, O.; Tsiouda, T.; Tsourouflis, G.; Psara, E.; Bikos, V.; et al. Association of Mediterranean Diet Adherence with Disease Progression Characteristics, Lifestyle Factors and Overall Survival in Gastric Cancer Patients. Med. Sci. 2023, 11, 74. https://doi.org/10.3390/medsci11040074
Pavlidou E, Papadopoulou SK, Tolia M, Mentzelou M, Tsoukalas N, Alexatou O, Tsiouda T, Tsourouflis G, Psara E, Bikos V, et al. Association of Mediterranean Diet Adherence with Disease Progression Characteristics, Lifestyle Factors and Overall Survival in Gastric Cancer Patients. Medical Sciences. 2023; 11(4):74. https://doi.org/10.3390/medsci11040074
Chicago/Turabian StylePavlidou, Eleni, Sousana K. Papadopoulou, Maria Tolia, Maria Mentzelou, Nikolaos Tsoukalas, Olga Alexatou, Theodora Tsiouda, Gerasimos Tsourouflis, Evmorfia Psara, Vasileios Bikos, and et al. 2023. "Association of Mediterranean Diet Adherence with Disease Progression Characteristics, Lifestyle Factors and Overall Survival in Gastric Cancer Patients" Medical Sciences 11, no. 4: 74. https://doi.org/10.3390/medsci11040074