
What about the Use of Ice Cream as a Supplementary Diet in Chronic Kidney Disease? A Case–Control Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karaca, O.B.; Guven, M.; Yasar, K.; Kaya, S.; Kahyaoglu, T. The functional, rheological and sensory characteristics of ice creams with various fat replacers. Int. J. Dairy Technol. 2009, 62, 93–99. [Google Scholar] [CrossRef]
- Spence, C.; Navarra, J.; Yopussef, J. Using ice-cream as an effective vehicle for energy/nutrient delivery in the elderly. Int. J. Gastron. Food Sci. 2019, 16, 100140. [Google Scholar] [CrossRef]
- Pérez-Torres, A.; González García, M.E.; Ossorio-González, M.; Álvarez García, L.; Bajo, M.A.; Del Peso, G.; Castillo Plaza, A.; Selgas, R. The Effect of Nutritional Interventions on Long-Term Patient Survival in Advanced Chronic Kidney Disease. Nutrients 2021, 13, 621. [Google Scholar] [CrossRef]
- Kaesler, N.; Baid-Agrawal, S.; Grams, S.; Nadal, J.; Schmid, M.; Schneider, M.P.; Eckardt, K.U.; Floege, J.; Bergmann, M.M.; Schlieper, G.; et al. Low adherence to CKD-specific dietary recommendations associates with impaired kidney function, dyslipidemia, and inflammation. Eur. J. Clin. Nutr. 2021, 75, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Casas, F.; León, C.; Jovell, E.; Gómez, J.; Corvitto, A.; Blanco, R.; Alfaro, J.; Seguí, M.; Saigí, E.; Massanés, T.; et al. Adapted ice cream as a nutritional supplement in cancer patients: Impact on quality of life and nutritional status. Clin. Transl. Oncol. 2012, 14, 66–72. [Google Scholar] [CrossRef] [PubMed]
- SSNV—Source: Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione, Tabelle di Composizione degli Alimenti (Updated Year 2000), EDRA Medical Publishing, Milan, Italy. Available online: https://www.edizioniedra.it/ (accessed on 10 April 2019).
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2015–2020, 8th ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 21 February 2024).
- Abdel-Haleem, A.M.H.; Awad, R.A. Some quality attributes of low fat ice cream substituted with hulless barley flour and barley ß-glucan. J. Food Sci. Technol. 2015, 52, 6425–6434. [Google Scholar] [CrossRef]
- Cicero, N.; Naccari, C.; Cammilleri, G.; Giangrosso, G.; Cicero, A.; Gervasi, T.; Tropea, A.; Albergamo, A.; Ferrantelli, V. Monitoring of neonicotinoid pesticides in beekeeping. Nat. Prod. Res. 2017, 31, 1258–1262. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Novellino, E.; Armini, V.; Ritieni, A. State of the art of Ready-to Use Therapeutic Food: A tool for nutraceuticals addition to foodstuff. Food Chem. 2013, 140, 843–849. [Google Scholar] [CrossRef]
- Santini, A.; Novellino, E. Nutraceuticals: Beyond the Diet Before the Drugs. Curr. Bioact. Compd. 2014, 10, 1–12. [Google Scholar] [CrossRef]
- Santini, A.; Tenore, G.C.; Novellino, E. Nutraceuticals: A paradigm of proactive medicine. Eur. J. Pharm. Sci. 2017, 96, 53–61. [Google Scholar] [CrossRef]
- Daliu, P.; Santini, A.; Novellino, E. From pharmaceuticals to nutraceuticals: Bridging disease prevention and management. Expert Rev. Clin. Pharmacol. 2019, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Cammarata, S.M.; Capone, G.; Ianaro, A.; Tenore, G.C.; Pani, L.; Novellino, E. Nutraceuticals: Opening the debate for a regulatory framework. Br. J. Clin. Pharmacol. 2018, 84, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Metro, D.; Tardugno, R.; Papa, M.; Bisignano, C.; Manasseri, L.; Calabrese, G.; Gervasi, T.; Dugo, G.; Cicero, N. Adherence to the Mediterranean diet in a Sicilian student population. Nat. Prod. Res. 2018, 32, 1775–1781. [Google Scholar] [CrossRef] [PubMed]
- Metro, D.; Papa, M.; Manasseri, L.; Gervasi, T.; Campone, L.; Pellizzeri, V.; Tardugno, R.; Dugo, G. Mediterranean diet in a Sicilian student population. Second part: Breakfast and its nutritional profile. Nat. Prod. Res. 2018, 34, 2255–2261. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2008, 351, 1296–1305, Erratum in N. Engl. J. Med. 2008, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Cupisti, A.; Locatelli, F.; Bolasco, P.; Brunori, G.; Cancarini, G.; Caria, S.; De Nicola, L.; Di Iorio, B.R.; Di Micco, L.; et al. Low-protein dietsfor chronic kidney disease patients: The italian experience. BMC Nephrol. 2016, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Nutrients and Energy Reference Intake for Italian Population, 4th ed.; SINU (Italian Society of Human Nutrition): Milano, Italy, 2012.
- Rose, B.D.; Post, T.W. Regulation of acid-base balance. In Clinical Physiology of Acid-Base and Electrolyte Disorder; Rose, B.D., Post, T.W., Eds.; McGraw-Hill: New York, NY, USA, 2001; pp. 325–371. [Google Scholar]
- Chernyshova, M.P.; Pristenskiy, D.V.; Lozbiakova, M.V.; Chalyk, N.E.; Bandaletova, T.Y.; Petyaev, I.M. Systemic and skin-targeting beneficial effects of lycopene-enriched ice cream: A pilot study. J. Dairy Sci. 2019, 102, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Gervasi, T.; Oliveri, F.; Gottuso, V.; Squadrito, M.; Bartolomeo, G.; Cicero, N.; Dugo, G. Nero d’Avola and Perricone cultivars: Determination of polyphenols, flavonoids and anthocyanins in grapes and wines. Nat. Prod. Res. 2016, 30, 2329–2337. [Google Scholar] [CrossRef]
- Tuttolomondo, T.; Dugo, G.; Ruberto, G.; Leto, C.; Napoli, E.M.; Cicero, N.; Gervasi, T.; Virga, G.; Leone, R.; Licata, M.; et al. Study of quantitative and qualitative variations in essential oils of Sicilian Rosmarinus officinalis L. Nat. Prod. Res. 2015, 29, 1928–1934. [Google Scholar] [CrossRef]
- Sanguigni, V.; Manco, M.; Sorge, R.; Gnessi, L.; Francomano, D. Natural antioxidant ice cream acutely reduces oxidative stress and improves vascular function and physical performance in healthy individuals. Nutrition 2017, 33, 225–233. [Google Scholar] [CrossRef]
- Kopple, I.D.; Monteon, F.J. Effect of energy intake on nitrogen metabolism in non-dialyzed patients with chronic renal failure. Kidney Int. 1986, 29, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Goraya NWesson, D.E. Dietary interventions to improve outcomes in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 505–510. [Google Scholar] [CrossRef]
- Tom, K.; Young, V.R.; Chapman, T.; Masud, T.; Akpele, L.; Maroni, B.J. Long-term adaptive responses to dietary protein restriction in chronic renal failure. Am. J. Physiol. Endocrinol. Metab. 1995, 268, E668–E677. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, J.; Beaufre, B.; Laville, M.; Fouque, D. Adaptive response to a low-protein diet in predialysis chronic renal failure patients. J. Am. Soc. Nephrol. 2001, 12, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Masud, T.; Young, V.R.; Chapman, T.; Maroni, B.J. Adaptive response to very loe protein diets: The first comparison of Ketoacids to essential amino acids. Kidney Int. 1994, 45, 1182–1192. [Google Scholar] [CrossRef]
- Goodship, T.H.; E Mitch, W.; Hoerr, R.A.; Wagner, D.A.; Steinman, T.I.; Young, V.R. Adaptation to low-protein diets in renal failure: Leucine turnover and nitrogen balance. J. Am. Soc. Nephrol. 1990, 1, 66–75. [Google Scholar] [CrossRef]
- Kopple, J.D.; Levey, A.S.; Greene, T.; Chumlea, W.C.; Gassman, J.J.; Hollinger, D.L.; Maroni, B.J.; Merrill, D.; Scherch, L.K.; Schulman, G.; et al. Effect of dietary protein restriction on nutritional status in the Modification of Diet in Renal Disease Study. Kidney Int. 1997, 52, 778–791. [Google Scholar] [CrossRef]
- Cianciaruso, B.; Pota, A.; Bellizzi, V.; Di Giuseppe, D.; Di Micco, L.; Minutolo, R.; Pisani, A.; Sabbatini, M.; Ravani, P. Effect of a low-versus moderate-protein diet on progression of CKD: Follow-up of a randomized controlled trial. Am. J. Kidney Dis. 2009, 54, 1052–1061. [Google Scholar] [CrossRef]
- Chauveau, P.; Barthe, N.; Rigalleau, V.; Ozenne, S.; Castaing, F.; Delclaux, C.; de Précigout, V.; Combe, C.; Aparicio, M. Outcome of nutritional status and body composition of uremic patients on a very low protein diet. Am. J. Kidney. Dis. 1999, 34, 500–507. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Products | Energy (Kcal) | Proteins (g) | Carbohydrates (g) | Lipids (g) | Ca (mg) | Na (mg) | P (mg) | K (mg) |
|---|---|---|---|---|---|---|---|---|
| Milk-based ice cream | 230–180 | 4.5–2.0 | 50–20 | 13.7–5.0 | 185–60 | 97–1 | 300–1 | 250–3 |
| Fruit-based ice cream | 200–100 | 4–2.5 | 24.3–6.2 | 6.5–0 | 100–10 | 200–35 | 100–0 | 100–26 |
| Frozen ice pop | 137 | - | 36.5 | - | - | - | - | - |
| Sorbet | 132 | 0.9 | 34.2 | - | 2 | 18 | 5 | 42 |
| Diet A | Diet B | |
|---|---|---|
| Breakfast |
|
|
| Snack | Rice crackers n. 3 | Rice crackers n. 3 |
| Lunch |
|
|
| Snack |
|
|
| Dinner |
|
|
| Kcal (100 g of Product) | Proteins (g) | P (mg) | Na (mg) | K (mg) | |
|---|---|---|---|---|---|
| Lemon sorbet | 132 | 0.9 | 5 | 18 | 42 |
| Vegetables (average values) | 15 | 1 | 32 | 18 | 210 |
| Fresh fruits (average values) | 45 | 0.2 | 12 | 2 | 120 |
| Diet A | Diet B | p | |
|---|---|---|---|
| No. patients | 19 | 17 | |
| Gender | |||
| Male | 9 | 7 | |
| Female | 10 | 10 | |
| Age (mean ± SD) | 72.7 ± 4.8 | 72.3 ± 3.7 | 0.76 + |
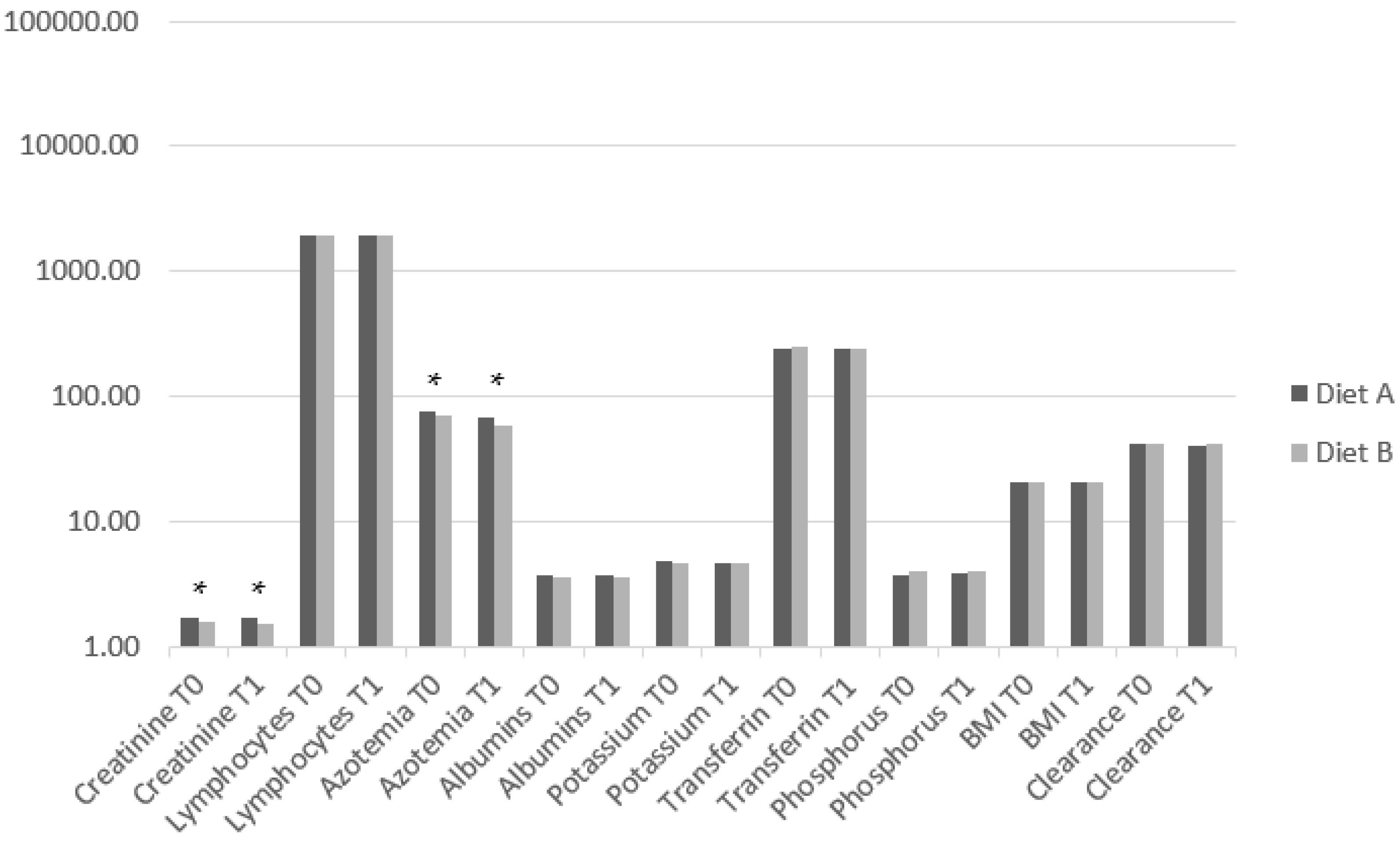
| Lymphocytes T1 | 1939.44 ± 112.12 | 1901.11 ± 61.06 | 0.4 < |
| p | 0.005 ± | 0.83 ± | |
| Azotemia T0 | 76.68 ± 2.23 | 69.17 ± 2.40 | <0.001 < |
| Azotemia T1 | 68.09 ± 1.76 | 59.12 ± 2.06 | <0.001 + |
| p | <0.001 + | <0.001 ± | |
| Albumins T0 | 3.69 ± 0.22 | 3.60 ± 0.21 | 0.28 < |
| Albumins T1 | 3.68 ± 0.18 | 3.60 ± 0.20 | 0.26 + |
| p | 1 ± | 1 + | |
| Potassium T0 | 4.76 ± 0.32 | 4.65 ± 0.50 | 0.59 < |
| Potassium T1 | 4.69 ± 0.27 | 4.64 ± 0.44 | 0.9 < |
| p | 0.29 ± | 0.82 + | |
| Transferrin T0 | 241.0 ± 22.14 | 251.39 ± 25.79 | 0.1 < |
| Transferrin T1 | 238.11 ± 27.58 | 241.11 ± 25.47 | 0.74 + |
| p | 0.77 ± | <0.001 ± | |
| Phosphorus T0 | 3.73 ± 0.58 | 3.98 ± 0.51 | 0.17 + |
| Phosphorus T1 | 3.78 ± 0.48 | 3.97 ± 0.42 | 0.21 + |
| p | 0.46 + | 0.86 + | |
| BMI T0 | 20.48 ± 1.59 | 20.49 ± 0.98 | 0.98 + |
| BMI T1 | 20.57 ± 1.50 | 20.50 ± 0.97 | 0.87 + |
| p | 0.44 + | 0.87 + | |
| Clearance T0 | 41.34 ± 3.57 | 41.8 ± 2.82 | 0.67 + |
| Clearance T1 | 40.87 ± 4.05 | 41.69 ± 2.90 | 0.49 + |
| p | 0.48 + | 0.11 + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metro, D.; Corallo, F.; Cardile, D.; Gembillo, G.; Manasseri, L.; Santoro, D.; Buda, M.; Calabrò, R.S.; Bonanno, L. What about the Use of Ice Cream as a Supplementary Diet in Chronic Kidney Disease? A Case–Control Study. Med. Sci. 2024, 12, 22. https://doi.org/10.3390/medsci12020022
Metro D, Corallo F, Cardile D, Gembillo G, Manasseri L, Santoro D, Buda M, Calabrò RS, Bonanno L. What about the Use of Ice Cream as a Supplementary Diet in Chronic Kidney Disease? A Case–Control Study. Medical Sciences. 2024; 12(2):22. https://doi.org/10.3390/medsci12020022
Chicago/Turabian StyleMetro, Daniela, Francesco Corallo, Davide Cardile, Guido Gembillo, Luigi Manasseri, Domenico Santoro, Martina Buda, Rocco Salvatore Calabrò, and Lilla Bonanno. 2024. "What about the Use of Ice Cream as a Supplementary Diet in Chronic Kidney Disease? A Case–Control Study" Medical Sciences 12, no. 2: 22. https://doi.org/10.3390/medsci12020022