Differences in Hypotensive vs. Non-Hypotensive Sepsis Management in the Emergency Department: Door-to-Antibiotic Time Impact on Sepsis Survival

 and
and
Abstract
:1. Introduction
2. Materials and Methods
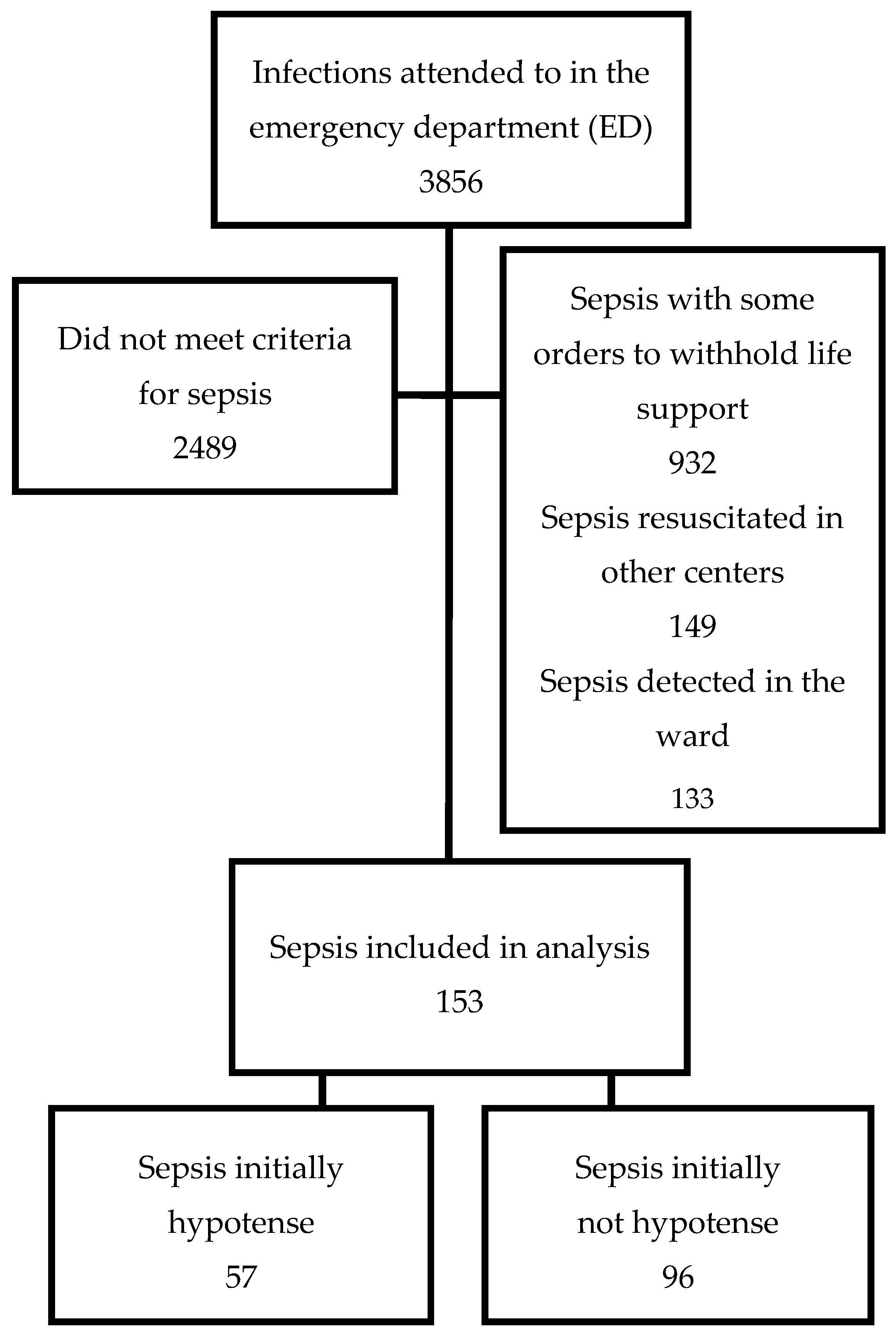
2.1. Patient Selection
2.2. Data Collection
2.3. Statistical Analysis
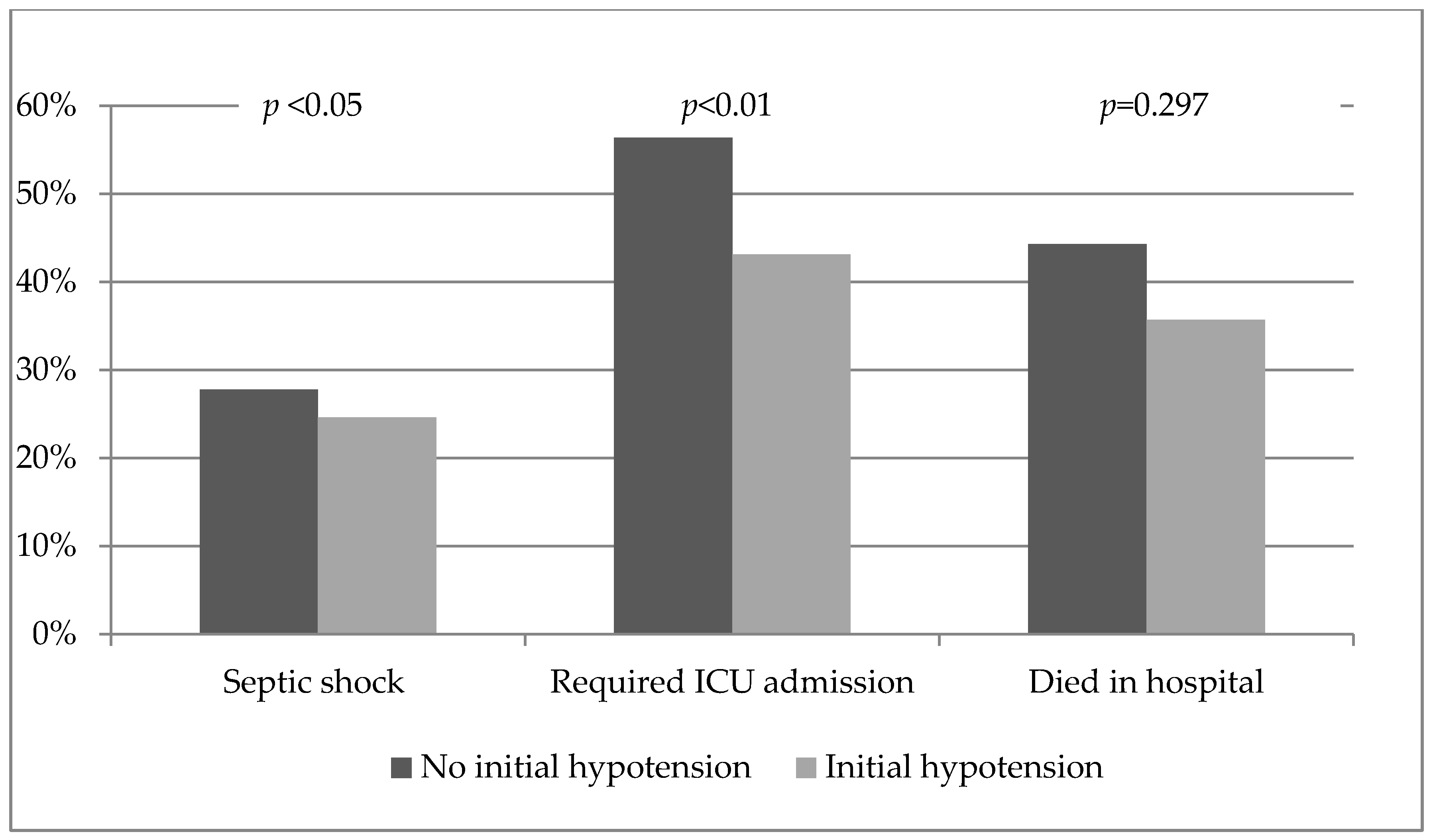
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G.; et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Yébenes, J.C.; Ruiz-Rodriguez, J.C.; Ferrer, R.; Clèries, M.; Bosch, A.; Lorencio, C.; Rodriguez, A.; Nuvials, X.; Martin-Loeches, I.; Artigas, A.; et al. Epidemiology of sepsis in Catalonia: Analysis of incidence and outcomes in a European setting. Ann. Intensive Care 2017, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Rubens, M.; Saxena, A.; Ramamoorthy, V.; Das, S.; Khera, R.; Hong, J.; Armaignac, D.; Veledar, E.; Nasir, K.; Gidel, L. Increasing Sepsis Rates in the United States: Results From National Inpatient Sample, 2005 to 2014. J. Intensive Care Med. 2018, 2, 885066618794136. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, D.P.; Laursen, C.B.; Jensen, T.G.; Hallas, J.; Pedersen, C.; Lassen, A.T. Incidence rate of community-acquired sepsis among hospitalized acute medical patients-a population-based survey. Crit. Care Med. 2015, 43, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Almirall, J.; Güell, E.; Capdevila, J.A.; Campins, L.; Palomera, E.; Martinez, R.; Miró, G.; de la Torre, M.C.; Solsona, M.; Yébenes, J.C. Epidemiology of community-acquired severe sepsis. A population-based study. Med. Clin. 2016, 147, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Gesten, F.; Prescott, H.C.; Friedrich, M.E.; Iwashyna, T.J.; Phillips, G.S.; Lemeshow, S.; Osborn, T.; Terry, K.M.; Levy, M.M. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N. Engl. J. Med. 2017, 376, 2235–2244. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Yanes, J.M.; Andueza-Lillo, J.A.; Gonzalez-Ramallo, V.J.; Pastor, L.; Munoz, J. Failure to implement evidence-based clinical guidelines for sepsis at the ED. Am. J. Emerg. Med. 2006, 24, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Vallés, J.; Rello, J.; Ochagavía, A.; Garnacho, J.; Alcalá, M.A. Community-acquired bloodstream infection in critically ill adult patients: Impact of shock and inappropriate antibiotic therapy on survival. Chest 2003, 123, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit. Care Med. 2008, 36, 296–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yébenes, J.C. Chain for the resuscitation of septic patients. PsterSSpsiaGreu2016CSdMCC.
- Marshall, J.C.; Cook, D.J.; Christou, N.V.; Bernard, G.R.; Sprung, C.L.; Sibbald, W.J. Multiple organ dysfunction score: A reliable descriptor of a complex clinical outcome. Crit. Care Med. 1995, 23, 1638–1652. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Phillips, G.; Beale, R.; Cecconi, M.; Chiche, J.D.; De Backer, D.; Divatia, J.; Du, B.; Evans, L.; Ferrer, R.; et al. The Surviving Sepsis Campaign bundles and outcome: Results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015, 41, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Artigas, A.; Levy, M.M.; Blanco, J.; González-Díaz, G.; Garnacho-Montero, J.; Ibáñez, J.; Palencia, E.; Quintana, M.; de la Torre-Prados, M.V.; et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 2008, 299, 2294–2303. [Google Scholar] [CrossRef] [PubMed]
- Coba, V.; Whitmill, M.; Mooney, R.; Horst, H.M.; Brandt, M.M.; Digiovine, B.; Mlynarek, M.; McLellan, B.; Boleski, G.; Yang, J.; et al. Resuscitation bundle compliance in severe sepsis and septic shock: Improves survival, is better late than never. J. Intensive Care Med. 2011, 26, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.B.; Corbett, S.W.; Steele, R.; Banta, J.; Clark, R.T.; Hayes, S.R.; Edwards, J.; Cho, T.W.; Wittlake, W.A. Implementation of a bundle of quality indicators for the early management of severe sepsis and septic shock is associated with decreased mortality. Crit. Care Med. 2007, 35, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Joo, Y.M.; Chae, M.K.; Hwang, S.Y.; Jin, S.C.; Lee, T.R.; Cha, W.C.; Jo, I.J.; Sim, M.S.; Song, K.; Jeong, Y.K.; et al. Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department. Clin. Exp. Emerg. Med. 2014, 1, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Puskarich, M.A.; Trzeciak, S.; Shapiro, N.I.; Arnold, R.C.; Horton, J.M.; Studnek, J.R.; Kline, J.A.; Jones, A.E. Emergency Medicine Shock Research Network (EMSHOCKNET). Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit. Care Med. 2011, 39, 2066–2071. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.F.; Zheng, R.Q.; Lin, H.; Shao, J.; Yu, J.Q.; Yang, D.G. Improved sepsis bundles in the treatment of septic shock: A prospective clinical study. Am. J. Emerg. Med. 2015, 33, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Rodriguez, A.; Solé-Violán, J.; Blanquer, J.; Almirall, J.; Rello, J. Community-Acquired Pneumonia Intensive Care Units (CAPUCI) Study Investigators. Effects of delayed oxygenation assessment on time to antibiotic delivery and mortality in patients with severe sepsis community-acquired pneumonia. Crit. Care Med. 2007, 35, 2509–2514. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.B.; Loomba, M.; Yang, J.J.; Jacobsen, G.; Shah, K.; Otero, R.M.; Suarez, A.; Parekh, H.; Jaehne, A.; Rivers, E.P. Early lactate clearance is associated with biomarkers of inflammation, coagulation, apoptosis, organ dysfunction and mortality in severe sepsis and septic shock. J. Inflamm. (Lond.) 2010, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranzani, O.T.; Monteiro, M.B.; Ferreira, E.M.; Santos, S.R.; Machado, F.R.; Noritomi, D.T. Reclassifying the spectrum of septic patients using lactate: Severe sepsis, cryptic shock, vasoplegic shock and dysoxic shock. Rev. Bras. Ter. Intensiva 2013, 25, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Sterling, S.A.; Puskarich, M.A.; Shapiro, N.I.; Trzeciak, S.; Kline, J.A.; Summers, R.L.; Jones, A.E. Emergency Medicine Shock Research Network (EMSHOCKNET). Characteristics and outcomes of patients with vasoplegic versus tissue dysoxic septic shock. Shock 2013, 40, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; Martín-Fernandez, M.; Almansa, R. Pre-sepsis: A necessary concept to complete the SEPSIS-3 picture? J. Crit. Care 2017, 44, 148. [Google Scholar] [CrossRef] [PubMed]
- Yébenes, J.C. Early detection of sepsis: To adapt or to die. Med. Clin. 2017, 149, 209–210. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Tsaganos, T.; Tsangaris, I.; Lada, M.; Routsi, C.; Sinapidis, D.; Koupetori, M.; Bristianou, M.; Adamis, G.; Mandragos, K.; et al. Validation of the new Sepsis-3 definitions: Proposal for improvement in early risk identification. Clin. Microbiol. Infect. 2017, 23, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; Almansa, R.; Yebenes, J.C. New Organ Failure as an Alternative Endpoint to Develop Diagnostic Criteria for Sepsis. Chest 2018, 153, 1278. [Google Scholar] [CrossRef] [PubMed]
- Allgöwer, M.; Buri, C. Schockindex. Deutsche Med. Wodenschrift 1967, 46, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Birkhahn, R.H.; Gaeta, T.J.; Terry, D.; Bove, J.J.; Tloczkowski, J. Shock Index in diagnosing early acute hypovolemia. Am. J. Emerg. Med. 2005, 23, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Berger, T.; Green, J.; Horeczko, T.; Hagar, Y.; Garg, N.; Suarez, A.; Panacek, E.; Shapiro, N. Shock Index and Early Recognition of Sepsis in the Emergency Department: Pilot Study. West. J. Emerg. Med. 2013, 14, 168–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, N.I.; Arnold, R.; Sherwin, R.; O’Connor, J.; Najarro, G.; Singh, S.; Lundy, D.; Nelson, T.; Trzeciak, S.W.; Jones, A.E. The association of near-infrared spectroscopy-derived tissue oxygenation measurements with sepsis syndromes, organ dysfunction and mortality in emergency department patients with sepsis. Crit. Care 2011, 15, R223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claverias, L.; Marí, M.; Marín-Corral, J.; Magret, M.; Trefler, S.; Bodí, M.; García-España, A.; Yébenes, J.C.; Pascual, S.; Gea, J.; et al. The prognostic value of muscle regional oxygen saturation index in severe community-acquired pneumonia: A prospective observational study. J. Intensive Care 2016, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.B.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013, 84, 465–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Heldens, M.; Schout, M.; Hammond, N.E.; Bass, F.; Delaney, A.; Finfer, S.R. Sepsis incidence and mortality are underestimated in Australian intensive care unit administrative data. Med. J. 2018, 6, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, E.K.; Rubenstein, A.R.; Radin, G.T.; Wiener, R.S.; Walkey, A.J. Two decades of mortality trends among patients with severe sepsis: A comparative meta-analysis. Crit. Care Med. 2014, 42, 625–631. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients | Survivors | Non-Survivors | p | ||
|---|---|---|---|---|---|
| n = 153 | n = 90 (59%) | n = 63 (41%) | OR (95% CI) | ||
| Gender | |||||
| Male | 54.5% | 62.2% | 44.4% | 0.03 | 2.06 (1.07–3.96) |
| Age | |||||
| Years | 73.6 ± 15.78 | 70.3 ± 16.1 | 78.4 ± 14.2 | 0.003 | 1.04 (1.01–1.06) |
| Infection | |||||
| Urinary | 29.9% | 28.9% | 30.2% | ns | 0.93 (0.41–2.12) |
| Respiratory | 26% | 28.9% | 22.2% | ns | 1.42 (0.63–3.22) |
| Abdominal | 24% | 23.3% | 25.4% | ns | 0.94 (0.44–2.02) |
| Initial vital signs | |||||
| Presence of AhT | 36.6% | 40.0% | 31.7% | ns | 0.70 (0.35–1.37) |
| Systolic BP (mmHg) | 106.2 ± 28.8 | 104.9 ± 30.4 | 108.1 ± 26.74 | ns | 1.00 (0.99–1.02) |
| MAP (mmHg) | 75.5 ± 17.86 | 74 ± 20.18 | 77.5 ± 19.43 | ns | 1.01 (0.99–1.03) |
| HR (beats/minute) | 99 ± 26.08 | 100 ± 24.03 | 98 ± 28.83 | ns | 0.99 (0.98–1.01) |
| RR (breaths/minute | 25 ± 7.20 | 24.5 ± 6.50 | 26.9 ± 7.79 | 0.04 | 1.05 (0.99–1.10) |
| Sat O2 B (%) | 91% ± 7.16 | 92.5 ± 6.67 | 89.8 ± 7.63 | 0.02 | 0.95 (0.91–0.99) |
| Glycemia (mg/dl) | 154.2 ± 97.9 | 158.9 ± 19.7 | 191.7 ± 134.4 | 0.01 | 0.99 (0.99–1.00) |
| Temperature (°C) | 37.06 ± 1.45 | 37.1 ± 1.5 | 37 ± 1.36 | ns | 0.97 (0.77–1.21) |
| Lactate | |||||
| 0 h | 5.24 ± 3.27 | 4.36 ± 2.1 | 6.68 ± 4.2 | 0.02 | 1.30 (1.04–0.62) |
| 6 h | 3.92 ± 3.35 | 3.00 ± 1.9 | 6.36 ± 5.03 | 0.001 | 1.38 (1.03–1.85) |
| SOFA score (6 h) | 4.9 ± 2.74 | 4.83 ± 2.74 | 4.98 ± 2.73 | ns | 1.02 (0.91–1.15) |
| Time to measures | |||||
| Door-to-antibiotic | 4.09 ± 4.13 | 3.38 ± 3.08 2.2 * (1.26–4.98) ** | 5.21 ± 5.20 3.25 * (1.46–7.20) ** | 0.05 | 1.12 (1.02–1.22) |
| Door-to-blood cultures | 2.34 ± 3.24 | 2.21 ± 3.22 | 2.59 ± 3.29 | ns | 1.04 (0.93–1.16) |
| Door-to-fluid resuscitation | 7.52 ± 4.28 | 7.14 ± 4.18 | 8.21 ± 4.42 | ns | 1.06 (0.96–1.17) |
| Required CVP | 53 (34.9%) | 33 (36.7%) | 20 (31.7%) | ns | 0.72 (0.36–1.42) |
| Door-to-CVP time | 6.72 ± 4.18 | 5.74 ± 3.22 | 8.34 ± 5.08 | 0.06 | 1.18 (1.01–1.37) |
| Required noradrenalin | 42 (27.5%) | 25 (27.8%) | 16 (25.4%) | ns | 0.75 (0.36–1.55) |
| Door-to-noradrenalin time | 7.59 ± 5.10 | 6.23 ± 3.65 | 9.72 ± 6.34 | 0.07 | 1.16 (1.01–1.34) |
| No Hypotension | Hypotension | p | ||
|---|---|---|---|---|
| n = 97 (63%) | n = 57 (37%) | OR (95%CI) | ||
| Gender | ||||
| Male | 55.7% | 52.6% | ns | 1.13 (0.59–2.18) |
| Age | ||||
| Years | 74.03 ± 15.94 | 72.86 ± 16.38 | ns | 0.99 (0.97–1.02) |
| Infection | ||||
| Urinary | 24.7% | 38.6 | ns | 0.52 (0.24–1.12) |
| Respiratory | 26.8% | 24.6% | ns | 1.33 (0.59–3.05) |
| Abdominal | 26.8% | 19.3% | ns | 1.81 (0.76–4.38) |
| Initial vital signs | ||||
| Systolic BP (mmHg) | 121.48 ± 25.16 | 80.19 ± 9.37 | ns | 0.82 (0.76–0.88) |
| MAP (mmHg) | 87 ± 19 | 55 ± 6.45 | - | |
| HR (beats/minute) | 101.52 ± 25.58 | 96.17 ± 26.80 | ns | 0.99 (0.98–1.01) |
| RR (breaths/minute) | 25.74 ± 6.92 | 25.28 ± 7.76 | ns | 0.99 (0.95–1.04) |
| Sat O2 B (%) | 91.6 ± 7.17 | 90.96 ± 7.21 | ns | 0.99 (0.94–1.03) |
| Glycemia (mg/dl) | 159.3 ± 85.0 | 145.8 ± 116.9 | 0.06 | 0.99 (0.99–1.00) |
| Temperature (°C) | 37.16 ± 1.50 | 36.89 ± 1.36 | ns | 0.88 (0.69–1.10) |
| Lactate | ||||
| 0 h | 4.42 ± 2.22 | 6.23 ± 4.03 | 0.03 | 1.22 (0.99–1.50) |
| 6 h | 3.99 ± 3.50 | 3.75 ± 3.15 | ns | 0.98 (0.78–1.23) |
| SOFA score (6 h) | 4.29 ± 2.41 | 5.95 ± 2.99 | <0.001 | 1.26 (1.10–1.45) |
| Time to measures | ||||
| Door-to-antibiotic * | 4.40 ± 4.25 2.63 * (1.62–6.32) ** | 3.62 ± 3.93 1.87 * (1.1–5.37) ** | 0.08 | 0.95 (0.87–1.04) |
| Door-to-blood cultures | 2.68 ± 3.57 | 1.82 ± 2.59 | 0.09 | 0.91 (0.80–1.04) |
| Door-to-fluid resuscitation | 8.49 ± 4.36 | 6.19 ± 3.83 | 0.01 | 0.87 (0.78–0.97) |
| Required CVP | 33; 34.3% | 20; 35% | ns | 1.06 (0.53–2.12) |
| Door-to-CVP time | 7.90 ± 4.15 | 4.78 ± 3.52 | 0.004 | 0.80 (0.67–0.95) |
| Required noradrenalin | 27; 28.1% | 14; 24.5% | ns | 0.82 (0.39–1.74) |
| Door-to-noradrenalin time | 8.99 ± 4.91 | 4.89 ± 4.46 | 0.01 | 0.81 (0.68–0.97) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballester, L.; Martínez, R.; Méndez, J.; Miró, G.; Solsona, M.; Palomera, E.; Capdevila, J.A.; Rodriguez, A.; Yébenes, J.C. Differences in Hypotensive vs. Non-Hypotensive Sepsis Management in the Emergency Department: Door-to-Antibiotic Time Impact on Sepsis Survival. Med. Sci. 2018, 6, 91. https://doi.org/10.3390/medsci6040091
Ballester L, Martínez R, Méndez J, Miró G, Solsona M, Palomera E, Capdevila JA, Rodriguez A, Yébenes JC. Differences in Hypotensive vs. Non-Hypotensive Sepsis Management in the Emergency Department: Door-to-Antibiotic Time Impact on Sepsis Survival. Medical Sciences. 2018; 6(4):91. https://doi.org/10.3390/medsci6040091
Chicago/Turabian StyleBallester, Leonor, Rafael Martínez, Juan Méndez, Gloria Miró, Manel Solsona, Elisabeth Palomera, Josep Anton Capdevila, Alejandro Rodriguez, and Juan Carlos Yébenes. 2018. "Differences in Hypotensive vs. Non-Hypotensive Sepsis Management in the Emergency Department: Door-to-Antibiotic Time Impact on Sepsis Survival" Medical Sciences 6, no. 4: 91. https://doi.org/10.3390/medsci6040091