Exercise Increases Adiponectin and Reduces Leptin Levels in Prediabetic and Diabetic Individuals: Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Risk of Bias Assessment
2.4. Data Extraction and Analysis
3. Results
3.1. Characteristics of Included Trials
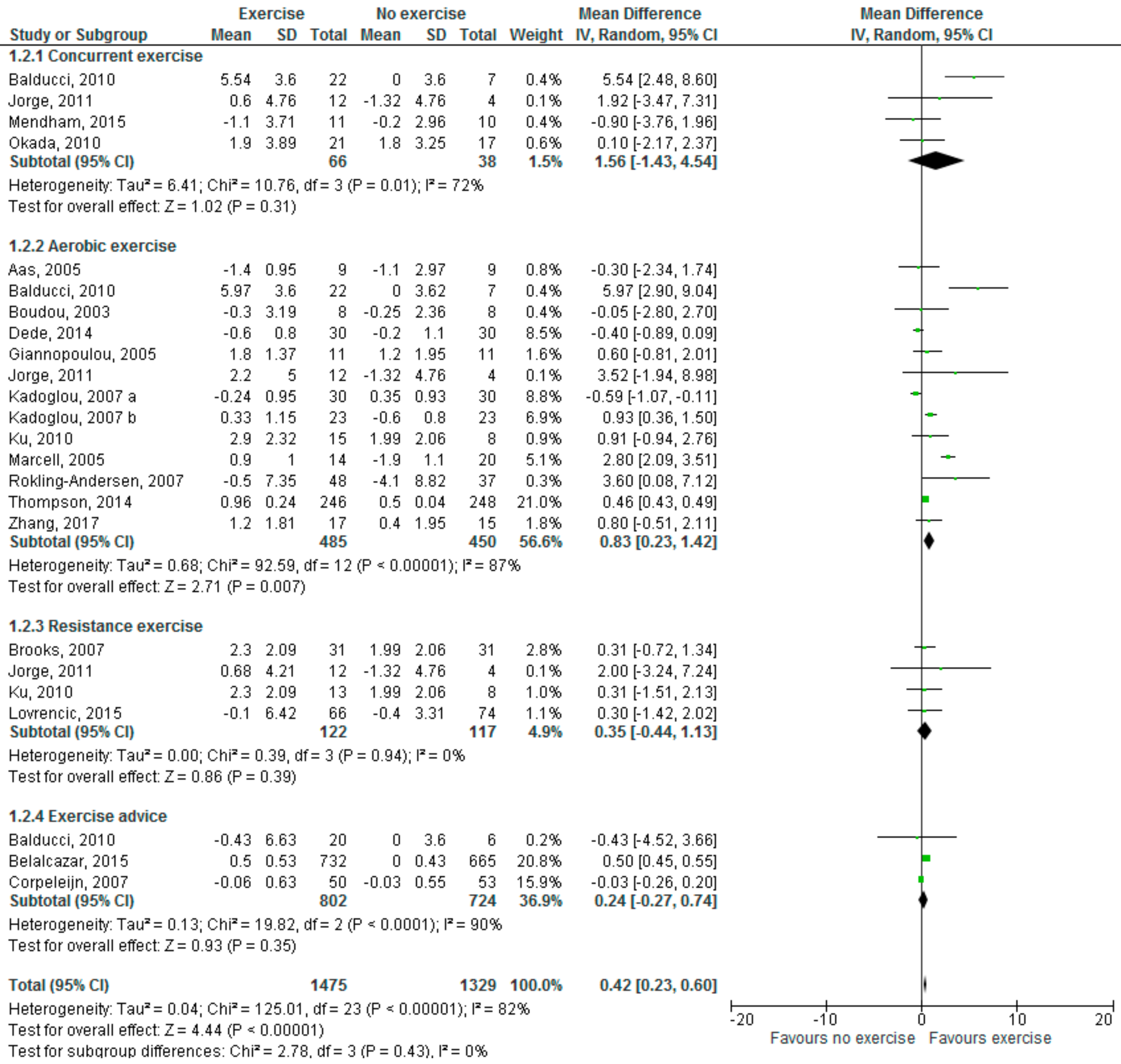
3.2. Influence of Exercise on Adiponectin and Leptin Levels
3.3. Sensitivity Analysis
3.4. Subgroup Analysis
3.5. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes. 2016. Available online: http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf (accessed on 3 April 2018).
- World Health Organization. Diabetes Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs138/en (accessed on 3 April 2018).
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS ONE 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- US National Center for Chronic Disease Prevention and Health Promotion. National Diabetes Statistics Report 2017: Estimates of Diabetes and its Burden in the United States. Available online: http://www.diabetes.org/assets/pdfs/basics/cdc-statistics-report-2017.pdf (accessed on 4 April 2018).
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2790. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- UK Academy of Medical Royal Colleges. Exercise—The Miracle Cure. 2015. Available online: http://www.aomrc.org.uk/wp-content/uploads/2016/05/Exercise_the_Miracle_Cure_0215.pdf (accessed on 5 April 2018).
- Jeon, C.Y.; Lokken, R.P.; Hu, F.B.; van Dam, R.M. Physical activity of moderate intensity and risk of type 2 diabetes, a systematic review. Diabetes Care 2007, 30, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Morrato, E.H.; Hill, J.O.; Wyatt, H.R.; Ghushchyan, V.; Sullivan, P.W. Physical activity in U.S. adults with diabetes and at risk for developing diabetes, 2003. Diabetes Care 2007, 30, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Boulé, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: A meta-analysis of controlled clinical trials. JAMA 2001, 286, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Boulé, N.G.; Kenny, G.P.; Haddad, E.; Wells, G.A.; Sigal, R.J. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in type 2 diabetes mellitus. Diabetologia 2003, 46, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; Iacobellis, G.; Parisi, L.; Di Biase, N.; Calandriello, E.; Leonetti, F.; Fallucca, F. Exercise training can modify the natural history of diabetic peripheral neuropathy. J. Diabetes Complications 2006, 20, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Pagkalos, M.; Koutlianos, N.; Kouidi, E.; Pagkalos, E.; Mandroukas, K.; Deligiannis, A. Heart rate variability modifications following exercise training in type 2 diabetic patients with definite cardiac autonomic neuropathy. Br. J. Sports Med. 2008, 42, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Eves, N.D.; Plotnikoff, R.C. Resistance training and type 2 diabetes. Considerations for implementation at the population level. Diabetes Care 2006, 29, 1933–1941. [Google Scholar] [CrossRef] [PubMed]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q.; et al. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Missbach, B.; Dias, S.; König, J.; Hoffmann, G. Impact of different training modalities on glycaemic control and blood lipids in patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetologia 2014, 57, 1789–1797. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Scott, C.A.; Mao, C.; Tang, J.; Farmer, A.J. Resistance exercise versus aerobic exercise for type 2 diabetes: A systematic review and meta-analysis. Sports Med. 2014, 44, 487–49. [Google Scholar] [CrossRef] [PubMed]
- Paulweber, B.; Valensi, P.; Lindström, J.; Lalic, N.M.; Greaves, C.J.; McKee, M.; Kissimova-Skarbek, K.; Liatis, S.; Cosson, E.; Szendroedi, J.; et al. A European evidence-based guideline for the prevention of type 2 diabetes. Horm. Metab. Res. 2010, 42 (Suppl. 1), S3–S36. [Google Scholar] [CrossRef] [PubMed]
- The American Diabetes Association. Standards of Medical Care in Diabetes—2016. Available online: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf (accessed on 18 April 2018).
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C.; White, R.D. Physical activity/exercise and type 2 diabetes. A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Proenca, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional cloning of the mouse obese gene and its human homologue. Nature 1994, 372, 425–432. [Google Scholar] [CrossRef] [PubMed]
- McGown, C.; Birerdinc, A.; Younossi, Z.M. Adipose tissue as an endocrine organ. Clin. Liver Dis. 2014, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Verheggen, R.J.; Maessen, M.F.; Green, D.J.; Hermus, A.R.; Hopman, M.T.; Thijssen, D.H. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef] [PubMed]
- Kelesidis, T.; Kelesidis, I.; Chou, S.; Mantzoros, C.S. Narrative review: The role of leptin in human physiology: Emerging clinical applications. Ann. Intern. Med 2010, 152, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, Y. Adiponectin: Identification, physiology and clinical relevance in metabolic and vascular disease. Atheroscler. Suppl. 2005, 6, 7–14. [Google Scholar] [CrossRef] [PubMed]
- López-Jaramillo, P.; Gómez-Arbeláez, D.; López-López, J.; López-López, C.; Martínez-Ortega, J.; Gómez-Rodríguez, A.; Triana-Cubillos, S. The role of leptin/adiponectin ratio in metabolic syndrome and diabetes. Horm. Mol. Biol. Clin. Investig. 2014, 18, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Hu, M.; Yan, Y.; Zhang, H. The effect of exercise on adiponectin and leptin levels in overweight or obese subjects: A meta-analysis of randomized controlled trials. Sport Sci. Health 2017, 13, 303–314. [Google Scholar] [CrossRef]
- Sturgeon, K.; Digiovanni, L.; Good, J.; Salvatore, D.; Fenderson, D.; Domchek, S.; Stopfer, J.; Galantino, M.L.; Bryan, C.; Hwang, W, T.; Schmitz, K. Exercise-induced dose-response alterations in adiponectin and leptin levels are dependent on body fat changes in women at risk for breast cancer. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Abbenhardt, C.; McTiernan, A.; Alfano, C.M.; Wener, M.H.; Campbell, K.L.; Duggan, C.; Foster-Schubert, K.E.; Kong, A.; Toriola, A.T.; Potter, J.D.; et al. Effects of individual and combined dietary weight loss and exercise interventions in postmenopausal women on adiponectin and leptin levels. J. Intern. Med. 2013, 274, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Greean, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1. Available online: http://handbook.cochrane.org (accessed on 19 April 2018).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Community: Review Manager 5.3. Available online: http://tech.cochrane.org/revman/download (accessed on 18 April 2018).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Bouassida, A.; Chamari, K.; Zaouali, M.; Feki, Y.; Zbidi, A.; Tabka, Z. Review on leptin and adiponectin responses and adaptations to acute and chronic exercise. Br. J. Sports Med. 2010, 44, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Annibalini, G.; Lucertini, F.; Agostini, D.; Vallorani, L.; Gioacchini, A.; Barbieri, E.; Guescini, M.; Casadei, L.; Passalia, A.; Del Sal, M.; et al. Concurrent aerobic and resistance training has anti-inflammatory effects and increases both plasma and leukocyte levels of IGF-1 in late middle aged type 2 diabetic. Oxid. Med. Cell. Longev. 2017, 2017, 3937842. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; Zanuso, S.; Nicolucci, A.; Fernando, F.; Cavallo, S.; Cardelli, P.; Fallucca, S.; Alessi, E.; Letizia, C.; Jimenez, A.; et al. Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Jorge, M.L.; de Oliveira, V.N.; Resende, N.M.; Paraiso, L.F.; Calixto, A.; Debs Diniz, A.L.; Resende, E.S.; Ropelle, E.R.; Carvalheira, J.B.; Espindola, F.S.; et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metabolism 2011, 60, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Loimaala, A.; Groundstroem, K.; Rinne, M.; Nennonen, A.; Huhtala, H.; Parkkari, J.; Vuori, I. Effect of long-term endurance and strength training on metabolic control and arterial elasticity in patients with type 2 diabetes mellitus. Am. J. Cardiol. 2009, 103, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Mendham, A.E.; Duffield, R.; Marino, F.; Coutts, A.J. A 12-week sports-based exercise programme for inactive Indigenous Australian men improved clinical risk factors associated with type 2 diabetes mellitus. J. Sci. Med. Sport 2015, 18, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Okada, S.; Hiuge, A.; Makino, H.; Nagumo, A.; Takaki, H.; Konishi, H.; Goto, Y.; Yoshimasa, Y.; Miyamoto, Y. Effect of exercise intervention on endothelial function and incidence of cardiovascular disease in patients with type 2 diabetes. J. Atheroscler. Thromb. 2010, 17, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Aas, A.M.; Seljeflot, I.; Torjesen, P.A.; Diep, L.M.; Thorsby, P.M.; Birkeland, K.I. Blood glucose lowering by means of lifestyle intervention has different effects on adipokines as compared with insulin treatment in subjects with type 2 diabetes. Diabetologia 2006, 49, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Boudou, P.; Sobngwi, E.; Mauvais-Jarvis, F.; Vexiau, P.; Gautier, J.F. Absence of exercise-induced variations in adiponectin levels despite decreased abdominal adiposity and improved insulin sensitivity in type 2 diabetic men. Eur. J. Endocrinol. 2003, 149, 421–444. [Google Scholar] [CrossRef] [PubMed]
- Dede, N.D.; Ipekci, S.H.; Kebapcilar, L.; Arslan, M.; Kurban, S.; Yildiz, M.; Gönen, M.S. Influence of exercise on leptin, adiponectin and quality of life in type 2 diabetics. Turkish J. Endocrin. Metable. 2015, 19, 7–13. [Google Scholar] [CrossRef]
- Giannopoulou, I.; Fernhall, B.; Carhart, R.; Weinstock, R.S.; Baynard, T.; Figueroa, A.; Kanaley, J.A. Effects of diet and/or exercise on the adipocytokine and inflammatory cytokine levels of postmenopausal women with type 2 diabetes. Metabolism 2005, 54, 866–875. [Google Scholar] [CrossRef] [PubMed]
- Ishii, T.; Yamakita, T.; Yamagami, K.; Yamamoto, T.; Miyamoto, M.; Kawasaki, K.; Hosoi, M.; Yoshioka, K.; Sato, T.; Tanaka, S.; et al. Effect of exercise training on serum leptin levels in type 2 diabetic patients. Metabolism 2001, 50, 1136–1140. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.; Iliadis, F.; Angelopoulou, N.; Perrea, D.; Ampatzidis, G.; Liapis, C.D.; Alevizos, M. The anti-inflammatory effects of exercise training in patients with type 2 diabetes mellitus. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.; Iliadis, F.; Liapis, C.D.; Perrea, D.; Angelopoulou, N.; Alevizos, M. Beneficial effects of combined treatment with rosiglitazone and exercise on cardiovascular risk factors in patients with type 2 diabetes. Diabetes Care 2007, 30, 2242–2244. [Google Scholar] [CrossRef] [PubMed]
- Ku, Y.H.; Han, K.A.; Ahn, H.; Kwon, H.; Koo, B.K.; Kim, H.C.; Min, K.W. Resistance exercise did not alter intramuscular adipose tissue but reduced retinol-binding protein-4 concentration in individuals with type 2 diabetes mellitus. J. Int. Med. Res. 2010, 38, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Marcell, T.J.; McAuley, K.A.; Traustadóttir, T.; Reaven, P.D. Exercise training is not associated with improved levels of C-reactive protein or adiponectin. Metabolism 2005, 54, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Rokling-Andersen, M.H.; Reseland, J.E.; Veierød, M.B.; Anderssen, S.A.; Jacobs, D.R.; Urdal, P.; Jansson, J.O.; Drevon, C.A. Effects of long-term exercise and diet intervention on plasma adipokine concentrations. Am. J. Clin. Nutr. 2007, 86, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Walhin, J.P.; Batterham, A.M.; Stokes, K.; Cooper, A.R.; Andrews, R.C. Effect of diet or diet plus physical activity versus usual care on inflammatory markers in patients with newly diagnosed type 2 diabetes: The Early ACTivity In Diabetes (ACTID) randomized, controlled trial. J. Am. Heart Assoc. 2014, 3, e000828. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Y.; Liu, T.; Teng, Y.Q.; Yao, X.Y.; Zhao, T.T.; Lin, L.Y.; Jin, Q.S.; Jin, Y.J. Effect of a 12-week aerobic exercise training on serum fetuin-A and adipocytokine levels in type 2 diabetes. Exp. Clin. Endocrinol. Diabetes 2017. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Brook, N.; Layne, J.E.; Gordon, P.L.; Roubenoff, R.; Nelson, M.E.; Castaneda-Sceppa, C. Strength training improves muscle quality and insulin sensitivity in Hispanic older adults with type 2 diabetes. Int. J. Med. Sci. 2006, 4, 19–27. [Google Scholar] [CrossRef]
- Vučić Lovrenčić, M.; Pibernik-Okanović, M.; Šekerija, M.; Prašek, M.; Ajduković, D.; Kos, J.; Hermanns, N. Improvement in depressive symptoms is associated with reduced oxidative damage and inflammatory response in type 2 diabetic patients with subsyndromal depression: The results of a randomized controlled trial comparing psychoeducation, physical exercise, and enhanced treatment as usual. Int. J. Endocrin. 2015, 2015, 210406. [Google Scholar] [CrossRef]
- Belalcazar, L.M.; Lang, W.; Haffner, S.M.; Schwenke, D.C.; Kriska, A.; Balasubramanyam, A.; Hoogeveen, R.C.; Pi-Sunyer, F.X.; Tracy, R.P.; Ballantyne, C.M. Improving adiponectin levels in individuals with diabetes and obesity: Insights from look AHEAD. Diabetes Care 2015, 38, 1544–1560. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, C.; Feskens, E.J.M.; Jansen, E.; Mensink, M.; Saris, W.; Blaak, E.E. Lifestyle intervention and adipokine levels in subjects at high Risk for type 2 diabetes. The study on lifestyle intervention and impaired glucose tolerance Maastricht (SLIM). Diabetes Care 2007, 30, 3125–3127. [Google Scholar] [CrossRef] [PubMed]
- Kishida, K.; Funahashi, T.; Shimomura, I. Molecular mechanisms of diabetes and atherosclerosis: Role of adiponectin. Endocr. Metab. Immune Disord. Drug Targets 2012, 12, 118–131. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Shin, H.J.; Ding, E.L.; van Dam, R.M. Adiponectin levels and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2009, 302, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Sweeney, G. Mechanisms regulating energy metabolism by adiponectin in obesity and diabetes. Biochem. Soc. Trans. 2006, 34, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Achari, A.E.; Jain, S.K. Adiponectin, a therapeutic target for obesity, diabetes, and endothelial dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.; Ruan, Y.; Gao, X.; Sun, J. Systematic review and meta-analysis of randomized, controlled trials on the effect of exercise on serum leptin and adiponectin in overweight and obese individuals. Horm. Metab. Res. 2017, 49, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Hayashino, Y.; Jackson, J.L.; Hirata, T.; Fukumori, N.; Nakamura, F.; Fukuhara, S.; Tsujii, S.; Ishii, H. Effects of exercise on C-reactive protein, inflammatory cytokine and adipokine in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Metabolism 2014, 63, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Baile, C.A.; Della-Fera, M.A.; Martin, R.J. Regulation of metabolism and body fat mass by leptin. Ann. Rev. Nutr. 2000, 20, 105–127. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Hanefeld, M.; Haffner, S.M.; Fusch, C.; Schwanebeck, U.; Kohler, C.; Fucker, K.; Julius, U. Insulin-resistant patients with type 2 diabetes mellitus have higher serum leptin levels independently of body fat mass. Acta Diabetol. 2002, 39, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Qasim, A.; Reilly, M.P. Leptin resistance: A possible interface of inflammation and metabolism in obesity-related cardiovascular disease. J. Am. Coll. Cardiol. 2008, 52, 1201–1110. [Google Scholar] [CrossRef] [PubMed]
- Meek, T.H.; Morton, G.J. Leptin, diabetes, and the brain. Indian J. Endocrinol. Metab. 2012, 16, 534–542. [Google Scholar] [CrossRef]
- Zhuravlyova, L.; Sokolnikova, N. The relationship between hyperleptinemia and diastolic dysfunction in patients with diabetes mellitus type 2. Arch. Cardiovasc. Dis. Suppl. 2016, 8, 23–40. [Google Scholar] [CrossRef]
- Zhou, Y.; Rui, L. Leptin signaling and leptin resistance. Front. Med. 2013, 7, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Sallam, N.; Laher, I. Exercise modulates oxidative stress and inflammation in aging and cardiovascular diseases. Oxid. Med. Cell. Longev. 2016, 2016, 7239639. [Google Scholar] [CrossRef] [PubMed]
- Steinera, A.A.; Romanovsky, A.A. Leptin: At the crossroads of energy balance and systemic inflammation. Prog. Lipid. Res. 2007, 46, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; Dolmage, T.E.; Robles, P.G.; Brooks, D.; Goldberg, R.S. The effects of exercise modality and intensity on energy expenditure and cardiorespiratory response in adults with obesity and treated obstructive sleep apnoea. Chron. Respir. Dis. 2017, 14, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Willis, L.H.; Slentz, C.A.; Bateman, L.A.; Shields, T.; Piner, L.W.; Bales, C.W.; Houmard, J.A.; Kraus, W. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J. Appl. Physiol. 2012, 113, 1831–1837. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Sample Size; % Female | Age (Years, Mean ± SD) | BMI (kg/m2, Mean ± SD) | Medical Condition | Training Sessions/Week | Intervention Duration in Weeks | Training Characteristics | Dietary Co-Intervention | Change in Outcomes as Compared to Baseline (Mean ± SD) † |
|---|---|---|---|---|---|---|---|---|---|
| Concurrent Exercise | |||||||||
| Annibalini, 2017 [38] | 16; 0% | I: 57 ± 9.1, C: 60 ± 6.8 | I: 28.3 ± 1.5, C: 29.0 ± 3.8 | T2D | 3 | 16 | Aerobic: 40–65% VO2max, 30–60 min; Resistance: 2–4 sets of 12–20 repetitions, 40% to 60% of 1-RM | No | Leptin: I: −0.1 ± 0.95, C: −0.1 ± 1.4 |
| Balducci, 2010 [39] | 42; I: 36.4%, C: 45% | I: 60.6 ± 9.3, C: 61.1 ± 7.1 | I: 30.5 ± 0.9, C: 30.9 ± 1.1 | T2D | 2 | 52 | Aerobic: 70–80% VO2max, 40 min; Resistance: 80% 1-RM, 40 min | No | Adiponectin: I: 5.54 ± 3.6, C: 0 ± 3.6; leptin: I: −7.29 ± 8.33, C: −2.08 ± 8.33 |
| Jorge, 2011 [40] | 24; I: 66.6%, C: 66.6% | I: 57.90 ± 9.82, C: 53.41 ± 9.82 | I: 31.24 ± 3.88, C: 29.59 ± 4.90 | T2D | 3 | 12 | Aerobic: 30 min, intensity set individually acc. to lactate threshold; Resistance: 30 min, circuit training with 7 exercises | No | Adiponectin: I: 0.6 ± 4.76, C: −1.32 ± 4.76 |
| Loimaala, 2009 [41] | 48; 0% | I: 53.6 ± 6.2, C: 54.0 ± 5.0 | I: 29.3 ± 3.7; 29.8 ± 3.6 | T2D | 4 | 104 | Aerobic: 70–80% VO2max, at least 30 min; Resistance: 3–4 sets with 10–12 repetitions, 80% 1-RM, at least 30 min | No | Leptin: I: −0.7 ± 3.9, C: 0.5 ± 3.6 |
| Mendham, 2013 [42] | 21; 0% | I: 39.5 ± 10.6, C: 36.1 ± 16.1 | I: 31.6 ± 3.1, C: 34.5 ± 6.6 | T2D | 3 | 12 | 45 min sessions; Aerobic: 80–85% VO2max; Resistance: free-weights training with 3 exercises; additional boxing session | No | Adiponectin: I: −1.1 ± 3.71, C: −0.2 ± 2.96 leptin: I: −5.71 ± 7.7, C: 0.49 ± 15.06 |
| Okada, 2010 [43] | 38; I: 52.3%, C: 35.3% | I: 61.9 ± 8.6, C: 64.5 ± 5.9 | I: 25.7 ± 3.2, C: 24.5 ± 2.9 | T2D | 3–5 | 12 | Aerobic: 40 min, Resistance: 20 min | No | Adiponectin: I: 1.9 ± 3.89, C: 1.8 ± 3.25 leptin: I: 1.2 ± 3.3, C: 1.4 ± 4.9 |
| Aerobic Exercise | |||||||||
| Aas, 2005 [44] | 18; I: 33.3%, C: 33.3% | I: 59 (45–67), C: 53 (39–66)a | I: 29.8 (26.7–34.5), C: 30.0 (25.8–31.0)a | T2D | 2 | 52 | 60 min, moderate intensity | Hypocaloric diet aimed at weight loss and improved metabolic control | Adiponectin: I: −1.4 ± 0.95, C: −1.1 ± 2.97 leptin: I: −1.17 ± 1.16, C: 3.17 ± 1.44 |
| Balducci, 2010 [39] | 40; 40% | I: 64.3 ± 8.1, C: 61.1 ± 7.1 | I: 29.4 ± 1.1, C: 30.9 ± 1.1 | T2D | 2 | 52 | 70–80% VO2max, 60 min | No | Adiponectin: I: 5.97 ± 3.6, C: 0 ± 3.62 leptin: I: −4.17 ± 8.33, C: −2.08 ± 8.33 |
| Boudou, 2003 [45] | 16; 0% | I: 42.90 ± 5.20, C: 47.9 ± 8.35 | I: 28.3 ± 3.90, C: 27.6 ± 4.30 | T2D | 3 | 8 | 2 sessions with continuous intensity: 75% VO2max (45 min), 1 session with alternating intensity: 50–85% VO2max (20 min) | No | Adiponectin: I: −0.3 ± 3.19, C: −0.25 ± 2.36, leptin: I: −0.45 ± 4.45; C: 0.14 ± 3.9 |
| Dede, 2015 [46] | 60; I: 50%; C: 53.3% | I: 52.5 ± 7.5, C: 55.5 ± 8.4 | I: 30.8 ± 4.6, C: 30.2 ± 4.5 | T2D | 3 | 12 | Sessions progressed from 15–20 min at 60% of VO2max to 45 min at 75% of VO2max | No | Adiponectin: I: −0.6 ± 0.8, C: −0.2 ± 1.1 leptin: I: −2.8 ± 19.79, C: 1.3 ± 17.16 |
| Giannopoulou, 2005 [47] | 22; 100% | 55.5 ± 1.7 | 35.9 ± 1.9 | T2D | 3–4 | 14 | 65–70% VO2max, 60 min | No | Adiponectin: I: 1.8 ± 1.37, C: 1.2 ± 1.95 leptin: I: −15.6 ± 8.77, C: −9.8 ± 8.77 |
| Iishi, 2001 [48] | 50; I: 60.9%; C: 59.3% | I: 56.0 ± 4.6, C: 57.9 ± 7.6 | I: 26.2 ± 3.5, C: 25.4 ± 3.2 | T2D | 5 | 6 | 50% VO2max, 60 min | 25- to 27-kcal/kg/d (54% to 58% carbohydrate, 22% to 24% protein, 18% to 20% fat) | Leptin: I: −2.6 ± 0.77, C: −1.1 ± 0.62 |
| Jorge, 2011 [40] | 24; I: 58.3%, C: 66.6% | I: 52.09 ± 8.71, C: 53.41 ± 9.82 | I: 29.30 ± 2.09, C: 29.59 ± 4.90 | T2D | 3 | 12 | Intensity set individually acc. to lactate threshold, 60 min | No | Adiponectin: I: 2.2 ± 5.0, C: −1.32 ± 4.76 |
| Kadoglou, 2007a [49] | 60; I: 56.6%, C: 60% | I: 59.33 ± 4.76, C: 63.82 ± 7.03 | I: 32.1 ± 3.19, C: 31.99 ± 3.41 | T2D | 4 | 26 | 50–75% VO2max, 30–45 min | No | Adiponectin: I: −0.24 ± 0.95, C: 0.35 ± 0–93 |
| Kadoglou, 2007b [50] | 46; I: 65.21%, C: 60.86% | I: 56.91 ± 7.09, C: 60.32 ± 9.28 | I: 31.14 ± 3.58, C: 28.96 ± 1.03 | T2D | 4 | 32 | 50–80% VO2max, 45–60 min | No | Adiponectin: I: 0.33 ± 1.15, C: −0.6 ± 0.8 |
| Ku, 2010 [51] | 31; 100% | I: 55.7 ± 7.0, C: 57.8 ± 8.1 | I: 27.1 ± 2.4, C: 27.4 ± 2.8 | T2D | 5 | 12 | 3.6–5.2 METs (1 MET = 3.5 mL O2/kg/min), 60 min | No | Adiponectin: I: 2.9 ± 2.32, C: 1.99 ± 2.06 leptin: I: −3.73 ± 3.1, C: −0.1 ± 3.52 |
| Marcell, 2005 [52] | 34; 60.7% | I: 44.4 ± 6.5, C: 44.1 ± 9.5 | I: 32.5 ± 5.3, C: 35.3 ± 3.7 | IR | 5 | 16 | 80–90% of age-predicted maximum heart rate (220 − age), 30 min | No | Adiponectin: I: 0.9 ± 1.0, C: −1.9 ± 1.1 |
| Rokling-Andersen, 2007 [53] | 85; 0% | 45.1 ± 2.51 | I: 28.5 ± 3.3, C: 28.5 ± 3.3 | IFG, IGT | 3 | 52 | 60–80% of measured maximum heart rate, 60 min | No | Adiponectin: I: −0.5 ± 7.35, C: −4.1 ± 8.82 leptin: I: −0.5 ± 4.7, C: 1.0 ± 7.61 |
| Thompson, 2014 [54] | 494; I: 66.0%, C: 64.0% | I: 60 ± 10, C: 60 ± 10 | I: 31.6 ± 5.6, C: 31.5 ± 5.7 | T2D | 5 | 52 | Low-intensity walking, 30 min | Hypocaloric diet aiming to produce 5–10% weight loss | Adiponectin: I: 0.96 ± 0.24, C: 0.5 ± 0.04 |
| Zhang, 2017 [55] | 32; I: 58,8%, C: 46,6% | I: 47.2 ± 10.5, C: 46.9 ± 11.1 | I: 27.6 ± 3.2, C: 27.9 ± 3.8 | T2D | 5 | 12 | 70% of age-predicted maximum heart rate (220 − age), 60 min | No | Adiponectin: I: 1.2 ± 1.81, C: 0.4 ± 1.95 leptin: I: −3.3 ± 6.57, C: −2.1 ± 7.7 |
| Resistance Exercise | |||||||||
| Brooks, 2007 [56] | 62; I: 32.2%, C: 38.7% | I: 66 ± 2, C: 66 ± 1 | I: 30.9 ± 1.1, C: 31.2 ± 1.0 | T2D | 3 | 16 | 60–80% of 1-RM, 3 sets with 8 repetitions, 35 min | No | Adiponectin: I: 2.3 ± 2.09, C: 1.99 ± 2.06 |
| Jorge, 2011 [40] | 24; I: 58.3%, C: C: 66.6% | I: 54.10 ± 8.94, C: 53.41 ± 9.82 | I: 31.29 ± 4.08, C: C: 29.59 ± 4.90 | T2D | 3 | 12 | 60 min, circuit training with 7 exercises | No | Adiponectin: I: 0.68 ± 4.21, C: −1.32 ± 4.76 |
| Ku, 2010 [51] | 29; 100% | I: 55.7 ± 6.2, C: 57.8 ± 8.1 | I: 27.1 ± 2.3, C: 27.4 ± 2.8 | T2D | 5 | 12 | Elastic band exercises with 40–50% of maximal exercise capacity, 3 sets with 15–20 repetitions | No | Adiponectin: I: 2.3 ± 2.09, C: 1.99 ± 2.06 leptin: I: −1.02 ± 2.89, C: −0.1 ± 3.52 |
| Lovrencic, 2015 [57] | 140; I: 56.1%; C: 54.1% | I: 58.5 ± 4.8, C: 57.7 ± 6.2 | I: 29.44 (4.67), C: 30.64 (4.54) | T2D | 6 | 52 | Strength exercises with light to medium intensity, 90 min | No | Adiponectin: I: −0.1 ± 6.42, C: −0.4 ± 3.31 |
| Exercise Advice | |||||||||
| Balducci, 2009 [39] | 40; 45% | I: 62.5 ± 7.1, C: 61.1 ± 7.1 | I: 30.0 ± 1.0, C: 30.9 ± 1.1 | T2D | NA | 52 | Counseling to perform low-level aerobic physical activity regularly | No | Adiponectin: I: −0.43 ± 6.63, C: 0 ± 3.6 leptin: I: −1.04 ± 2.89, C: −0.1 ± 3.52 |
| Belalcazar, 2015 [58] | 1397; I: 57%, C: 57% | I: 57.1 ± 7.1, C: 57.3 ± 7.3 | I: 36.4 ± 6.4, C: 36.0 ± 5.9 | T2D | NA | 52 | Advice to increase moderate intensity physical activity to at least 175 min per week | Hypocaloric diet aiming at 7% weight loss, 1200–1500 kcal/day if body weight <114 kg, 1500–1800 kcal/day if body weight ≥114 kg | Adiponectin: I: 0.5 ± 0.53, C: 0 ± 0.43 |
| Corpeleijn, 2007 [59] | 103; 45.5% | I: 55.6 ± 0.9, C: 57.8 ± 1.0 | I: 29.8 ± 0.5, C: 29.3 ± 0.4 | IGT | NA | 52 | Advice to perform 30 min of moderate intensity physical activity at least 5 times per week | Hypocaloric diet aiming at 5–7% weight loss, carbohydrate intake of at least 55% of total energy intake; total fat of 30 to 35% of total energy intake, with <10% energy intake of saturated fatty acids and cholesterol intake of <33 mg/MJ; protein 10 to 15% of total energy; dietary fiber at least 3 g/MJ | Adiponectin: I: −0.06 ± 0.63, C: −0.03 ± 0.55 leptin: I: −2.37 ± 1.3, C: 0.06 ± 0.93 |
| Adiponectin | Leptin | |||
|---|---|---|---|---|
| MD (95% CI), p-Value, I2-Value | Test for Subgroup Differences | MD (95% CI), p-Value, I2-Value | Test for Subgroup Differences | |
| Intervention duration | ||||
| ≤12 weeks | 0.12 (0.02, 0.29), p = 0.57, I2 = 0% | p = 0.0009, I2 = 85.2% | −1.50 (−1.88, −1.12), p < 0.00001, I2 = 0% | p = 0.05, I2 = 74.7% |
| >12 weeks | 0.49 (0.29, 0.68), p < 0.00001, I2 = 88% | −2.69 (−3.79, −1.58), p < 0.00001, I2 = 46% | ||
| Dietary co-intervention | ||||
| Yes | 0.40 (0.28, 0.51), p < 0.00001, I2 = 85% | p = 0.11, I2 = 60.2% | −2.60 (−3.72, −1.47), p < 0.00001, I2 = 92% | p = 0.01, I2 = 83.6% |
| No | 0.99 (0.27, 1.71), p = 0.007, I2 = 82% | −0.87 (−1.65, −0.09), p = 0.03, I2 = 0% | ||
| Training sessions/week | ||||
| ≤3 times/week | 1.70 (0.29, 3.12), p = 0.02, I2 = 76% | p = 0.24, I2 = 28.1% | −2.27 (−4.49, −0.05), p = 0.05, I2 = 75% | p = 0.68, I2 = 0% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becic, T.; Studenik, C.; Hoffmann, G. Exercise Increases Adiponectin and Reduces Leptin Levels in Prediabetic and Diabetic Individuals: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Med. Sci. 2018, 6, 97. https://doi.org/10.3390/medsci6040097
Becic T, Studenik C, Hoffmann G. Exercise Increases Adiponectin and Reduces Leptin Levels in Prediabetic and Diabetic Individuals: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medical Sciences. 2018; 6(4):97. https://doi.org/10.3390/medsci6040097
Chicago/Turabian StyleBecic, Tarik, Christian Studenik, and Georg Hoffmann. 2018. "Exercise Increases Adiponectin and Reduces Leptin Levels in Prediabetic and Diabetic Individuals: Systematic Review and Meta-Analysis of Randomized Controlled Trials" Medical Sciences 6, no. 4: 97. https://doi.org/10.3390/medsci6040097
APA StyleBecic, T., Studenik, C., & Hoffmann, G. (2018). Exercise Increases Adiponectin and Reduces Leptin Levels in Prediabetic and Diabetic Individuals: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medical Sciences, 6(4), 97. https://doi.org/10.3390/medsci6040097