Integrated FISH, Karyotyping and aCGH Analyses for Effective Prenatal Diagnosis of Common Aneuploidies and Other Cytogenomic Abnormalities

Abstract
:1. Introduction
2. Materials and Methods
3. Cytogenomic Results
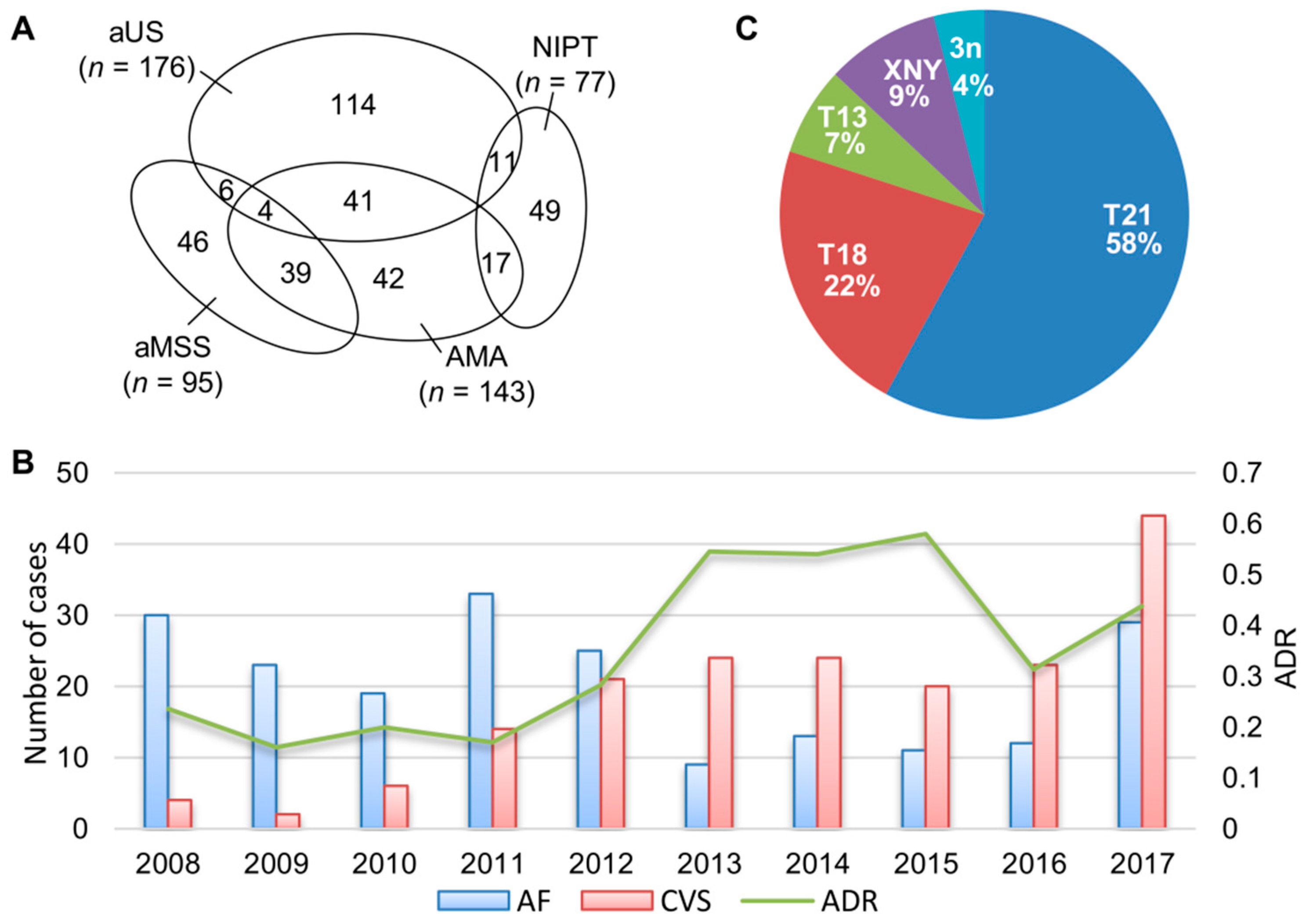
3.1. Clinical Indications and Common Aneuploidies Detected
3.2. Cases with Mosaic Patterns
3.3. Chromosomal Structural Abnormalities and Pathogenic Copy Number Variants
4. Discussion
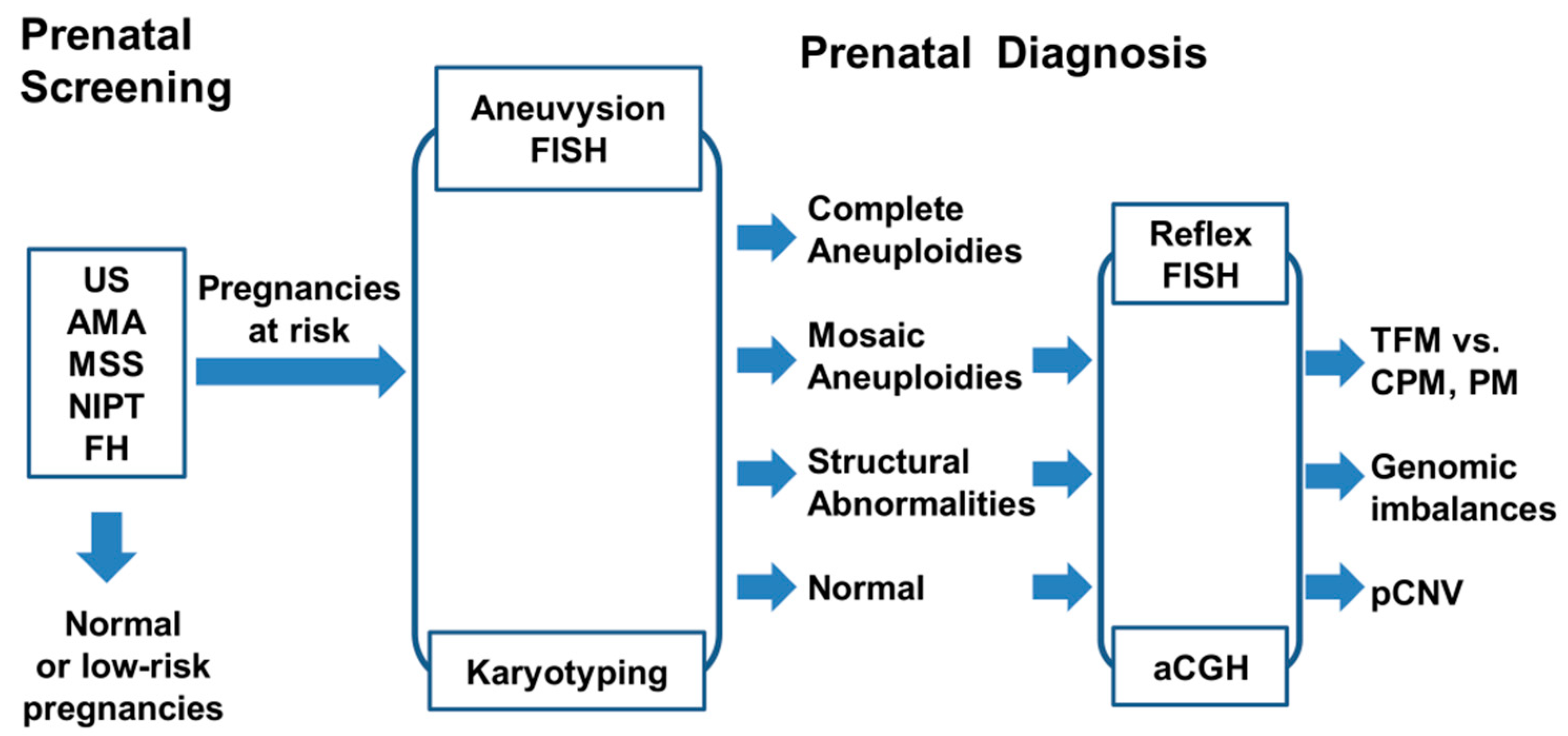
- Aneuvysion FISH provides a quick and reliable testing of common aneuploidies. Once a mosaic pattern is detected, a reflex FISH test using targeted locus-specific probes should be considered to confirm the mosaic pattern in directly prepared cells and to verify the inconsistent findings from cultured cells. The cut-off value and frequencies of false positive and false negative from FISH tests should be monitored carefully [24,25]. Abnormal results detected by a quick FISH test should be interpreted with cautions and communicated clearly with genetic counselors and physicians. It is important to have a disclaimer clearly state that false positive or negative results as well as maternal cell contamination have been demonstrated in prenatal FISH analysis; the American College of Medical Genetics recommends that irreversible therapeutic action should not be initiated on the basis of FISH results alone.
- Karyotyping is still a valuable method on detecting common aneuploidies, balanced or unbalanced structural rearrangements, and mosaic patterns. Follow up amniocentesis should always be recommended on mosaic findings from CVS. However, the low analytical resolution by G-banding and the limitation on resolving low-level mosaicism should be taken into consideration.
- Efforts should be applied to resolve pseudo-mosaicism, CPM, and TFM in prenatal diagnosis [9,10,11]. Technically, additional workup to define the level I, II, and III of mosaicism should be performed according to the laboratory protocol and documented in the worksheet. The distinction of pseudo-mosaicism, CPM, and TFM should be based on completed chromosome and FISH results. Pseudo-mosaicism by culture artifact and variant mosaic patterns introduced by in vitro cell culture should be resolved by a reflex FISH preferably in uncultured cells. Technical limitations in analyzing low level mosaic patterns should be described clearly [14]. Complete chromosome and aneuvysion FISH results and adequate interpretation should be provided in a timely fashion.
- Reporting of mosaic patterns should be based on laboratory findings and current evidence. Current survey indicated that CPM and TFM accounted for 86% and 14% of prenatal mosaic cases, respectively. It was estimated that the risk of finding a mosaicism in CVS after a high-risk cell free DNA test result for trisomy 21, trisomy 18, trisomy 13, and monosomy X is 2%, 4%, 22%, and 59%, respectively. After the detection of a mosaic pattern in CVS, the likelihood of fetal confirmation for trisomy 21, trisomy 18, trisomy 13 and monosomy X is 44%, 14%, 4%, and 26%, respectively [11]. A web-based database for chromosome mosaicism (http://mosaicism.bcchr.ca/) could also be helpful in interpreting mosaic findings. Prenatal mosaic findings should be reported and communicated directly to genetic counselors and referring physicians.
- The aCGH should be performed for cases with abnormal structural chromosomal rearrangements and normal chromosome findings. Any pCNV detected by aCGH should be confirmed by a reflex FISH using targeted locus-specific probes. The clinical significance of pCNV should be interpreted based on evidences from current clinical database and literature. Follow up parental study should be recommended for cases with structural chromosome rearrangements and pCNV.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sago, H. Prenatal diagnosis of chromosomal abnormalities through amniocentesis. J. Mamm. Ova Res. 2004, 21, 18–21. [Google Scholar] [CrossRef]
- Ward, B.E.; Gersen, S.L.; Carelli, M.P.; McGuire, N.M.; Dackowski, W.R.; Weinstein, M.; Sandlin, C.; Warren, R.; Klinger, K.W. Rapid prenatal diagnosis of chromosomal aneuploidies by fluorescence in situ hybridization: Clinical experience with 4500 specimens. Am. J. Hum. Genet. 1993, 52, 854–865. [Google Scholar] [CrossRef] [PubMed]
- Cui, C.; Shu, W.; Li, P. Fluorescence in situ hybridization: Cell-based genetic diagnostic and research applications. Front. Cell Dev. Biol. 2016, 4, 89. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.Y.; Geng, Q.; Luo, F.W.; Xu, F.; Li, P.; Xie, J.S. Multiplex ligation-dependent probe amplification and array comparative genomic hybridization analyses for prenatal diagnosis of cytogenomic abnormalities. Mol. Cytogenet. 2014, 7, 84. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Pomianowski, P.; DiMaio, M.S.; Florio, J.R.; Rossi, M.R.; Xiang, B.; Xu, F.; Yang, H.; Geng, Q.; Xie, J.; Mahoney, M.J. Genomic characterization of prenatally detected chromosomal structural abnormalities using oligonucleotide array comparative genomic hybridization. Am. J. Med. Genet. 2011, 155, 1605–1615. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.Y.; Xie, J.S.; Meng, J.L.; Li, P.; Pan, X.H.; Zhou, Q.H. Non-invasive prenatal diagnosis: A comparison of cell free fetal DNA (cffDNA) based screening and fetal nucleated red blood cell (fnRBC) initiated testing. N. Am. J. Med. Sci. 2013, 6, 194–199. [Google Scholar] [CrossRef]
- Al-Ibraheemi, Z.; Rosenn, B.; Porat, N.; Taylor, D.; Kalberer, M.; Nelson, Z. Changing face of invasive diagnostic testing in the era of cell-free DNA. Am. J. Perinatol. 2017, 34, 1142–1147. [Google Scholar] [CrossRef]
- Meng, J.L.; Matarese, C.; Crivello, J.; Wilcox, K.; Wang, D.; DiAdamo, A.; Xu, F.; Li, P. Changes in and efficacies of indications for invasive prenatal diagnosis of cytogenomic abnormalities: 13 years of experience in a single center. Med. Sci. Monit. 2015, 21, 1942–1948. [Google Scholar]
- Crane, J.P.; Cheung, S.W. An embryogenic model to explain cytogenetic inconsistencies observed in chorionic villus versus fetal tissue. Prenat. Diagn. 1988, 8, 119–129. [Google Scholar] [CrossRef]
- Taylor, T.H.; Gitlin, S.A.; Patrick, J.L.; Crain, J.L.; Wilson, J.M.; Griffin, D.K. The origin, mechanisms, incidence and clinical consequences of chromosomal mosaicism in humans. Hum. Reprod. Update 2014, 20, 571–581. [Google Scholar] [CrossRef]
- Grati, F.R.; Malvestiti, F.; Branca, L.; Agrati, C.; Maggi, F.; Simoni, G. Chromosomal mosaicism in the fetoplacental unit. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 42, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Xiang, B.; Li, A.; Valentin, D.; Novak, N.; Zhao, H.Y.; Li, P. Analytical and clinical validity of whole genome oligonucleotide array comparative genomic hybridization for pediatric patients with mental retardation and developmental delay. Am. J. Med. Genet. 2008, 146, 1942–1954. [Google Scholar] [CrossRef] [PubMed]
- Xiang, B.; Hemingway, S.; Qumsiyeh, M.; Li, P. CytoAccess: A relational laboratory information management system for a clinical cytogenetics laboratory. J. Assoc. Genet. Technol. 2006, 32, 168–170. [Google Scholar]
- Hook, E.B. Exclusion of chromosomal mosaicism: Tables of 90%, 95%, and 99% confidence limits and comments on use. Am. J. Hum. Genet. 1977, 29, 94–97. [Google Scholar]
- Leach, N.T.; Chudoba, I.; Stewart, T.V.; Holmes, L.B.; Weremowicz, S. Maternally inherited duplication of chromosome 7, dup(7)(p11.2p12), associated with mild cognitive deficit without features of Silver-Russell syndrome. Am. J. Med. Genet. 2007, 143A, 1489–1493. [Google Scholar] [CrossRef]
- Nagamani, S.C.; Zhang, F.; Shchelochkov, O.A.; Bi, W.; Ou, Z.; Scaglia, F.; Probst, F.J.; Shinawi, M.; Eng, C.; Hunter, J.V.; et al. Microdeletions including YWHAE in the Miller-Dieker syndrome region on chromosome 17p13.3 result in facial dysmorphisms, growth restriction, and cognitive impairment. J. Med. Genet. 2009, 36, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Coppinger, J.; McDonald-McGinn, D.; Zackai, E.; Shane, K.; Atkin, J.F.; Asamoah, A.; Leland, R.; Weaver, D.D.; Lansky-Shafer, S.; Schmidt, K.; et al. Identification of familial and de novo microduplications of 22q11.21-q11.23 distal to the 22q11.21 microdeletion syndrome region. Hum. Mol. Genet. 2009, 18, 1377–1383. [Google Scholar] [CrossRef]
- Feldman, B.; Ebrahim, S.A.D.; Gyi, K.; Flore, L.A.; Evans, M.I. Rapid confirmation of previously detected prenatal mosaicism by fluorescence in situ hybridization in interphase uncultured amniocytes. Genet. Test. 2000, 4, 61–63. [Google Scholar] [CrossRef]
- Wei, Y.; Gao, X.F.; Yan, L.Y.; Xu, F.; Li, P.; Zhao, Y.Y. Prenatal diagnosis and postnatal follow up of partial trisomy 13q and partial monosomy 10p: A case report and review of the literature. Case Rep. Genet. 2012, 821347. [Google Scholar]
- Cook, S.; Wilcox, K.; Grommisch, B.; Li, P.; Xu, F. Prenatal diagnosis of Xq26.1-q26.3 duplication in two fetuses of a woman with gonadal mosaicism. N. Am. J. Med. Sci. 2014, 7, 176–179. [Google Scholar]
- DiMaio, S.M.; Yang, H.; Mahoney, M.; McGrath, J.; Li, P. Familial GPC3 and GPC4-TFDP3 deletions at Xq26 associated with Simpson-Golabi-Behmel syndrome. Meta Gene 2017, 11, 147–151. [Google Scholar] [CrossRef]
- Li, P.; DiAdamo, A.; Grommisch, B.; Boyle, J.; Amato, K.; Wang, D.; Chai, H. Diagnostic yield of cytogenomic abnormalities in current prenatal diagnosis: A retrospective analysis in a clinical cytogenetics laboratory. N. Am. J. Med. Sci. 2016, 9, 136–140. [Google Scholar]
- Wei, Y.; Xu, F.; Li, P. Technology-driven and evidence-based genomic analysis for integrated pediatric and prenatal genetic evaluation. J. Genet. Genomics 2013, 40, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Liehr, T.; Ziegler, M. Rapid prenatal diagnostics in the interphase nucleus: Procedure and cut-off rates. J. Histochem. Cytochem. 2005, 53, 289–291. [Google Scholar] [CrossRef]
- Tepperberg, J.; Pettenati, M.J.; Rao, P.N.; Lese, C.M.; Rita, D.; Wyandt, H.; Gersen, S.; White, B.; Schoonmaker, M.M. Prenatal diagnosis using interphase fluorescence in situ hybridization (FISH): 2-year multi-center retrospective study and review of the literature. Prenat. Diagn. 2001, 21, 293–301. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Trisomy 21 | Trisomy 18 | Trisomy 13 | 45,X | 47,XXX | 47,XXY | 47,XYY | 69,XXX | Total | |
|---|---|---|---|---|---|---|---|---|---|
| NIPT | 38 * | 11 | 3 | 7 | 1 | 1 | 1 | 1 | 63 |
| FISH | 33 | 11 | 3 | 3 ** | 1 | 0 | 1 | 1 | 53 |
| Karyotyping | 33 | 11 | 3 | 2 | 1 | 0 | 1 | 1 | 52 |
| Case No. | Sample | Karyotype Results | Aneuvysion FISH Results |
|---|---|---|---|
| 1 | AF | mos 47,XY,+21[15]/46,XY[2] | nuc ish(DXZ1x1,DYZ3x1,D18Z1x2)[40] nuc ish(RB1x2,D21S259x3)[41/50]/(RB1,D21S259)x2[9/50] |
| 2 | CV | mos 47,XX,+21[12]/46,XX[3] | nuc ish(DXZ1,D18Z1)x2[100] nuc ish(RB1x2,D21S259x3)[75/100]/(RB1,D21S259)x2[25/100] |
| 3 | CV | mos 47,XY,+21[2]/45,XY,-21[12]/46,XY[1] nuc ish(ETV6x2,RUNX1x3)[56/200]/(ETV6x2,RUNX1x1)[113/200] | nuc ish(DXZ1x1,DYZ3x1,D18Z1x2)[100] nuc ish(RB1x2,D21S259x3)[96/100]/(RB1,D21S259)x2[4/100] |
| 4 | CV | mos 47,XX,+21[17]/47,XX,+5[3] | nuc ish(DXZ1,D18Z1)x2[30], nuc ish(RB1x2,D21S259x3)[30] |
| 5 | AF | mos 47,XX,+21[4]/46,XX[11] | nuc ish(RB1,D21S259)x2[195/200]/(RB1x2,D21S259x3)[5/200] |
| 6 | CV | mos 46,XY,i(18)(q10)[7]/46,XY[8] | nuc ish(DXZ1x1,DYZ3x1,D18Z1x2)[50] nuc ish(RB1,D21S259)x2[100] |
| 7 | CV | mos 47,XY,+18[2]/46,XY[48] | nuc ish(DXZ1x1,DYZ3x1,D18Z1x2)[88/100]/(DXZ1x1,DYZ3x1,D18Z1x3)[12/100] nuc ish(RB1x2,D21S259)x2[30] |
| AF | 46,XY.nuc ish(IGH,BCL2)x2[200] | nuc ish(DXZ1x1,DYZ3x1,D18Z1x2)[49/60]/(DXZ1x1,DYZ3x1,D18Z1x3)[11/60] | |
| 8 | CV | mos 47,XX,+13[6]/46,XX[14] | nuc ish(RB1x3,D21S259x2)[46/50]/(RB1,D21S259)x2[4/50] |
| 9 | CV | mos 45,X[5]/46,XX[15] | nuc ish(DXZ1x2)[252/300]/(DXZ1x1)[48/300] |
| 10 | CV | mos 45,X[6]/46,XX[14] | nuc ish(DXZ1x1,D18Z1x2)[7/100]/(DXZ1,D18Z1)x2[93/100] nuc ish(RB1,D21S259)x2[100] |
| 11 | CV | mos 45,X[4]/47,XXX[16] | nuc ish(DXZ1,D18Z1)x2[8/100]/(DXZ1x1,D18Z1x2)[69/100]/(DXZ1x3,D18Z1x2)[23/100] nuc ish(RB1,D21S259)x2[75] |
| 12 | AF | mos 45,X[20]/47,XXX[1] | nuc ish(DXZ1x1,D18Z1x2)[16/25]/(DXZ1x3,D18Z1x2)[9/25] nuc ish(RB1,D21S259)x2[25] |
| 13 | CV | 46,XX | nuc ish(DXZ1x2,D18Z1x2)[38/100]/(DXZ1x1,D18Z1x2)[62/100] |
| Case No. | Sample | Chromosome Results | Reflex Locus-Specific FISH Results | aCGH Results (hg19) |
|---|---|---|---|---|
| 14 | AF | 46,XX,t(4;19)(q25;q13.3)pat | ||
| 15 | AF | 46,XY,t(6;17)(p21.1;q24)dn | ||
| 16 | CV | 46,XX,t(9;21)(p23;q21)dn | ||
| 17 | AF | 46,XX,der(5)t(5;7)(p15.3;q21.1)mat | ||
| 18 | CV | 46,XY,dup(7)(p11.2p12.1)pat | arr 7p12.1p11.2(51,277,556-57,809,908)x3pat | |
| 19 | AF | 46,XX | nuc ish(PAFAH1B1x1,RAI1x2)[25] | arr 17p13.3p13.2(1,078,112-3,566,410)x1 |
| 20 | CV | 46,XY,der(22)t(16;22)(p12.2;q13.31)pat | ish der(22)t(16;22)(TBX1+,SHANK3-)[25] | arr 16p13.3p12.2(96,766-22,645,765)x3, 22q13.31q13.33(44,505,356-51,193,680)x1 |
| 21 | AF | 46,XY | ish del(22)(q11.21q11.21)(TBX1-,SHANK3+)[25] | arr 22q11.21(18,894,835-21,025,713)x1 |
| 22 | AF | 46,XX | nuc ish(ABL1x2,BCRx3)[200] | arr 22q11.21q11.23(21,808,950-24,643,108)x3dn |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chai, H.; DiAdamo, A.; Grommisch, B.; Boyle, J.; Amato, K.; Wang, D.; Wen, J.; Li, P. Integrated FISH, Karyotyping and aCGH Analyses for Effective Prenatal Diagnosis of Common Aneuploidies and Other Cytogenomic Abnormalities. Med. Sci. 2019, 7, 16. https://doi.org/10.3390/medsci7020016
Chai H, DiAdamo A, Grommisch B, Boyle J, Amato K, Wang D, Wen J, Li P. Integrated FISH, Karyotyping and aCGH Analyses for Effective Prenatal Diagnosis of Common Aneuploidies and Other Cytogenomic Abnormalities. Medical Sciences. 2019; 7(2):16. https://doi.org/10.3390/medsci7020016
Chicago/Turabian StyleChai, Hongyan, Autumn DiAdamo, Brittany Grommisch, Jennifer Boyle, Katherine Amato, Dongmei Wang, Jiadi Wen, and Peining Li. 2019. "Integrated FISH, Karyotyping and aCGH Analyses for Effective Prenatal Diagnosis of Common Aneuploidies and Other Cytogenomic Abnormalities" Medical Sciences 7, no. 2: 16. https://doi.org/10.3390/medsci7020016
APA StyleChai, H., DiAdamo, A., Grommisch, B., Boyle, J., Amato, K., Wang, D., Wen, J., & Li, P. (2019). Integrated FISH, Karyotyping and aCGH Analyses for Effective Prenatal Diagnosis of Common Aneuploidies and Other Cytogenomic Abnormalities. Medical Sciences, 7(2), 16. https://doi.org/10.3390/medsci7020016