Learning to Learn: towards a Relational and Transformational Model of Learning for Improved Integrated Care Delivery

Abstract
:1. Introduction
2. Theoretical Framework: Complex Adaptive Systems
3. Learning to Learn (L2L) for Improved Integrated Care Delivery

{kind=link}
| TERM | DESCRIPTION |
|---|---|
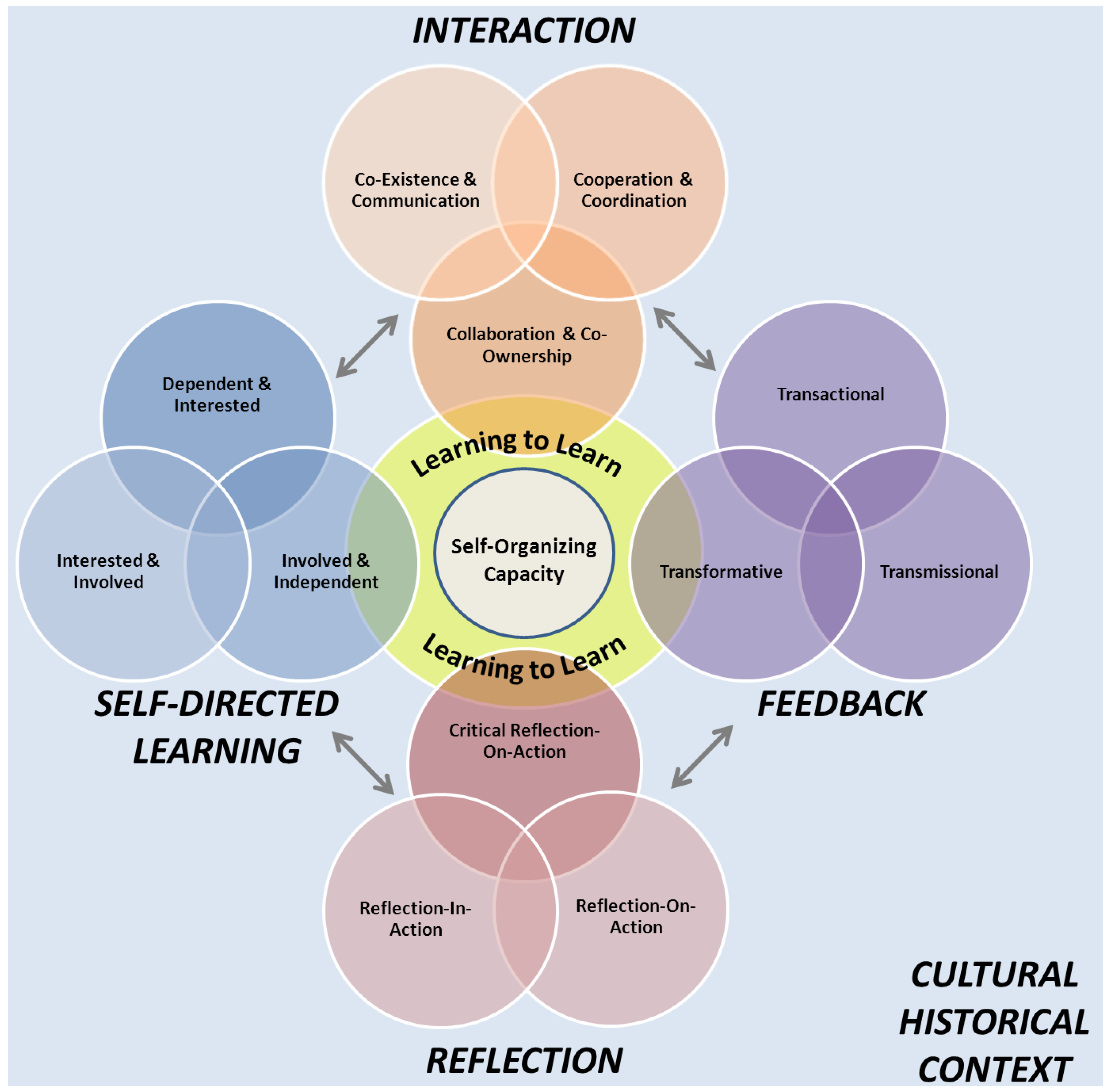
| Learning to Learn (L2L) | an ongoing nonlinear process by which learners achieve meta-cognition (the capacity to monitor, evaluate and change how one thinks and learns) |
| Interaction [92] | |
| Co-Existence & Communication | minimal interaction and early efforts to get to know one another |
| Cooperation & Coordination | working together towards shared goals within defined parameters |
| Collaboration & Co-ownership | high degree of commitment and investment, shared responsibility, and a willingness to work outside of traditional rules or norms for mutual benefit |
| Reflection [93] | |
| Reflection-in-Action | rapid reaction, which often results in a temporary solution or way of dealing with a situation or problem; usually personal and private |
| Reflection-on-Action | observation and analysis followed by action to improve the situation or solve the problem; usually interpersonal and collegial |
| Critical Reflection-on-Action | Observation, research, evaluation and theory-testing on an ongoing basis; usually interpersonal and collegial |
| Self-Directed Learning [94] | |
| Dependent & Interested | requires external direction and support, responds to motivational techniques |
| Interested & Involved | engages in learning independently, but facilitation is required to help develop confidence, sense of direction, and ability to work with and learn from others |
| Involved & Independent | sets goals and standards, continually self-assesses with or without external help, seeks resources to support learning, and willing and able to take responsibility for personal learning and productivity |
| Feedback [48,95,96] | |
| Transmissional | transmitted by an authority (knowledge is disconnected and replicated in practice) |
| Transactional | acquired through application, experience, and interaction (connections are made and relationships are appreciated) |
| Transformative | used to actively create and co-create new frames of reference (connections are understood as a whole and reconceptualised) |
3.1. Interaction
3.2. Feedback
3.3. Reflection
3.4. Self-Directed Learning
4. Discussion and Conclusions
Conflict of Interest
References
- Ham, C.; Curry, N. Clinical and Service Integration: The Route to Improved Outcomes; The King’s Fund: London, UK, 2010. [Google Scholar]
- Shortell, S.; Gillies, R.; Anderson, D.; Mitchell, J.; Morgan, K. Creating organized delivery systems: The barriers and facilitators. Hosp. Health Serv. Adm. 1993, 38, 447–466. [Google Scholar]
- Singer, S.; Burgers, J.; Friedberg, M.; Rosenthal, M.; Leape, L.; Schneider, E. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Med. Care Res. Rev. 2011, 68, 112–127. [Google Scholar] [CrossRef]
- Glouberman, S.; Mintzberg, H. Managing the care of health and the cure of disease—Part 1: Differentiation. Health Care Manage. Rev. 2001, 26, 56–69. [Google Scholar] [CrossRef]
- Orlikowski, W. Knowing in practice: Enacting a collective capability in distributed organizing. Organ. Sci. 2002, 13, 249–273. [Google Scholar] [CrossRef]
- Wenger, E. Communities of practice: Learning as a social system. Syst. Thinker 1998, 9, 225–246. [Google Scholar]
- Anand, N.; Gardner, H.; Morris, T. Knowledge-based innovation: Emergence and Embedding of new practice areas in management consulting firms. Acad. Manage. J. 2007, 50, 406–428. [Google Scholar] [CrossRef]
- Barnsley, J.; Lemieux-Charles, L.; McKinney, M. Integrating learning into integrated delivery systems. Health Care Manage. Rev. 1998, 23, 18–28. [Google Scholar] [CrossRef]
- Evans, J.; Baker, R. Shared mental models of integrated care: Aligning multiple stakeholder perspectives. J. Health Organ. Manag. 2012, 26, 713–736. [Google Scholar] [CrossRef]
- van Wijngaarden, J.; de Bont, A.; Huijsman, R. Learning to cross boundaries: The integration of a health network to deliver seamless care. Health Pol. 2006, 79, 203–213. [Google Scholar] [CrossRef]
- Fincham, R.; Forbes, T. Inter-professional Rivalry and Knowledge Integration: Problems in the Delivery of Integrated Mental Health Care. In Proceedings of ProPEL Conference: Professions and Professional Learning in Troubling Times: Emerging Practices and Transgressive Knowledges, Stirling, UK, 9–11 May 2012; Stirling University.
- Visse, M.; Widdershoven, G.; Abma, T. Moral learning in an integrated social and healthcare service network. Health Care Anal. 2012, 20, 281–296. [Google Scholar] [CrossRef]
- Williams, P. Integration of health and social care: A case of learning and knowledge management. Health Soc. Care Community. 2012, 2095, 550–560. [Google Scholar]
- Kodner, D. All together now: A conceptual exploration of integrated care. Healthc. Q. 2009, 13, 6–15. [Google Scholar]
- Suter, E.; Oelke, N.; Adair, C.; Armitage, G. Ten Key principles for successful health systems integration. Healthc. Q. 2009, 13, 16–23. [Google Scholar]
- Browne, G.; Kingston, D.; Grdisa, V.; Markle-Reid, M. Conceptualization and measurement of integrated human service networks for evaluation. Int. J. Integr. Care 2007, 7, 1–6. [Google Scholar]
- Devers, K.; Shortell, S.; Gillies, R.; Anderson, D.; Mitchell, J.; Erickson, K. Implementing organized delivery systems: An integration scorecard. Health Care Manage. R. 1994, 19, 7–20. [Google Scholar]
- Gillies, R.; Shortell, S.; Anderson, D.; Mitchell, J.; Morgan, K. Conceptualizing and measuring integration: Findings from the health systems integration study. Hosp. Health Serv. Adm. 1993, 38, 467–489. [Google Scholar]
- Lukas, C.; Meterko, M.; Lowcock, S.; Donaldson-Parlier, R.; Blakely, M.; Davies, M.; Petzel, R. Monitoring the progress of system integration. Qual. Manag. Health Care 2002, 10, 1–11. [Google Scholar]
- Minkman, M.; Ahaus, K.; Fabbricotti, I.; Nabitz, U.; Huijsman, R. A quality management model for integrated care: Results of a delphi and concept mapping study. Int. J. Qual. Health C. 2008, 21, 66–75. [Google Scholar]
- Minkman, M.; Ahaus, K.; Huijsman, R. A four phase development model for integrated care services in the Netherlands. BMC Health Serv. Res. 2009, 9, 42. [Google Scholar] [CrossRef]
- Salomon, G. (Ed.) Distributed Cognitions: Psychological and Educational Considerations; Cambridge University Press: New York, NY, USA, 1993.
- McDaniel, R.; Driebe, D. Complexity Science and Health Care Managemen. In Advances in Health Care Management; Blair, J.D., Fottler, M.D., Savage, G.T., Eds.; Emerald Group Publishing: Bingley, UK, 2002; Volume 2, pp. 11–36. [Google Scholar]
- Olson, E.E.; Eoyang, G.H. Facilitating Organization Change: Lessons from Complexity Science; Jossey-Bass/Pfeiffer: San Francisco, CA, USA, 2001. [Google Scholar]
- Ferlie, E.; Fitzgerald, L.; Wood, M.; Hawkins, C. The nonspread of innovations: The mediating role of professionals. Acad. Manage. J. 2005, 48, 117–134. [Google Scholar] [CrossRef]
- Carlile, P. Transferring, Translating and transforming: An integrative framework for managing knowledge across boundaries. Organ. Sci. 2004, 15, 555–568. [Google Scholar] [CrossRef]
- Elwyn, G.; Taubert, M.; Kowalczuk, J. Sticky knowledge: A possible model for investigating implementation in healthcare contexts. Implement. Sci. 2007, 2, 44. [Google Scholar] [CrossRef]
- Swan, J.; Scarbrough, H.; Robertson, M. The construction of communities of practice in the management of innovation. Manage. Learn. 2002, 33, 477–496. [Google Scholar]
- Argyris, C. Strategy, Change and Defensive Routines; Pitma: Boston, MA, USA, 1985. [Google Scholar]
- Tsoukas, H. A dialogical approach to the creation of new knowledge in organizations. Organ. Sci. 2009, 20, 941–957. [Google Scholar] [CrossRef]
- Denis, J.; Lamothe, L.; Langley, A.; Breton, M.; Gervais, J.; Trottier, L.; Contandriopoulos, D.; Dubois, C. The reciprocal dynamics of organizing and sense-making in the implementation of major public-sector reforms. Can. Public Adm. 2009, 52, 225–248. [Google Scholar] [CrossRef]
- Friedman, L.; Goes, J. Why integrated health networks have failed. Front. Health Serv. Manage. 2001, 17, 3–54. [Google Scholar]
- Williams, P.; Sullivan, H. Faces of Integration. Int. J. Integr. Care 2009, 9, e100. [Google Scholar]
- Pate, J.; Fischbacher, M.; Mackinnon, J. Health improvement: Countervailing pillars of partnership and profession. J. Health Organ. Manag. 2010, 24, 200–217. [Google Scholar]
- Bloom, S.W. Structure and ideology in medical education: An analysis of resistance to change. J. Health Soc. Behav. 1988, 29, 294–306. [Google Scholar] [CrossRef]
- Bevan, G.; Janus, K. Why hasn’t integrated health care developed widely in the United States and not at all in England? J. Health Polit. Policy Law 2011, 36, 141–164. [Google Scholar] [CrossRef]
- Hudson, B. Ten years of jointly commissioning health and social care in England. Int. J. Integr. Care 2011, 11, e005. [Google Scholar]
- Jiwani, I.; Fleury, M. Divergent models of integration: The Canadian way. Int. J. Integr. Care 2011, 11, e018. [Google Scholar]
- Edgren, L. The meaning of integrated care: A systems approach. Int. J. Integr. Care 2008, 8, e68. [Google Scholar]
- Edgren, L.; Barnard, K. Complex adaptive systems for management of integrated care. Leadersh. Health Serv. 2012, 25, 39–51. [Google Scholar] [CrossRef]
- Nugus, P.; Carroll, K.; Hewett, D.; Short, A.; Forero, R.; Braithwaite, J. Integrated care in the emergency department: A complex adaptive systems perspective. Soc. Sci. Med. 2010, 71, 1997–2004. [Google Scholar] [CrossRef]
- Tsasis, P.; Evans, J.; Owen, S. Reframing the challenges to integrated care: A complex-adaptive systems perspective. Int. J. Integr. Care 2012, 12, e190. [Google Scholar]
- Waldrop, M. Complexity: The Emerging Science at the Edge of Order and Chaos; Simon and Shuster: New York, NY, USA, 1992. [Google Scholar]
- Plsek, P.; Greenhalgh, T. The challenge of complexity in health care. Brit. Med. J. 2001, 323, 625–628. [Google Scholar] [CrossRef]
- Stacey, R. The emergence of knowledge in organizations. Emergence 2000, 2, 23–39. [Google Scholar] [CrossRef]
- Wallis, S. Emerging order in CAS theory: Mapping some perspectives. Kybernetes 2008, 37, 1016–1029. [Google Scholar] [CrossRef]
- Vygotsky, L.S. The Collected Works of L.S. Vygotsky, Vol. 5; Rieber, R.W., Hall, M.J., Eds.; Plenum Press: New York, NY, USA, 1998. [Google Scholar]
- Edwards, A. Keynote Presentation: Theorizing the New Partnership Landscape. In Teacher Education Advancement Network and the Association for Partnership in Education Conference, London, UK, 12 March 2013; University of Cumbria.
- Capra, F. The Web of Life; Anchor Books: New York, NY, USA, 1996. [Google Scholar]
- Meek, J.; De Ladurantey, J.; Newell, W. Complex systems, governance and policy administration consequences. Emergence Complexity Organ. 2007, 9, 24–36. [Google Scholar]
- Boisot, M.; McKelvey, B. Integrating modernist and postmodernist perspectives on organizations: a complexity science bridge. Acad. Manage. Rev. 2010, 35, 415–433. [Google Scholar] [CrossRef]
- Laihonen, H. Knowledge flows in self-organizing processes. J. Knowl. Manag. 2006, 10, 27–135. [Google Scholar] [CrossRef]
- Lanham, H.; Leykum, L.; Taylor, B.; McCannon, C.; Lindberg, C.; Lester, R. How complexity science can inform scale-up and spread in health care: Understanding the role of self-organization in variation across local contexts. Soc. Sci. Med. 2012. ID: 22819737. [Google Scholar]
- Comfort, L. Self-organization in Complex Systems. J. Publ. Adm. Res. Theor. 1994, 4, 393–410. [Google Scholar]
- Begun, J.; Zimmerman, B.; Dooley, K. Health Care Organizations as Complex Adaptive Systems. In Advances in Health Care Organization Theory; Mick, S.M., Wyttenbach, M., Eds.; Jossey-Bass: San Francisco, CA, USA, 2003; pp. 253–288. [Google Scholar]
- Arrow, H.; Henry, K.B. Using complexity to promote group learning in healthcare. J. Eval. Clin. Practice 2010, 16, 861–866. [Google Scholar] [CrossRef]
- Heylighen, F. Self-organization in Communicating Groups: The Emergence of Coordination, Shared References and Collective Intelligence. In Language and Complexity; Barcelona University Press: Barcelona, Spain, 2011. [Google Scholar]
- Weick, K.E. Sensemaking in Organizations; Sage Publications: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Guastello, S.J. Self-organization and leadership emergence in emergency response teams. Nonlinear Dynamics Psychol. Life Sci. 2010, 14, 179–204. [Google Scholar]
- Griffin, D.; Shaw, P.; Stacey, R. Knowing and acting in conditions of uncertainty: A complexity perspective. Syst. Pract. Act. Res. 1999, 12, 295–309. [Google Scholar] [CrossRef]
- Kitson, A. The need for systems change: Reflections on knowledge translation and organizational change. J. Adv. Nurs. 2009, 65, 217–228. [Google Scholar] [CrossRef]
- Lindberg, C.; Schneider, M. Leadership in a Complex Adaptive System: Insights from Positive Deviance. Academy of Management Best Paper Proceedings. Boston, MA, USA, 2012. [Google Scholar]
- Suchman, A.; Sluyter, D.; Williamson, P. Leading Change in Healthcare: Transforming Organizations Using Complexity, Positive Psychology and Relationship-Centered Care; Radcliffe Publishing: London, UK, 2011. [Google Scholar]
- Greenhalgh, T.; Wieringa, S. Is it time to drop the ‘Knowledge Translation’ Metaphor? A critical review. J. R. Soc. Med. 2011, 104, 501–509. [Google Scholar] [CrossRef]
- Cook, S.D.N.; Brown, J.S. Bridging epistemologies: The generative dance between organizational knowledge and organizational knowing. Organ. Sci. 1999, 10, 381–400. [Google Scholar] [CrossRef]
- Berger, P.; Luckmann, T. The Social Construction of Reality: A Treatise in the Sociology of Knowledge; Doubleday & Company: Garden City, NY, USA, 1966. [Google Scholar]
- Bourdieu, P. Outline of a Theory of Practice; Cambridge University Press: Cambridge, UK, 1977. [Google Scholar]
- Dewey, J. Experience and Education; Kappa Delta Pi: New York, NY, USA, 1938. [Google Scholar]
- Boland, R., Jr.; Tenkasi, R. Perspective making and perspective taking in communities of knowing. Organ. Sci. 1995, 6, 350–372. [Google Scholar] [CrossRef]
- Brown, J.; Duguid, P. Organizational learning and communities-of-practice: Toward a unified view of working, learning and innovation. Organ. Sci. 1991, 2, 40–57. [Google Scholar] [CrossRef]
- Rush, L.; Diamond, J. Exploring Key Variations and Meanings in Understanding Intra-organisational Collaboration at One University. In Proceedings of SRHE Conference, Celtic Manor, UK, 12 December 2009; Birmingham City University: Birmingham, UK, 2009. [Google Scholar]
- Watkins, C. Learning about Learning Enhances Performance; Institute of Education: London, UK, 2002; Research Matters Series No. 13. [Google Scholar]
- Claxton, G. Expanding the Capacity to Learn: A New End for Education? In Proceedings of British Educational Research Association Annual Conference, Warwick University, UK, 6 September 2006.
- Vaill, P. Learning as a Way of Being: Strategies for Survival in a World of Permanent White Water; Jossey-Bass: San Francisco, CA, USA, 1996. [Google Scholar]
- Axelrod, R.; Cohen, M. Harnessing Complexity: Organizational Implications of a Scientific Frontier; Basic Books: New York, NY, USA, 2000. [Google Scholar]
- Flavell, J. Metacognition and cognitive monitoring: A new era of cognitive-developmental inquiry. Am. Psychol. 1979, 34, 906–911. [Google Scholar] [CrossRef]
- Deakin-Crick, R. Learning how to learn: The dynamic assessment of learning power. Curriculum J. 2007, 18, 135–153. [Google Scholar] [CrossRef]
- Bransford, J.; Brown, A.; Cocking, R. (Eds.) How People Learn: Brain, Mind, Experience, and School; National Academy Press: Washington, DC, USA, 2000.
- Suchman, A. A new theoretical foundation for relationship-centered care: Complex responsive processes of relating. J. Gen. Intern. Med. 2006, 21, S40–S44. [Google Scholar]
- Mezirow, J.; Marswick, V. Education for Perspective Transformation: Women’s Re-entry Programs in Community Colleges; Teachers College, Columbia University: New York, NY, 1978. [Google Scholar]
- Kegan, R. What “form” transforms? A Constructive-Developmental Approach to Transformative Learning. In Contemporary Theories of Learning: Learning Theorists in Their Own Words; Illeris, K., Ed.; Routledge: New York, NY, USA, 2009. [Google Scholar]
- Meyer, J.; Land, R. Threshold Concepts and Troublesome Knowledge: Linkages to Ways of Thinking and Practising Within the Disciplines. In Improving Student Learning: Improving Student Learning Theory and Practice—Ten Years On; Rust, C., Ed.; Oxford Centre for Staff and Learning Development: Oxford, UK, 2003. [Google Scholar]
- Rush, L. Expanding the Capacity to Learn in ITT: A Personal Reflection on Embedding and Enacting a Distinct Pedagogic Approach to Partnership Learning. In Proceedings of BERA Conference, University of Warwick, Coventry, UK, 1–3 September 2010; University of Warwick: Coventry, UK, 2010. [Google Scholar]
- Rush, L.; Diamond, J. New Professionalism and Public Sector Management: A Reflection on Collaborative Practice in UK Teacher Education. In Proceedings of XVI Annual Conference of the International Research Society for Public Management, Rome, Italy, 2012; University of Rome.
- Claxton, G. Cultivating Positive Learning Dispositions. In The Routledge Companion to Education; Daniels, H., Lauder, H., Porter, J., Eds.; Routledge: London, UK, 2008. [Google Scholar]
- Merriam, S.; Caffarella, R. Learning in Adulthood: A Comprehensive Guide, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 1999. [Google Scholar]
- Mezirow, J. Learning as Transformation: Critical Perspectives on a Theory in Progress; Jossey-Bass: San Francisco, CA, USA, 2000. [Google Scholar]
- Carley, K.; Hill, V. Structural change and learning within organizations. In Dynamics of Organizations: Computational Modeling and Organization Theories; Larsen, E.R., Ed.; MIT Press: Menlo Park, CA, USA, 2001; pp. 63–92. [Google Scholar]
- Hedegaard, M. Analyzing children’s learning and development in everyday settings from a cultural-historical wholeness approach. Mind Cult. Activ. 2012, 19, 127–138. [Google Scholar] [CrossRef]
- Vygotsky, L. Thought and Language; MIT Press: Cambridge, MA, USA, 1962. [Google Scholar]
- Vygotsky, L. Mind in Society: The Development of Higher Psychological Processes; Harvard University Press: Boston, MA, USA, 1978. [Google Scholar]
- Bailey, D.; Koney, K. Strategic Alliances among Health and Human Services Organizations: From Affiliations to Consolidations; Sage Publications: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Griffiths, M.; Tann, S. Using reflective practice to link personal and public theories. J. Educ. Teaching 1992, 18, 69–84. [Google Scholar] [CrossRef]
- Grow, G. Teaching learners to be self-directed. Adult Educ. Quart. 1991, 41, 125–149. [Google Scholar] [CrossRef]
- Miller, J.; Seller, W. Curriculum: Perspectives and Practice; Longman: New York, NY, USA, 1990. [Google Scholar]
- Biggs, J. Teaching for Quality Learning at University: What the Student Does; Society for Research into Higher Education, Open University Press: Philadelphia, PA, USA, 1999. [Google Scholar]
- Teaching and Learning in the Primary School; Pollard, A.; Bourne, J. (Eds.) Routledge: New York, NY, USA, 1994.
- Delamont, S. Interaction in the Classroom; Methuen: London, UK, 1983. [Google Scholar]
- Gajda, R. Utilizing collaboration theory to evaluate strategic alliances. Am. J. Eval. 2004, 25, 65–77. [Google Scholar]
- Stryker, S.; Statham, A. Symbolic Interaction and Role Theory. In Handbook of Social Psychology, 3rd ed.; Lindzey, G., Aronson, E., Eds.; Random House: New York, NY, 1985; Volume 1, pp. 311–378. [Google Scholar]
- Wrzesniewski, A.; Dutton, J.E.; Debebe, G. Interpersonal sensemaking and the meaning of work. Res. Organ. Behav. 2003, 25, 93–135. [Google Scholar] [CrossRef]
- Wegner, D.M.; Giuliano, T.; Hertel, P.T. Cognitive Interdependence in Close Relationships. In Compatible and Incompatible Relationships; Ickes, W.J., Knowles, E.S., Eds.; Springer-Verlag: New York, NY, 1985; pp. 253–276. [Google Scholar]
- Liang, D.; Moreland, R.; Argote, L. Group versus individual training and group performance: the mediating role of group transactive memory. Pers. Soc. Psychol. B 1995, 21, 384–393. [Google Scholar] [CrossRef]
- Weick, K.; Roberts, K. Collective mind in organizations: Heedful interrelating on flight decks. Adm. Sci. Q. 1993, 38, 357–381. [Google Scholar] [CrossRef]
- Faraj, S.; Xiao, Y. Coordination in fast response organizations. Manage. Sci. 2006, 52, 1155–1169. [Google Scholar] [CrossRef]
- Tan, J.; Wen, H.; Awad, N. Health care and service delivery systems as complex adaptive systems. Comm. ACM 2005, 48, 36–44. [Google Scholar]
- Bechky, B. Sharing meaning across occupational communities: The transformation of understanding on a production floor. Organ. Sci. 2003, 14, 312–330. [Google Scholar] [CrossRef]
- Ling, T.; Brereton, L.; Conklin, A.; Newbould, J.; Roland, M. Barriers and facilitators to integrating care: Experiences from the English integrated care pilots. Int. J. Integr. Care 2012, 12, e129. [Google Scholar]
- Reid, B. But we’re doing it already: Exploring a response to the concept of reflective practice in order to improve its facilitation. Nurs. Educ. Today 1993, 13, 305–309. [Google Scholar] [CrossRef]
- Hatton, N.; Smith, D. Reflection in teacher education: Towards definition and implementation. Teach. Teach. Educ. 1995, 11, 33–49. [Google Scholar] [CrossRef]
- Eoyang, G.; Holladay, R. Adaptive Action: Leveraging Uncertainty in Your Organization; Stanford University Press: Palo Alto, CA, USA, 2013. [Google Scholar]
- Gustafsson, C.; Fagerberg, I. Reflection, the way to professional development? J. Clin. Nurs. 2004, 13, 271–280. [Google Scholar] [CrossRef]
- Schon, D. The Reflective Practitioner: How Professionals Think in Action; Basic Books: New York, NY, USA, 1983. [Google Scholar]
- Mann, K.; Gordon, J.; MacLeoid, A. Reflection and reflective practice in health professions education: A systematic review. Adv. Health Sci. Educ. 2009, 14, 595–621. [Google Scholar] [CrossRef]
- L’Aigulle, Y. Pushing Back the Boundaries of Personal Experience. In Reflective Practice in Nursing: The Growth of the Professional Practitioner; Palmer, A.M., Burns, S., Bulman, C., Eds.; Blackwell Scientific Publications: London, UK, 1994. [Google Scholar]
- Driscoll, J. Reflective practice for practice: A framework of structured reflection for clinical areas. Sr. Nurse 1994, 13, 47–50. [Google Scholar]
- Fisher, R. Teaching Children to Think; Basil Blackwell: Oxford, UK, 1990. [Google Scholar]
- Freeman, J. Educating the Very Able: Current International Research; Ofsted Reviews of Research, Office for Standards in Education: London, UK, 1998. [Google Scholar]
- Ames, G.; Ames, K. Report on Teaching at the Center for Environmental Management and Planning. In Georgian Academy of Sciences; Department of Agricultural and Applied Economics, University of Georgia: Athens, Greece, 1993; Faculty Series FS93-06, Tbilisi, Republic of Georgia, 1–26 October 1992. [Google Scholar]
- Dweck, C.; Leggett, E. A social- cognitive approach to motivation and personality. Psychol. Rev. 1988, 95, 256–273. [Google Scholar] [CrossRef]
- Nicholls, J.G. The Competitive Ethos and Democratic Education; Harvard University Press: Cambridge, MA, USA, 1989. [Google Scholar]
- Mortimore, P. (Ed.) Understanding Pedagogy and Its Impact on Learning; Paul Chapman: London, UK, 1999.
- Colthart, I.; Bagnall, G.; Evans, A.; Allbutt, H.; Haig, A.; Illing, J.; McKinstry, B. The effectiveness of self-assessment on the identification of learner needs, learner activity, and impact on clinical practice: BEME Guide No. 10. Med. Teach. 2008, 30, 124–145. [Google Scholar]
- Bleakley, A. Social comparison, Peer learning and democracy in medical education. Med. Teach. 2010, 32, 878–879. [Google Scholar] [CrossRef]
- Bleakley, A. Broadening conceptions of learning in medical education: The message from team working. Med. Educ. 2006, 40, 150–157. [Google Scholar] [CrossRef]
- Eva, K.; Regehr, G. Self-assessment in the health professions: A reformulation and research agenda. Acad. Med. 2005, 80, S46–S54. [Google Scholar] [CrossRef]
- Benneworth, P. Leading Innovation: Building Effective Regional Coalitions for Innovation; NESTA: London, UK, 2007. [Google Scholar]
- Harris, A. Distributed leadership: According to the evidence. J. Educ. Admin. 2008, 46, 172–188. [Google Scholar]
- Karlsson, J.; Anderberg, E.; Booth, S.; Odenrick, P.; Christmansson, M. Reaching beyond disciplines through collaboration. J. Workplace Learn. 2008, 20, 98–113. [Google Scholar] [CrossRef]
- Whitchurch, C. Professional Managers in UK Higher Education: Preparing for Complex Futures—Final Report; Leadership Foundation for Higher Education: London, UK, 2008. [Google Scholar]
- Greeno, J.G. Theories and practices of thinking and learning to think. Am. J. Educ. (Chic Ill) 1997, 106, 85–126. [Google Scholar]
- Greeno, J.G. Learning in Activity. In The Cambridge Handbook of the Learning Sciences; Sawyer, R., Ed.; Cambridge University Press: Cambridge, UK, 2006; pp. 79–96. [Google Scholar]
- Kodner, D.; Spreeuwenberg, C. Integrated care: Meaning, logic, applications, and implications—a discussion paper. Int. J. Integr. Care 2002, 2, e12. [Google Scholar]
- Kauffman, S.A. At Home in the Universe: The Search for the Laws of Self-Organization and Complexity; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Stacey, R.D. Strategic Management and Organizational Dynamics: The Challenge of Complexity, 4th ed.; Pearson Education/Prentice Hall: Harlow, UK, 2003. [Google Scholar]
- Weick, K.E. Making Sense of the Organization; Blackwell Publishing: Malden, MA, USA, 2001. [Google Scholar]
- Morgan, G. Images of Organization; Sage Publications: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Cilliers, P. Complexity and Postmodernism: Understanding Complex Systems; Routledge: London, UK, 1998. [Google Scholar]
- Poerksen, B. Learning how to learn. Kybernetes 2005, 34, 471–484. [Google Scholar]
- Mezirow, J. Transformative Dimensions of Adult Learning; Jossey-Bass: San Francisco, CA, USA, 1991. [Google Scholar]
- Gittell, J. Coordinating mechanisms in care provider groups: Relational coordination as a mediator and input uncertainty as a moderator of performance effects. Manage. Sci. 2002, 48, 1408–1426. [Google Scholar] [CrossRef]
- Gittell, J.; Fairfield, K.; Bierbaum, B.; Head, W.; Jackson, R.; Kelly, M.; Laskin, R.; Lipson, S.; Siliski, J.; Thornhill, T.; et al. Impact of relational coordination on quality of care, postoperative pain and functioning, and length of stay: A nine-hospital study on surgical patients. Med. Care 2000, 38, 807–819. [Google Scholar] [CrossRef]
- Easterby-Smith, M.; Snell, R.; Gherardi, S. Organizational learning: Diverging communities of practice? Manag. Learn. 1998, 29, 259–272. [Google Scholar] [CrossRef]
- Mork, B.; Hoholm, T.; Ellingsen, G.; Edwin, B.; Aanestad, M. Challenging expertise: On power relations within and across communities of practice in medical innovation. Manag. Learn. 2010, 41, 575–592. [Google Scholar]
- Layder, D. The Realist Image in Social Science; MacMillan: London, UK, 1990. [Google Scholar]
- Patton, M. Q. Systems Thinking and Complexity Concepts for Developmental Evaluation in Developmental Evaluation: Applying Complexity Concepts to Enhance Innovation and Use; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Bradbury, H.; Lichenstein, B.M.B. Relationality in organizational research: Exploring the space between. Organ. Sci. 2000, 11, 551–564. [Google Scholar]
- Czarniawska, B. A Theory of Organizing; Edward Elgar Publishing: Cheltenham, UK, 2008. [Google Scholar]
- Grove, J.; Barry, K.; Haas, T. EvaluLead: A Guide for Shaping and Evaluating Leadership Development Programs; The Public Health Institute: California, CA, USA, 2005. [Google Scholar]
- W.K. Kellogg Foundation. Designing Initiative Evaluation a Systems-oriented Framework for Evaluating Social Change Efforts; W.K. Kellogg Foundation: Battle Creek, MI, USA, 2007.
- Stacey, R.D. Complex Responsive Processes in Organizations: Learning and Knowledge Creation; Routledge: London, UK, 2001. [Google Scholar]
- Dooley, K. Complexity Science Models of Organizational Change and Innovation. In Handbook of Organizational Change and Innovation; Poole, M.S., Van de Ven, A., Eds.; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Poole, M.; Van De Ven, A.H.; Dooley, K. Organizational Change and Innovation Processes: Theory and Methods for Research; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Guastello, S.; Gregson, R. (Eds.) Nonlinear Dynamical Systems Analysis for the Behavioral Sciences using Real Data; CRC Press: Boca Raton, FL, USA, 2011.
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tsasis, P.; Evans, J.M.; Rush, L.; Diamond, J. Learning to Learn: towards a Relational and Transformational Model of Learning for Improved Integrated Care Delivery. Adm. Sci. 2013, 3, 9-31. https://doi.org/10.3390/admsci3020009
Tsasis P, Evans JM, Rush L, Diamond J. Learning to Learn: towards a Relational and Transformational Model of Learning for Improved Integrated Care Delivery. Administrative Sciences. 2013; 3(2):9-31. https://doi.org/10.3390/admsci3020009
Chicago/Turabian StyleTsasis, Peter, Jenna M. Evans, Linda Rush, and John Diamond. 2013. "Learning to Learn: towards a Relational and Transformational Model of Learning for Improved Integrated Care Delivery" Administrative Sciences 3, no. 2: 9-31. https://doi.org/10.3390/admsci3020009
APA StyleTsasis, P., Evans, J. M., Rush, L., & Diamond, J. (2013). Learning to Learn: towards a Relational and Transformational Model of Learning for Improved Integrated Care Delivery. Administrative Sciences, 3(2), 9-31. https://doi.org/10.3390/admsci3020009