Temporal Trend of PM10 and Associated Human Health Risk over the Past Decade in Cluj-Napoca City, Romania

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Population
2.2. Air Quality Data
2.3. Air Quality Index
2.4. Human Health Risk Assessment
3. Results and Discussion
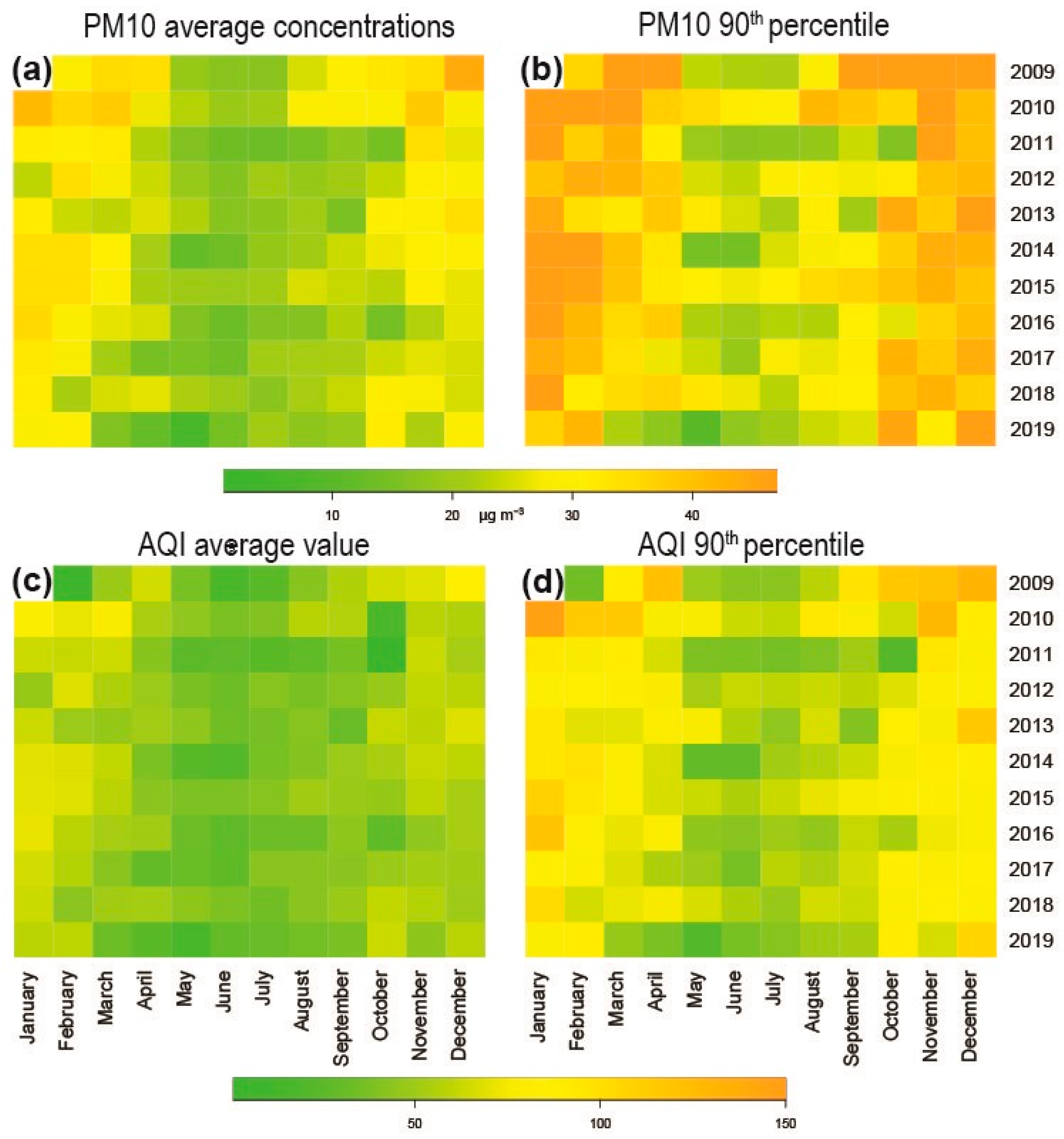
3.1. Air Quality
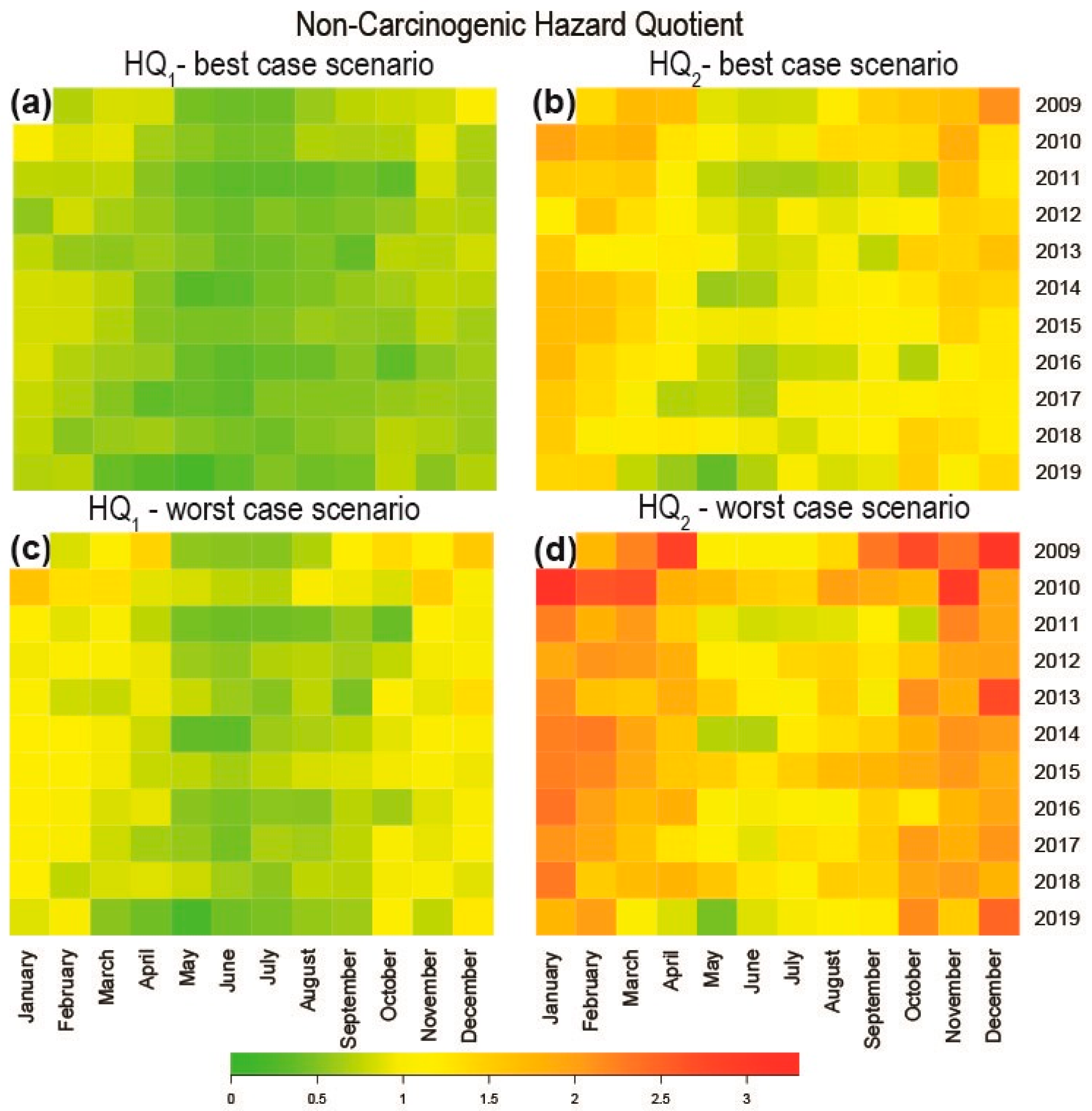
3.2. Human Health Risk Assessment
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Malandrino, M.; Di Martino, M.; Ghiotti, G.; Geobaldo, F.; Grosa, M.M.; Giacomino, A. Abollino OInter-annual seasonal variability in PM10 samples monitored in the city of Turin (Italy) from 2002 to, 2005. Microchem. J. 2013, 107, 76–85. [Google Scholar] [CrossRef]
- Zhong, S.; Yu, Z.; Zhu, W. Study of the effects of air pollutants on human health based on Baidu indices of disease symptoms and air quality monitoring data in Beijing, China. Int. J. Environ. Res. Public Health 2019, 16, 1014. [Google Scholar] [CrossRef] [Green Version]
- Hassanvand, M.S.; Naddafi, K.; Faridi, S.; Sowlat, M.H.; Momeniha, F.; Gholampour, A.; Arhami, M.; Kashani, H.; Zare, A.; Niazi, S.; et al. Characterization of PAHs and metals in indoor/outdoor PM10/PM2.5/PM1 in a retirement home and a school dormitory. Sci. Total Environ. 2015, 527, 100–110. [Google Scholar] [CrossRef]
- EEA (European Environment Agency). Air Quality in Europe—2019 Report European Environment Agency; Publications Office of the European Union: Luxembourg, 2019; Available online: https://www.eea.europa.eu/publications/air-quality-in-europe-2019 (accessed on 2 July 2020).
- Henschel, S.; Chan, G. Health Risks of Air Pollution in Europe, HRAPIE Project: New Emerging Risks to Health from Air Pollution—Results from the Survey of Experts; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0017/234026/e96933.pdf?ua=1 (accessed on 3 July 2020).
- Hoffer, A.; Jancsek-Turóczi, B.; Tóth, Á.; Kiss, G.; Naghiu, A.; Levei, E.A.; Marmureanu, L.; Machon, A.; Gelencsér, A. Emission factors for PM10 and PAHs from illegal burning of different types of municipal waste in households. Atmos. Chem. Phys. Discuss. 2020, 1–18. [Google Scholar] [CrossRef]
- Air Pollutant Emissions Data Viewer (Gothenburg Protocol, LRTAP Convention) 1990–2017. Available online: https://www.eea.europa.eu/data-and-maps/dashboards/air-pollutant-emissions-data-viewer-2 (accessed on 30 June 2020).
- Belis, C.A.; Larsen, B.; Fulvio, A.; El Haddad, I.; Favez, O.; Harrison, R.M.; Hopke, P.; Nava, S.; Paatero, P.; Prevot, A.; et al. European Guide on with Receptor Models Air Pollution Source Apportionment; Joint Research Centre of the European Commission: Luxemburg, 2014; pp. 1–88. [Google Scholar]
- Marmureanu, L.; Vasilescu, J.; Slowik, J.; Prevot, A.S.H.; Marin, C.A.; Antonescu, B.; Vlachou, A.; Nemuc, A.; Dandocsi, A.; Szidat, S. Online chemical characterization and source identification of summer and winter aerosols in Magurele, Romania. Atmosphere 2020, 11, 385. [Google Scholar] [CrossRef] [Green Version]
- Gruszecka-Kosowska, A. Assessment of the Krakow inhabitants’ health risk caused by the exposure to inhalation of outdoor air contaminants. Stoch. Environ. Res. Risk Assess. 2018, 32, 485–499. [Google Scholar] [CrossRef] [Green Version]
- Khaniabadi, Y.O.; Polosa, R.; Chuturkova, R.Z.; Daryanoosh, M.; Goudarzi, G.; Borgini, A.; Tittarelli, A.; Basiri, H.; Armin, H.; Nourmoradi, H.; et al. Human health risk assessment due to ambient PM10 and SO2 by an air quality modeling technique. Process. Saf. Environ. 2017, 111, 346–354. [Google Scholar] [CrossRef]
- Kelly, F.J.; Fussell, J.C. Size, source and chemical composition as determinants of toxicity attributable to ambient particulate matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Dehghani, M.; Keshtgar, L.; Javaheri, M.R.; Derakhshan, Z.; Oliveri Conti, G.; Zuccarello, P.; Ferrante, M. The effects of air pollutants on the mortality rate of lung cancer and leukemia. Mol. Med. Rep. 2017, 15, 3390–3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaniabadi, Y.O.; Goudarzi, G.; Daryanoosh, S.M.; Borgini, A.; Tittarelli, A.; De Marco, A. Exposure to PM10, NO2, and O3 and impacts on human health. Environ. Sci. Pollut. Res. 2017, 24, 2781–2789. [Google Scholar] [CrossRef] [PubMed]
- De Donno, A.; De Giorgi, M.; Bagordo, F.; Grassi, T.; Idolo, A.; Serios, F.; Ceretti, E.; Ferretti, D.; Villarini, M.; Moretti, M.; et al. Health risk associated with exposure to PM10 and benzene in three Italian towns. Int. J. Environ. Res. Public Health 2018, 15, 1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kliengchuay, W.; Cooper Meeyai, A.; Worakhunpiset, S.; Tantrakarnapa, K. Relationships between meteorological parameters and particulate matter in Mae Hong Son Province. Thailand. Int. J. Environ. Res. Public Health 2018, 15, 2801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A.; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalvatzaki, E.; Chatoutsidou, S.E.; Lehtomaki, H.; Almeida, S.M.; Eleftheriadis, K.; Hanninen, O.; Lazaridis, M. Characterization of human health risks from particulate air pollution in selected European cities. Atmosphere 2019, 10, 96. [Google Scholar] [CrossRef] [Green Version]
- Yin, F.; Ma, Y.; Zhao, X.; Lv, Q.; Liu, Y.; Li, X.; Zhang, T. Analysis of the effect of PM10 on hand, foot and mouth disease in a basin terrain city. Sci. Rep. 2019, 98, 3233. [Google Scholar] [CrossRef] [Green Version]
- Riojas-Rodriguez, H.; Alamo-Hernandez, U.; Texcalac-Sangrador, J.L.; Romieu, I. Health impact assessment of decreases in PM10 and ozone concentrations in the Mexico City metropolitan area. A basis for a new air quality management program. Salud. Publica Mex. 2014, 56, 579–591. [Google Scholar] [CrossRef]
- Romanazzi, V.; Casazza, M.; Malandrino, M.; Maurino, V.; Piano, A.; Schiliro, T.G.; Gilli, G. PM10 size distribution of metals and environmental-sanitary risk analysis in the city of Torino. Chemosphere 2014, 112, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Vaduganathan, M.; De Palma, G.; Manerba, A.; Goldoni, M.; Triggiani, M.; Apostoli, P.; Cas, L.D.; Nodari, S. Risk of cardiovascular hospitalizations from exposure to coarse particulate matter (PM10) below the European Union safety threshold. Am. J. Cardiol. 2016, 117, 123–135. [Google Scholar] [CrossRef]
- European Parliament, Council of the European Union. Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe. Off. J. Eur. Union 2008, L152, 1–44. Available online: https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A32008L0050 (accessed on 18 June 2020).
- Outdoor Air Pollution, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; No. 109, ARC Working Group on the Evaluation of Carcinogenic Risk to Humans; International Agency for Research on Cancer, WHO Press: Lyon, France, 2016; Available online: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Outdoor-Air-Pollution-2015 (accessed on 2 June 2020).
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef]
- US Environmental Protection Agency. Risk Assessment Guidance for Superfund Volume I, Human Health Evaluation Manual, Part F, Supplement Guidance for Inhalation Risk Assessment; Office of Emergency and Remedial Response: Washington, DC, USA, 2011. Available online: https://www.epa.gov/sites/production/files/2015-09/documents/partf_200901_final.pdf (accessed on 2 June 2020).
- Air Quality in Europe-2018 Report. Available online: https://op.europa.eu/en/publication-detail/-/publication/223e663b-1340-11e9-81b4-01aa75ed71a1 (accessed on 4 June 2020).
- Romania-Air Pollution Country Fact Sheet. Available online: https://www.eea.europa.eu/themes/air/country-fact-sheets/2019-country-fact-sheets/romania (accessed on 23 June 2020).
- Law 104 from 15 June 2011, Regarding the Environmental Air Quality. Official Monitor, No. 452 from 28 June 2011. Available online: http://www.calitateaer.ro/export/sites/default/.galleries/Legislation/national/Lege-nr.-104_2011-calitatea-aerului-inconjurator.pdf_2063068895.pdf (accessed on 2 June 2020).
- Hu, X.; Zhang, Y.; Ding, Z.H.; Wang, T.; Lian, H.; Sun, Y.; Wu, J. Bio-accessibility and health risk of arsenic and heavy metals (Cd, Co, Cr, Cu, Ni, Pb, Zn and Mn) in TSP and PM2.5 in Nanjing, China. Atmos. Environ. 2012, 57, 146–152. [Google Scholar] [CrossRef]
- Kassomenos, P.A.; Vardoulakis, S.; Chaloulakou, A.; Paschalidou, A.K.; Grivas, G.; Borge, R.; Lumbreras, J. Study of PM10 and PM2.5 levels in three European cities: Analysis of intra and inter urban variations. Atmos. Environ. 2014, 87, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Zhao, B.; Zhang, L.; Luo, R. Department spatiotemporal variations of PM2.5 and PM10 concentrations between 31 Chinese cities and their relationships with SO2, NO2, CO and O3. Particuology 2015, 20, 141–149. [Google Scholar] [CrossRef]
- Madureira, J.; Paciencia, I.; Cavaleiro Rufo, J.; Severo, M.; Ramos, E.; Barros, H.; De Oliveira Fernandes, E. Source apportionment of CO2, PM10 and VOCs levels and health risk assessment in naturally ventilated primary schools in Porto, Portugal. Build. Environ. 2016, 96, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Rumana, H.S.; Sharma, R.C.; Beniwal, V.; Sharma, A.K. A retrospective approach to assess human health risks associated with growing air pollution in urbanized area of Thar Desert, western Rajasthan, India. J. Environ. Health Sci. 2014, 12, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Pascal, M.; Falq, G.; Wagner, V.; Chatignoux, E.; Corso, M.; Blanchard, M.; Host, S.; Pascal, L.; Larrieu, S. A short-term impact of particulate matter (PM10, PM10-2.5, PM2.5) on mortality in nine French cities. Atmos. Environ. 2014, 95, 175–184. [Google Scholar] [CrossRef]
- Maji, K.J.; Dikshit, A.K.; Deshpande, A. Human health risk assessment due to air pollution in 10 urban cities in Maharashtra India. Cogent Environ. Sci. 2016, 2, 1193110. [Google Scholar]
- Bulejko, P.; Adamec, V.; Skeril, R.; Schüllerová, B.; Bencko, V. Levels health risk assessment of PM10 aerosol in Brno Czech Republic. Cent. Eur. J. Public Health 2017, 25, 129–134. [Google Scholar] [CrossRef]
- Megido, L.; Suarez-Pena, B.; Negral, L.; Castrillon, L.; Fernandez-Nava, Y. Suburban air quality: Human health hazard assessment of potentially toxic elements in PM10. Chemosphere 2017, 177, 284–291. [Google Scholar] [CrossRef]
- Leitte, A.M.; Petrescu, C.; Franck, U.; Richter, M.; Suciu, O.; Ionovici, R.; Herbarth, O.; Schlink, U. Respiratory health effects of ambient air pollution its modification by air humidity in Drobeta-Turnu Severin Romania. Sci. Total Environ. 2009, 407, 4004–4011. [Google Scholar] [CrossRef]
- Dunea, D.; Iordache, S.; Liu, H.Y.; Bøhler, T.; Pohoata, A.; Radulescu, C. Quantifying the impact of, P.M.2.5.; associated heavy metals on respiratory health of children near metallurgical facilities. Environ. Sci. Pollut. Res. 2016, 23, 15395–15406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Statistics and the Statistical Division of the Cluj County. Available online: http://www.cluj.insse.ro/produse-si-servicii/statistici-judetene/populatia/ (accessed on 5 June 2020).
- Geicu, A.; Candea, I. Clima Romaniei (The Climate of Romania), Romanian National Meteorological Administration; Romanian Academy Press: Bucharest, Romania, 2008. [Google Scholar]
- Planul integrat de calitate a aerului pentru aglomerarea Cluj-Napoca pentru indicatorii oxizi de azot (NOx/NO2) și particule in suspensie (PM10) perioada 2019–2023, Primaria Cluj-Napoca. Available online: https://files.primariaclujnapoca.ro/2019/05/23/Plan-Integrat-de-calitate-a-aerului-pentru-aglomerarea-Cluj-Napoca.pdf (accessed on 16 June 2020).
- Air Quality. National Air Quality Monitoring Network. Available online: http://www.calitateaer.ro/public/monitoring-page/reports-reports-page/?__locale=en (accessed on 2 June 2020).
- Mohan, M.; Kandya, A. An analysis of the annual seasonal trends of Air Quality Index of Delhi. Environ. Monit. Assess. 2007, 131, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Iorga, G. Air Quality—Measurement Modeling Air Pollution Monitoring: A Case Study from Romania. In Air Quality-Measurement and Modelling; Sallis, P.J., Ed.; Intech Open: London, UK, 2016; pp. 135–162. [Google Scholar]
- Miclean, M.; Cadar, O.; Levei, E.A.; Roman, R.; Ozunu, A.; Levei, L. Metal (Pb, Cu, Cd, and Zn) Transfer along food chain health risk assessment through raw milk consumption from free-range cows. Int. J. Environ. Res. Public Health 2019, 16, 4064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proorocu, M.; Odagiu, A.; Oroian, I.G.; Ciuiu, G.; Dan, V. Particulate matter status in Romanian urban areas: PM10 pollution levels in Bucharest. Environ. Eng. Manag. J. 2014, 3, 3115–3122. [Google Scholar] [CrossRef]
- Iorga, G.; Balaceanu Raicu, C.; Stefan, S. Annual air pollution level of major primary pollutants in Greater Area of Bucharest. Atmos. Pollut. Res. 2015, 6, 824–834. [Google Scholar]
- Zhao, W.; Cheng, J.; Li, D.; Duan, Y.; Wei, H.; Ji, R.; Wang, W. Urban ambient air quality investigation health risk assessment during haze non-haze periods in Shanghai China. Atmos. Pollut. Res. 2013, 4, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Morakinyo, O.M.; Adebowale, A.S.; Mokgobu, M.I.; Mukhola, M.S. Health risk of inhalation exposure to sub-10 μm particulate matter gaseous pollutants in an urban-industrial area in South Africa: An ecological study. BMJ Open 2017, 7, e013941. [Google Scholar] [CrossRef]
- Stylianou, M.; Nicolich, M.J. Cumulative effects and threshold levels in air pollution mortality: Data analysis of nine large US cities using the NMMAPS dataset. Environ. Pollut. 2009, 157, 2216–2223. [Google Scholar] [CrossRef]
- Xia, Y.; Tong, H. Cumulative effects of air pollution on public. Stat. Med. 2006, 25, 3548–3559. [Google Scholar] [CrossRef]
- Mauderly, J.L.; Samet, J.M. Is there evidence for synergy among air pollutants in causing health effects. Environ. Health Perspect. 2009, 117, 1–6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PM10 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Minimum | 2.0 | 6.35 | 2.7 | 5.8 | 6.7 | 7.0 | 7.5 | 2.7 | 3.2 | 7.9 | 3.6 |
| Maximum | 86.8 | 111.3 | 59.7 | 54.8 | 61.6 | 65.7 | 61.6 | 76.6 | 56.5 | 59.5 | 62.2 |
| Average | 27.4 | 29.5 | 23.2 | 24.0 | 24.4 | 24.9 | 25.7 | 22.0 | 22.2 | 24.4 | 20.3 |
| Standard deviation | 15.9 | 14.5 | 11.1 | 9.8 | 10.7 | 11.2 | 10.1 | 10.6 | 10.1 | 9.4 | 10.7 |
| 10th percentile | 9.8 | 14.2 | 11.4 | 12.2 | 12.8 | 11.8 | 14.4 | 9.7 | 10.4 | 13.8 | 8.7 |
| 50th percentile | 24.6 | 26.8 | 19.9 | 22.5 | 21.3 | 22.6 | 23.7 | 20.4 | 21.04 | 22.7 | 18.0 |
| 90th percentile | 51.6 | 47.6 | 40.9 | 38.1 | 39.2 | 40.1 | 39.9 | 36.5 | 38.1 | 37.6 | 35.3 |
| Skewness | 1.1 | 1.5 | 0.8 | 0.5 | 0.9 | 0.6 | 0.7 | 1.0 | 0.7 | 0.8 | 1.1 |
| Kurtosis | 0.6 | 4.0 | −0.2 | −0.6 | 0.4 | −0.2 | 0.1 | 2.3 | 0.17 | 0.5 | 1.4 |
| Days with PM10 > 50 μg/m3 | 29 | 26 | 4 | 1 | 6 | 6 | 5 | 3 | 3 | 5 | 9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levei, L.; Hoaghia, M.-A.; Roman, M.; Marmureanu, L.; Moisa, C.; Levei, E.A.; Ozunu, A.; Cadar, O. Temporal Trend of PM10 and Associated Human Health Risk over the Past Decade in Cluj-Napoca City, Romania. Appl. Sci. 2020, 10, 5331. https://doi.org/10.3390/app10155331
Levei L, Hoaghia M-A, Roman M, Marmureanu L, Moisa C, Levei EA, Ozunu A, Cadar O. Temporal Trend of PM10 and Associated Human Health Risk over the Past Decade in Cluj-Napoca City, Romania. Applied Sciences. 2020; 10(15):5331. https://doi.org/10.3390/app10155331
Chicago/Turabian StyleLevei, Levente, Maria-Alexandra Hoaghia, Marius Roman, Luminita Marmureanu, Corina Moisa, Erika Andrea Levei, Alexandru Ozunu, and Oana Cadar. 2020. "Temporal Trend of PM10 and Associated Human Health Risk over the Past Decade in Cluj-Napoca City, Romania" Applied Sciences 10, no. 15: 5331. https://doi.org/10.3390/app10155331