Evaluating the Risk Factors of Post Inflammatory Hyperpigmentation Complications with Nd-YAG Laser Toning Using LASSO-Based Algorithm


 , ,
, ,
Abstract
:1. Introduction
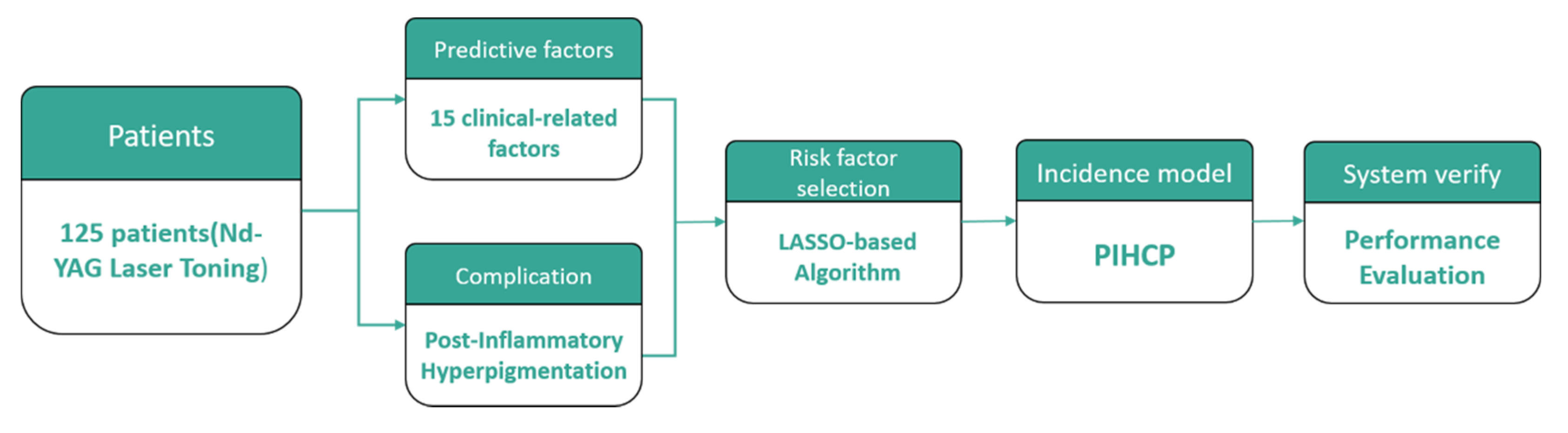
2. Methods
2.1. Samples
2.2. Treatment
2.3. Post-Inflammatory Hyperpigmentation Complications
2.4. Predictive Risk Factors
2.5. PIHCP Evaluation (LASSO)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Ethical Statement
References
- Li, J.Y.; Geddes, E.R.; Robinson, D.M.; Friedman, P.M. A review of melasma treatment focusing on laser and light devices. Semin. Cutan. Med. Surg. 2016, 35, 223–232. [Google Scholar] [CrossRef]
- Sugawara, J.; Kou, S.; Kou, S.; Yasumura, K.; Satake, T.; Maegawa, J. Influence of the frequency of laser toning for melasma on occurrence of leukoderma and its early detection by ultraviolet imaging. Lasers Surg. Med. 2015, 47, 161–167. [Google Scholar] [CrossRef]
- Wanner, M.; Sakamoto, F.H.; Avram, M.M.; Chan, H.H.; Alam, M.; Tannous, Z.; Anderson, R.R. Immediate skin responses to laser and light treatments: Therapeutic endpoints: How to obtain efficacy. J. Am. Acad. Dermatol. 2016, 74, 821–833. [Google Scholar] [CrossRef] [PubMed]
- Wanner, M.; Sakamoto, F.H.; Avram, M.M.; Anderson, R.R. Immediate skin responses to laser and light treatments: Warning endpoints: How to avoid side effects. J. Am. Acad. Dermatol. 2016, 74, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Song, H.S.; Kang, H.Y. Time sequential changes of melanocytes and melanogenic factors in laser-induced postinflammatory hyperpigmentation: P6854. J. Am. Acad. Dermatol. 2013, 68, AB190. [Google Scholar]
- Silpa-Archa, N.; Kohli, I.; Chaowattanapanit, S.; Lim, H.W.; Hamzavi, I. Postinflammatory hyperpigmentation: A comprehensive overview: Epidemiology, pathogenesis, clinical presentation, and noninvasive assessment technique. J. Am. Acad. Dermatol. 2017, 77, 591–605. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.-J.; van der Schaaf, A.; Schilstra, C.; Langendijk, J.A.; van’t Veld, A.A. Impact of statistical learning methods on the predictive power of multivariate normal tissue complication probability models. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e677–e684. [Google Scholar] [CrossRef]
- Xu, C.-J.; van der Schaaf, A.; Van’t Veld, A.A.; Langendijk, J.A.; Schilstra, C. Statistical validation of normal tissue complication probability models. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e123–e129. [Google Scholar] [CrossRef]
- Xu, J.; Yin, J. Kernel least absolute shrinkage and selection operator regression classifier for pattern classification. IET Comput. Vis. 2013, 7, 48–55. [Google Scholar] [CrossRef]
- Lee, T.-F.; Liou, M.-H.; Huang, Y.-J.; Chao, P.-J.; Ting, H.-M.; Lee, H.-Y.; Fang, F.-M. LASSO NTCP predictors for the incidence of xerostomia in patients with head and neck squamous cell carcinoma and nasopharyngeal carcinoma. Sci. Rep. 2014, 4, 6217. [Google Scholar] [CrossRef] [Green Version]
- Kong, C.; Zhu, X.-Z.; Lee, T.-F.; Feng, P.-B.; Xu, J.-H.; Qian, P.-D.; Zhang, L.-F.; He, X.; Huang, S.-F.; Zhang, Y.-Q. LASSO-based NTCP model for radiation-induced temporal lobe injury developing after intensity-modulated radiotherapy of nasopharyngeal carcinoma. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Langendijk, J.A.; Doornaert, P.; Rietveld, D.H.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Slotman, B.J. A predictive model for swallowing dysfunction after curative radiotherapy in head and neck cancer. Radiother. Oncol. 2009, 90, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-F.; Chao, P.-J.; Ting, H.-M.; Chang, L.; Huang, Y.-J.; Wu, J.-M.; Wang, H.-Y.; Horng, M.-F.; Chang, C.-M.; Lan, J.-H. Using multivariate regression model with least absolute shrinkage and selection operator (LASSO) to predict the incidence of xerostomia after intensity-modulated radiotherapy for head and neck cancer. PLoS ONE 2014, 9, e89700. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-F.; Fang, F.-M. Quantitative analysis of normal tissue effects in the clinic (QUANTEC) guideline validation using quality of life questionnaire datasets for parotid gland constraints to avoid causing xerostomia during head-and-neck radiotherapy. Radiother. Oncol. 2013, 106, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B (Methodol.) 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J.; Franklin, J. The elements of statistical learning: Data mining, inference and prediction. Math. Intell. 2005, 27, 83–85. [Google Scholar]
- Wattanakrai, P.; Mornchan, R.; Eimpunth, S. Low-fluence Q-switched neodymium-doped yttrium aluminum garnet (1,064 nm) laser for the treatment of facial melasma in Asians. Dermatol. Surg. 2010, 36, 76–87. [Google Scholar] [CrossRef]
- Beetz, I.; Schilstra, C.; Burlage, F.R.; Koken, P.W.; Doornaert, P.; Bijl, H.P.; Chouvalova, O.; Leemans, C.R.; de Bock, G.H.; Christianen, M.E. Development of NTCP models for head and neck cancer patients treated with three-dimensional conformal radiotherapy for xerostomia and sticky saliva: The role of dosimetric and clinical factors. Radiother. Oncol. 2012, 105, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Beetz, I.; Schilstra, C.; van der Schaaf, A.; van den Heuvel, E.R.; Doornaert, P.; van Luijk, P.; Vissink, A.; van der Laan, B.F.; Leemans, C.R.; Bijl, H.P. NTCP models for patient-rated xerostomia and sticky saliva after treatment with intensity modulated radiotherapy for head and neck cancer: The role of dosimetric and clinical factors. Radiother. Oncol. 2012, 105, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Chan, N.P.; Ho, S.G.; Shek, S.Y.; Yeung, C.K.; Chan, H.H. A case series of facial depigmentation associated with low fluence Q-switched 1,064 nm Nd: YAG laser for skin rejuvenation and melasma. Lasers Surg. Med. 2010, 42, 712–719. [Google Scholar] [CrossRef]
- Sim, J.H.; Park, Y.L.; Lee, J.S.; Lee, S.Y.; Choi, W.B.; Kim, H.J.; Lee, J.H. Treatment of melasma by low-fluence 1064 nm Q-switched Nd: YAG laser. J. Dermatol. Treat. 2014, 25, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.M.; Perez, M.I. Treatment of hyperpigmentation. Facial Plast. Surg. Clin. 2011, 19, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.C.; Callender, V.D. Postinflammatory hyperpigmentation: A review of the epidemiology, clinical features, and treatment options in skin of color. J. Clin. Aesthetic Dermatol. 2010, 3, 20. [Google Scholar]
- Hirsch, R.; Stier, M. Complications and their management in cosmetic dermatology. Dermatol. Clin. 2009, 27, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Abad-Casintahan, F.; Chow, S.K.W.; Goh, C.L.; Kubba, R.; Hayashi, N.; Noppakun, N.; See, J.; Suh, D.H.; Xiang, L.H.F.; Kang, S. Frequency and characteristics of acne-related post-inflammatory hyperpigmentation. J. Dermatol. 2016, 43, 826–828. [Google Scholar] [CrossRef]
- Kim, B.W.; Lee, M.H.; Chang, S.E.; Yun, W.J.; Won, C.H.; Lee, M.W.; Choi, J.H.; Moon, K.C. Clinical efficacy of the dual-pulsed Q-switched neodymium: Yttrium-aluminum-garnet laser: Comparison with conservative mode. J. Cosmet. Laser Ther. 2013, 15, 340–341. [Google Scholar] [CrossRef]
- Kim, J.E.; Chang, S.; Yeo, U.; Haw, S.; Kim, I.H. Histopathological study of the treatment of melasma lesions using a low-fluence Q-switched 1064-nm neodymium: Yttrium–aluminium–garnet laser. Clin. Exp. Dermatol. Clin. Dermatol. 2013, 38, 167–171. [Google Scholar] [CrossRef]
- Kim, M.; Kim, J.; Cho, S. Punctate leucoderma after melasma treatment using 1064-nm Q-switched Nd: YAG laser with low pulse energy. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 960–962. [Google Scholar] [CrossRef]
- Wong, Y.; Lee, S.S.J.; Goh, C.L. Hypopigmentation induced by frequent low-fluence, large-spot-size QS Nd: YAG laser treatments. Ann. Dermatol. 2015, 27, 751–755. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Factors | (n = 125) Value-x (%) |
|---|---|
| Age (years) | |
| Mean | 47.18 |
| Range | 21.00–77.00 |
| <51 | 83 (66.4) |
| 51–60 | 25 (20.0) |
| 61–70 | 13 (10.4) |
| >71 | 4 (3.2) |
| FSPT | |
| Type III | 85 (68.0) |
| Type IV | 27 (21.6) |
| Type V | 13 (10.4) |
| Melasma | |
| No | 81 (64.8) |
| Yes | 44 (35.2) |
| Acne | |
| No | 108 (86.4) |
| Yes | 17 (13.6) |
| ZN | |
| No | 115 (92.0) |
| Yes | 10(8.0) |
| Lentigines | |
| No | 45 (36.0) |
| Yes | 80 (64.0) |
| Pores | |
| No | 85 (68.0) |
| Yes | 40 (32.0) |
| LD | |
| <750 | 28 (22.4) |
| 750–850 | 62 (49.6) |
| >850 | 35 (28.0) |
| Laser Mode | |
| Fractional | 40 (32.0) |
| Zoom | 85 (68.0) |
| IEL | |
| Erythema | 21 (16.8) |
| Petechiae | 95 (76.0) |
| E mild P | 9 (7.2) |
| PIH | |
| No | 104 (83.2) |
| Yes | 21 (16.8) |
| No. | Factors | Range or Classification | Median or Frequency | Correlation |
|---|---|---|---|---|
| 1 | Age | 21–77 | 46 | −0.001 |
| 2 | IPL | 0–10 | 0 | 0.197 |
| 3 | AHA Peels | 0–11 | 0 | 0.458 |
| 4 | Sonophoresis | 0–41 | 0 | 0.175 |
| 5 | Skin Care | 0–96 | 0 | −0.129 |
| 6 | TF | 2–28 | 6 | −0.018 |
| 7 | LD | 600–1000 | 750 | −0.002 |
| 8 | Melasma | 0, 1 * | 81, 44 | 0.969 |
| 9 | FSPT | 0, 1, 2 | 85, 27, 13 | #1 |
| 10 | ZN | 0, 1 * | 115, 10 | −1.271 |
| 11 | Lentigines | 0, 1 * | 45, 80 | −0.378 |
| 12 | Acnes | 0, 1 * | 109, 16 | 1.052 |
| 13 | Pores | 0, 1 * | 85, 40 | 0.773 |
| 14 | LM | 0, 1 * | 85, 40 | 1.431 |
| 15 | IEL | 0, 1, 2 | 95, 21, 9 | #2 |
| Predictive Factors | β | p-Value | Odds Ratio | 95% CI |
|---|---|---|---|---|
| (n = 5) | ||||
| Immediately Endpoints of Laser (IEL) | ||||
| Erythema (0) | 0.02 | |||
| Petechiae (1) | 1.41 | 0.06 | 4.09 | 0.95–17.71 |
| Erythema mild Petechiae (2) | 2.30 | <0.01 | 9.92 | 1.78–55.27 |
| AHA Peels | 0.38 | 0.02 | 1.46 | 1.05–2.03 |
| FSPT | ||||
| Type III (0) | 0.26 | |||
| Type IV (1) | 0.46 | 0.56 | 1.59 | 0.33–7.65 |
| Type V (2) | 1.23 | 0.10 | 3.43 | 0.75–15.06 |
| Acnes | ||||
| Yes (1) | 1.32 | 0.06 | 3.75 | 0.94–15.02 |
| Melasma | ||||
| Yes (1) | 0.57 | 0.34 | 1.76 | 0.56–5.59 |
| Constant () | −3.29 | <0.01 | 0.04 |
| Predictive Factors Selected | HL | SB-S | R2 | Omnibus | AUC |
|---|---|---|---|---|---|
| IEL, | 1.00 | 0.06 | 0.08 | 0.06 | 0.62 (0.48–0.77) |
| IEL, AHA Peels | 0.60 | 0.09 | 0.13 | 0.02 | 0.67 (0.53–0.81) |
| IEL, AHA Peels, FSPT | 0.82 | 0.10 | 0.16 | 0.03 | 0.73 (0.60–0.85) |
| IEL, AHA Peels, FSPT, Acnes | 0.44 | 0.12 | 0.18 | 0.03 | 0.75 (0.63–0.87) |
| IEL, AHA Peels, FSPT, Acnes, Melasma | 0.29 | 0.11 | 0.20 | 0.02 | 0.79 (0.70–0.88) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-H.; Shieh, C.-S.; Huang, T.-L.; Lin, C.-H.; Chao, P.-J.; Huang, Y.-J.; Lee, H.-F.; Yeh, S.-A.; Tseng, C.-D.; Wu, J.-M.; et al. Evaluating the Risk Factors of Post Inflammatory Hyperpigmentation Complications with Nd-YAG Laser Toning Using LASSO-Based Algorithm. Appl. Sci. 2020, 10, 2049. https://doi.org/10.3390/app10062049
Liu C-H, Shieh C-S, Huang T-L, Lin C-H, Chao P-J, Huang Y-J, Lee H-F, Yeh S-A, Tseng C-D, Wu J-M, et al. Evaluating the Risk Factors of Post Inflammatory Hyperpigmentation Complications with Nd-YAG Laser Toning Using LASSO-Based Algorithm. Applied Sciences. 2020; 10(6):2049. https://doi.org/10.3390/app10062049
Chicago/Turabian StyleLiu, Chao-Hong, Chin-Shiuh Shieh, Tai-Lin Huang, Chih-Hsueh Lin, Pei-Ju Chao, Yu-Jie Huang, Hsiao-Fei Lee, Shyh-An Yeh, Chin-Dar Tseng, Jia-Ming Wu, and et al. 2020. "Evaluating the Risk Factors of Post Inflammatory Hyperpigmentation Complications with Nd-YAG Laser Toning Using LASSO-Based Algorithm" Applied Sciences 10, no. 6: 2049. https://doi.org/10.3390/app10062049