Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks

 , , , , , and
, , , , , and
Abstract
:1. Introduction
Related Work
2. Materials and Methods
2.1. Datasets
2.2. Experimental Setup
3. Results
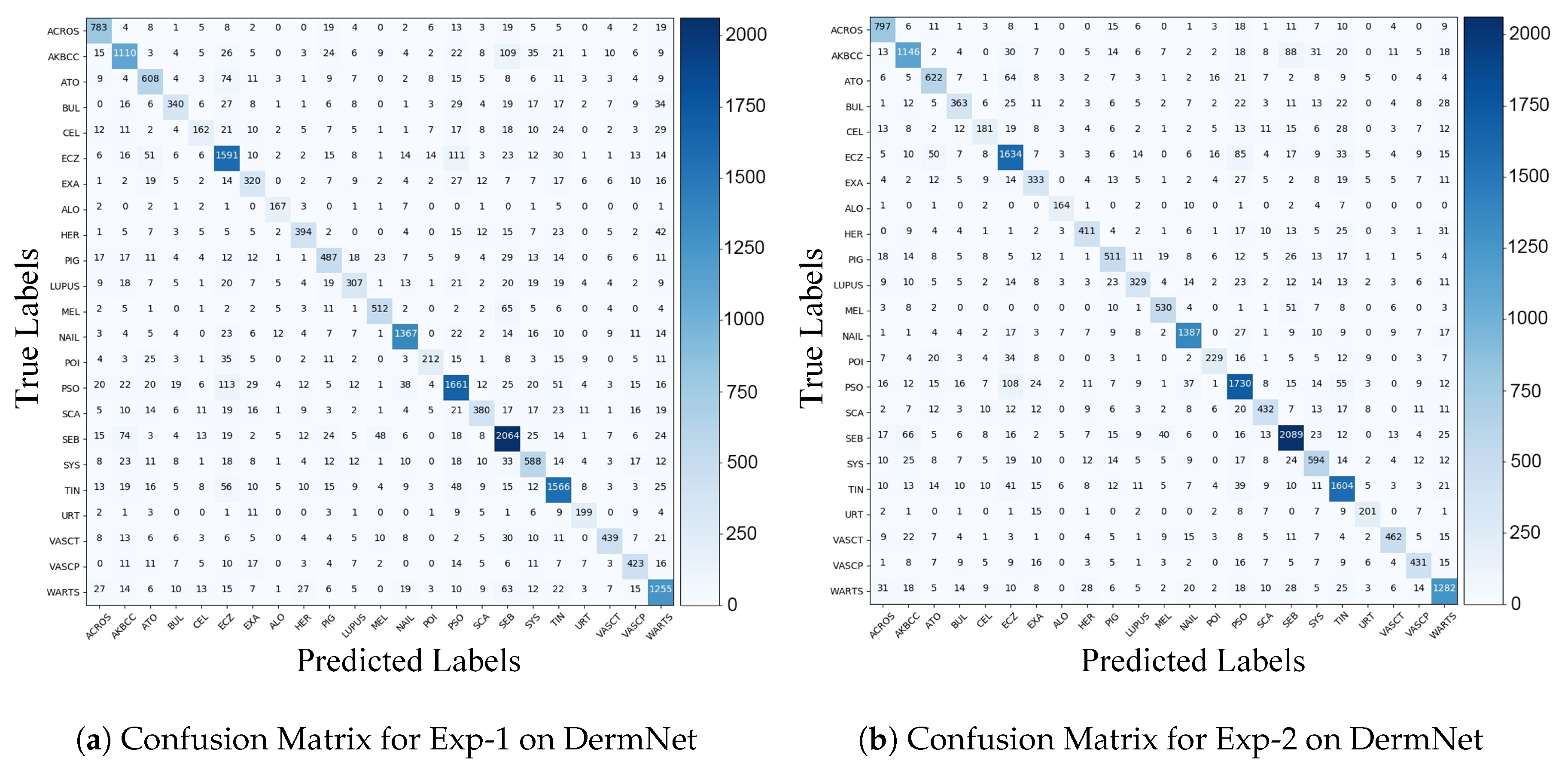
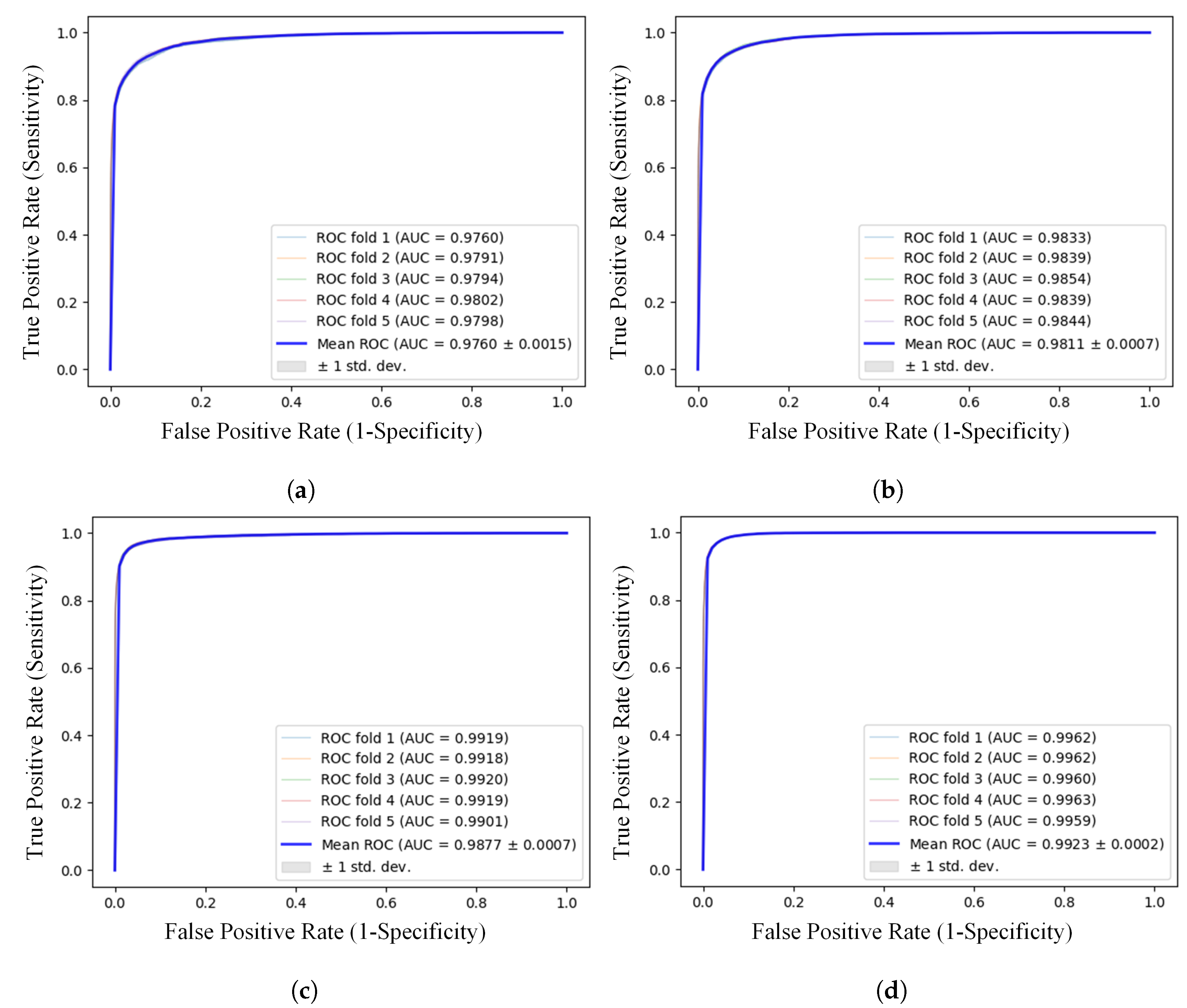
3.1. Results on DermNet
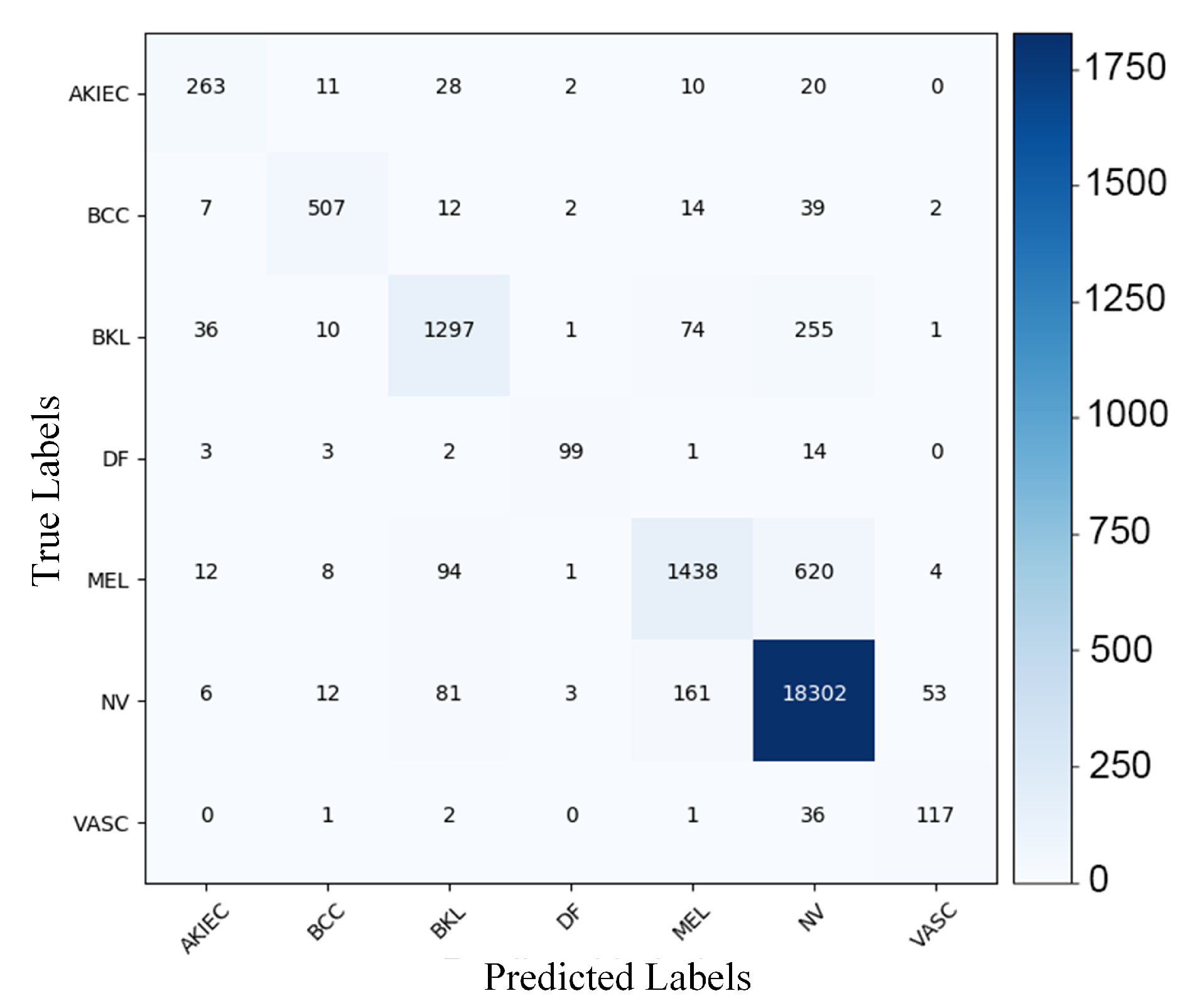
3.2. Results on ISIC Archive-2018
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| DL | Deep Learning |
| AI | Artificial Intelligence |
| CAD | Computer-Aided Diagnosis |
| CNN | Convolutional Neural Network |
| DNN | Deep Neural Network |
| ISBI | International Symposium on Biomedical Imaging |
| ISIC | International Skin Imaging Collaboration |
| AUC | Area Under the Curve |
| MCA | Mean Class Accuracy |
| ROC | Receiver Operating Characteristic |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Top-1 Accuracy (%) | Top-5 Accuracy (%) | AUC (%) | |||
|---|---|---|---|---|---|---|
| Exp-1 | Exp-2 | Exp-1 | Exp-2 | Exp-1 | Exp-2 | |
| Resnet-152 | 70.13 ± 0.89 | 75.09 ± 0.40 | 91.17 ± 0.61 | 93.12 ± 0.31 | 96.15 ± 0.27 | 97.31 ± 0.11 |
| Densenet-161 | 73.34 ± 0.68 | 77.21 ± 0.40 | 92.16 ± 0.36 | 93.91 ± 0.35 | 96.61 ± 0.15 | 97.66 ± 0.06 |
| SE_ResNeXt-101 | 74.46 ± 0.29 | 77.28 ± 0.60 | 92.59 ± 0.95 | 94.07 ± 0.25 | 96.84 ± 0.22 | 97.56 ± 0.05 |
| NASNet | 72.78 ± 0.73 | 77.21 ± 0.48 | 91.68 ± 0.58 | 92.57 ± 0.32 | 96.19 ± 0.34 | 96.79 ± 0.15 |
| Ensemble | 77.53 ± 0.64 | 79.94 ± 0.45 | 93.87 ± 0.37 | 95.02 ± 0.15 | 97.60 ± 0.15 | 98.11 ± 0.07 |
| Model | Top-1 Accuracy (%) | Top-5 Accuracy (%) | AUC (%) |
|---|---|---|---|
| Resnet-152 | 60.82 ± 0.51 | 82.16 ± 0.43 | 98.50 ± 0.10 |
| Densenet-161 | 63.51 ± 0.68 | 84.46 ± 0.46 | 98.49 ± 0.06 |
| SE_ResNeXt-101 | 64.03 ± 0.77 | 84.26 ± 0.66 | 98.48 ± 0.08 |
| NASNet | 60.69 ± 0.72 | 81.09 ± 0.61 | 97.90 ± 0.03 |
| Ensemble | 66.74 ± 0.64 | 86.26 ± 0.54 | 98.77 ± 0.07 |
| Model | Top-1 Accuracy (%) | Top-2 Accuracy (%) | AUC (%) |
|---|---|---|---|
| Resnet-152 | 89.79 ± 0.29 | 97.30 ± 0.24 | 98.97 ± 0.02 |
| Densenet-161 | 91.27 ± 0.35 | 97.46 ± 0.21 | 99.04 ± 0.03 |
| SE_ResNeXt-101 | 91.63 ± 0.17 | 97.77 ± 0.21 | 99.07 ± 0.03 |
| NASNet | 91.52 ± 0.38 | 97.57 ± 0.28 | 98.97 ± 0.05 |
| Ensemble | 93.06 ± 0.31 | 98.18 ± 0.06 | 99.23 ± 0.02 |

References
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Hirschberg, J.; Manning, C.D. Advances in natural language processing. Science 2015, 349, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Wen, L.T.; Tanaka, A.; Nonoyama, M. Identification of Marek’s disease virus nuclear antigen in latently infected lymphoblastoid cells. J. Virol. 1988, 62, 3764–3771. [Google Scholar] [CrossRef] [Green Version]
- Teare, P.; Fishman, M.; Benzaquen, O.; Toledano, E.; Elnekave, E. Malignancy detection on mammography using dual deep convolutional neural networks and genetically discovered false color input enhancement. J. Dig. Imaging 2017, 30, 499–505. [Google Scholar] [CrossRef]
- Bajwa, M.N.; Malik, M.I.; Siddiqui, S.A.; Dengel, A.; Shafait, F.; Neumeier, W.; Ahmed, S. Two-stage framework for optic disc localization and glaucoma classification in retinal fundus images using deep learning. BMC Med. Inform. Decis. Mak. 2019, 19, 136. [Google Scholar]
- Bajwa, M.N.; Taniguchi, Y.; Malik, M.I.; Neumeier, W.; Dengel, A.; Ahmed, S. Combining Fine-and Coarse-Grained Classifiers for Diabetic Retinopathy Detection. In Proceedings of the Annual Conference on Medical Image Understanding and Analysis, Liverpool, UK, 24–26 July 2019; pp. 242–253. [Google Scholar]
- Prevedello, L.M.; Erdal, B.S.; Ryu, J.L.; Little, K.J.; Demirer, M.; Qian, S.; White, R.D. Automated critical test findings identification and online notification system using artificial intelligence in imaging. Radiology 2017, 285, 923–931. [Google Scholar] [CrossRef]
- Carli, P.; Quercioli, E.; Sestini, S.; Stante, M.; Ricci, L.; Brunasso, G.; De Giorgi, V. Pattern analysis, not simplified algorithms, is the most reliable method for teaching dermoscopy for melanoma diagnosis to residents in dermatology. Br. J. Dermatol. 2003, 148, 981–984. [Google Scholar] [CrossRef]
- Carrera, C.; Marchetti, M.A.; Dusza, S.W.; Argenziano, G.; Braun, R.P.; Halpern, A.C.; Jaimes, N.; Kittler, H.J.; Malvehy, J.; Menzies, S.W.; et al. Validity and reliability of dermoscopic criteria used to differentiate nevi from melanoma: A web-based international dermoscopy society study. JAMA Dermatol. 2016, 152, 798–806. [Google Scholar] [CrossRef] [Green Version]
- Masood, A.; Ali Al-Jumaily, A. Computer aided diagnostic support system for skin cancer: A review of techniques and algorithms. Int. J. Biomed. Imaging 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, G.; Soyer, H.; De Giorgi, V.; Piccolo, D.; Carli, P.; Delfino, M. Interactive Atlas of Dermoscopy (Book and CD-ROM). 2000. Available online: http://www.dermoscopy.org/atlas/order_cd.asp (accessed on 5 March 2020).
- Ballerini, L.; Fisher, R.B.; Aldridge, B.; Rees, J. A color and texture based hierarchical K-NN approach to the classification of non-melanoma skin lesions. In Color Medical Image Analysis; Springer: Berlin, Germany, 2013; pp. 63–86. [Google Scholar]
- Giotis, I.; Molders, N.; Land, S.; Biehl, M.; Jonkman, M.F.; Petkov, N. MED-NODE: A computer-assisted melanoma diagnosis system using non-dermoscopic images. Expert Syst. Appl. 2015, 42, 6578–6585. [Google Scholar] [CrossRef]
- Mendonça, T.; Ferreira, P.M.; Marques, J.S.; Marcal, A.R.; Rozeira, J. PH 2-A dermoscopic image database for research and benchmarking. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5437–5440. [Google Scholar]
- Ali, A.R.A.; Deserno, T.M. A systematic review of automated melanoma detection in dermatoscopic images and its ground truth data. Medical Imaging 2012: Image Perception, Observer Performance, and Technology Assessment. Int. Soc. Opt. Photon. 2012, 8318, 83181I. [Google Scholar]
- Sato, I.; Nishimura, H.; Yokoi, K. Apac: Augmented pattern classification with neural networks. arXiv 2015, arXiv:1505.03229. [Google Scholar]
- Graham, B. Fractional max-pooling. arXiv 2014, arXiv:1412.6071. [Google Scholar]
- Lee, C.Y.; Gallagher, P.W.; Tu, Z. Generalizing pooling functions in convolutional neural networks: Mixed, gated, and tree. Artif. Intell. Stat. 2016, 464–472. [Google Scholar]
- Liu, C.; Zoph, B.; Neumann, M.; Shlens, J.; Hua, W.; Li, L.J.; Fei-Fei, L.; Yuille, A.; Huang, J.; Murphy, K. Progressive neural architecture search. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 19–34. [Google Scholar]
- Kawahara, J.; BenTaieb, A.; Hamarneh, G. Deep features to classify skin lesions. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 1397–1400. [Google Scholar]
- Ge, Z.; Demyanov, S.; Bozorgtabar, B.; Abedini, M.; Chakravorty, R.; Bowling, A.; Garnavi, R. Exploiting local and generic features for accurate skin lesions classification using clinical and dermoscopy imaging. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 986–990. [Google Scholar]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Haenssle, H.A.; Fink, C.; Schneiderbauer, R.; Toberer, F.; Buhl, T.; Blum, A.; Kalloo, A.; Hassen, A.B.H.; Thomas, L.; Enk, A.; et al. Man against machine: Diagnostic performance of a deep learning convolutional neural network for dermoscopic melanoma recognition in comparison to 58 dermatologists. Ann. Oncol. 2018, 29, 1836–1842. [Google Scholar] [CrossRef]
- Gutman, D.; Codella, N.C.; Celebi, E.; Helba, B.; Marchetti, M.; Mishra, N.; Halpern, A. Skin lesion analysis toward melanoma detection: A challenge at the international symposium on biomedical imaging (ISBI) 2016, hosted by the international skin imaging collaboration (ISIC). arXiv 2016, arXiv:1605.01397. [Google Scholar]
- Li, Y.; Esteva, A.; Kuprel, B.; Novoa, R.; Ko, J.; Thrun, S. Skin cancer detection and tracking using data synthesis and deep learning. In Proceedings of the Workshops at the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–5 February 2017. [Google Scholar]
- Li, Y.; Shen, L. Skin lesion analysis towards melanoma detection using deep learning network. Sensors 2018, 18, 556. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7132–7141. [Google Scholar]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 8697–8710. [Google Scholar]
- Liao, H. A Deep Learning Approach to Universal Skin Disease Classification; University of Rochester Department of Computer Science, CSC: Rochester, NY, USA, 2016. [Google Scholar]
- Cıcero, F.M.; Oliveira, A.H.M.; Botelho, G.M.; da Computaçao, C.d.C. Deep learning and convolutional neural networks in the aid of the classification of melanoma. In Proceedings of the Conference on Graphics, Patterns and Images, SIBGRAPI, Sao Paulo, Brazil, 4–7 October 2016. [Google Scholar]
- Prabhu, V.; Kannan, A.; Ravuri, M.; Chablani, M.; Sontag, D.; Amatriain, X. Prototypical Clustering Networks for Dermatological Disease Diagnosis. arXiv 2018, arXiv:1811.03066. [Google Scholar]
- Codella, N.C.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection: A challenge at the 2017 international symposium on biomedical imaging (isbi), hosted by the international skin imaging collaboration (isic). In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 168–172. [Google Scholar]
- Codella, N.; Rotemberg, V.; Tschandl, P.; Celebi, M.E.; Dusza, S.; Gutman, D.; Helba, B.; Kalloo, A.; Liopyris, K.; Marchetti, M.; et al. Skin lesion analysis toward melanoma detection 2018: A challenge hosted by the international skin imaging collaboration (isic). arXiv 2019, arXiv:1902.03368. [Google Scholar]
- Menegola, A.; Fornaciali, M.; Pires, R.; Bittencourt, F.V.; Avila, S.; Valle, E. Knowledge transfer for melanoma screening with deep learning. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 297–300. [Google Scholar]
- Nasr-Esfahani, E.; Samavi, S.; Karimi, N.; Soroushmehr, S.M.R.; Jafari, M.H.; Ward, K.; Najarian, K. Melanoma detection by analysis of clinical images using convolutional neural network. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 17–20 August 2016; pp. 1373–1376. [Google Scholar]
- Yu, L.; Chen, H.; Dou, Q.; Qin, J.; Heng, P.A. Automated melanoma recognition in dermoscopy images via very deep residual networks. IEEE Trans. Med. Imaging 2016, 36, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Codella, N.; Cai, J.; Abedini, M.; Garnavi, R.; Halpern, A.; Smith, J.R. Deep learning, sparse coding, and SVM for melanoma recognition in dermoscopy images. In Proceedings of the International Workshop on Machine Learning in Medical Imaging, Munich, Germany, 5 October 2015; pp. 118–126. [Google Scholar]
- Ma, Z.; Tavares, J.M.R. Effective features to classify skin lesions in dermoscopic images. Expert Syst. Appl. 2017, 84, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.R.; Giro-i Nieto, X.; Burdick, J.; Marques, O. Skin lesion classification from dermoscopic images using deep learning techniques. In Proceedings of the 2017 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017; pp. 49–54. [Google Scholar]
- Shoieb, D.A.; Youssef, S.M.; Aly, W.M. Computer-aided model for skin diagnosis using deep learning. J. Image Graph. 2016, 4, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Brinker, T.J.; Hekler, A.; Utikal, J.S.; Grabe, N.; Schadendorf, D.; Klode, J.; Berking, C.; Steeb, T.; Enk, A.H.; von Kalle, C. Skin cancer classification using convolutional neural networks: Systematic review. J. Med. Internet Res. 2018, 20, e11936. [Google Scholar] [CrossRef]
- Navarrete-Dechent, C.; Dusza, S.W.; Liopyris, K.; Marghoob, A.A.; Halpern, A.C.; Marchetti, M.A. Automated dermatological diagnosis: Hype or reality? J. Invest. Dermatol. 2018, 138, 2277–2279. [Google Scholar] [CrossRef] [Green Version]
- Han, S.S.; Kim, M.S.; Lim, W.; Park, G.H.; Park, I.; Chang, S.E. Classification of the clinical images for benign and malignant cutaneous tumors using a deep learning algorithm. J. Invest. Dermatol. 2018, 138, 1529–1538. [Google Scholar] [CrossRef] [Green Version]
- Han, S.S.; Lim, W.; Kim, M.S.; Park, I.; Park, G.H.; Chang, S.E. Interpretation of the Outputs of a Deep Learning Model Trained with a Skin Cancer Dataset. J. Invest. Dermatol. 2018, 138, 2275. [Google Scholar] [CrossRef] [Green Version]



| Class Label | Abbreviation | Super-Class Name | Np. of Images | No. of Sub-Classes |
|---|---|---|---|---|
| 0 | ACROS | Acne and Rosacea | 912 | 21 |
| 1 | AKBCC | Actinic Keratosis, Basal Cell Carcinoma, and other Malignant Lesions | 1437 | 60 |
| 2 | ATO | Atopic Dermatitis | 807 | 11 |
| 3 | BUL | Bullous Diseases | 561 | 12 |
| 4 | CEL | Cellulitis, Impetigo, and other Bacterial Infections | 361 | 25 |
| 5 | ECZ | Eczema Photos | 1950 | 47 |
| 6 | WXA | Exanthems and Drug Eruptions | 497 | 18 |
| 7 | ALO | Alopecia and other Hair Diseases | 195 | 23 |
| 8 | HER | Herpes, Genetal Warts and other STIs | 554 | 15 |
| 9 | PIG | Pigmentation Disorder | 711 | 32 |
| 10 | LUPUS | Lupus and other Connective Tissue diseases | 517 | 20 |
| 11 | MEL | Melanoma and Melanocytic Nevi | 635 | 15 |
| 12 | NAIL | Nail Fungus and other Nail Disease | 1541 | 48 |
| 13 | POI | Poison Ivy and other Contact Dermatitis | 373 | 12 |
| 14 | PSO | Psoriasis Lichen Planus and related diseases | 2112 | 39 |
| 15 | SCA | Scabies Lyme Disease and other Infestations and Bites | 611 | 25 |
| 16 | SEB | Seborrheic Keratoses and other Benign Tumors | 2397 | 50 |
| 17 | SYS | Systemic Disease | 816 | 43 |
| 18 | TIN | Tinea Candidiasis and other Fungal Infections | 1871 | 36 |
| 19 | URT | Urticaria | 265 | 9 |
| 20 | VASCT | Vascular Tumors | 603 | 18 |
| 21 | VASCP | Vasculitis | 569 | 17 |
| 22 | WARTS | Common Warts, Mollusca Contagiosa and other | 1549 | 26 |
| Total | 21844 | 622 | ||
| Class Label | Abbreviation | Class | Np. of Images |
|---|---|---|---|
| 0 | AKIEC | Bowen Disease | 334 |
| 1 | BCC | Basal Cell Carcinoma | 583 |
| 2 | BKL | Benign Keratosis-like Lesions | 1674 |
| 3 | DF | Dermatofibroma | 122 |
| 4 | MEL | Melanoma | 2177 |
| 5 | NV | Melanocytic Nevi | 18,618 |
| 6 | VASC | Vascular Lesions | 157 |
| Total | 23,665 | ||
| Class | Precision (%) | Sensitivity (%) | Specificity (%) | F-1 Score (%) | ||||
|---|---|---|---|---|---|---|---|---|
| Exp-1 | Exp-2 | Exp-1 | Exp-2 | Exp-1 | Exp-2 | Exp-1 | Exp-2 | |
| ACROS | 81.39 | 81.66 | 85.86 | 87.39 | 98.90 | 98.94 | 83.56 | 84.43 |
| AKBCC | 79.17 | 81.45 | 77.24 | 79.75 | 98.19 | 98.43 | 78.20 | 80.59 |
| ATO | 71.95 | 75.76 | 75.34 | 77.08 | 98.57 | 98.83 | 73.61 | 76.41 |
| BUL | 75.72 | 74.08 | 60.61 | 64.71 | 99.35 | 99.26 | 67.33 | 69.08 |
| CEL | 61.60 | 64.18 | 44.88 | 50.14 | 99.40 | 99.42 | 51.92 | 56.30 |
| ECZ | 75.19 | 78.41 | 81.59 | 83.79 | 96.69 | 97.24 | 78.26 | 81.01 |
| WXA | 62.99 | 65.17 | 64.39 | 67.00 | 98.88 | 98.97 | 63.68 | 66.07 |
| ALO | 76.96 | 81.19 | 85.64 | 84.10 | 99.70 | 99.78 | 81.07 | 82.62 |
| HER | 77.87 | 77.99 | 71.12 | 74.19 | 99.33 | 99.32 | 74.34 | 76.04 |
| PIG | 69.57 | 73.31 | 68.50 | 71.87 | 98.72 | 98.91 | 69.03 | 72.59 |
| LUPUS | 69.61 | 74.60 | 59.38 | 63.64 | 99.20 | 99.35 | 64.09 | 68.68 |
| MEL | 82.85 | 83.46 | 80.63 | 83.46 | 99.36 | 99.38 | 81.72 | 83.43 |
| NAIL | 89.64 | 89.08 | 88.71 | 90.01 | 99.00 | 98.95 | 89.17 | 89.53 |
| POI | 76.81 | 75.33 | 56.84 | 61.39 | 99.62 | 99.57 | 65.33 | 67.65 |
| PSO | 78.39 | 79.61 | 78.65 | 81.91 | 97.09 | 97.26 | 78.52 | 80.75 |
| SCA | 74.51 | 77.42 | 62.19 | 70.70 | 99.22 | 99.27 | 67.80 | 73.91 |
| SEB | 79.14 | 85.16 | 86.10 | 87.15 | 96.47 | 97.69 | 82.48 | 86.14 |
| SYS | 68.61 | 72.35 | 72.06 | 72.79 | 98.38 | 98.67 | 70.29 | 72.57 |
| TIN | 80.97 | 80.97 | 83.70 | 85.73 | 97.66 | 97.68 | 82.31 | 83.28 |
| URT | 75.67 | 78.21 | 75.09 | 75.85 | 99.62 | 99.68 | 78.38 | 77.01 |
| VASCT | 83.30 | 84.77 | 72.80 | 76.62 | 99.47 | 99.51 | 77.70 | 80.49 |
| VASCP | 72.43 | 77.24 | 74.34 | 75.75 | 99.03 | 99.26 | 73.37 | 76.49 |
| WARTS | 77.76 | 81.97 | 81.02 | 82.76 | 97.76 | 98.29 | 79.36 | 82.36 |
| Weighted Average | 71.81 | 79.82 | 77.53 | 79.94 | 98.14 | 98.40 | 77.34 | 79.80 |
| Standard Deviation | 06.46 | 05.89 | 11.20 | 09.83 | 00.95 | 00.75 | 08.42 | 07.72 |
| Class | Precision (%) | Sensitivity (%) | Specificity (%) | F1-Score (%) |
|---|---|---|---|---|
| Bowen Disease (AKIEC) | 80.43 | 78.74 | 99.71 | 79.58 |
| Basal Cell Carcinoma (BCC) | 91.85 | 86.96 | 99.79 | 89.34 |
| Benign Keratosis-like Lesions (BKL) | 85.55 | 77.48 | 98.95 | 81.32 |
| Dermatofibroma (DF) | 91.67 | 81.15 | 99.96 | 86.09 |
| Melanoma (MEL) | 84.64 | 66.05 | 98.75 | 74.20 |
| Melanocytic Nevi (NV) | 94.90 | 98.30 | 79.09 | 96.57 |
| Vascular Lesions (VASC) | 66.10 | 74.52 | 99.73 | 70.06 |
| Weighted Average | 85.02 | 80.46 | 96.57 | 82.45 |
| Standard Deviation | 09.10 | 09.38 | 07.15 | 08.38 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajwa, M.N.; Muta, K.; Malik, M.I.; Siddiqui, S.A.; Braun, S.A.; Homey, B.; Dengel, A.; Ahmed, S. Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks. Appl. Sci. 2020, 10, 2488. https://doi.org/10.3390/app10072488
Bajwa MN, Muta K, Malik MI, Siddiqui SA, Braun SA, Homey B, Dengel A, Ahmed S. Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks. Applied Sciences. 2020; 10(7):2488. https://doi.org/10.3390/app10072488
Chicago/Turabian StyleBajwa, Muhammad Naseer, Kaoru Muta, Muhammad Imran Malik, Shoaib Ahmed Siddiqui, Stephan Alexander Braun, Bernhard Homey, Andreas Dengel, and Sheraz Ahmed. 2020. "Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks" Applied Sciences 10, no. 7: 2488. https://doi.org/10.3390/app10072488