
Effects of Wearing a Swimming Cap and Goggles on Phoria and Fusional Vergence

Department of Optometry, Kangwon National University, Samcheok 25949, Korea
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(21), 10797; https://doi.org/10.3390/app122110797
Submission received: 1 August 2022
/
Revised: 23 September 2022
/
Accepted: 19 October 2022
/
Published: 25 October 2022
Abstract
:This study evaluated changes in phoria and negative (NFV) and positive fusional vergence (PFV) when wearing a cap and/or goggles. Thirty-five healthy university students aged 20–25 years participated in the study. All participants were examined for phoria, NFV, and PFV at distance and near. A rotary prism was used before and after wearing a cap, goggles, and both a cap and goggles. The frequency of overall average change in phoria, NFV, and PFV after wearing swimming equipment compared with non-wearing ranged from one-third to four-fifths. The order of frequency in change was wearing of goggles and a cap, goggles alone, and a cap alone. The frequency of a prism prescription, determined by the relationship between phoria and vergence, was similar or higher for wearing than for non-wearing and higher at near than at distance. The effect on change in phoria and fusional vergence was greater when wearing both a cap and goggles than when wearing either alone. These findings demonstrate that wearing both swimming cap and goggles that contact or attach around the eyes influence phoria and fusional vergence by inducing pressure or pulling. These changes may contribute to the discomfort associated with the wearing of swimming equipment.
1. Introduction
Binocular vision refers to the ability to focus on an object and perceive a single image by coordinated use of both the eyes. Binocular vision disorders associated with visual impairment [1,2], strabismus due to loss of coordination of movement between the two eyes [3], and impaired stereopsis [4] can affect vision-related quality of life and the ability to perform tasks of daily living. Furthermore, non-strabismic binocular vision disorders, including phoria other than strabismus, create lifestyle problems, and affect the quality of life of schoolchildren, producing symptoms that include discomfort, headaches, visual fatigue, blurred vision, double vision, word skip, and line skip [5,6]. Appropriate correction and eye protection are required to eliminate or reduce these symptoms in individuals with non-strabismic binocular vision disorders [5,7].
Even in the eyes that are not affected by non-strabismic binocular vision disorders, it is important to wear eye equipment, including spectacles, goggles, or face shields, which protect the eyes from hazardous factors, such as flying objects, hazardous liquids, gases, or other materials; or prescription corrective lenses to improve visual functions, such as visual acuity and contrast sensitivity, in everyday life, including when pursuing hobbies [8,9,10]. However, the wearing of equipment that protects the eye and face results in a reduced visual field and auditory reaction time [11,12], decreased eye–hand coordination [13], and an inability to see and respond to visual stimuli [14]. Furthermore, when a pair of swimming googles are worn, there is a decrease in central anterior chamber depth, anterior chamber volume, and anterior chamber angle [15], as well as a small but significant elevation in the intraocular pressure [16]. Moreover, the use of swimming goggles causes acute corneal thinning, reduction in the iridocorneal angle [17], and a reduction in break-up time [18].
Thus far, as mentioned above, studies of eye-related protective equipment have been limited to changes in ocular biometric parameters and ocular physiology, including the visual field, visual response, and intraocular pressure. Furthermore, despite the fact that goggles used for swimming, which is one of the most popular sports and health-related leisure activities [19,20], are eye protective and fit closely to the eyes. When evaluating non-strabismic binocular vision, it is essential to analyze the relationship between phoria and fusional vergence to maintain the zone of clear single binocular vision [21,22]. Phoria and fusional vergence are closely related to the extraocular muscle action required for binocular vision [23,24,25]. However, until now, there have been no studies on changes in phoria and fusional vergence induced by wearing of a cap and/or goggles while swimming.
The purpose of this study was to evaluate the changes in phoria and fusional vergence at distance (6 m) and near (40 cm) before and after wearing a cap and/or goggles. The study focused on horizontal phoria, negative (NPV) and positive fusional vergence (PFV), and prism prescription according to Sheard’s criterion.
2. Materials and Methods
2.1. Participants
The study participants were 35 healthy university students (24 males, 11 females) aged 20–25 years. The inclusion criteria were non-strabismic binocular vision, no history of refractive surgery, no strabismus or amblyopia, and no use of medication. Suppression was excluded while performing the phoria test without swimming equipment. However, suppression while wearing the swimming equipment was evaluated as the effect of wearing.
Minimum sample size was calculated using G*power 3.1 software (Version 3.1.9.4; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). Based on an alpha of 0.05, a statistical power of 0.80, an effect size of 0.10 corresponding to small as defined by Cohen [26], four study groups (non-wearing, wearing a swimming cap, wearing goggles, and wearing both), a number of repeated measures of 3, correlation among repeated measures of 0.80 with high correlation, and a non-sphericity correlation of 0.5 with the lowest value from 1/(number of repetitions—1), we calculated that a total sample of more than 108 (27 per study group) would be required for repeated-measures analysis of variance (ANOVA). A sample size of 36 per group was similarly needed in 3 of the study groups to compare the changes between non-wearing and wearing of swimming equipment. Therefore, to allow for comparison among 3 or 4 groups, 35 participants were determined as the sample size to allow for a number 10% larger than the mean of 27 and 36 participants.
This study was approved by the Kangwon National University Institutional Review Board (KWNUIRB-2021-04-002-001) and adhered to the tenets of the Declaration of Helsinki. All study participants provided written informed consent.
2.2. Swimming Equipment
The swimming cap (A0AC1AC20; Arena, Seoul, Korea) worn in the study was made of silicone, weighed approximately 32 g, and had a width of 22 cm and a height of 19 cm. The pairs of swimming goggles (AMAAG61; Arena) used by the participants were made of polycarbonate and silicone rubber, weighed approximately 26 g, had a front size of 17 cm × 5 cm × 4 cm (length × width × height), adjustable bridges with a distance between the centers of the lenses of 6.8 ± 0.4 cm, and oval-shaped, gray-tinted lenses with a horizontal width of 4 cm and a vertical width of 3 cm.
For all participants, the order of tests related to the wearing of swimming equipment was as follows: non-wearing, wearing a cap, wearing goggles, and wearing both a cap and pair of goggles according to the normal wearing order. Each testing was performed after a 5 min break. After wearing a cap, goggles, or both a cap and a pair of goggles, the relative mean (± standard deviation) weights measured by a portable scale (PHS-700; CAS Corporation, Jiashan, China) when pulling the band in the right temporal area by 1 cm were 400 ± 95 g, 464 ± 108 g, and 653 ± 90 g, respectively.
2.3. Clinical Refraction
The ocular health of all study participants was evaluated from their medical history, followed by ocular motility testing and a cover-uncover test to rule out strabismus. Static retinoscopy was performed using a retinoscope (Model 18245; Welch Allyn, Skaneateles Falls, NY, USA) while the participant watched a letter corresponding to 0.5 decimal visual acuity. Next, a fogging method was used to assess the subjective refraction, which was performed using a phoropter (Model 11625B; Reichert Technologies, Depew, NY, USA) and an LCD chart (LUCID’LC; Everview, Seoul, Korea) to find the best refractive correction at 6 m. Swimmers who require prescription spectacles wore the cap and/or goggles over their corrective contact lenses or goggles with corrective refractive power. Therefore, participants who required prescription spectacles wore spherical equivalent power-converted soft contact lenses instead of goggles with corrective refractive power. Prescriptions for eyeglasses with a vertex distance of 12 mm were converted to prescriptions for contact lenses. The soft contact lenses used in this study were disposable and made of etafilcon A with a base curve of 8.5 mm, a diameter of 14.2 mm, and a water content of 55%.
2.4. Measurement of Phoria and Fusional Vergence
For all study participants, the order in which the measurements were recorded after clinical refraction was distance phoria, near phoria, NFV at distance, PFV at distance, NFV at near, and PFV at near.
Both phoria and fusional vergence while wearing swimming goggles should be measurable in free space at distance (6 m) and at near (40 cm). To this end, the following conditions were required: a Howell phoria card for distance (3 m) (CDHPC; Cyclopean Design, Heathmont, VIC, Australia) and near (33.3 cm) (CDHPCN; Cyclopean Design) modified to 6 m (1 Δ, 1 prism diopter = 6 cm) and 40 cm (1 Δ = 0.4 cm). NFV and PFV were measured using handheld Risley rotary prisms (ARPHH30; Bernell, Mishawaka, IN, USA).
For the Howell phoria card, a 6 Δ base-down prism was placed in front of the right eye. In the lower chart image, the numbers on the right indicated by the arrow represent exophoria whereas the numbers on the left represent esophoria. Phoria was measured on three consecutive occasions at distance followed by at near.
The NFV values at distance and near were measured using the handheld Risley prisms. A single letter (0.5 decimal) was used for fixation at distance and at near. The Risley prisms were increased gradually at a speed of 1–2 Δ/s of base-in (BI) prism and participants were asked to report when the fixation object appeared to blur. If the participant reported a sustained blurring at a point then this point was considered a blur point. If the participant did not report any blurring but instead reported diplopia first, then there was deemed to be no blur point. The amount of prism was increased until the participant reported sustained double vision. The prism power was noted at the break point and the prism power was then gradually decreased. Thereafter, the point at which the patient regained single vision was recorded as the recovery point. Blur points, break points, and recovery points of PFV at distance and near were measured using handheld Risley base-out prisms. Changes were not analyzed because the blur points of NFV and PFV did not appear in many cases [27].
Sheard’s criterion requires the compensating vergence (PFV or base-out for exophoria; NFV or base-in for esophoria) to blur and to be twice the heterophoria. A prism can be prescribed if this criterion is not met. Clinically, the amount of prism that needed to be prescribed to meet Sheard’s criterion was determined as two-thirds the phoria minus one-third of the fusional vergence [28]. If there was no blur point, the break point was used instead.
The coefficient of repeatability was calculated by multiplying the standard deviation of differences between measurements by 1.96 to detect changes in phoria between measurements. Values within and outside the range of the coefficient of repeatability were determined to represent no change and change, respectively. Therefore, the respective criteria for change in phoria at distance and near were 1.10 Δ and 1.60 Δ. Applying the 95% limits of agreement (LOA) in rotary prism fusional vergence [29], the criteria for changes in fusional vergence were over 2.5 Δ for the break and recovery points of NFV at distance; over 4.0 Δ for the break point and 2.5 Δ for the recovery point of NFV at near; over 5.5 Δ for the break point and 5.0 Δ for the recovery point of PFV at distance; and over 4.0 Δ for the break point and 5.5 Δ for the recovery point of PFV at near.
2.5. Statistical Analysis
The Kolmogorov–Smirnov test was used to test for normality. Repeated-measures ANOVA followed by Bonferroni’s post hoc test was performed to evaluate the differences in phoria and fusional vergence among the participants wearing swimming equipment including a cap, goggles, or both a cap and a pair of goggles. In addition, an independent samples t-test was performed to compare the difference between wearing and non-wearing of soft contact lenses. The chi-squared test was used to evaluate whether there was a difference in changes according to the wearing of swimming equipment. Linear regression analysis (r2, the coefficient of determination) was used to explain changes in phoria and fusional vergence when wearing swimming equipment. Pearson’s correlation coefficient was used instead of the coefficient of determination when there was no relationship between one dependent variable and one or more independent variables. All statistical analyses were performed using MedCalc (Version 12.7.7.0; MedCalc Software, Ostend, Belgium). A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Participant Demographics and Vision Correction
Thirty-five study participants were assessed for changes in phoria and fusional vergence before and after wearing swimming equipment, namely, a cap and/or goggles. The demographics and refractive characteristics of the participants are presented in Table 1. The participants comprised a homogeneous group of university students with a mean (± standard deviation) age of 22.31 ± 1.71 years (range, 20–25). The proportions of participants with corrected and uncorrected refractive errors were 74.3% and 25.7%, respectively. The spherical equivalent of the soft contact lenses obtained by manifest refraction was −4.50 ± 2.72 D (range, −9.50, −0.50), the visual acuity at the spherical equivalent was 0.8 decimal (range, 0.5–1.2), and the visual acuity without refractive error was 1.1 decimal (range, 0.8–1.2), allowing for evaluation of phoria and fusional vergence.
3.2. Changes in Phoria and Fusional Vergence
To compare phorias before and after wearing the swimming equipment rather than the comparison between wearing spectacles and wearing contact lenses, we confirmed initially the mean difference for phorias between wearing (myopia) and non-wearing of soft contact lenses (emmetropia). No statistically significant difference was observed in phoria (Table 2).
Changes in phoria and fusional vergence, including NFV and PFV before and after wearing a cap, goggles, and both a cap and goggles for swimming, were analyzed as (1) the difference among means, (2) the frequency based on changes above the coefficient of repeatability or the 95% limits of agreement, and 3) the frequency of prism prescription based on Sheard’s criterion.
Table 3 shows the difference among the means for phoria and fusional vergence before and after wearing swimming equipment. Phoria is shown as plus for esophoria and minus for exophoria, and fusional vergence is presented as the blur, break, and recovery points. Blur points were excluded from the analysis because blur and no blur can coexist. Differences among the means for phoria, NFV, and PFV at distance and at near were not statistically significant (all p > 0.05, repeated-measures ANOVA). However, NFV at near and PFV at distance and at near while wearing a cap, goggles, or cap and goggles showed suppression in 1–6 cases. Furthermore, when analyzing changes based on non-wearing as a baseline, there were various cases in which an increase, decrease, and no change in phoria or fusional vergence occurred but without showing a definite tendency. Changes were observed in 1050 cases, namely, 84.7% (using cumulative values, 396 cases increased, 449 cases decreased, and 44 cases were suppressed). In 350 cases, the frequency of changes when wearing a cap, goggles, and both a cap and goggles were 86.0% (301 cases), 83.4% (292 cases), and 84.6% (296 cases), respectively. That is, on about four-fifths of occasions, changes in phoria and fusional vergence were a result of wearing the swimming equipment.
Criteria for changes in the coefficient of repeatability or 95% LOA in the present study were applied to analyze distinct changes using “existence” or “non-existence” as nominal variables rather than unclear changes. The results are shown in Table 4. Changes in phoria, NFV, and PFV at distance or at near according to whether a cap, goggles, or both a cap and goggles were worn were significant (subtotal, p < 0.001; chi-squared test). The frequency of changes in the overall average was 29.0% (range, 8.6–62.9). Approximately one third (34.9%, 122 of 350 cases) showed changes when wearing both a cap and goggles. Changes in phoria ranged from 17.1% when wearing a cap at distance to 45.7% when wearing both a cap and goggles at near. Changes in NFV at distance ranged from 25.7% at the recovery point when wearing goggles to 40.0% when wearing both a cap and goggles. Changes in NFV at near ranged from 8.6% at the break point when wearing a cap to 62.9% at the recovery point when wearing goggles. Changes in PFV at distance ranged from 14.3% at the recovery point when wearing a cap to 45.7% at the recovery point when wearing both a cap and goggles. Changes in PFV at near ranged from 14.3% at the break point when wearing a cap to 34.3% at the break or recovery point when wearing both a cap and goggles. The order of frequency for the subtotal was 34.9% when wearing both a cap and goggles, 30.6% when wearing goggles alone, and 21.4% when wearing a cap alone. The results of comparison using the chi-squared test between wearing goggles versus wearing both a cap and goggles were statistically significant more often than between wearing a cap versus goggles and wearing a cap versus both a cap and goggles.
As shown in Table 5, the frequency of a prism prescription based on Sheard’s criterion was 20.0–22.9% at distance and 42.9–51.4% at near when wearing swimming equipment, which was higher than that of 17.1% at distance and 42.9% at near when not wearing swimming equipment (all p < 0.05, chi-squared test), and that of a prism description was higher at near than at distance when wearing this equipment. The frequency of a prism prescription at distance was higher when wearing goggles, and the frequency at near was higher when wearing both a cap and goggles than when wearing a cap or goggles or when wearing no swimming equipment. All between-group differences were statistically significant (p < 0.05, chi-squared test).
3.3. Relationships between Changes in Phoria and Fusional Vergence
The relationship between a cap and goggles was not evaluated based on the coefficient of determination (r2) because the dependency could not be defined, but was evaluated using Pearson’s correlation coefficient (r), which quantifies the interdependency between a cap and goggles. The effect of wearing a cap and wearing goggles on wearing both a cap and goggles was evaluated based on the coefficient of determination, which is the proportion of the variation in wearing a cap and goggles that is predictable from wearing a cap alone and goggles alone. From these analyses, we found that the correlation between wearing a cap and goggles was significant in phoria at distance, in the NFV for break and recovery at near, and in the PFV for break and recovery at distance. The explanatory power of the effect on wearing both a cap and goggles was greater for wearing goggles (r2 = 0.278–0.692) than for wearing a cap (r2 = 0.158–0.482) in the evaluation by coefficient of determination.
Relationships between wearing a swimming cap, goggles, and both a cap and goggles in terms of changes in phoria at distance and near are shown in Figure 1. Pearson’s correlation coefficient between cap and goggles was significant at distance (Figure 1a: r = 0.644, p < 0.001). The coefficients of determination for wearing both a cap and goggles were larger when wearing goggles than when wearing a cap at distance and near (Figure 1b: r2 = 0.581, p < 0.001; Figure 1e: 0.692, p < 0.001).
Relationships between wearing a swimming cap, goggles, and both a cap and goggles for changes in NFV at distance and near are shown in Figure 2. Pearson’s correlation coefficient between cap and goggles was not significant for the break and recovery points at distance (Figure 2a,d), but was significant for the break and recovery points at distance (Figure 2g: r = 0.672, p < 0.001; Figure 2j: 0.511, p = 0.002). The coefficients of determination for the break and recovery points of wearing both a cap and goggles were larger when wearing goggles than when wearing a cap at distance and near (Figure 2b: r2 = 0.542, p < 0.001; Figure 2h: 0.468, p < 0.001; Figure 2k: 0.417, p < 0.001), except for the recovery point when wearing a cap at distance (Figure 2f: r2 = 0.461, p < 0.001).
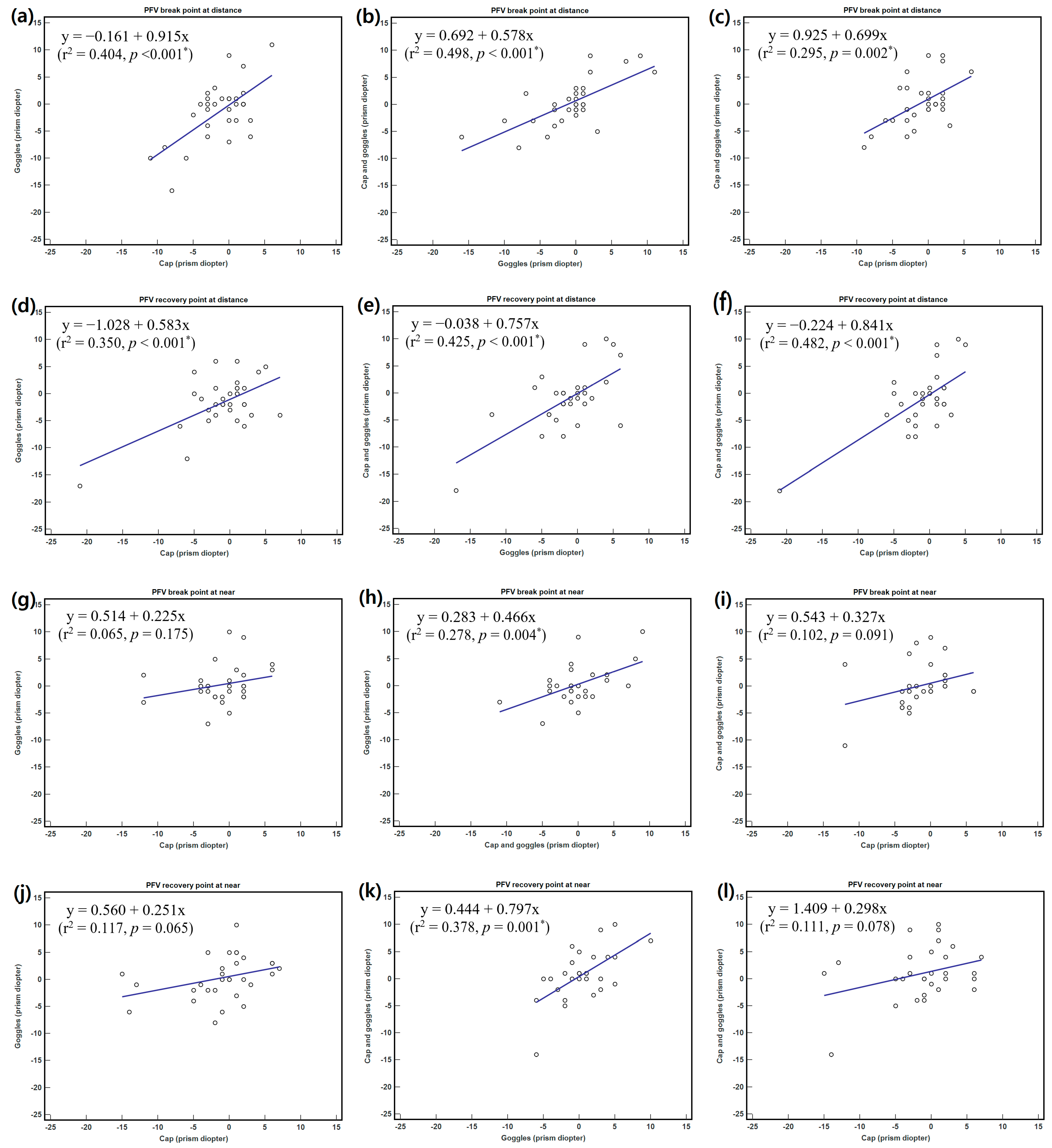
Relationships between a swimming cap, goggles, and both a cap and goggles for changes in PFV at distance and near are shown in Figure 3. Pearson’s correlation coefficient between cap and goggles was significant for the break and recovery points at distance (Figure 3a,d: r = 0.636, p < 0.001; 0.591, p < 0.001), but not for the break and recovery points at distance (Figure 3g,j). The coefficients of determination for break and recovery points of wearing both a cap and goggles were larger when wearing goggles than when wearing a cap at distance and near (Figure 3b: r2 = 0.498, p < 0.001; Figure 3h: 0.278, p = 0.004; Figure 3k: 0.378, p = 0.001), except for the recovery point when wearing a cap at distance (Figure 3f: r2 = 0.482, p < 0.001).
Table 6 shows the results of the correlation analysis performed to determine the relationship between phoria and the relative weight loaded. Phoria showed low positive correlations with wearing both a cap and goggles at distance and wearing goggles at near (r = 0.426, p = 0.011; 0.345, p = 0.042), and did not show a significant relationship with wearing a cap. The change in phoria according to the relative weight loaded showed a different tendency at distance and near.
4. Discussion
Although this study of a homogeneous group of healthy university students was not performed while the participants were swimming, its findings show that wearing swimming equipment can change phoria and fusional vergence by at least one-third to at most four-fifths. The factors of change seen when wearing both a cap and goggles suggest that wearing a pair of goggles has a greater influence than wearing a swimming cap. These findings have important implications, given that the changes in visual function may be the factor associated with discomfort while wearing a swimming cap and/or goggles.
This study included 26 participants (74.3%) with visual acuity corrected using the spherical equivalent, although not maximum plus to maximum visual acuity, of 0.5 to 1.2 decimal, and 9 participants (25.7%) with uncorrected visual acuity of 0.8 to 1.2 decimal, excluding the participants with strabismus, amblyopia, or suppression while not wearing swimming equipment. In all participants who met these criteria, it was possible to evaluate phoria and fusional vergence with visual acuity that met the setting conditions in procedures of measurement for phoria and fusional vergence [30,31].
4.1. Changes in Phoria and Fusional Vergence
Phoria and fusional vergence measurements are important parameters for evaluating the binocular function [21,22]. Our study evaluated the changes in phoria and fusional vergence before and after wearing of swimming equipment regardless of whether contact lenses were worn (myopia) or not (emmetropia). Although the changes associated with the wearing of contact lenses in myopia included more esophoric shift and poorer accommodative and vergence functions than the wearing of spectacles [32], the effect of the difference between wearing and non-wearing of contact lenses could be measured regardless of the changes in phoria and fusional vergence caused by the wearing of contact lenses and spectacles. In the previous results based on phoria, the differences between wearing and non-wearing of contact lenses were found to be insignificant. Therefore, it would be more appropriate to analyze both wearing (myopia) and non-wearing of contact lenses (emmetropia) rather than analyzing them separately. In addition, it was reported that phoria was changed in the esophoric shift of 0.85 ∆ for 5°– 1.93 ∆ for 25° when a lens having the same refractive power as that of goggles had a face form angle [33]. However, we did not take this effect into account because the swimming goggles with plano lenses over the contact wear had the minimal effect of the face form angle.
In the evaluation of changes in phoria, NFV, and PFV at distance and near among non-wearing, wearing a cap, wearing goggles, and wearing both a cap and a pair of goggles, there were no statistically significant differences in the means for phoria, NFV, or PFV. However, variations in the frequencies of increase, decrease, and no change compared to non-wearing were observed, albeit without a specific tendency. The changes in phoria and fusional vergence while wearing swimming equipment were approximately four-fifths and were occasionally accompanied by suppression. Randomness in the direction of these changes is attributed to the swimming equipment touching or attaching around the eyes.
A variety of changes, especially in phoria, have been found in other studies performed under different conditions. In a study of the effect of lid elevation on the results of the cross-cover test [34], 76% of the eyes developed phoria when lifting a lid, and the horizontal deviations were rarely exophoria and most were esophoria. The study investigators suggested that lifting the lid produced an iatrogenic phoria that mimics a skew or paresis of cranial nerve IV. An unsurprising finding in another study [35] was that the effects of lifting the lid varied from subject to subject because different subjects had different degrees of laxity in the pulley system and in the soft tissue attaching the lid to the system. In studies of eye movement or changes in ocular biometric parameters and ocular physiology owing to other causes, blinking was accompanied by eye movements, such as rotation in the horizontal, vertical, and torsional planes because of the extra co-contraction of the inferior and superior rectus muscles [36], and the eye blink rate was increased in the head-mounted display environment as the far/near-distance exophoria increased [37]. In other studies related to wearing swimming goggles [38,39], the headband tension of the goggles transmitted into the orbit through the rubber seal of the frames of the goggles increased the orbital tissue pressure, compressing the globe and leading to an elevation in the intraocular pressure. In another study of change in visual perception and balance caused by different types of hats [40], it was demonstrated that visual perception was lower while wearing a hat than when not wearing a hat. Furthermore, another study found that vision and sensory performance was negatively impacted by wearing a helmet rather than a hat [13].
Inferring factors of change from previous studies, our study demonstrates that a swimming cap and goggles that touch or are attached around the eyes affect phoria and fusional vergence by pressing or pulling.
The coefficient of repeatability or 95% LOA can be applied as an exclusion criterion to distinguish distinct from borderline changes in phoria, NFV, and PFV [29]. In our study, phoria and fusional vergence were changed by approximately one-third when wearing swimming equipment. The frequency of changes in the overall average for phoria, NFV, and PFV was 29.0% and increased to 34.9% when wearing both a cap and goggles. Changes in phoria were larger at near than at distance, and larger in the order of wearing both a cap and googles, goggles alone, and a cap alone. These results likely reflect the magnitude of the pressure on the eyes. However, the change in fusional vergence varied and there was no specific trend. The significance of the change between wearing goggles alone and wearing both a cap and goggles was greater than that among other wearing groups. This finding means that wearing goggles has a greater impact, probably because the pressure and position of the goggles is closer to the eyes rather than that of the cap, which is further away from the eyes. Moreover, there are reports demonstrating that wearing both swimming cap and goggles cause headache and increased intraocular pressure [38,41,42]. A headache caused by pressure applied over the scalp or forehead by goggles or a tight swim cap would be unusual, and a more likely explanation would be the compression of nerve endings from the branches of the trigeminal and occipital nerves [41,42]. A report of a patient showed a decrease in the air pressure between a pair of swimming goggles and the eye up on removal of the swimming goggles [43]. This effect could be explained by the increased external pressure on the goggles, which would most likely increase the pressure on the eye [38]. As in other studies, our findings indicate that wearing a swimming cap and a pair of goggles may affect the visual function by pressing on the eye or the temporal and supraorbital nerve regions.
4.2. Changes in Prism Prescription
A prism prescription is useful for allowing more comfortable fusion in patients with strabismus or a non-strabismic binocular disorder [44]. Changes in phoria and fusional vergence that occur when wearing swimming equipment place demands on the wearer’s fusion system. The frequency of a prism prescription, which is determined by the relationship between phoria and fusional vergence, can be an indicator of a change in this relationship. Although a prism prescription relies upon the criteria devised by Sheard [21] and Percival [45], we chose the Sheard’s criterion because it is readily accepted in optometry, although the Percival criterion is more effective for esophoria at near. When measuring PFV and NFV at near and distance, subjects can be expected to notice the blur point [46]. However, if a study participant does not report a blur, the prism value used in Sheard’s criterion should be the break point instead of the blur point [31].
Our results show that the frequency of a prism prescription based on Sheard’s criterion was similar to or 1.2–1.3 times higher when wearing than when not wearing swimming equipment. In addition, the frequency of a prism prescription was 1.9–2.6 times higher at near than at distance. Although the difference in frequency between non-wearing, wearing a cap, wearing goggles, and wearing both a cap and goggles was small, the chi-squared test found a significant difference according to the presence or absence of a prescription. In particular, the frequency of a prism prescription was higher when wearing goggles than when wearing a cap at distance and higher when wearing both a cap and goggles than when wearing a cap alone at near. As mentioned above, goggles are more likely to have a significant effect on pressure than a swimming cap because they are worn closer to the eyes.
4.3. Relationship between Swimming Equipment and Visual Changes
When we evaluated the relationships between changes in phoria and fusional vergence when wearing a cap and goggles, a correlation of change in phoria and PFV was found at distance but not at near, and the correlation of change in NFV was found at near but not at distance. Therefore, in terms of the correlation of cap and goggles with phoria, it is likely that wearing this swimming equipment affects PFV at distance and NFV at near, regardless of phoria at near. For fusion of both the eyes when wearing a cap and goggles, interaction between phoria and PFV at distance seems to be related to voluntary convergence (moving the eyes inwards to see closer objects clearly), and the interaction between phoria and NFV at near seems to be related to voluntary divergence (moving the eyes outward to see objects that are further away) [47].
To evaluate the relative contribution of the cap and the goggles when wearing both a cap and goggles, the explanatory power was defined by the coefficient of determination and evaluated by linear regression analysis. The explanatory power for wearing both a cap and goggles was greater than for wearing goggles or for wearing a cap, except for the NFV recovery point at distance and PFV recovery point at near. These results suggest that the effects of the periocular pressure exerted by the goggles were greater than that exerted by pulling of the eyelids by the cap. As previously discussed, it appears that the pressure exerted in the orbital tissue by the rubber seal on the goggle frames [38] is greater than that exerted by pulling of the eyelids by the cap [34].
The effect of the load on phoria was low or insignificant but did have an effect when wearing goggles. In particular, the effect of wearing goggles alone was greater than that when wearing both a cap and goggles at near. This finding can be explained by the fact that the pulling effect of the cap and the pressure effect of the goggles are slightly offset when wearing both a cap and goggles, whereas wearing only goggles prevents the common natural phenomenon of narrowing of the palpebral fissures on downgaze at near fixation [48,49].
In this study, changes in phoria and fusional vergence when wearing swimming equipment were affected by the wearing position, the pressure exerted, and the fixation distance, and the influence of goggles was considered to be substantial. The discomfort experienced by our study participants is consistent with that in another study, in which subjects reported subjective symptoms of poor visual acuity, asthenopia, and gait disturbance when wearing swimming goggles [50]. It is noteworthy that our present findings are based on data obtained over a short period of time. Actual swimming sessions last much longer, and the visual discomfort caused by swimming caps and googles is likely to be worse than that detected in this study.
This study has some limitations. We did not evaluate changes in the effect of full correction rather than the spherical equivalent power on phoria and fusional vergence while swimming. Furthermore, we did not investigate whether these changes returned to baseline levels after removal of the swimming equipment. However, these limitations are unlikely to have influenced our results because the rotation of the astigmatism axis with full correction and the dynamic movements involved in swimming are likely to have acted as factors of change. In addition, the vergence demands on the wearer’s fusion system may create more discomfort to the swimmers than simply the wearing of the swimming equipment.
5. Conclusions
According to the criteria of change applied in this study, phoria and fusional vergence showed a frequency of change, including suppression, in the order of one-third to four-fifths when wearing swimming equipment. The frequency of a prism prescription was similar or 1.2–1.3 times higher when wearing than when non-wearing, and 1.9–2.6 times higher at near than at distance when wearing. Changes in phoria and fusional vergence were greater when both a cap and goggles were worn than when only a cap was worn, probably because goggles are closer to the eyes and exert greater pressure on the eyes than a cap, which is further away from the eyes. A swimming cap and goggles that touch or attach around the eyes affect phoria and fusional vergence by pressing or pulling. Our findings suggest that changes in visual function associated with wearing a swimming cap and/or goggles may contribute to the discomfort caused by wearing this type of swimming equipment and have important implications.
Author Contributions
Conceptualization, D.-S.Y. and S.-C.P.; methodology, D.-S.Y., S.-C.P. and H.-G.C.; validation, D.-S.Y., S.-C.P. and H.-G.C.; formal analysis, S.-C.P. and S.-Y.K.; investigation, S.-C.P. and H.-G.C.; resources, S.-C.P. and B.-Y.M.; data curation, S.-C.P. and B.-Y.M.; writing—original draft preparation, review and editing, S.-C.P., D.-S.Y., H.-G.C. and B.-Y.M.; visualization, B.-Y.M. and S.-Y.K.; supervision, D.-S.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Kangwon National University Institutional (KWNUIRB-2021-04-002-001, 6 May 2021).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Asaoka, R.; Crabb, D.P.; Yamashita, T.; Russell, R.A.; Wang, Y.X.; Garway-Heath, D.F. Patients have two eyes!: Binocular versus better eye visual field indices. Invest. Ophthalmol. Vis. Sci. 2011, 52, 7007–7011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yibekal, B.T.; Alemu, D.S.; Anbesse, D.H.; Alemayehu, A.M.; Alimaw, Y.A. Vision-related quality of life among adult patients with visual impairment at University of Gondar, Northwest Ethiopia. J. Ophthalmol. 2020, 2020, 9056097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatt, S.R.; Leske, D.A.; Kirgis, P.A.; Bradley, E.A.; Holmes, J.M. The effects of strabismus on quality of life in adults. Am. J. Ophthalmol. 2007, 144, 643–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuang, T.M.; Hsu, W.M.; Chou, C.K.; Tsai, S.Y.; Chou, P. Impact of stereopsis on quality of life. Eye (Lond). 2005, 19, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Chandra, P.; Akon, M. Non-strabismic binocular vision abnormalities. J. Ophthalmol. Vis. Sci. 2016, 1, 1006. [Google Scholar]
- Hu, J.; Wang, G.; Zhou, Z.; Sun, Y.; Zhang, Q.; Wu, J.; Gao, Y. Evaluation of a novel quality of life scale for schoolchildren with nonstrabismic binocular vision anomalies. Biomed. Res. Int. 2020, 2020, 4723402. [Google Scholar] [CrossRef]
- Cacho Martínez, P.; García Muñoz, A.; Ruiz-Cantero, M.T. Treatment of accommodative and nonstrabismic binocular dysfunctions: A systematic review. Optometry 2009, 80, 702–716. [Google Scholar] [CrossRef]
- Dain, S.J. Materials for occupational eye protectors. Clin. Exp. Optom. 2012, 95, 129–139. [Google Scholar] [CrossRef]
- Eppig, T.; Speck, A.; Zelzer, B.; Langenbucher, A. Protective glasses. Personal eye protection for professional use. Ophthalmologe 2014, 111, 681–691. [Google Scholar] [CrossRef]
- Hoskin, A.K.; Mackey, D.A.; Keay, L.; Agrawal, R.; Watson, S. Eye Injuries across history and the evolution of eye protection. Acta Ophthalmol. 2019, 97, 637–643. [Google Scholar] [CrossRef]
- Miller, B.A.; Miller, S.J. Visual fields with protective eyewear. J. Orthop. Sports Phys. Ther. 1993, 18, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.K.; Kaur, M.; Choity, M. Effect of helmet use on visual and auditory reaction time and peripheral field of vision. Natl. J. Physiol. Pharm. Pharmacol. 2019, 9, 307–311. [Google Scholar] [CrossRef]
- Kramer, M.R.; Teel, E.F.; Wasserman, E.B.; Mihalik, J.P. Effect of protective helmets on vision and sensory performance in healthy men. Athletic Train. Sports Health Care 2021, 13, 130–135. [Google Scholar] [CrossRef]
- Kramer, M.R.; Wasserman, E.B.; Teel, E.F.; Mihalik, J.P. Effect of protective helmets on vision and sensory performance. Br. J. Sports Med. 2017, 51, A65. [Google Scholar] [CrossRef]
- Ma, K.T.; Chung, W.S.; Seo, K.Y.; Seong, G.J.; Kim, C.Y. The effect of swimming goggles on intraocular pressure and blood flow within the optic nerve head. Yonsei Med. J. 2007, 48, 807–809. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wang, H.; Nie, Y.; Li, W. Short-Term Effects of Two Types of Goggles on Intraocular Pressure and Anterior Eye Segment Biometrics. BMC Ophthalmol. 2021, 22, 73. [Google Scholar] [CrossRef]
- Jiménez, R.; Molina, R.; García, J.A.; Redondo, B.; Vera, J. Wearing swimming goggles reduces central corneal thickness and anterior chamber angle, and increases intraocular pressure. Curr. Eye Res. 2020, 45, 535–541. [Google Scholar] [CrossRef]
- Vera, J.; Redondo, B.; Molina, R.; Jiménez, R. Effects of wearing swimming goggles on non-invasive tear break-up time in a laboratory setting. J. Optom. 2022, 15, 535–541. [Google Scholar] [CrossRef]
- Chase, N.L.; Sui, X.; Blair, S.N. Comparison of the health aspects of swimming with other types of physical activity and sedentary lifestyle habits. Int. J. Aquatic Res. Educ. 2008, 2, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Chan, D.K.C.; Lee, A.S.Y.; Hamilton, K. Descriptive epidemiology and correlates of children’s swimming competence. J. Sports Sci. 2020, 38, 2253–2263. [Google Scholar] [CrossRef]
- Sheard, C. Zones of ocular comfort. Am. J. Optom. 1930, 7, 9–25. [Google Scholar] [CrossRef]
- Michaels, D.D. Indications for prescribing spectacles. Surv. Ophthalmol. 1981, 26, 55–74. [Google Scholar] [CrossRef]
- Shaunak, S.; O’Sullivan, E.; Kennard, C. Eye movements. J. Neurol. Neurosurg. Psychiatry 1995, 59, 115–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demer, J.L.; Clark, R.A.; Crane, B.T.; Tian, J.R.; Narasimhan, A.; Karim, S. Functional anatomy of the extraocular muscles during vergence. Prog. Brain Res. 2008, 171, 21–28. [Google Scholar] [PubMed] [Green Version]
- Gupta, S.K.; Aparna, S. Effect of yoga ocular exercises on binocular vision functions. Optom. Vis. Perf. 2019, 7, 229–237. [Google Scholar]
- Prajapati, B.; Dunne, M.C.M.; Armstrong, R.A. Sample size estimation and statistical power analyses. Optometry Today 2010, 50, 1–9. Available online: https://www.researchgate.net/publication/265399772_Sample_size_estimation_and_statistical_power_analyses (accessed on 25 January 2022).
- Scheiman, M.; Herzberg, H.; Frantz, K.; Margolies, M. A normative study of step vergence in elementary schoolchildren. J. Am. Optom. Assoc. 1989, 60, 276–780. [Google Scholar]
- Worrell, B.E., Jr.; Hirsch, M.J.; Morgan, M.W. An evaluation of prism prescribed by Sheard’s criterion. Am. J. Optom. Arch. Am. Acad. Optom. 1971, 48, 373–376. [Google Scholar] [CrossRef]
- Penisten, D.K.; Hofstetter, H.W.; Goss, D.A. Reliability of rotary prism fusional vergence ranges. Optometry 2001, 72, 117–122. [Google Scholar]
- Anstice, N.S.; Davidson, B.; Field, B.; Mathan, J.; Collins, A.V.; Black, J.M. The repeatability and reproducibility of four techniques for measuring horizontal heterophoria: Implications for clinical practice. J. Optom. 2021, 14, 275–281. [Google Scholar] [CrossRef]
- Goss, D.A.; Becker, E. Comparison of near fusional vergence ranges with rotary prisms and with prism bars. Optometry 2011, 82, 104–107. [Google Scholar] [CrossRef]
- Jiménez, R.; Martínez-Almeida, L.; Salas, C.; Ortíz, C. Contact lenses vs spectacles in myopes: Is there any difference in accommodative and binocular function? Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Ko, D.Y.; Kim, K.H.; Lee, D.H. Clinical evaluation on variation of face form angle of eyewear. J. Korean Ophthalmic Opt. Soc. 2015, 20, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M.L.; Gizzi, M.S. The effect of lid elevation on the cross-cover test. J. Neuroophthalmol. 2001, 21, 87–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.M. Understanding and misunderstanding extraocular muscle pulleys. J. Vis. 2007, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bour, L.J.; Aramideh, M.; de Visser, B.W. Neurophysiological aspects of eye and eyelid movements during blinking in humans. J. Neurophysiol. 2000, 83, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kumar, Y.S.; Yoo, J.; Kwon, S. Change of blink rate in viewing virtual reality with HMD. Symmetry 2018, 10, 400. [Google Scholar] [CrossRef] [Green Version]
- Morgan, W.H.; Cunneen, T.S.; Balaratnasingam, C.; Yu, D.Y. Wearing swimming goggles can elevate intraocular pressure. Br. J. Ophthalmol. 2008, 92, 1218–1221. [Google Scholar] [CrossRef] [Green Version]
- Plaut, G.S. Diplopia in a swimmer due to badly fitting goggles. Postgrad. Med. J. 1998, 74, 607. [Google Scholar] [CrossRef] [Green Version]
- Roh, H. Change in visual perception and balance caused by different types of hat. J. Phys. Ther. Sci. 2014, 26, 199–201. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, J.C., Jr. Swimmer’s headache, or supraorbital neuralgia. Proc. Bayl. Univ. Med. Cent. 2004, 17, 418–419. [Google Scholar] [CrossRef] [Green Version]
- Krymchantowski, A.V. Headaches due to external compression. Curr. Pain Headache Rep. 2010, 14, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Wakely, L.A.; Reeves, G.; Ashraff, N.; Wells, A.P. Swimming goggles suck. Br. J. Ophthalmol. 2004, 88, 1600–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frantz, K.A. Prescribing relieving prism for patients with binocular vision disorders. J. Optometr. Vision Dev. 1997, 28, 54–67. [Google Scholar]
- Percival, A. The Prescribing of Spectacles, 3rd ed.; John Wright & Sons: Bristol, UK, 1928; pp. 102–109. Available online: https://archive.org/details/b21287405/page/102 (accessed on 21 January 2022).
- Antona, B.; Barrio, A.; Barra, F.; Gonzalez, E.; Sanchez, I. Repeatability and agreement in the measurement of horizontal fusional vergences. Ophthalmic Physiol. Opt. 2008, 28, 475–491. [Google Scholar] [CrossRef] [Green Version]
- Eskridge, J.B. An investigation of voluntary vergence. Am. J. Optom. Arch. Am. Acad. Optom. 1971, 48, 741–746. [Google Scholar] [CrossRef]
- Stoller, S.H.; Meyer, D.R. Quantitating the change in upper eyelid position during downgaze. Ophthalmology 1994, 101, 1604–1607. [Google Scholar] [CrossRef]
- Read, S.A.; Collins, M.J.; Carney, L.G.; Iskander, D.R. The morphology of the palpebral fissure in different directions of vertical gaze. Optom. Vis. Sci. 2006, 83, 715–722. [Google Scholar] [CrossRef]
- Chu, B.S. Assessment of visual satisfaction and visual function with prescription swimming goggles in-air and underwater. J. Korean. Oph. Opt. Soc. 2013, 18, 357–363. [Google Scholar] [CrossRef]
Figure 1.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in phoria at distance and near. (a) Cap vs. goggles, (b) goggles vs. cap and goggles, (c) cap vs. cap and goggles at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.
Figure 1.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in phoria at distance and near. (a) Cap vs. goggles, (b) goggles vs. cap and goggles, (c) cap vs. cap and goggles at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.

Figure 2.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in break and recovery points of negative fusional vergence at distance and near. (a) Cap vs. goggles, (b) goggles vs. cap and goggles, and (c) cap vs. cap and goggles for the NFV break point at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles for the NFV recovery point at distance; (g) cap vs. goggles, (h) goggles vs. cap and goggles, and (i) cap vs. cap and goggles for the NFV break point at near; (j) cap vs. goggles, (k) goggles vs. cap and goggles, and (l) cap vs. cap and goggles for the NFV recovery point at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.
Figure 2.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in break and recovery points of negative fusional vergence at distance and near. (a) Cap vs. goggles, (b) goggles vs. cap and goggles, and (c) cap vs. cap and goggles for the NFV break point at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles for the NFV recovery point at distance; (g) cap vs. goggles, (h) goggles vs. cap and goggles, and (i) cap vs. cap and goggles for the NFV break point at near; (j) cap vs. goggles, (k) goggles vs. cap and goggles, and (l) cap vs. cap and goggles for the NFV recovery point at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.

Figure 3.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in in break and recovery point of positive fusional vergence (PFV) at distance and near. (a) cap vs. goggles, (b) goggles vs. cap and goggles, and (c) cap vs. cap and goggles for the PFV break point at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles for the PFV recovery point at distance; (g) cap vs. goggles, (h) goggles vs. cap and goggles, and (i) cap vs. cap and goggles for the PFV break point at near; (j) cap vs. goggles, (k) goggles vs. cap and goggles, and (l) cap vs. cap and goggles for the PFV recovery point at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.
Figure 3.
Regression analyses between a swimming cap, goggles, and both a cap and goggles for changes in in break and recovery point of positive fusional vergence (PFV) at distance and near. (a) cap vs. goggles, (b) goggles vs. cap and goggles, and (c) cap vs. cap and goggles for the PFV break point at distance; (d) cap vs. goggles, (e) goggles vs. cap and goggles, and (f) cap vs. cap and goggles for the PFV recovery point at distance; (g) cap vs. goggles, (h) goggles vs. cap and goggles, and (i) cap vs. cap and goggles for the PFV break point at near; (j) cap vs. goggles, (k) goggles vs. cap and goggles, and (l) cap vs. cap and goggles for the PFV recovery point at near. R-squared (r2) is the coefficient of determination. * p < 0.05 indicates a statistically significant finding.

{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographic and refractive characteristics of the study participants.
| Mean ± SD | Range | |
|---|---|---|
| All participants (n) | 35 | |
| Age (years) | 22.31 ± 1.71 | 20–25 |
| Male/female (n) | 24/11 | |
| Manifest refraction (n) | 26 | |
| Spherical power | −4.29 ± 2.91 D | −9.75–0.50 D |
| Cylindrical power | −1.38 ± 0.81 D | −3.50–−0.25 D |
| Spherical equivalent | −4.91 ± 3.07 D | −11.00–−0.50 D |
| Refractive correction with soft contact lenses | 26 | |
| Spherical equivalent | −4.50 ± 2.72 D | −9.50–−0.50 D |
| Visual acuity (decimal) | 0.8 (0.7–1.0) 1 | 0.5–1.2 |
| Visual acuity (logMAR) | 0.09 ± 0.09 | −0.0–0.30 |
| No refractive error (n) | 9 | |
| Visual acuity (decimal) | 1.1 (1.0–1.2) 1 | 0.8–1.2 |
| Visual acuity (logMAR) | −0.04 ± 0.05 | −0.08–0.10 |
| Myopia after wearing soft contact lenses (n) | 26 | |
| Phoria at distance (∆) 2 | −1.46 ± 3.07 | −8.33–6.33 |
| Phoria at near (∆) | −5.08 ± 6.32 | −16.00–10.00 |
| Emmetropia after non-wearing of soft contact lenses (n) | 9 | |
| Phoria at distance (∆) | −1.33 ± 2.06 | −6.00–0.67 |
| Phoria at near (∆) | −5.71 ± 5.72 | −13.00–1.00 |
1 Deviation of the SD based on decimal calculated from the SD of the logMAR; 2 Plus and minus signs as prism diopter (∆) indicate esophoria and exophoria, respectively. logMAR = logarithm of the minimum angle of resolution; SD = standard deviation.
Table 2.
Differences in phoria between wearing (myopia) and non-wearing of soft contact lenses (emmetropia).
Table 2.
Differences in phoria between wearing (myopia) and non-wearing of soft contact lenses (emmetropia).
| Soft Contact Lenses | p-Value | ||
|---|---|---|---|
| Wearing (Myopia) | Non-Wearing (Emmetropia) | ||
| Non-wearing of swimming equipment | |||
| Distance | −1.46 ± 3.07 | −1.33 ± 2.06 | 0.913 |
| Near | −5.08 ± 6.32 | −5.71 ± 5.72 | 0.794 |
| Wearing cap | |||
| Distance | −1.13 ± 3.50 | −1.19 ± 2.36 | 0.964 |
| Near | −4.35 ± 6.50 | −4.63 ± 6.28 | 0.913 |
| Wearing goggles | |||
| Distance | −1.49 ± 3.09 | −1.41 ± 2.38 | 0.940 |
| Near | −4.43 ± 5.34 | −5.00 ± 5.95 | 0.789 |
| Wearing cap and goggles | |||
| Distance | −1.45 ± 3.09 | −1.17 ± 2.49 | 0.807 |
| Near | −4.66 ± 5.37 | −5.52 ± 6.89 | 0.703 |
Data are shown as the mean ± standard deviation (∆, prism diopter). Plus and minus signs indicate esophoria and exophoria, respectively.
Table 3.
Differences in phoria and fusional vergence between wearing and non-wearing of swimming cap and goggles.
Table 3.
Differences in phoria and fusional vergence between wearing and non-wearing of swimming cap and goggles.
| a. Non-wearing (n) | b. Cap (n: +, −, 0) 1 | c. Goggles (n: +, −, 0) | d. Cap + Goggles (n: +, −, 0) | p-Value | |
|---|---|---|---|---|---|
| Phoria 2 | |||||
| Distance | −1.42 ± 2.82 (35) | −1.14 ± 3.21 (14, 13, 8) | −1.47 ± 2.89 (12, 18, 5) | −1.38 ± 2.91 (14, 18, 3) | 0.204 |
| Near | −5.24 ± 6.10 (35) | −4.42 ± 6.35 (22, 9, 4) | −4.58 ± 5.42 (21, 11, 3) | −4.88 ± 5.70 (16, 15, 4) | 0.084 |
| NFV at distance | |||||
| Blur (n, blur vs. no blur) | (9:26) | (6:29) | (13:22) | (6:29) | |
| Break | 10.26 ± 3.22 (35) | 10.63 ± 4.65 (16, 14, 5) | 11.00 ± 4.41 (16, 11, 8) | 11.03 ± 4.85 (14, 13, 8) | 0.435 |
| Recovery | 6.40 ± 3.22 (35) | 6.09 ± 2.78 (13, 18, 4) | 6.26 ± 3.21 (13, 13, 9) | 7.03 ± 3.44 (16, 12, 7) | 0.190 |
| NFV at near | Suppression (n = 2) | Suppression (n = 2) | |||
| Blur (n, blur vs. no blur) | (11:24) | (7:28) | (5:30) | (8:27) | |
| Break | 17.54 ± 6.38 (35) | 17.51 ± 6.12 (16, 16, 3) | 16.30 ± 5.38 (8, 20, 5) | 17.09 ± 4.64 (10, 17, 6) | 0.052 |
| Recovery | 12.91 ± 5.55 (35) | 12.63 ± 5.35 (14, 15, 6) | 11.67 ± 4.84 (9, 19, 5) | 12.79 ± 4.40 (11, 17, 5) | 0.072 |
| PFV at distance | Suppression (n = 1) | Suppression (n = 2) | Suppression (n = 4) | ||
| Blur (n, blur vs. no blur) | (21:14) | (15:20) | (11:24) | (9:26) | |
| Break | 14.00 ± 6.33 (35) | 12.53 ± 6.20 (12, 16, 6) | 12.55 ± 6.47 (11, 14, 8) | 13.61 ± 5.55 (12, 14, 5) | 0.263 |
| Recovery | 9.57 ± 5.55 (35) | 8.62 ± 5.46 (15, 15, 4) | 8.03 ± 5.15 (10, 19, 4) | 8.26 ± 4.75 (9, 17, 5) | 0.378 |
| PFV at near | Suppression (n = 5) | Suppression (n = 6) | |||
| Blur (n, blur vs. no blur) | (6:29) | (5:30) | (4:31) | (5:30) | |
| Break | 14.77 ± 5.75 (35) | 13.31 ± 5.51 (10, 20, 5) | 14.77 ± 6.36 (10, 13, 7) | 15.10 ± 6.85 (10, 14, 5) | 0.286 |
| Recovery | 9.77 ± 5.83 (35) | 8.54 ± 5.51 (13, 18, 4) | 9.97 ± 6.35 (14, 12, 4) | 11.00 ± 6.19 (15, 8, 6) | 0.220 |
Data are shown as the mean ± standard deviation (∆, prism diopter). Values in parentheses represent the number of participants. 1 Changes based on non-wearing as a baseline; 2 Plus and minus signs indicate esophoria and exophoria, respectively; NFV = negative fusional vergence; PFV = positive fusional vergence.
Table 4.
Frequency of changes in phoria and in negative and positive fusional vergence.
| a. Cap | b. Goggles | c. Cap + Goggles | Subtotal Average | p-Value | |||
|---|---|---|---|---|---|---|---|
| a vs. b | b vs. c | a vs. c | |||||
| Phoria | |||||||
| Distance | 6 (17.1%) | 7 (20.0%) | 9 (25.7%) | 22/105 (21.05%) | 0.010 * | 0.009 * | 0.326 |
| Near | 9 (25.7%) | 10 (28.6%) | 16 (45.7%) | 35/105 (33.3%) | 0.099 | 0.003 * | 0.009 * |
| NFV at distance | |||||||
| Break | 10 (28.6%) | 13 (37.1%) | 10 (28.6%) | 33/105 (31.4%) | 0.167 | 0.034 * | 0.003 * |
| Recovery | 10 (28.6%) | 9 (25.7%) | 14 (40.0%) | 33/105 (31.4%) | 0.427 | 0.134 | 0.056 |
| NFV at near | |||||||
| Break | 3 (8.6%) | 7 (20.0%) | 7 (20.0%) | 17/105 (16.2%) | 0.880 | 0.027 * | 0.174 |
| Recovery | 13 (37.1%) | 22 (62.9%) | 17 (48.6%) | 52/105 (49.5%) | 0.336 | 0.204 | 0.897 |
| PFV at distance | |||||||
| Break | 7 (20.0%) | 12 (34.3%) | 12 (34.3%) | 31/105 (29.5%) | 0.006 * | 0.001 * | 0.006 * |
| Recovery | 5 (14.3%) | 8 (22.9%) | 13 (45.7%) | 26/105 (24.8%) | 0.007 * | 0.035 * | 0.101 |
| PFV at near | |||||||
| Break | 5 (14.3%) | 10 (28.6%) | 12 (34.3%) | 27/105 (25.7%) | 0.939 | 0.001 * | 0.827 |
| Recovery | 7 (20.0%) | 9 (25.7%) | 12 (34.3%) | 28/105 (26.7%) | 0.772 | <0.001 * | 0.423 |
| Subtotal average | 75/350 (21.4%) | 107/350 (30.6%) | 122/350 (34.9) | 304/1050 (29.0%) 1 | <0.001 * | <0.001 * | <0.001 * |
Data are shown as the number (percentage) of participants. 1 Overall average; * p < 0.05, statistically significant between-group difference (chi-squared test); NFV = negative fusional vergence; PFV = positive fusional vergence.
Table 5.
Frequency of changes in prism prescription based on Sheard’s criterion.
| Distance | Near | |
|---|---|---|
| Non-wearing | 6 (17.1%) | 15 (42.9%) |
| a. Cap | 7 (20.0%) | 16 (45.7%) |
| b. Goggles | 8 (22.9%) | 15 (42.9%) |
| c. Cap + goggles | 7 (20.0%) | 18 (51.4%) |
| p-value | ||
| Non-wearing vs. cap | 0.010 * | <0.001 * |
| Non-wearing vs. goggles | 0.023 * | 0.001 * |
| Non-wearing vs. cap + goggles | 0.010 * | 0.001 * |
| Cap vs. goggles | <0.001 * | <0.001 * |
| Goggles vs. cap + goggles | <0.001 * | <0.001 * |
| Cap vs. cap + goggles | <0.001 * | <0.001 * |
Data are shown as the number (percentage) of a prism prescription. * p < 0.05, statistically significant between-group difference (chi-squared test).
Table 6.
Pearson’s correlation coefficient between phoria and the relative weight loaded.
| Relative Weight | r (p-Value) | ||
|---|---|---|---|
| Mean ± SD (g) | Phoria at Distance | Phoria at Near | |
| Cap | 400 ± 95 | 0.163 (0.350) | 0.023 (0.896) |
| Goggles | 464 ± 108 | 0.314 (0.066) | 0.345 (0.042 *) |
| Cap + goggles | 653 ± 90 | 0.426 (0.011 *) | 0.225 (0.194) |
* p < 0.05 indicates a statistically significant result.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Park, S.-C.; Cho, H.-G.; Moon, B.-Y.; Kim, S.-Y.; Yu, D.-S. Effects of Wearing a Swimming Cap and Goggles on Phoria and Fusional Vergence. Appl. Sci. 2022, 12, 10797. https://doi.org/10.3390/app122110797
AMA Style
Park S-C, Cho H-G, Moon B-Y, Kim S-Y, Yu D-S. Effects of Wearing a Swimming Cap and Goggles on Phoria and Fusional Vergence. Applied Sciences. 2022; 12(21):10797. https://doi.org/10.3390/app122110797
Chicago/Turabian StylePark, Seung-Chul, Hyun-Gug Cho, Byeong-Yeon Moon, Sang-Yeob Kim, and Dong-Sik Yu. 2022. "Effects of Wearing a Swimming Cap and Goggles on Phoria and Fusional Vergence" Applied Sciences 12, no. 21: 10797. https://doi.org/10.3390/app122110797
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.