
Changes of Gait Patterns after Correction of Refractive Error in the Elderly with Cataracts

Department of Optometry, College of Health Science, Kangwon National University, Samcheok-si 25949, Republic of Korea
*
Author to whom correspondence should be addressed.
Appl. Sci. 2023, 13(10), 6140; https://doi.org/10.3390/app13106140
Submission received: 5 April 2023
/
Revised: 10 May 2023
/
Accepted: 16 May 2023
/
Published: 17 May 2023
Abstract
:The aim of this study was to verify whether providing older adults with actual corrected glasses for refractive errors would have a positive impact on their gait patterns. This study included 30 subjects with an average age of 78.77 ± 7.27 years. The measurement of gait patterns was performed using the Optogait analysis system, and a comparative analysis was performed to compare the patients before and after they wore correction glasses. Step length, stride length, and width showed significant increases after the patients wore correction glasses, and cadence showed a decrease compared to before they wore correction glasses (p < 0.05). A strong positive correlation was observed between step length and stride length (r = 0.779, p < 0.001), and a decrease in cadence (r = −0.686, p < 0.001) was observed with increasing step length. In addition, a proportional increase in speed with increasing step length was observed after the patients wore correction glasses (r = 0.416, p < 0.05). The correction of residual refractive errors in order to provide optimal visual information can have a positive effect on gait patterns. Therefore, efforts by optometry professionals to provide the accurate correction of refractive errors in elderly patients can contribute to the prevention of falls, and collaboration with other experts is needed.
1. Introduction
Gait is a fundamental and natural aspect of human movement involving periodic physical movement [1]. The synchronization of various types of sensory information is essential for the maintenance of stable movements while walking. First, the vestibular system has a function in recognizing the senses involved in rotational movements and linear acceleration during walking. Second, the position and velocity of all body parts, contact with external objects, and direction of gravity are determined by the somatic system, which functions as a sensor. Finally, information about the surroundings, locations of obstacles, and ground conditions is collected by the visual system [2]. In general, the evaluation of gait patterns is based on the temporal and spatial characteristics of the gait cycle. Step length, stride length, walking velocity, and cadence are factors that can have an effect on gait patterns. Gait patterns can vary depending on the ground conditions [3], with the occurrence of significant changes in walking velocity and step length according to physiological factors such as aging [4] and gender [5]. Step width is related to balance control, and an increase in step width will lead to greater stability, making this a possible compensation for instability [6]. In addition, pathological causes such as stroke, arthritis, diabetes, and Parkinson’s disease can destabilize gait patterns [7,8].
The modification of gait patterns by using visual information occurs through feedback mechanisms from various pathways. Walking velocity is usually influenced by the flow of visual stimuli. As reported by Lackner and DeZio, their study’s participants showed increased stride length after the rotation speed of an optokinetic drum was doubled [9]. Figueiro et al. [10], who performed an analysis of changes in gait patterns according to lighting conditions, reported that walking velocity was decreased and step length showed a significant decrease under dark lighting conditions. In a study on vision problems that can affect gait patterns, Elliot et al. [11] reported on simulated cataracts, including data on decreased visual acuity and contrast sensitivity, and a narrow visual field; they found that even young adults can be affected through increases in the frequency of collisions with obstacles and deviations from intended walking paths. According to Kim [12], as a result of visual impairments, individuals with congenital low vision are not able to learn appropriate concepts regarding movement during the process of development. Visual impairment can be a cause of walking errors such as collisions, errors made at intersection crossings and road crossings, and significantly reduced walking stability and delayed walking time. Therefore, the maintenance of a stable gait requires the prediction of future movements along with awareness of the current surroundings and the ability to adapt to changing surroundings. The acquisition of appropriate and continuous visual information is essential [13].
Refractive errors are the most common causes of visual blur, which occurs when parallel rays that have entered through the eyes fail to focus on an image on the retina while the ciliary muscle is in a relaxed state [14]. Although refractive errors are common, they may not be considered a serious problem because they do not cause fatal problems compared to other eye diseases. Visual blur caused by refractive errors can interfere with the acquisition of appropriate visual information for the maintenance of a stable gait; however, until recently, research on refractive errors and gait patterns has been limited due to the aforementioned prejudice. The authors of the present paper previously investigated the effects of refractive errors by type on static postural control and fall risk [15,16,17]. We reported that astigmatic blur had negative effects on postural control [15], and that when the hyperopic refractive error condition was induced, despite maintaining visual acuity without glasses of power 1.0 or higher, the participants reported a decrease in postural stability compared to when their condition was fully corrected [16]. Moreover, in an earlier study, we had found that postural stability was significantly improved compared to before wearing correction glasses [17]. Based on our previous research results, we considered that postural stability studies analyzed in a static state should be further expanded to gait analysis studies in order to analyze whether the correction of refractive errors can be used as an effective optical intervention for fall prevention. We previously studied changes in gait patterns under experimental conditions wherein different types of refractive errors were induced in young adult subjects [18]. Although our recent research yielded meaningful results, the results were obtained under limited experimental conditions. In addition, the results of a study that included healthy young adult subjects with low risk of falls were limited to application to the elderly population. Therefore, in the present study, we attempted to determine whether wearing glasses for the correction of distance visual acuity can have a positive effect on gait patterns among elderly subjects who have not worn correction glasses during the past year.
2. Materials and Methods
2.1. Subjects
A total of 30 elderly subjects with a mean age of 78.77 ± 7.27 years, who had not worn corrective lenses during the passing year (in order to exclude the effects of adaptation and habituation due to the experience of wearing glasses) and were able to walk independently without the aid of assistive devices, were selected for inclusion in this study. A questionnaire was administered in order to confirm that the subjects had no histories of frequent falls or balance-related conditions such as neuro-musculoskeletal conditions, systemic diseases, or related medication. All participants had received a diagnosis of age-related cataracts in one or both eyes from an ophthalmologist; however, our selection was limited to those who had not undergone cataract surgery. The average of spherical equivalent refractive powers in the binocular was S + 0.13 ± 0.77 D (ranging from S − 1.50 D to + 2.19 D), and the mean astigmatism was C − 0.72 ± 0.56 D (ranging from C − 0.00 to − 2.00 D). The average visual acuity in the binocular without glasses was 0.64 ± 0.23, and the average visual acuity in the binocular with glasses was 0.82 ± 0.19. All participants received appropriate verbal and written explanations of the purpose and methods of the study and their consent was obtained prior to the conduction of the experiment.
2.2. Evaluation of Gait Patterns
The measurement of changes in gait patterns before and after the correction of refractive errors was performed using the Optogait gait analysis system (Optogait, Microgate, Bolzano, Italy). Optogait consists of two transmission and reception bars, each 1 m long, with light-emitting diodes installed at 1-cm intervals on one bar. Two bars are installed facing each other, enabling extension up to 100 m [19]. The analysis of various gait patterns can be performed using continuous infrared communication sent from the transmission bar to the reception bar. This system can be used for the evaluation of both natural walking and walking on a treadmill. The analysis of the factors affecting gait patterns included step length (cm), stride length (cm), and stride width (cm), as well as cadence (steps/min) and walking velocity (s/m), as shown in Figure 1. Step length indicates the distance by which the foot can move forward during each swing. Stride length is the distance between two successive placements of the same foot, and it consists of two step lengths—left and right—each of which is the distance by which the named foot moves forward in front of the other one. Step width indicates the side-to-side distance between the lines of the two feet, measured usually at the midpoint of the backs of the heels but sometimes below the centers of the ankle joints. Finally, cadence is the number of steps taken in a given time, with the usual unit being steps per minute, and walking velocity is the distance covered by the whole body in a given time [20].
2.3. Experimental Procedures
An objective refraction was performed on the subjects using a retinoscope (Retinoscope, WelchAllyn, Auburn, NY, USA) and a 6-m LCD chart (LUCID’LC, Everview, Seoul, Republic of Korea), and a subjective refraction test was then performed using a manual phoropter (Ultramatic RX Master, Reichert, Depew, NY, USA). The endpoint of refractive correction was determined by MPMVA (Maximum to Plus Maximum Visual Acuity) [21], and the visual acuity was recorded as the corresponding decimal visual acuity when reading more than four numbers in each decimal visual acuity line, wherein there are five numbers in one line in order to represent each decimal visual acuity level. The tests were performed by a skilled examiner, and the measurement of each subject’s corrective power for refractive errors was performed. Based on the measured correction powers, each subject received glasses made for the correction of distance. In many previous studies, the paths of walking test was performed at 5 m or less, and its effectiveness was also proven [22,23]. In addition, the reproducibility of the Optogait system has been confirmed by previous studies [24]. In this experiment, the actual walking distance was 7 m in total (the start and end points were placed at a 1-m distance in order to reduce the effects of acceleration/deceleration) and the evaluation walking distance was 5 m. For the measurement of changes in gait patterns before and after participants wore correction glasses, two Optogait measuring bars were extended to 5 m and installed facing each other on both sides of the walking path. Each subject were instructed to walk in their normal manner while focusing on a target located ahead of them. A randomized order of measurement before and after the participants wore correction glasses was utilized for each individual in order to avoid effects caused by familiarity with the use of the devices. Each subject was allowed a rest period of 5 min in order to avoid fatigue before the second measurement. An analysis of the collected data was performed to determine whether wearing the correction glasses had resulted in significant changes in gait patterns among the elderly subjects.
2.4. Analysis of Measurements
The analysis of data was performed using SPSS for Windows (Ver. 24.0, SPSS Inc., Chicago, IL, USA). Paired t-tests were performed for the comparison of the mean values of each evaluation element before and after the participants wore glasses for the correction of distance visual acuity. Pearson’s correlation analysis was performed for the analysis of the correlation between factors of visual measurement and gait patterns. A p-value of less than 0.05 was considered statistically significant in all analyses.
3. Results
3.1. The Effect of Correction Glasses for Distance on Gait Patterns in Elderly Subjects
The changes in each factor that had an effect on gait patterns before and after wearing correction glasses for the elderly participants in this study are shown in Table 1. In the participants, the mean step length increased from 45.57 ± 5.37 cm to 47.78 ± 5.81 cm (p < 0.05), and the mean stride length increased from 89.09 ± 10.41 cm before wearing correction glasses to 94.09 ± 12.57 cm after wearing correction glasses (p < 0.05). The mean cadence decreased from 108.16 ± 12.59 before the participants wore correction glasses to 102.67 ± 19.74 (p < 0.05) after, and the step width changed from 10.21 ± 2.07 cm before the participants wore correction glasses to 10.93 ± 1.68 cm after they wore correction glasses (p < 0.05). However, no significant difference in the average walking velocity was observed before and after the participants wore glasses for the correction of distance (p > 0.05).
3.2. Analysis of Correlation between Change in Step Length and Each Gait Pattern
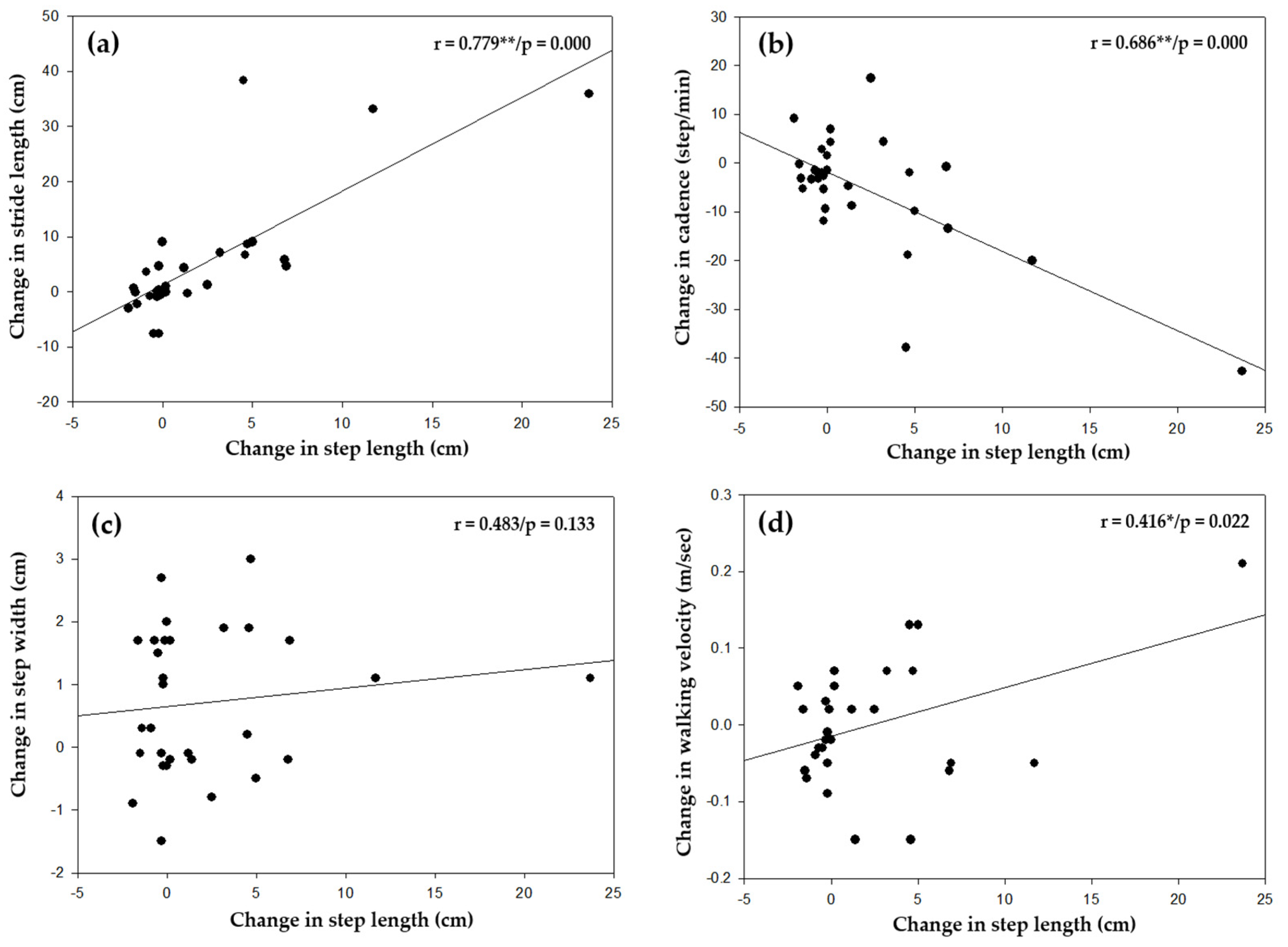
Correlation analysis was performed in order to examine possible associations between the changes in other factors affecting gait pattern, including stride length, cadence, width, and walking velocity, and change in step length after the participants wore correction glasses (Figure 2). The results showed a strong positive correlation between step length and stride length (r = 0.779/p = 0.000, Figure 2a), with a decrease in cadence (r = 0.686/p = 0.000, Figure 2b) along with increasing step length. Despite an increase in step length, no effect on step width was observed; however, a proportional correlation was observed between walking velocity and increasing step length (r = 0.416/p = 0.022, Figure 2d).
3.3. Analysis of Correlation between the Factors of Visual Measurements and Gait Patterns
An analysis was performed to determine the correlation between each gait pattern and the spherical equivalent power, astigmatic diopter power, and improvement of visual acuity lines after the participants wore correction glasses, as shown in Table 2. No clear correlation was observed between any factors affecting the gait pattern that were measured in this study and the subjects’ refractive error component and increase in corrected visual acuity.
4. Discussion
The visual system is an essential sensory organ that enables stable posture control and gait by continuously providing body position information through the recognition of objects and the surrounding environment [25]. A decrease in gait ability is unavoidable in the elderly due to physiological age-related degenerative changes, as well as the deterioration of the senses including the visual system and cognitive functions. For this reason, each specialized field is making efforts to prevent fall accidents in the elderly by identifying the causes of gait stability deterioration and proposing the necessary solutions. The objective of this study was to verify whether there is a positive effect on gait patterns after providing the elderly who have cataracts with actual corrected glasses for refractive errors. Based on this, we would like to emphasize the social role of optometrists and the necessity of collaboration with related specialists to improve gait ability in the elderly and prevent fall accidents.
Changes in gait patterns can develop as a result of the decline of the sensory-motor system, pelvic rotation, extension of the hip joint, and a decrease in the types of exercise that can be performed due to joint damage, pain, and fear of falling, all of which affect the elderly [26,27]. In such situations reduced walking velocity is a common compensatory action for the maintenance of gait stability [28]. A strategy of shortening the step length is employed and adapted to the pattern in cases where walking velocity cannot be reduced [29]. Previous studies have demonstrated that changes in gait patterns can be a result of poor visual information. Patla et al. [30] reported that when walking, patients with age-related macular degeneration take shorter steps than normal individuals. According to Wood et al. [31], decreased contrast sensitivity can be a cause of changes in gait patterns, leading to reduced walking velocity and step length. In particular, for people with this condition, the narrowing of the visual field occurs while climbing up and down stairs, and thus distinguishing the edge position or distance of the floor can be difficult for them, resulting in slower walking velocities and shorter step lengths [32].
As shown in Table 1, changes in gait pattern were observed when the participants were wearing correction glasses, with longer mean step and stride lengths, decreased cadence, and wider step width compared to what the participants had shown before wearing the glasses. In our previous study that included healthy young adult subjects [18,33], which compared a fully corrected condition to induced myopia of S + 1.00 D for both eyes and induced hyperopia of S − 1.00 D for both eyes, step length showed a significant decrease, while cadence increased, with expansion of the area of body sway during the process of walking in both anterior–posterior and left–right directions. Based on these findings, we can confirm that changes in habitual gait patterns can occur regardless of age as a result of uncorrected refractive errors. Step width is related to balance control and increased gait stability, and it can be an important factor in gait analysis. Brach et al. [34] suggest that extreme (either too little or too much) step width variability is associated with falls in elderly people who walk at or near normal gait speed and not in in the elderly who walk slowly. Although the step width increased after the participants wore correction glasses in this study, the degree of change was very small, and so there is a limit when it comes to suggesting clinical significance.
An analysis of the correlation between changes in step length and different factors affecting gait patterns was here performed in order to determine the cause of changes in gait patterns resulting from the correction of residual refractive errors in elderly subjects (Figure 2). A correlation was observed between an increase in step length after wearing correction glasses and an increase in stride length (r = 0.779/p = 0.000, Figure 2a), which resulted in a decrease in cadence (r = − 0.686/p = 0.000, Figure 2b). A proportional increase in speed with increasing step length was observed with regard to walking velocity after the participants wore correction glasses (r = 0.416/p = 0.022, Figure 2d). The degeneration of foot and ankle joint function in the elderly is a major cause of postural instability and the increased risk of falls [35]. As suggested by Lee and Lishman [36], the ability to process information from feet and ankle joints might decrease with aging, leading to greater dependence on visual information in order to maintain balance. According to the findings of our previous study [37], elderly subjects showed improved synchronization in the left foot as a whole and for both heels, both forefeet, and the left forefoot and right heel after wearing correction glasses. The improvement of static postural stability through the maintenance of the somatic system and enhancement of the capacity for sensory integration was also observed. Therefore, based on the results of our previous research as well as those of this study, the positive effects of correcting refractive errors in elderly patients are not limited to the ability to maintain posture but also extend to gait patterns for mobility. These findings should be considered important for professionals who perform analysis of balance and gait models or are involved in administration of rehabilitation therapy for the accurate diagnosis and treatment of elderly patients. In particular, the findings of this study, which was not conducted under the same experimental conditions employed in our previous studies (in other words, the participants in this study had not previously worn correction glasses), demonstrated that merely wearing correction glasses can result in a more stable change in gait patterns in the elderly; thus, the clinical implications are significant [18,33].
In addition, we examined changes in the gait patterns of the participants in order to determine the effect of refractive error components and visual improvement after vision corrections (Table 2). According to our findings, the level of spherical equivalent power and astigmatic diopter power had no influence on the subjects’ gait patterns. Despite the improvement of the average of visual acuity in the binocular from the scenarios without glasses (0.64 ± 0.23) to the average of visual acuity in the scenarios with glasses (0.82 ± 0.19), no clear correlation was observed between visual improvement and gait patterns. Thus, we were able to confirm the effectiveness of wearing correction glasses for the maintenance of gait stability in our elderly subjects regardless of the level of corrected visual acuity and the degree of refractive error. However, in this study, there were limitations in the ranges of visual improvement due to age-related cataracts in one or both eyes in the patients, and the range of refractive errors was also limited. Therefore, the conduction of additional studies is required in order to perform a more accurate analysis.
Visual information is essential in the process of adapting to various surroundings and modifying gait patterns. As a proactive strategy during adaptation for walking, by utilizing one’s sense of vision, potential obstacles in the surroundings can be predicted and thereby avoided during forward movement [38]. The proactive control of vision during movement is classified according to strategies for avoidance and accommodation. Strategies for avoidance involve shifting foot placement in an effort to adapt to the surroundings, increasing foot lift from the ground in order to avoid obstacles, and changing the direction of movement or stopping in order to avoid obstacles. Therefore, the accurate correction of refractive errors in the elderly can facilitate the initiation of visual scans of the surroundings, which could result in the development of more efficient proactive strategies for adaptation to walking with minimal consumption of energy. For humans, the optimal walking speed minimizes the consumption of energy per unit of distance. Walking at a slower or faster speed can cause a disruption of the optimal walking model, thus requiring much higher consumption of energy [39]. Based on the findings of this study, the authors would like to emphasize that improving the visual correction status in elderly patients can result in more efficient processing of visual information through the initiation of scans of the surroundings, leading ultimately to the stabilization of gait patterns.
Globally, 30% of the elderly population aged 65 years or older have experienced falls, and recurrent falls have been reported in half of them [40]. Jack et al. [41] reported that visual problems were present in 76% of elderly patients hospitalized for fall incidents, and in 79% of them, was able to recover their vision via either the correction of refractive error (40%) or cataract surgery (37%). Hospitalization for fall treatment increases the medical costs and socioeconomic burden associated with poor quality of life for the elderly [42]. Therefore, through the results of this study, gait rehabilitation experts should also recognize that appropriate optical correction for refractive error is an important factor leading to the prevention of frequent falls in the elderly by improving gait stability.
This study has the following limitations. First, because the measurements used in the analysis of the results were taken immediately after the participants wore correction glasses, there was no consideration of adaptation effects that might occur after the participants wore correction glasses. Second, no analysis of the effects of major visual functions, such as contrast sensitivity and stereopsis, on gait patterns in the elderly subjects was performed. Finally, the establishment of correlations between each participant’s body balance and factors affecting gait patterns will be required in order to determine the specific causes of changes in gait patterns after the correction of refractive errors. The conduction of follow-up studies to address these limitations is currently underway.
5. Conclusions
The results of an analysis of changes in gait patterns after the correction of refractive errors in elderly subjects showed an increase in step and stride lengths and width, a decrease in cadence, and an increase in walking velocity, resulting in overall stable gait patterns. Moreover, a proportional correlation was observed between walking velocity and increasing step length. Results showing such changes in gait patterns after the correction of refractive errors are expected to have a positive effect on the prevention of falls in the elderly. Therefore, an optimal gait model can be maintained via the correction of even mild cases of uncorrected refractive errors in the elderly.
Falls, which represent a significant threat to public health, are also associated with substantial social and medical costs. Thus, the prevention of falls is an urgent matter requiring attention from various specialties. Therefore, efforts by optometry professionals to provide the accurate correction of refractive errors in the elderly can contribute to the prevention of falls, and closer collaboration with other relevant experts is needed.
Author Contributions
Conceptualization, J.-H.N.; methodology, J.-H.N. and S.-Y.K.; validation, J.-H.N., H.-G.C., D.-S.Y., B.-Y.M. and S.-Y.K.; investigation, J.-H.N. and S.-Y.K.; resources, J.-H.N., H.-G.C., D.-S.Y., B.-Y.M. and S.-Y.K.; data curation, J.-H.N. and S.-Y.K.; writing—original draft preparation, J.-H.N.; writing—review and editing, J.-H.N., H.-G.C., D.-S.Y., B.-Y.M. and S.-Y.K.; visualization, J.-H.N., H.-G.C., D.-S.Y., B.-Y.M. and S.-Y.K.; supervision, S.-Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Kangwon National University Institutional Review Board (KWNUIRB 2018-04-004-008) and conducted in accordance with the tenets of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all participants included in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kim, J.H.; Oh, T.Y. The comparison of characteristics of foot pressure between treadmill and ground walking in normal person. J. Korean Phys. Ther. 2010, 5, 53–61. [Google Scholar]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Lim, W.S.; Ryu, T.B.; Choi, H.W.; Chung, M.K. A comparison of gait characteristics between korean and western young people. J. Ergon. Soc. Korea 2006, 25, 33–41. [Google Scholar]
- Beom, J.W. Characteristics of elderly gait. Korean Soc. Prosthet. Orthot. 2014, 8, 29–32. [Google Scholar]
- Yamasaki, M.; Sasaki, T.; Torii, M. Sex difference in the pattern of lower limb movement during treadmill walking. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 62, 99–103. [Google Scholar] [CrossRef]
- Gabell, A.; Nayak, U.S.L. The effect of age and variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly people living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Josephson, K.R.; Robbins, A.S. Falls in the nursing home. Ann. Intern. Med. 1994, 121, 442–451. [Google Scholar] [CrossRef]
- Lackner, J.R.; DiZio, P. Visual stimulation affects the perception of voluntary leg movements during walking. Perception 1998, 17, 71–80. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Plitnick, B.; Rea, M.S.; Gras, L.Z.; Rea, M.S. Lighting and perceptual cues: Effects on gait measures of older adults at high and low risk for falls. BMC Geriatr. 2011, 11, 49. [Google Scholar] [CrossRef]
- Elliott, D.B.; Bullimore, M.A.; Patla, A.E.; Whitaker, D. Effect of a cataract simulation on clinical and real world vision. Br. J. Ophthalmol. 1996, 80, 799–804. [Google Scholar] [CrossRef]
- Kim, J.H. A Study on travel errors of children with low vision. Korean J. Vis. Impair. 2005, 21, 27–41. [Google Scholar]
- Patla, A.E.; Vickers, J.N. Where and when do we look as we approach and step over an obstacle in the travel path. Neuroreport 1997, 8, 3661–3665. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.; Ellwein, L. Prevalence of refractive error in the United States, 1999–2004. Arch. Ophthalmol. 2008, 126, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Moon, B.Y.; Cho, H.G. Changes in falling risk depending on induced axis directions of astigmatism on static posture. J. Phys. Ther. Sci. 2015, 27, 1971–1973. [Google Scholar] [CrossRef]
- Moon, B.Y.; Choi, J.H.; Yu, D.S.; Kim, S.Y. Effect of induced hyperopia on fall risk and Fourier transformation of postural sway. PeerJ 2019, 7, e8329. [Google Scholar] [CrossRef]
- Bae, J.I.; Yu, D.S.; Kim, S.Y. Effect of optical correction by fully corrected glasses on postural stability. PLoS ONE 2020, 15, e0235919. [Google Scholar] [CrossRef]
- Choi, J.H.; Cho, H.G.; Moon, B.Y.; Yu, D.S.; Kim, S.Y. Changes in the gait pattern depending on induced refractive error and correlation analysis of visual functions. J. Korean Opthalmic. Opt. Soc. 2020, 25, 299–306. [Google Scholar] [CrossRef]
- Bernal, A.G.; Becerro-de-Bengoa-Vallejo, R.; Losa-lglesias, M.E. Reliability of the optogait portable photoelectric cell system for the quantification of spatial-temporal parameters of gait in young adults. Gait Posture 2016, 50, 196–200. [Google Scholar] [CrossRef]
- Whittle, M. Gait Analysis an Introduction, 4th ed.; Butterworth-Heinemann Elsevir: Philadelphia, PA, USA, 2007; pp. 54–57. [Google Scholar]
- Carlson, N.B.; Kurtz, D. Clinical Procedures for Ocular Examination, 3rd ed.; McGraw-Hill: New York, NY, USA, 2004; pp. 104–105. [Google Scholar]
- Daher, N.; Lee, S.; Yang, Y.J. Effects of elastic band orthosis (aider) on balance and gait in chronic stroke patients. J. Phys. Ther. Rehabil. Sci. 2013, 2, 81–86. [Google Scholar] [CrossRef]
- Beulertz, J.; Bloch, W.; Prokop, A.; Rustler, V.; Fizen, C.; Herich, L.; Streckmann, F.; Baumann, F.T. Limitations in ankle dorsiflexion range of motion, gait and walking efficiency in childhood cancer survivors. Cancer Nurs. 2016, 39, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.M.; Song, C.H.; Lee, K.J.; Jung, S.W.; Shin, D.C.; Shin, S.H. Concurrent validity and test-retest reliability of the OPTOGait phoelectric cell system for the assessment of spatio-temporal parameters of the gait of young adults. J. Phys. Ther. Sci. 2014, 26, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Gaerlan, M.G.; Alpert, P.T.; Cross, C.; Louis, M.; Kowalski, S. Postural balance in young adults: The role of visual, vestibular and somatosensory systems. J. Am. Acad. Nurse Pract. 2012, 24, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Callisaya, M.L.; Blizzard, L.; Schmidt, M.D.; McGinley, J.L.; Srikanth, V.K. Sex modifies the relationship between age and gait: A population-based study of older adults. J. Gerontol. 2008, 63, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Judge, J.O.; Davis, R.B.; Õunpuu, S. Step length reductions in advanced age: The role of ankle and hip kinetics. J. Gerontol. 1996, 51, 303–312. [Google Scholar] [CrossRef]
- Dingwell, J.B.; Marin, L.C. Kinematic variability and local dynamic stability of upper body motions when walking at different speeds. J. Biomech. 2006, 39, 444–452. [Google Scholar] [CrossRef]
- Hak, L.; Houdijk, H.; Steenbrink, F.; Mert, A.; van der Wurff, P.; Beek, P.J.; van Dieën, J.H. Stepping strategies for regulating gait adaptability and stability. J. Biomech. 2013, 46, 905–911. [Google Scholar] [CrossRef]
- Patla, A.E.; Davies, T.C.; Niechwiej, E. Obstacle avoidance during locomotion using haptic information in normally sighted humans. Exp. Brain. Res. 2004, 155, 173–185. [Google Scholar] [CrossRef]
- Wood, J.M.; Lacherez, P.F.; Black, A.A.; Cole, M.H.; Boon, M.Y.; Kerr, G.K. Postural stability and gait among older adults with age-related maculopathy. Investig. Ophthalmol. Vis. Sci. 2009, 50, 482–487. [Google Scholar] [CrossRef]
- Marigold, D.S.; Patla, A.E. Visual information from the lower visual field is important for walking across multi-surface terrain. Exp. Brain. Res. 2008, 188, 23–31. [Google Scholar] [CrossRef]
- Choi, J.H.; Moon, B.Y.; Yu, D.S.; Cho, H.G.; Kim, S.Y. Effects of induced refractive errors on gait patterns. J. Korean Opthalmic. Opt. Soc. 2018, 23, 259–264. [Google Scholar] [CrossRef]
- Brach, J.S.; Berlin, J.E.; VanSwearingen, J.M.; Newman, A.B.; Studenski, S.A. Too much or too little step width variability is associated with a fall history in older persons who walk at or near normal gait speed. J. Neuroeng. Rehabil. 2005, 2, 21. [Google Scholar] [CrossRef]
- Lee, D.N.; Eric, A. Visual proprioceptive control of standing in human infants. Percept. Psychophys. 1974, 15, 529–532. [Google Scholar] [CrossRef]
- Lee, D.N.; Lishman, J.R. Visual proprioceptive control of stance. J. Hum. Mov. Stud. 1975, 1, 87–95. [Google Scholar]
- Yu, D.S.; Kim, S.Y. Changes in postural control ability after wearing corrective glasses for distance in older adults and their causes. Int. J. Environ. Res. Public Health. 2022, 19, 6643. [Google Scholar] [CrossRef] [PubMed]
- Patla, A.E. Understanding the roles of vision in the control of human locomotion. Gait Posture 1997, 5, 54–69. [Google Scholar] [CrossRef]
- Mochon, S.; McMahon, T.A. Ballistic walking. J. Biomech. 1980, 13, 49–57. [Google Scholar] [CrossRef]
- Robert, R. Clinical prediction of falls in the elderly. Am. J. Phys. Med. Rehabil. 1997, 5, 54–69. [Google Scholar]
- Jack, C.I.A.; Smith, T.; Neoh, C.; Lye, M.; McGalliard, J.N. Prevalence of low vision in elderly patients admitted to an acute geriatric unit in Liverpool: Elderly people who fall are more likely to have low vision. Gerontology 1995, 41, 280–285. [Google Scholar] [CrossRef]
- Kannus, P.P.; Sieväneu, H.; Palvanen, M.; Järvien, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef]
Figure 1.
Factors affecting gait patterns used in this study.

Figure 2.
Analysis of correlation between change in step length and each gait pattern after wearing correction glasses; (a) Change in step length vs. change in stride length; (b) Change in step length vs. change in cadence; (c) Change in step length vs. change in step width; (d) Change in step length vs. change in walking velocity; * p < 0.05, ** p < 0.001: significantly difference according to Pearson’s correlation coefficient analysis n = 30 for each analysis.
Figure 2.
Analysis of correlation between change in step length and each gait pattern after wearing correction glasses; (a) Change in step length vs. change in stride length; (b) Change in step length vs. change in cadence; (c) Change in step length vs. change in step width; (d) Change in step length vs. change in walking velocity; * p < 0.05, ** p < 0.001: significantly difference according to Pearson’s correlation coefficient analysis n = 30 for each analysis.

{kind=link}
{kind=link}
Table 1.
Change in gait patterns before and after the participants wore correction glasses.
| Condition of Refractive Correction | Factors Affecting Gait Patterns | n | ||||
|---|---|---|---|---|---|---|
| Step Length (cm) | Stride Length (cm) | Cadence (Steps/min) | Step Width (cm) | Walking Velocity (m/s) | ||
| Before | 45.57 ± 5.37 | 89.09 ± 10.41 | 108.16 ± 12.59 | 10.21 ± 2.07 | 0.84 ± 0.16 | each 30 |
| After | 47.78 ± 5.81 | 94.09 ± 12.57 | 102.67 ± 19.74 | 10.93 ± 1.68 | 0.84 ± 0.17 | |
| t/p-value | −2.363/0.025 * | −2.43/0.022 * | 2.467/0.020 * | −3.410/0.002 * | 0.070/0.945 | |
| cogen’s d (effect size) | 0.395 | 0.433 | 0.332 | 0.203 | - | |
Data are expressed as mean ± SD. * p < 0.05: a significant difference according to the paired t-test.
Table 2.
Analysis of correlation between the factors of visual measurements and each gait pattern.
| Visual Measurement Factors | Gait Patterns | ||||
|---|---|---|---|---|---|
| Step Length (cm) | Stride Length (cm) | Cadence (Steps/min) | Step Width (cm) | Walking Velocity (m/s) | |
| Spherical equivalent power | r = −0.047/p = 0807 | r = −0.121/p = 0.524 | r = −0.011/p = 0.953 | r = −0.176/p = 0.351 | r = −0.095/p = 0.618 |
| Astigmatic diopter power | r = 0.193/p = 0.307 | r = 0.257/p = 0.171 | r = −0.134/p = 0.480 | r = 0.146/p = 0.442 | r = 0.228/p = 0226 |
| Improvement of visual acuity lines | r = 0.027/p = 0.887 | r = 0.056/p = 0.770 | r = −0.053/p = 0.780 | r = −0.082/p = 0.668 | r = −0.151/p = 0.427 |
Data are expressed as mean ± SD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Noh, J.-H.; Cho, H.-G.; Moon, B.-Y.; Yu, D.-S.; Kim, S.-Y. Changes of Gait Patterns after Correction of Refractive Error in the Elderly with Cataracts. Appl. Sci. 2023, 13, 6140. https://doi.org/10.3390/app13106140
AMA Style
Noh J-H, Cho H-G, Moon B-Y, Yu D-S, Kim S-Y. Changes of Gait Patterns after Correction of Refractive Error in the Elderly with Cataracts. Applied Sciences. 2023; 13(10):6140. https://doi.org/10.3390/app13106140
Chicago/Turabian StyleNoh, Jae-Hyeon, Hyun-Gug Cho, Byeong-Yeon Moon, Dong-Sik Yu, and Sang-Yeob Kim. 2023. "Changes of Gait Patterns after Correction of Refractive Error in the Elderly with Cataracts" Applied Sciences 13, no. 10: 6140. https://doi.org/10.3390/app13106140
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.