
Antibacterial Agents Used in Modifications of Dental Resin Composites: A Systematic Review


Department of General Dentistry, Medical University of Lodz, 251 Pomorska Str., 92-213 Lodz, Poland
*
Author to whom correspondence should be addressed.
Appl. Sci. 2024, 14(9), 3710; https://doi.org/10.3390/app14093710
Submission received: 10 March 2024
/
Revised: 23 April 2024
/
Accepted: 23 April 2024
/
Published: 26 April 2024
(This article belongs to the Special Issue Dental Materials: Latest Advances and Prospects, Third Edition)
Abstract
:Introduction: Resin-based composites (RBCs) are very common and often applicable in dentistry. Their disadvantage is susceptibility to secondary caries due to the formation of bacterial biofilm at the interface with the patient’s tissues. Antimicrobial additive incorporation into RBCs seems to be a justified method to alleviate the above-mentioned negative phenomenon. The aim of this review is to provide a juxtaposition of strategies and results on the topic of antimicrobial composites. It also provides insights into future research and prospects for clinical applications. Methods: This review summarizes the literature from 2017 to 2024, describing potential antimicrobial agents incorporated into dental composites. The research methodology involved a systematic search using the Population/Intervention/Comparison/Outcome (PICO) structure and selecting articles from databases such as Pubmed, ScienceDirect, and Elsevier, which allowed for an in-depth review of substances utilized for the antibacterial modification of RBCs. Results: A total of 159 articles were identified, 43 of which met the inclusion criteria. Conclusions: This review is a summary of novel approaches in the field of dental materials science. The results show the variety of approaches to modifying composites for antimicrobial efficacy. It is worth underlining that there is a significant difficulty in comparing the studies selected for this review. This is related to the different modifiers used and the modification of composites with different compositions. Unfortunately, there is still a lack of a standardized approach to the modification of dental materials to give them a biocidal character and simultaneously maintain the stability of their mechanical and chemical properties.
1. Introduction
Resin-based composites (RBCs) are some of the most popular materials in current dentistry. They are used to manufacture various types of proto-restorations, such as inlays, onlays, bridges, and direct restorations. Despite RBCs having many advantages, they also have disadvantages. The most common reason for replacing restorations made of resin-based composites is the development of secondary caries. In the oral cavity, one can find bacteria such as Firmicutes, Bacillus, Proteobacteria, and Actinomycetes. The most common pathogens found in the oral environment are Streptococcus mutans, Porphyromonas gingivalis, Staphylococcus, and Lactobacillus [1]. Streptococcus bacteria in combination with the oral fungus Candida produce a biofilm that can lead to many oral diseases. Bacteria such as Streptococcus mutans, Streptococcus sanguis, Lactobacillus, and Actinomyces viscocus have been reported to be the most common contributors to the formation of secondary caries [1,2,3,4].
During the polymerization reaction of RBCs, a gap at the interface between the composite and the patient’s tissues occurs [5]. The resulting gap is an ideal place for developing bacterial biofilm, which, in the long run, may lead to chemical and mechanical degradation of the restoration. The above phenomenon is unfavorable for the patient and exposes them to unnecessary loss of their tissues during the placement of new restorations, as well as generating further costs.
In recent years, numerous studies have been conducted with the common purpose of developing RBCs that could eliminate secondary caries. Researchers have attempted to modify matrices or fillers using various substances with potential antibacterial effects [6,7].
The review summarizes the antibacterial agents added to dental composite materials, commercial and experimental. It includes articles published from January 2017 to February 2024 accessible via the Science Direct, PubMed, and Elsevier databases. The introduction of potentially antibacterial agents can improve oral health and raise patients’ standard of living. Composite materials with antibacterial properties can prevent the occurrence of complications, consequent on which is the preservation of a healthy smile and lower healthcare costs for patients.
A composite material is composed mainly of organic, inorganic, and binding phases. The matrix, otherwise known as the organic phase, is made from a mixture of monomers (usually dimethacrylates) which are enriched with such components as polymerization initiators, inhibitors, and stabilization agents. The matrix allows the transfer of stresses to the reinforcing material; more than that, it keeps the inorganic particles in the right form, which allows the material to maintain its shape. The organic phase defines the chemical and thermal properties of an RBC [8,9]. The organic phase is reinforced with inorganic phase-particles, usually based on silicon or zirconium (with a micro/nano size). The above phases are bonded together by a chemical reaction through the bonding phase (silanes) [10,11]. In recent years, new “bulk-fill”-type composites have been developed. These materials are used to reduce the time consumed in the application of incremental layers while at the same time providing adequate strength properties and high aesthetics for the prosthetic reconstructions created. To achieve these properties, more reactive photoinitiators and chemically modified monomers are introduced into the formulations [12].
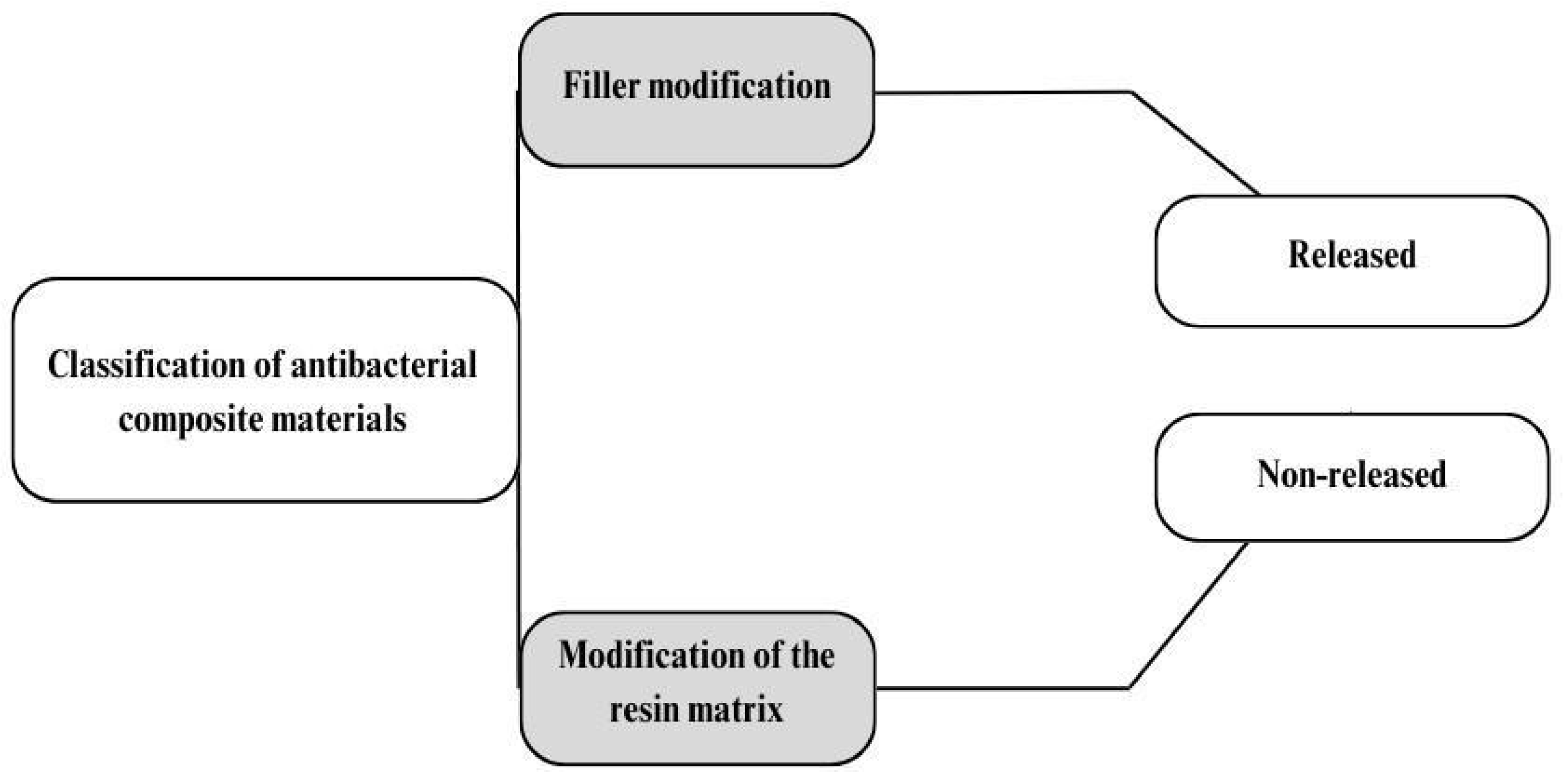
Antimicrobial modifications of composite materials can be based on modification of the resin matrix or the filler. Depending on the method chosen, agents can be released or non-released [11] (Figure 1).
The diffusion of a released antibacterial substance will be difficult to control, both in terms of release time and concentration. Released substances may irritate surrounding tissues; moreover, during diffusion, the structure of the material will be altered, and, consequently, the mechanical properties of the material may change. In the case of non-releasable modifiers, there is no change in the mechanical or physical properties of the material. The modifier’s action will be less intense than that of a release modification due to the immobilization of the modifier. However, the effect will be prolonged [6,13,14]. In addition, a division can be made in terms of whether the modifier will participate in polymerization or just be an additive to the material [15].
2. Methods
2.1. Research Strategy
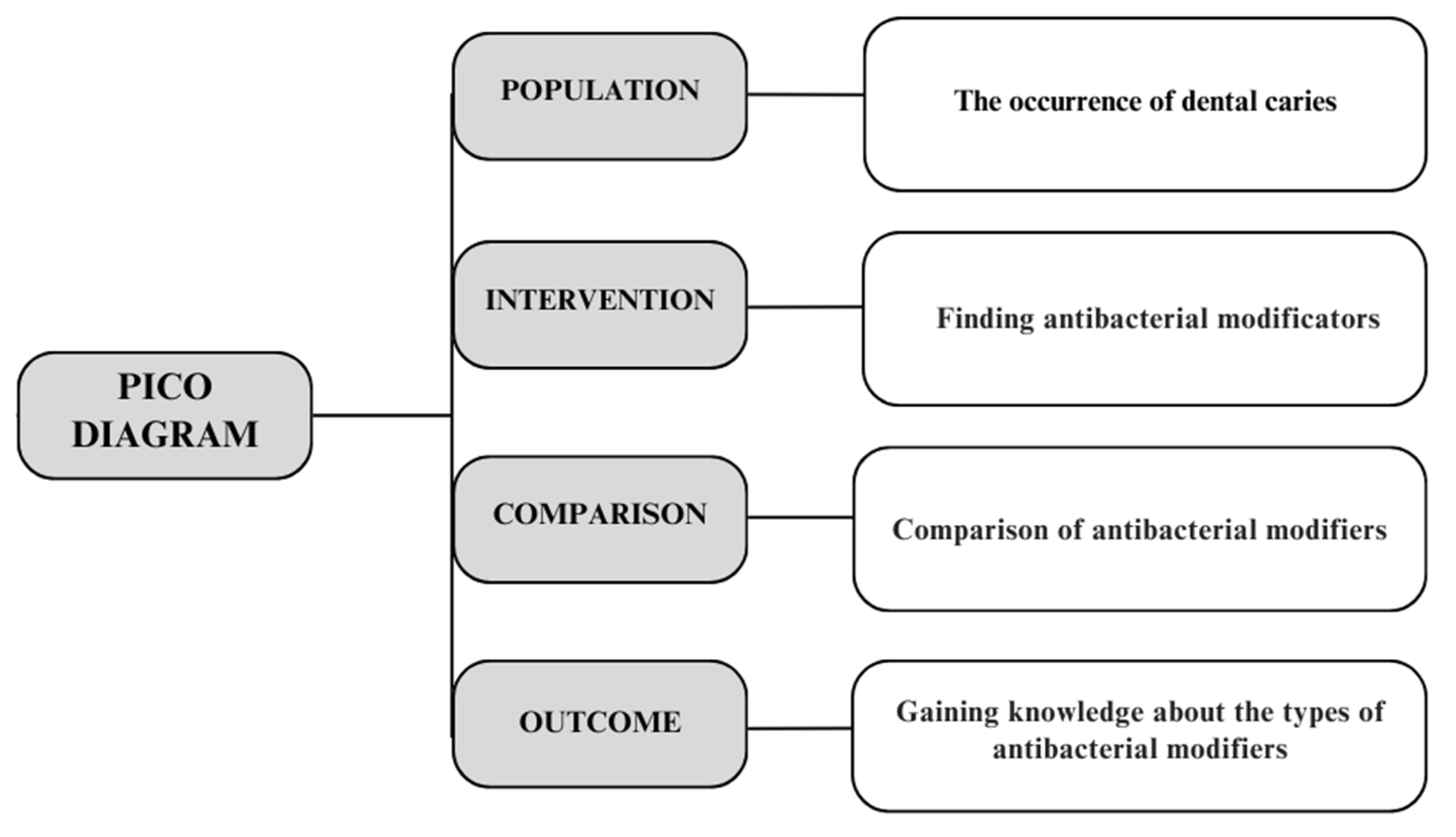
The Population/Intervention/Comparison/Outcome (PICO) framework [16] was used to establish a literature search plan (Figure 2).
A search of the peer-reviewed literature (considering titles and abstracts) was conducted using databases such as Science Direct, PubMed, Elsevier, and Google Scholar. The following were used as inclusion criteria:
- −
- The keyword combinations used were as follows: “dental AND materials AND antibacterial modifier” OR “dental AND materials AND antibacterial agent” OR “antibacterial polymer” OR “antibacterial dental resin” OR “resin composites AND antibacterial modification AND antibacterial agent” OR “antimicrobial monomers AND dental resin composite” OR “dental AND composite AND antibacterial” OR “dental AND composite AND antibacterial AND properties”.
- −
- Only English-language publications were analyzed.
- −
- Publications published between 2017 and 2024.
The literature search was performed until February 2024. The article titles and abstracts that met the above criteria were evaluated for relevance to this review. Articles not directly related to antibacterial modifiers for dental materials were excluded.
2.2. Article Selection
Publication abstracts retrieved using search engines were selected using inclusion and exclusion criteria by the first reviewer (MZ). Duplicate articles were removed manually. With the second reviewer’s (KB) participation, we discussed any discrepancies in the evaluation. In the next step, the reviewers (MZ and KB) evaluated the full articles and the literature references contained in them, which made it possible, through a manual search, to find more articles related to the field of the review. All publications that met the inclusion criteria were downloaded electronically and analyzed (Table 1).
3. Results
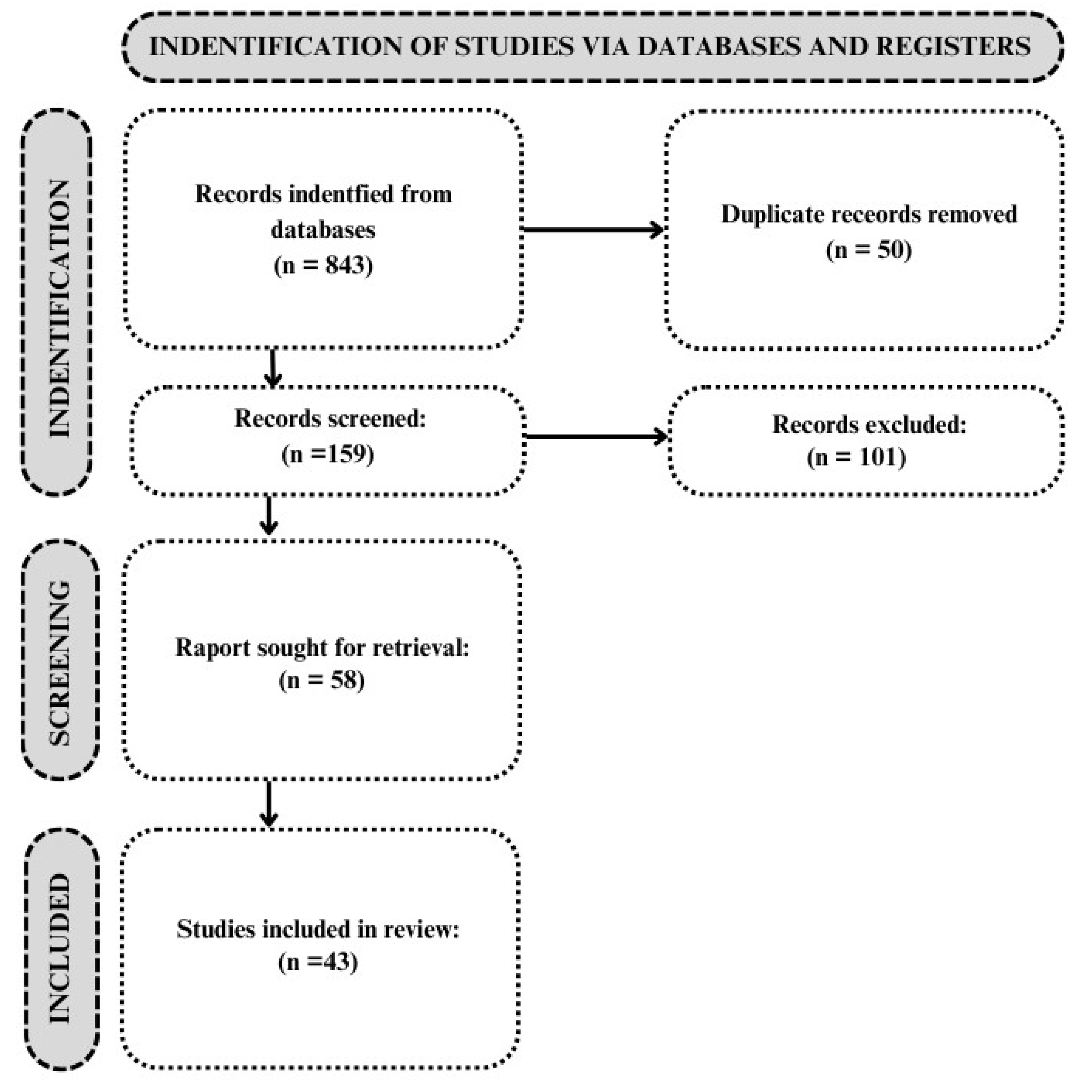
With the use of databases, 159 articles were identified. A total of 101 studies were excluded based on the exclusion criteria. Then, 43 articles were selected from the remaining 58 articles based on the inclusion and exclusion criteria shown in Table 1. The PRISMA study selection process is shown in the diagram below [17] (Figure 3, Table S1). All relevant articles are summarized in Table 2.
4. Discussion
In the review, it was found that there is a large number of different antibacterial substances. The general characteristics of the study are described above.
4.1. Modification with Released Agents
Released antimicrobial agents (Figure 4) are substances incorporated into composite materials that are released over time into the oral cavity. One such substance is triclosan (TCN), which is used, for instance, in the production of toothpastes and mouthwashes. It is characterized by antibacterial properties against Staphylococcus aureus, Streptococcus mutans, Lactobacillus species, and Actinomyces. Cuncha et al. [18] decided to mixed triclosan-encapsulated halloysite nanotubes (HNT/TCNs) with RBCs. Their study showed no changes in the antibacterial properties of the modified composites over 5 days and some improvements in their mechanical properties and an increase in polymerization stress. But, as stated by the authors, the antimicrobial test methods may not be fully suitable for comprehensively evaluating composites, and it is worthwhile for them to be accompanied by aging protocols.
Wang et al. [19] attempted to obtain antimicrobial properties by incorporating a deeply eutectic solvent (DES) derived from the antimicrobial agent benzalkonium chloride (BC) mixed with acrylic acid (AA). The composite containing DES (DES-C) exhibited superior flexural strength and biocompatibility compared to a similar composite incorporating BC (BC-C) at equivalent BC levels. Although both BC-containing composites demonstrated antibacterial activity, BC-C produced larger inhibition zones than DES-C at equivalent BC concentrations (against Streptococcus mutans and Staphylococcus aureus). Control composites without BC showed minimal antibacterial activity. Following artificial aging, DES-C maintained mechanical properties better than BC-C compared to the control, albeit with a slight decrease observed during the three-point bending test, especially under elevated-temperature storage conditions.
Chlorhexidine is a commonly used antiseptic that acts against Gram-negative and Gram-positive bacteria, parts of viruses, molds, and yeast. It is used in oral fluids to reduce post-operative infections and inflammation of the gums [20]. Additionally, chlorhexidine can also be used as an antimicrobial modifier for polymethylmethacrylate (PMMA) [61,62]. Montmorillonite clay (MMT) is used as a carrier for drugs or macromolecules, such as DNA, proteins, and nucleotides [63].
Boaro et al. [20] used MMT enriched with chlorhexidine (CHX/MMT) to modify RBCs. CHX/MMT, in addition to having antibacterial properties, can reinforce the structure of composites. In their study, the antimicrobial activity of experimental composite materials against Porphyromonas gingivalis was tested. They showed that materials enriched with 5 wt% of MMT and 10 wt% chlorhexidine (Figure 5) achieved the best inhibitory properties. The modification with CHX/MMT did not adversely affect elastic modulus or flexural strength values or the degree of conversion of the composites.
Another idea for achieving antibacterial properties was conceived by Cao et al. [21]. They decided to use a composite enriched with a light-cured AgBr core–shell/cationic polymer nanocomposite (AgBr/BHPVP). The Ag+ released from the material acts against Streptococcus mutans. Such a material seems promising and capable of reducing the appearance of secondary caries. Evaluation of its cytotoxicity, however, showed that materials modified with less than 1 wt% of AgBr/BHPVP obtained results similar to the control. The study also showed that the modification increased the hardness of the material and did not negatively affect its elastic modulus or flexural strength. Nevertheless, it needs to be evaluated whether this substance would have similar effectiveness in filled materials.
Altaie et al. [64] used fluorapatite (FA) crystals as a secondary filler. The crystals were introduced into material at 10, 20, 30, and 40% by weight. The filler content was kept at 80% by weight (63–67% by volume). Tests were conducted in neutral and acidic buffers. The modified composites achieved lower elastic modulus and flexural strength values. The hardness after modification was comparable to the values of the control test. The fracture toughness was influenced by the FA amount. Fluoride release was found to increase with the amount of modificator used.
Zhou et al. [22] indicated that a TiO2/thyme-containing composite showed significant growth inhibition zones against Streptococcus mutans, Lactobacillus acidophilus, and Candida albicans compared to the oil-free control. Thyme oil was found to be released over 15 days, using concentrations of 1–2 wt% TiO2/thyme, while maintaining antibacterial properties (reduction of 68–99% of pathogens). Dental pulp stem cell viability exceeded 90% for all resin formulations, indicating excellent cytocompatibility. Incorporation of thyme/TiO2 up to 2 wt% in the composite did not affect the flexural strength, elastic modulus, or surface microhardness values. For thyme/TiO2 concentrations of 0.5–2 wt%, Zhou et al. showed that the microtensile bond strengths between resin and dentin ranged from 45 to 50 MPa, indicating no substantial difference from the control [22].
Although the above-described modifications of composites led to positive results in terms of biocidal properties, these studies should be continued. Since there is a risk that composites will change their morphology during the release of biocidal substances, which may result in a change in physicochemical properties, it seems reasonable to examine the long-term behavior of such composites. Studies on changes in properties like hardness, strength, modulus, water sorption, and biotolerance over time (or after artificial aging protocols) should be performed. With such analyses, more in-depth evaluation of the proposed modifications would be possible.
4.2. Modification of RBC Compositions
4.2.1. Organic Compounds and Monomers
Antimicrobial modification of resin monomers allows for a sustained bactericidal effect due to the integration of the agent into the matrix during polymerization. This action will be independent of the filler release process. The action may not be as strong, but it will be long-lasting. Among the most common matrix modifiers are quaternary ammonium compounds (QACs). They disrupt the electrical balance of bacterial cells. One consequence of electrical imbalance is disruption to the bacterial cell wall, resulting in the outflow of cytoplasmic components and, ultimately, bacterial death [14,15,23].
Zalega et al. made experimental RBCs with potentially antibacterial agents—hexadecyltrimethylammonium bromide (CTAB) and dimethyldioctadecylammonium bromide (DODAB). They then studied the effects of these agents on the mechanical properties of the experimental material. It consisted of a mixture of bis-GMA/UDMA/HEMA/TEGDMA monomers filled with silanized silica (45 wt%). It was shown that the type and amount of modifier affected the flexural strength, hardness, and shrinkage stress. However, the modification did not affect the diametral tensile strength of the experimental composites [65].
Among the most commonly used antibacterial agents are quaternary ammonium (QA) monomers of methacrylate. These agents tend to degrade in the oral environment due to their structure (they contain ester bonds). The use of monomers free of ester bonds may be a way to overcome this problem [23].
Fugolin et al. [23] used QA monomers based on methacrylamides. Tertiary quaternary ammonium acrylamides (AMs) and methacrylamides (MAMs) with 9- and 14-carbon alkyl side chains were used in the study. The substances were then incorporated into experimental composites, which were based on bisphenol A-glycidyl methacrylate (bis-GMA) and triethyleneglycol di-methacrylate (TEGDMA). The study showed that all versions of the composites containing 14 carbons per chain showed strong antibacterial properties, resulting in a twofold reduction in biofilm titers. Evaluation of cytotoxicity showed no significant differences between the control sample and the MAM and AM modifications, which may suggest good biocompatibility of the material with patient tissues. The degree of conversion showed similar levels for all groups tested. Composites modified with MAM and AM with alkyl side chain lengths of 14 carbons showed lower polymerization rates. Flexural strength and modulus values were similar for all groups under dry conditions. But issues related to wet mechanical properties still need to be addressed.
Fanfoni et al. [24] synthesized and structurally characterized nine new antibacterial di-methacrylate monomers derived from bis-quaternary ammonium salts (bis-QAMs). In most cases, a complete bactericidal effect was achieved with bis-QAM concentrations below 1 mg/mL. Notably, two of these structures demonstrated comparable or superior activity against Streptococcus mutans compared to MDBP. Moreover, all modified bis-QAMs successfully inhibited Streptococcus mutans biofilm formation at concentrations equal to their MIC values. The monomers used demonstrated low cytotoxicity on human dental pulp stem cells. Cytotoxicity studies should be expanded and long-term effects on tissues should be investigated to ensure high biocompatibility. Also, this study was only focused on resin formulations; hence, the properties and biocidal activity of composites prepared with bis-QAMs must be evaluated.
Cherchali et al. [25] prepared a dental composite with methacrylate-based monomers enriched with quaternary ammonium dimethyl-hexadecyl-methacryloxyethyl-ammonium iodide (DHMAI; Figure 6) and methacryloyl ethoxylphosphorylcholine (MPC). The study showed that using 7.5% DHMAI improved the conversion rate of the composite and provided a strong antibacterial effect with a reduction in CFUs (colony-forming units) and metabolic activity while maintaining acceptable mechanical properties. Still, the long-time antibacterial activity, durability, and cytotoxicity of this composite should be analyzed.
Huang et al. [26] investigated the properties of an experimental composite resin containing the quaternary ammonium compound urethane-dimethacrylate (UDMQA-12). The modified antibacterial resin composite demonstrated biocompatibility and mechanical properties (flexural strength and modulus) comparable to those of the conventional composites used as controls. The antimicrobial activity of the modified material against Streptococcus mutans was demonstrated, and cytotoxicity tests showed the material’s biocompatibility. It would be useful to perform long-term cytotoxicity and mechanical strength tests to verify the safety and reliability of the material.
He et al. [27] synthesized three diquaternary ammonium methacrylates that differed in alkyl chain length (biQAMA-12, biQAMA-14, and biQAMA-16). They concluded that the most optimal alkyl chain length was a 12-carbon chain. This dental composite material had the best antibacterial properties against Streptococcus mutans due to its having the highest antibacterial charge density. Additionally, mechanical tests showed that modification of 5 wt% biQAMAs did not change the properties of the experimental material. Unfortunately, both biQAMA-14 and biQAMA-16 increased the cytotoxicity of the prepared composites. Also, the modification affected water sorption—its value increased but was still within the ISO standard. The increase in water sorption, although within the ISO standard, can vary over time. Long-term studies should be carried out to investigate whether the strength of the material changes over time. Strategies may need to be found to limit the increase in water sorption.
One monomer that may find use in the production of an antibacterial composite is the quaternary urethane-dimethacrylate ammonium derivative QAUDMA-m (where m corresponds to the number of carbon atoms in the N-alkyl substituent, this being 8, 10, 12, 14, 16, and 18 in the studies considered). Chrószcz-Porębska et al. [28,29] conducted a study showing that resin matrices containing QAUDMA-m 8/10/12 compositions were most effective against Staphylococcus aureus and Escherichia coli. The occurrence of lower water sorption, hardness, and solubility in water was related to the elongation of the N-alkyl chain. As the N-alkyl chain lengthened from 8 to 10 carbon atoms, the elastic modulus and flexural strength increased. Furthermore, the copolymers exhibited high biocidal activity during pilot studies. Nevertheless, it is necessary to determine whether such biocidal activity will last in composites (after filling) and to investigate the long-term safety in conjunction with water sorption, the stability of the mechanical properties, and the cytotoxicity.
Dimethylaminododecyl methacrylate (DMADDM) can be used as a promising, effective antibacterial modifier. Alhussein et al. [30] used DMADDM at different concentrations (0%, 1.5%, 3%, and 5 wt%). The study showed that using 3 wt% of DMADDM did not affect the composite. DMADDM appeared to have the best antimicrobial properties against Streptococcus mutans. Chen et al. [31] also incorporated DMADDM into commercial giomer (Beautifil II F03 A2, SHOFU Inc., Kioto, Japan) and applied it against Helicobacter pylori. In vitro trials revealed that the minimum inhibitory concentration (MIC) and the minimum bactericidal concentration (MBC) of DMADDM were 6.25 μg/mL and 25 μg/mL, respectively. DMADDM–modified materials effectively reduced Helicobacter pylori biofilm formation in reconstructions. The antibacterial activity of DMADDM appears promising, but cytotoxicity and long-term behavior studies need to be carried out to ensure safe use.
Another monomer used in dentistry is methacryloyloxydodecylpyridinium bromide (MDPB; Figure 7). MDPB allows the preparation of composites with antibacterial properties [66,67].
Saiprasert et al. [32] decided to investigate the use of MDPB and different methacrylamide–based QACs as antimicrobial agents in a resin formulation. Such modifications significantly reduced the activity of Streptococcus mutans and Enterococcus faecalis. Worth further study is the monomer 1-(11-Methacryla-midoundecyl) pyridine-1-ium bromide (MAUPB). Studies on the properties of composites enriched with these monomers should be continued.
Because of MDPB’s color fickleness, Bienek et al. proposed another alternative, ionic dimethacrylates (IDMAs), which also exhibit antibacterial properties [68]. In the cited research, IDMA1 (2-(methacryloxy)-N-(2-(methacryloxy)ethyl)-N,N-dimethylethane-1-amine bromide) and IDMA2 (N,N′-([1,1′-biphenyl]-2,2′-diylbis (methylene)) bis(2-methacryloyloxy)-N,N-dimethylethan-1-aminium) bromide) were synthesized. The study showed that using IDMA increased the conversion rate of the material used without affecting its wettability. Material prepared with IDMA showed little or no toxicity to cells. The addition of IDMA as a comonomer reduces the flexural strength and modulus of elasticity of polymers. Only neat materials were evaluated in the study; no information about filled resin properties was provided.
Silva et al. [33] introduced myristyltrimethylammonium bromide (MYTAB) to composites at concentrations of 0.5, 1, and 2 wt%. Antimicrobial activity against Streptococcus mutans was tested by two in vitro evaluations—against planktonic bacteria and biofilm formation—on cured material samples. The study showed that the composite material enriched with 2 wt% significantly reduced the abundance of Streptococcus mutans in the planktonic and biofilm stages compared to the control sample and had no effect on the material’s tensile strength or its conversion factor. Cytotoxicity was found to increase with increasing MYTAB concentration. The increase in cytotoxicity with increasing concentrations of the MYTAB modifier raises concerns about the safety of the experimental composite material. Further research is needed to resolve the cytotoxicity issue.
Due to the use of quaternary ammonium compounds, an analysis of cytotoxicity should be performed. The long-term biocidal efficiency, the stability of the mechanical properties, and the water sorption of materials modified with this type of substance should be examined as well.
Garcia et al. [34] studied the addition of resins containing 2.5 or 5 wt% of the monomer 1,3,5-triacryloylhexahydro-1,3,5-triazine methacrylate (TAT). There were no discernible differences noted in terms of the degree of conversion; the incorporation of TAT at a 5 wt% led to increased Knoop hardness, enhanced resistance to solvent softening, and higher ultimate tensile strength. Elevated concentrations of TAT correlated with heightened antibacterial activity. It was found that the application of TAT modification at 2.5% w/w showed no cytotoxicity compared with the control sample. In contrast, a 5% w/w TAT concentration resulted in reduced cell viability. Similarly to an earlier study, only resin formulations were evaluated. Other studies on the use of TAT in composites are necessary and should include long-term durability and cytotoxicity evaluations.
Another option for reducing Streptococcus mutans bacteria is the use of composite materials enriched with methacrylated chitosan (CH–MA). Stenhagen et al. have shown that the use of CH–MA modifications reduces biofilm formation. However, it should be noted that the higher the amount of CH-MA, the lower the flexural strength and hardness of the composite [35].
Burujeny et al. [36] used Triazolium/POSS, which serves as an effective bactericidal additive to composites based on a ternary formulation of thiol-allyl ether and methacrylate. The results of the study showed that, despite a partial increase in the water absorption of the sample containing Triazolium/POSS, this parameter was more favorable compared to that of a composite made with DMAEMA-BC. The inclusion of Triazolum/POSS did not significantly affect the shrinkage strain and cytocompatibility of the composite sample. However, a decrease in some mechanical properties was observed.
A different method to obtain antimicrobial properties involves the use of a fluorinated monomer—fluorinated dimethacrylate (FDMA) or fluorinated diluent methacrylate (FBMA). He et al. [37] found that modifications with these substances showed a higher degree of conversion (DC) compared to a Bis-GMA-based resin. The FDMA/FBMA resin system showed a lower flexural strength and elastic modulus, in contrast to the material with the FDMA/TEGDMA system. Both systems showed reduced water sorption and solubility compared to control samples. It was found that the FDMA/FBMA resin system showed lower free energy. With a smooth surface, the FDMA/FBMA resin system exhibited reduced adhesion to Streptococcus mutans compared to the control sample; with a rough surface, the FDMA/FBMA system showed adherence to Streptococcus mutans comparable to that of the control [37]. It would also be worthwhile to conduct cytotoxicity studies and estimate the mechanical properties of filled matrices before and after aging.
4.2.2. Other Additives
Zajdowicz et al. [38] proposed CuAAC-based composites made from different azide monomers and different copper concentrations. They formed biofilms from Streptococcus mutans strains expressing luciferase. It was shown that the number of viable bacteria was reduced for biofilms grown on CuAAC-based composites compared to the control sample. No information about the strength and cytotoxicity of the modified materials was provided.
Al-Dulaijan et al. [39] proposed a composite prepared with amorphous calcium phosphate nanoparticles (NACPs) with or without dimethylaminohexadecyl methacrylate (DMAHDM). The study showed that the flexural strength and modulus of the experimental composite enriched with NACP-DMAHDM were similar to those of the control sample. The addition of DMHDM to the rechargeable NACP composite did not adversely affect the release and loading of Ca and P ions, and the composite showed significantly less biofilm growth [39]. These promising results in terms of remineralization and biostatic properties should be studied further to assess their lastingness and efficiency. Bhadila et al. [40] also used DMAHDM or low-shrinkage-stress resin and NACP as potential composites with remineralizing and antimicrobial (against Streptococcus mutans) properties. As a control, a commercial composite (Heliomolar, Ivoclar) was used. The experimental monomers were found to have similar fibroblast viability to the commercial material used as a control. There was no negative effect of DMAHDM on the hydration of Ca and P ions. In addition, the flexural strength was similar to that of the control material, while the hardness of the control was twice as low as the values obtained for the experimental materials.
Commercial bulk-fill materials containing antimicrobial fillers (alkasite), such as barium aluminosilicate glass and ytterbium trifluoride, were characterized by antibacterial properties, but these properties were weaker than those presented by chlorhexidine [41].
Barot et al. [42] introduced a filler in the form of halloysite nanotubes loaded with chlorhexidine (HNT/CHXs; various mass fractions from 1 to 10% by weight). The experimental composite enriched with HNT/CHXs inhibited the growth of Streptococcus mutans. In addition, MTT tests showed that materials prepared with halloysite nanotubes loaded with chlorhexidine showed no cytotoxicity against NIH 3T3 fibroblast cells compared to the control sample. The results of the study may suggest a favorable safety profile, which in the long term may allow the material to be used clinically. Tests showed that the modification improved the elastic modulus, flexural strength, and compressive strength of the tested material [42]. The improvement in these properties is very promising, but it is important to evaluate the long-lasting durability and strength of the material. Core–shell chlorhexidine/amorphous calcium phosphate (CHX/ACP) nanoparticles were also successfully used to modify the resin composite. The best compromise between antimicrobial and mechanical properties was presented by the material prepared with 5 wt% CHX/ACPs [43]. Since this composite releases some ions, further studies on changes in its properties should be planned.
Tian et al. [44] used an inorganic antiseptic, magnesium oxide (nMgO), and a remineralizing agent, bioactive glass (BAG), to modify a composite resin. During the study, it was shown that the simultaneous introduction of nMgO and BAG into the composite material achieved very good antimicrobial properties against Streptococcus mutans, while the presence of BAG resulted in improved remineralization capacity with increasing substance concentration. The modification did not significantly affect hardness, flexural, or compressive strength, but the water sorption and curing depth increased with increasing amounts of nMgO and BAG. Increased water sorption can cause premature material degradation, affecting material performance. Further research is needed regarding the stability of the experimental composite.
Another invention proposed by Ai et al. [45] that can provide both structural reinforcement and antimicrobial activity is the use of a modified filler consisting of hydroxyapatite (HA) nanodrills coated with polydopamine (HA–PDAs). HA–PDAs were loaded afterwards with silver nanoparticles (AgNPs). The HA-PDA-AgNP nanodrutes were incorporated into a resin matrix. The prepared composite enhanced the strength of the material, while the silver ions released provided antibacterial activity. It was also found that modification with 6–8 wt% HA–PDA–Ag nanowires resulted in a significant increase in modulus and flexural strength. But it should be noted that this modification is appropriate for composites that are thermocured as opposed to photocured because of the color of PDA, which could negatively influence light transmission [45].
An effective modification of dental composites in terms of biocidal effect is the addition of chitosan or chitosan loaded with particles of anhydrous dibasic calcium phosphate (DCPA) [46]. It was found that the modified materials resulted in about 20% less biofilm (Streptococcus mutans) compared to the control. Additionally, the modification did not adversely affect the flexural strength, fracture strength, modulus of elasticity, or conversion rate compared to the control group after 90 days of aging in water.
Dias et al. [47] used TiO2 and TiO2/Ag nanoparticles for antibacterial modification. Their study showed that the introduction of 2 wt% TiO2/Ag nanoparticles reduced the accumulation of Streptococcus mutans biofilm on the surface of a dental composite. TiO2/Ag also had a positive effect on the mechanical properties of the material, increasing the compressive strength, while the conversion factor remained unchanged. The surface roughness was also investigated, and it was found that this parameter increased with increasing concentration of nanoparticles. Further research is needed, especially on the issue of cytotoxicity and long-lasting antibacterial activity and the stability of the mechanical properties. Chambers et al. [48], in their trials, showed that, in small amounts, Ag–TiO2 showed bactericidal activity under visible light contact with Streptococcus mutans. After incorporation into a composite, however, the photocatalytic properties of Ag–TiO2 particles were significantly reduced, but a strong bactericidal effect against Streptococcus mutans was still achieved. In this study, no physical/mechanical properties of the composites were evaluated.
Bioactive glass derived from Ag–doped sol–gel (Ag–BG) was used as another filler of dental composites [49]. The modifier was used at 5, 10, and 15 wt% concentrations, and bacterial mortality in the biofilm (produced by Streptococcus mutans) increased significantly as the concentration of Ag–BG in the composites increased. During the study, the microstructural properties and elemental composition of the developed Ag–BG composite were analyzed. Total strength tests showed that 3 months after immersion in the medium, there was no statistically significant change in the bond of the surrounding tooth tissue to the restorative material. The modification requires further research, and the strength properties of composites should be considered.
Arif et al. [50] used ciprofloxacin-loaded silver nanoparticles (CIP–AgNPs) to modify a composite. The use of the modified CIP–AgNPs was shown to achieve biocidal activity against Enterococcus faecalis, Streptococcus mutans, and saliva microcosms. During the test, it was shown that the compressive strength of the experimental material was higher than that of the control material. The researchers showed that the modified composite materials exhibited biocompatibility compared to composites containing AgNPs. No mechanical properties other than compressive strength were tested, and long-term mechanical testing is needed to determine the real strength over time and under varying environmental conditions.
Srivastava et al. [51] used commercial barium borosilicate-based glass powders, which are commonly used fillers in dentistry. However, the powders were covalently immobilized with silver sulfadiazine to allow them to provide antimicrobial activity. Modification of the glass powders resulted in strong antimicrobial activity against Streptococcus mutans. Composite materials based on bisGMA, with 2% to 10% glass powders with silver sulphadiazine, were shown to exhibit strong and sustained antibacterial efficacy against Streptococcus mutans. This modification did not adversely affect the mechanical properties of the prepared composites. Cytotoxicity tests should be performed and consider the overall effect of adding such fillers in terms of material longevity.
Dias et al. [52] used antimicrobial modification with 3D zinc oxide (ZnO) microstructures. The use of small amounts of ZnO microparticles reduced the growth of Streptococcus mutans bacteria on the surface of the material used. It was shown that the modification did not adversely affect the compression strength of the composite, nor did it affect the diametral tensile strength. Zinc oxide was also used for another antibacterial modification. Cellulose nanocrystal/zinc oxide (CNC/ZnO) nanohybrids were introduced into the experimental composite. Studies by Wang et al. showed that the use of a 2 wt% CNC/ZnO nanohybrid reduced the number of Streptococcus mutans bacteria by up to 78%. High concentrations of CNC/ZnO nanohybrids led to a reduction in compressive strength, flexural strength, and Vickers microhardness, but not flexural modulus [53].
Chen and others used core–mesoporous shell-structured ZnO@m-SiO2 to modify composites. It was found that the composite modified with Z7S63 (ZnO@m-SiO2:silanized SiO2 = 7:63 wt./wt., total filler content 70 wt%) showed the best compressive and flexural strength and modulus of elasticity. The experimental composite demonstrated remarkable antibacterial efficacy (>99.9%) [54].
Qin et al. [55] decided to enrich the composite material with potentially antibacterial silanized hydroxyapatite nanofibers loaded with erythromycin (s–HAFs@EM). The resin modified with 15% s–HAFs@EM exhibited the highest flexural strength and elastic modulus. Compared with pure resin, these values increased by 65.43% and 90.7%. The study showed that the resin containing 15–20% of the modifier showed a significant antimicrobial index (against Streptococcus mutans) compared to the control. In addition, it showed some remineralization capacity and good in vitro biosafety. The observed ability to remineralize is promising, but it is nevertheless necessary to study the long-lasting stability of the mechanical properties of these experimental materials.
Another way to avoid the development of caries is to use hydrated calcium silicate (hCS). Yang et al. [56] discovered that an experimental material containing hCS showed significantly stronger antimicrobial activity compared to the group without hCS filler. The addition of hCS to the studied composite resulted in higher water sorption, solubility, and release of Ca and Si ions. The phenomenon of increased water sorption can have a negative impact on mechanical properties, leading to material degradation; hence, studies on the long-lastingness of the properties in wet conditions are required. After immersion in artificial saliva solution (for 30, 60, and 90 days), it was noted that the composite material with 52.5 wt% hCS filler produced precipitates that consisted largely of Ca and P, which were detected as hydroxyapatite [56].
Go et al. [57] decided to use strontium-modified phosphate glass (Sr-PBG) as a matrix filler. The filler was incorporated at three concentrations—3, 6, and 9 wt%—into a commercial composite (Filtek Z350XT, 3M ESPE). The study showed that the Sr-PBG-enriched composite material inhibited the growth of Streptococcus mutans, and the release of remineralizing Ca and P ions increased with increasing Sr-PBG concentration in the material. The addition of this modifier was found to not affect the mechanical properties (microhardness, tensile strength, and elastic modulus) of the composite, even after thermocycling.
Zhang et al. [58] used a low-shrinkage resin consisting of a 20 wt% mixture of the anti-shrinkage expansive monomer 3,9-diethyl-3,9-dimethylol-1,5,7,11-tetraoxaspiro[5,5] undecane and the epoxy resin monomer bisphenol diallo. They also included diglycidyl ether and the addition of antimicrobial microcapsules—nanoparticle-modified MCs with a nano-antibacterial inorganic filler (NIF) containing a quaternary ammonium salt—at concentrations of 0, 2.5, 5, 7.5, 10 wt%. The microcapsules can self-regenerate. This dental resin’s mechanical properties, polymerization shrinkage, antimicrobial activity, self-healing ability, and cytotoxicity were investigated. No negative effect on mechanical properties was shown. It was found that the volumetric polymerization shrinkage of the composite containing 20 wt% EU and 7.5 wt% microcapsule resin was reduced by 30.12% compared to the control group. Good self-healing performance and high antimicrobial activity were also demonstrated. Still, studies of the filled composites in simulated oral environments are needed.
Adeeb et al. [59] used silver sodium zirconium hydrogen phosphate as a matrix filler. They determined the efficacy against Enterococcus faecalis. The study showed that bacterial colonies of the Enterococcus faecalis strain were reduced. A similar phenomenon of bacterial colony reduction was achieved at concentrations ranging from 7% to 13%, and it was also found that at a concentration of 1% and in the control group, the number of colonies increased [59]. Despite the promising antimicrobial properties, further studies, such as durability tests and cytotoxicity tests, are needed. Analysis is necessary to reliably assess the clinical suitability of the material.
Lapinska et al. modified a composite resin restorative material (SDR flow, Dentsply Sirona, Charlotte, NC, USA) with essential oils. These composites were evaluated only for antimicrobial and antifungal activity. It was shown that thyme and cinnamon oils showed the best antimicrobial properties against Streptococcus mutans and Lactobacillus acidophilus—the bacteria responsible for caries formation. Additionally, all tested oils showed antifungal properties against Candida albicans [60].
4.3. Limitation of the Review and Future Insights
The collected studies show that there is a large group of different modifiers showing antibacterial properties. The antibiocidal character of materials are tested against different, not standardized microorganisms like Streptococcus mutans, Staphylococcus aureus, Porphyromonas gingivalis, Lactobacillus acidophilus, Enterococcus faecalis, Staphylococcus aureus, Streptococcus sanguinis, Streptococcus mitis, Escherichia coli, and Helicobacter pylori. Therefore, it is worth proposing at this point to limit pathogen testing to the use of cultures that participate to the greatest extent in the development of caries, i.e., Streptococcus mutans and Candida albicans, as well as to establish specific, standardized/unified test procedures.
Comprehensive analysis to determine whether a modifier can be used in a resin-based dental composite examining at least the basic mechanical (hardness, flexural strength, and modulus) and chemical properties (water sorption) and their long-term stability is crucial. Unfortunately, in some of the cited studies, the methodology was not enriched with any basic strength tests or tests related to the biocompatibility and cytotoxicity of the modifications used, which, on the one hand, indicates potential opportunities for development, but, on the other hand, makes it difficult to select the most promising antibacterial substances. Additionally, some of the cited works took into account only the composition of pure resins, so there is a concern about whether these modifications will also be effective in filled materials, although only such materials are used in dentistry due to the required functional properties.
5. Conclusions
Dental composites, despite their many advantages, are prone to bacterial invasion and biofilm formation on their surfaces or in gaps between the replacement materials and teeth. Developing RBCs whose compositions are able to reduce bacterial colonization would improve clinical success. It is also important that a modification does not adversely affect the mechanical properties of the material, reducing the strength of the RBCs. The development of an antimicrobial composite that is embedded in the structure of the material without being released directly from the structure could positively influence the longevity of composite reconstructions. An antimicrobial agent incorporated into the structure would avoid changes in the structure caused by the release of the modifier and thus limit changes in the mechanical properties of the material.
Quaternary ammonium compounds are an interesting option, as they can achieve high antibacterial efficiency. However, there are reports of their potential cytotoxicity, so further studies are needed to verify these hypotheses to see what effects lower concentrations of QACs have and how they affect the strength properties of composites. A composite modified with ZnO@m-SiO2 and non-porous SiO2 particles is a noteworthy proposal, and it achieved high antimicrobial efficiencies of over 99.9%.
However, additional studies are required to investigate the sustained antimicrobial efficacy and mechanical durability of composites enriched in such compounds over longer periods. Utilizing translational models to test these substances in environments that simulate the conditions of the oral cavity is essential to validate their clinical performance and explore novel applications of these materials. Some studies have found deterioration in the mechanical properties of composite materials. Therefore, it is necessary to develop standardized testing methodologies and strategies to obtain a material with antimicrobial properties while maintaining adequate material strength to ensure the durability and longevity of restorations.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app14093710/s1, Table S1. Prisma 2020 Checklist [17].
Author Contributions
Conceptualization, M.Z. and K.B.; methodology, M.Z. and K.B.; formal analysis, M.Z. and K.B.; investigation, M.Z.; data curation, M.Z.; writing—original draft preparation, M.Z.; writing—review and editing, M.Z. and K.B.; visualization, M.Z.; supervision, K.B.; project administration, M.Z. and K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lu, M.; Xuan, S.; Wang, Z. Oral Microbiota: A New View of Body Health. Food Sci. Hum. Wellness 2019, 8, 8–15. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is Secondary Caries with Composites a Material-Based Problem? Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef] [PubMed]
- Mjör, I.A.; Toffenetti, F. Secondary Caries: A Literature Review with Case Reports. Quintessence Int. 2000, 31, 165–179. [Google Scholar] [PubMed]
- Forssten, S.D.; Björklund, M.; Ouwehand, A.C. Streptococcus Mutans, Caries and Simulation Models. Nutrients 2010, 2, 290–298. [Google Scholar] [CrossRef]
- Al Sunbul, H.; Silikas, N.; Watts, D.C. Polymerization Shrinkage Kinetics and Shrinkage-Stress in Dental Resin-Composites. Dent. Mater. 2016, 32, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Suh, B.I.; Yang, J. Antibacterial Dental Restorative Materials: A Review. Am. J. Dent. 2018, 31, 6B–12B. [Google Scholar]
- Alansy, A.S.; Saeed, T.A.; Guo, Y.; Yang, Y.; Liu, B.; Fan, Z. Antibacterial Dental Resin Composites: A Narrative Review. Open J. Stomatol. 2022, 12, 147–165. [Google Scholar] [CrossRef]
- Sakaguchi, R.; Ferracane, J.; Powers, J. (Eds.) Chapter 9—Restorative Materials: Resin Composites and Polymers. In Craig’s Restorative Dental Materials, 14th ed.; Elsevier: Philadelphia, PA, USA, 2019; pp. 135–170. ISBN 978-0-323-47821-2. [Google Scholar]
- Combe, E.C.; Purzyński, M. Wstęp Do Materiałoznawstwa Stomatologicznego; Wydawnictwo Medyczne Sanmedica: Warszawa, Poland, 1997; ISBN 8386516321. [Google Scholar]
- Fabiano, F.; Calabrese, L.; Proverbio, E. Chapter 9—Mechanical Behavior of Hydroxyapatite-Based Dental Resin Composites. In Materials for Biomedical Engineering; Holban, A.-M., Grumezescu, A.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 251–295. ISBN 978-0-12-816909-4. [Google Scholar]
- Elfakhri, F.; Alkahtani, R.; Li, C.; Khaliq, J. Influence of Filler Characteristics on the Performance of Dental Composites: A Comprehensive Review. Ceram. Int. 2022, 48, 27280–27294. [Google Scholar] [CrossRef]
- Ludovichetti, F.S.; Lucchi, P.; Zambon, G.; Pezzato, L.; Bertolini, R.; Zerman, N.; Stellini, E.; Mazzoleni, S. Depth of Cure, Hardness, Roughness and Filler Dimension of Bulk-Fill Flowable, Conventional Flowable and High-Strength Universal Injectable Composites: An In Vitro Study. Nanomaterials 2022, 12, 1951. [Google Scholar] [CrossRef]
- Beyth, N.; Farah, S.; Domb, A.J.; Weiss, E.I. Antibacterial Dental Resin Composites. React. Funct. Polym. 2014, 75, 81–88. [Google Scholar] [CrossRef]
- Mitwalli, H.; Alsahafi, R.; Balhaddad, A.A.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Emerging Contact-Killing Antibacterial Strategies for Developing Anti-Biofilm Dental Polymeric Restorative Materials. Bioengineering 2020, 7, 83. [Google Scholar] [CrossRef]
- Ren, J.; Guo, X. The Germicidal Effect, Biosafety and Mechanical Properties of Antibacterial Resin Composite in Cavity Filling. Heliyon 2023, 9, e19078. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa-Pacher, A. Research Questions with PICO: A Universal Mnemonic. Publications 2022, 10, 21. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cunha, D.A.; Rodrigues, N.S.; Souza, L.C.; Lomonaco, D.; Rodrigues, F.P.; Degrazia, F.W.; Collares, F.M.; Sauro, S.; Saboia, V.P.A. Physicochemical and Microbiological Assessment of an Experimental Composite Doped with Triclosan-Loaded Halloysite Nanotubes. Materials 2018, 11, 1080. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Dong, X.; Yu, Q.; Baker, S.N.; Li, H.; Larm, N.E.; Baker, G.A.; Chen, L.; Tan, J.; Chen, M. Incorporation of Antibacterial Agent Derived Deep Eutectic Solvent into an Active Dental Composite. Dent. Mater. 2017, 33, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Boaro, L.C.C.; Campos, L.M.; Varca, G.H.C.; dos Santos, T.M.R.; Marques, P.A.; Sugii, M.M.; Saldanha, N.R.; Cogo-Müller, K.; Brandt, W.C.; Braga, R.R.; et al. Antibacterial Resin-Based Composite Containing Chlorhexidine for Dental Applications. Dent. Mater. 2019, 35, 909–918. [Google Scholar] [CrossRef]
- Cao, W.; Zhang, Y.; Wang, X.; Chen, Y.; Li, Q.; Xing, X.; Xiao, Y.; Peng, X.; Ye, Z. Development of a Novel Resin-Based Dental Material with Dual Biocidal Modes and Sustained Release of Ag+ Ions Based on Photocurable Core-Shell AgBr/Cationic Polymer Nanocomposites. J. Mater. Sci. Mater. Med. 2017, 28, 103. [Google Scholar] [CrossRef]
- Zhou, S.; Deng, C.; Liu, H.; Sun, Y.; Zhang, J. Investigating the Antibacterial Activity of Thyme Oil/TiO2 Modified Resins against Oral Pathogenic Bacteria. Alex. Eng. J. 2024, 89, 195–201. [Google Scholar] [CrossRef]
- Fugolin, A.P.; Dobson, A.; Huynh, V.; Mbiya, W.; Navarro, O.; Franca, C.M.; Logan, M.; Merritt, J.L.; Ferracane, J.L.; Pfeifer, C.S. Antibacterial, Ester-Free Monomers: Polymerization Kinetics, Mechanical Properties, Biocompatibility and Anti-Biofilm Activity. Acta Biomater. 2019, 100, 132–141. [Google Scholar] [CrossRef]
- Fanfoni, L.; Marsich, E.; Turco, G.; Breschi, L.; Cadenaro, M. Development of Di-Methacrylate Quaternary Ammonium Monomers with Antibacterial Activity. Acta Biomater. 2021, 129, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Cherchali, F.Z.; Mouzali, M.; Tommasino, J.B.; Decoret, D.; Attik, N.; Aboulleil, H.; Seux, D.; Grosgogeat, B. Effectiveness of the DHMAI Monomer in the Development of an Antibacterial Dental Composite. Dent. Mater. 2017, 33, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Huang, S.; Liang, X.; Qin, W.; Liu, F.; Lin, Z.; He, J. The Antibacterial, Cytotoxic, and Flexural Properties of a Composite Resin Containing a Quaternary Ammonium Monomer. J. Prosthet. Dent. 2018, 120, 609–616. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Ye, L.; He, R.; He, J.; Ouyang, S.; Zhang, J. Antibacterial Dental Resin Composites (DRCs) with Synthesized Bis-Quaternary Ammonium Monomethacrylates as Antibacterial Agents. J. Mech. Behav. Biomed. Mater. 2022, 135, 105487. [Google Scholar] [CrossRef] [PubMed]
- Chrószcz-Porębska, M.; Kazek-Kęsik, A.; Chladek, G.; Barszczewska-Rybarek, I. Novel Mechanically Strong and Antibacterial Dimethacrylate Copolymers Based on Quaternary Ammonium Urethane-Dimethacrylate Analogues. Dent. Mater. 2023, 39, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Chrószcz-Porębska, M.W.; Barszczewska-Rybarek, I.M.; Chladek, G. Characterization of the Mechanical Properties, Water Sorption, and Solubility of Antibacterial Copolymers of Quaternary Ammonium Urethane-Dimethacrylates and Triethylene Glycol Dimethacrylate. Materials 2022, 15, 5530. [Google Scholar] [CrossRef] [PubMed]
- Alhussein, A.; Alsahafi, R.; Wang, X.; Mitwalli, H.; Filemban, H.; Hack, G.D.; Oates, T.W.; Sun, J.; Weir, M.D.; Xu, H.H.K. Novel Dental Low-Shrinkage-Stress Composite with Antibacterial Dimethylaminododecyl Methacrylate Monomer. J. Funct. Biomater. 2023, 14, 335. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shan, T.; Ren, B.; Zhang, L.; Xu, H.H.K.; Wang, N.; Zhou, X.; Li, H.; Cheng, L. Dimethylaminododecyl Methacrylate-Incorporated Dental Materials Could Be the First Line of Defense against Helicobacter Pylori. Int. J. Mol. Sci. 2023, 24, 13644. [Google Scholar] [CrossRef] [PubMed]
- Saiprasert, P.; Tansakul, C.; Pikulngam, A.; Promphet, P.; Naorungroj, S.; Ratanasathien, S.; Aksornmuang, J.; Talungchit, S. Novel Hydrolytic Resistant Antibacterial Monomers for Dental Resin Adhesive. J. Dent. 2023, 135, 104597. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.A.M.; Garcia, I.M.; Nunes, J.; Visioli, F.; Leitune, V.C.B.; Melo, M.A.; Collares, F.M. Myristyltrimethylammonium Bromide (MYTAB) as a Cationic Surface Agent to Inhibit Streptococcus Mutans Grown over Dental Resins: An in Vitro Study. J. Funct. Biomater. 2020, 11, 9. [Google Scholar] [CrossRef]
- Garcia, I.M.; Leitune, V.C.B.; Rücker, V.B.; Nunes, J.; Visioli, F.; Collares, F.M. Physicochemical and Biological Evaluation of a Triazine-Methacrylate Monomer into a Dental Resin. J. Dent. 2021, 114, 103818. [Google Scholar] [CrossRef]
- Stenhagen, I.S.R.; Rukke, H.V.; Dragland, I.S.; Kopperud, H.M. Effect of Methacrylated Chitosan Incorporated in Experimental Composite and Adhesive on Mechanical Properties and Biofilm Formation. Eur. J. Oral Sci. 2019, 127, 81–88. [Google Scholar] [CrossRef]
- Burujeny, S.B.; Yeganeh, H.; Atai, M.; Gholami, H.; Sorayya, M. Bactericidal Dental Nanocomposites Containing 1,2,3-Triazolium-Functionalized POSS Additive Prepared through Thiol-Ene Click Polymerization. Dent. Mater. 2017, 33, 119–131. [Google Scholar] [CrossRef]
- He, J.; Stenhagen, I.S.R.; Dragland, I.S.; Kopperud, H.M. Preparation of a Fluorinated Dental Resin System and Its Anti-Adhesive Properties against S. Mutans. Dent. Mater. 2023, 39, 402–409. [Google Scholar] [CrossRef]
- Zajdowicz, S.; Song, H.B.; Baranek, A.; Bowman, C.N. Evaluation of biofilm formation on novel copper-catalyzed azide-alkyne cycloaddition (CuAAC)-based resins for dental restoratives. Dent. Mater. 2018, 34, 657–666. [Google Scholar] [CrossRef]
- Al-Dulaijan, Y.A.; Cheng, L.; Weir, M.D.; Melo, M.A.S.; Liu, H.; Oates, T.W.; Wang, L.; Xu, H.H.K. Novel Rechargeable Calcium Phosphate Nanocomposite with Antibacterial Activity to Suppress Biofilm Acids and Dental Caries. J. Dent. 2018, 72, 44–52. [Google Scholar] [CrossRef]
- Bhadila, G.; Wang, X.; Zhou, W.; Menon, D.; Melo, M.A.S.; Montaner, S.; Oates, T.W.; Weir, M.D.; Sun, J.; Xu, H.H.K. Novel Low-Shrinkage-Stress Nanocomposite with Remineralization and Antibacterial Abilities to Protect Marginal Enamel under Biofilm. J. Dent. 2020, 99, 103406. [Google Scholar] [CrossRef]
- Mohamed, N.I.; Safy, R.K.; Elezz, A.F.A. Microtensile Bond Strength, Marginal Leakage, and Antibacterial Effect of Bulk Fill Resin Composite with Alkaline Fillers versus Incremental Nanohybrid Composite Resin. Eur. J. Dent. 2021, 15, 425–432. [Google Scholar] [CrossRef]
- Barot, T.; Rawtani, D.; Kulkarni, P. Development of Chlorhexidine Loaded Halloysite Nanotube Based Experimental Resin Composite with Enhanced Physico-Mechanical and Biological Properties for Dental Applications. J. Compos. Sci. 2020, 4, 81. [Google Scholar] [CrossRef]
- Yang, Y.; Xu, Z.; Guo, Y.; Zhang, H.; Qiu, Y.; Li, J.; Ma, D.; Li, Z.; Zhen, P.; Liu, B.; et al. Novel Core–Shell CHX/ACP Nanoparticles Effectively Improve the Mechanical, Antibacterial and Remineralized Properties of the Dental Resin Composite. Dent. Mater. 2021, 37, 636–647. [Google Scholar] [CrossRef]
- Tian, J.; Wu, Z.; Wang, Y.; Han, C.; Zhou, Z.; Guo, D.; Lin, Y.; Ye, Z.; Fu, J. Multifunctional Dental Resin Composite with Antibacterial and Remineralization Properties Containing NMgO-BAG. J. Mech. Behav. Biomed. Mater. 2023, 141, 105783. [Google Scholar] [CrossRef]
- Ai, M.; Du, Z.; Zhu, S.; Geng, H.; Zhang, X.; Cai, Q.; Yang, X. Composite Resin Reinforced with Silver Nanoparticles–Laden Hydroxyapatite Nanowires for Dental Application. Dent. Mater. 2017, 33, 12–22. [Google Scholar] [CrossRef]
- Tanaka, C.B.; Lopes, D.P.; Kikuchi, L.N.T.; Moreira, M.S.; Catalani, L.H.; Braga, R.R.; Kruzic, J.J.; Gonçalves, F. Development of Novel Dental Restorative Composites with Dibasic Calcium Phosphate Loaded Chitosan Fillers. Dent. Mater. 2020, 36, 551–559. [Google Scholar] [CrossRef]
- Dias, H.B.; Bernardi, M.I.B.; Bauab, T.M.; Hernandes, A.C.; de Souza Rastelli, A.N. Titanium Dioxide and Modified Titanium Dioxide by Silver Nanoparticles as an Anti Biofilm Filler Content for Composite Resins. Dent. Mater. 2019, 35, e36–e46. [Google Scholar] [CrossRef]
- Chambers, C.; Stewart, S.B.; Su, B.; Jenkinson, H.F.; Sandy, J.R.; Ireland, A.J. Silver Doped Titanium Dioxide Nanoparticles as Antimicrobial Additives to Dental Polymers. Dent. Mater. 2017, 33, e115–e123. [Google Scholar] [CrossRef]
- Chatzistavrou, X.; Lefkelidou, A.; Papadopoulou, L.; Pavlidou, E.; Paraskevopoulos, K.M.; Christopher Fenno, J.; Flannagan, S.; González-Cabezas, C.; Kotsanos, N.; Papagerakis, P. Bactericidal and Bioactive Dental Composites. Front. Physiol. 2018, 9, 103. [Google Scholar] [CrossRef]
- Arif, W.; Rana, N.F.; Saleem, I.; Tanweer, T.; Khan, M.J.; Alshareef, S.A.; Sheikh, H.M.; Alaryani, F.S.; AL-Kattan, M.O.; Alatawi, H.A.; et al. Antibacterial Activity of Dental Composite with Ciprofloxacin Loaded Silver Nanoparticles. Molecules 2022, 27, 7182. [Google Scholar] [CrossRef]
- Srivastava, R.; Sun, Y. Silver Sulfadiazine Immobilized Glass as Antimicrobial Fillers for Dental Restorative Materials. Mater. Sci. Eng. C 2017, 75, 524–534. [Google Scholar] [CrossRef]
- Dias, H.B.; Bernardi, M.I.B.; Ramos, M.A.D.S.; Trevisan, T.C.; Bauab, T.M.; Hernandes, A.C.; de Souza Rastelli, A.N. Zinc Oxide 3D Microstructures as an Antimicrobial Filler Content for Composite Resins. Microsc. Res. Tech. 2017, 80, 634–643. [Google Scholar] [CrossRef]
- Wang, Y.; Hua, H.; Li, W.; Wang, R.; Jiang, X.; Zhu, M. Strong Antibacterial Dental Resin Composites Containing Cellulose Nanocrystal/Zinc Oxide Nanohybrids. J. Dent. 2019, 80, 23–29. [Google Scholar] [CrossRef]
- Chen, H.; Wang, R.; Zhang, J.; Hua, H.; Zhu, M. Synthesis of Core-Shell Structured ZnO@m-SiO2 with Excellent Reinforcing Effect and Antimicrobial Activity for Dental Resin Composites. Dent. Mater. 2018, 34, 1846–1855. [Google Scholar] [CrossRef]
- Qin, L.; Yao, S.; Meng, W.; Zhang, J.; Shi, R.; Zhou, C.; Wu, J. Novel Antibacterial Dental Resin Containing Silanized Hydroxyapatite Nanofibers with Remineralization Capability. Dent. Mater. 2022, 38, 1989–2002. [Google Scholar] [CrossRef]
- Yang, S.Y.; Han, A.R.; Choi, J.W.; Kim, K.M.; Kwon, J.S. Novel Antibacterial and Apatite Forming Restorative Composite Resin Incorporated with Hydrated Calcium Silicate. Biomater. Res. 2023, 27, 1–15. [Google Scholar] [CrossRef]
- Go, H.B.; Lee, M.J.; Seo, J.Y.; Byun, S.Y.; Kwon, J.S. Mechanical Properties and Sustainable Bacterial Resistance Effect of Strontium-Modified Phosphate-Based Glass Microfiller in Dental Composite Resins. Sci. Rep. 2023, 13, 17763. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, J.; Zhang, T.; Yao, S.; Wang, Z.; Zhou, C.; Wu, J. Novel Low-Shrinkage Dental Resin Containing Microcapsules with Antibacterial and Self-Healing Properties. J. Mech. Behav. Biomed. Mater. 2023, 148, 106212. [Google Scholar] [CrossRef]
- Adeeb, S.; Adeeb, S.; Chladek, G.; Pakieła, W.; Mertas, A. Influence of Silver-Containing Filler on Antibacterial Properties of Experimentaresin Composites against Enterococcus Faecalis. J. Achiev. Mater. Manuf. Eng. 2021, 109, 59–67. [Google Scholar] [CrossRef]
- Lapinska, B.; Szram, A.; Zarzycka, B.; Grzegorczyk, J.; Hardan, L.; Sokolowski, J.; Lukomska-Szymanska, M. An in Vitro Study on the Antimicrobial Properties of Essential Oil Modified Resin Composite against Oral Pathogens. Materials 2020, 13, 4383. [Google Scholar] [CrossRef]
- Kim, K.H.; Mai, H.N.; Hyun, D.C.; Lee, D.H. New Autonomous Water-Enabled Self-Healing Coating Material with Antibacterial-Agent-Releasing Properties. Pharmaceutics 2022, 14, 1005. [Google Scholar] [CrossRef]
- Mai, H.N.; Kim, D.Y.; Hyun, D.C.; Park, J.H.; Lee, S.M.; Lee, D.H. A New Antibacterial Agent-Releasing Polydimethylsiloxane Coating for Polymethyl Methacrylate Dental Restorations. J. Clin. Med. 2019, 8, 1831. [Google Scholar] [CrossRef]
- ul Haque, S.; Nasar, A.; Inamuddin. 27—Montmorillonite Clay Nanocomposites for Drug Delivery. In Applications of Nanocomposite Materials in Drug Delivery; Woodhead Publishing Series in Biomaterials; Inamuddin, Asiri, A.M., Mohammad, A., Eds.; Woodhead Publishing: Cambridge, UK, 2018; pp. 633–648. ISBN 978-0-12-813741-3. [Google Scholar]
- Altaie, A.; Bubb, N.; Franklin, P.; German, M.J.; Marie, A.; Wood, D.J. Development and Characterisation of Dental Composites Containing Anisotropic Fluorapatite Bundles and Rods. Dent. Mater. 2020, 36, 1071–1085. [Google Scholar] [CrossRef]
- Zalega, M.; Nowak, J.; Bociong, K. The Influence of Quaternary Ammonium Salts on Mechanical Properties of Light-Cured Resin Dental Composites. Polimery 2023, 68, 195–205. [Google Scholar] [CrossRef]
- Fujimura, Y.; Weerasinghe, D.; Kawashima, M. Development of an Antibacterial Bioactive Dental Adhesive: Simplicity and Innovation. Am. J. Dent. 2018, 31, 13B–16B. [Google Scholar] [PubMed]
- Xue, J.; Wang, J.; Feng, D.; Huang, H.; Wang, M. Application of Antimicrobial Polymers in the Development of Dental Resin Composite. Molecules 2020, 25, 4738. [Google Scholar] [CrossRef] [PubMed]
- Bienek, D.R.; Frukhtbeyn, S.A.; Giuseppetti, A.A.; Okeke, U.C.; Pires, R.M.; Antonucci, J.M.; Skrtic, D. Ionic Dimethacrylates for Antimicrobial and Remineralizing Dental Composites. Ann. Dent. Oral Disord. 2018, 2, 108. [Google Scholar] [PubMed]
Figure 1.
Classification of antibacterial composite modifications.
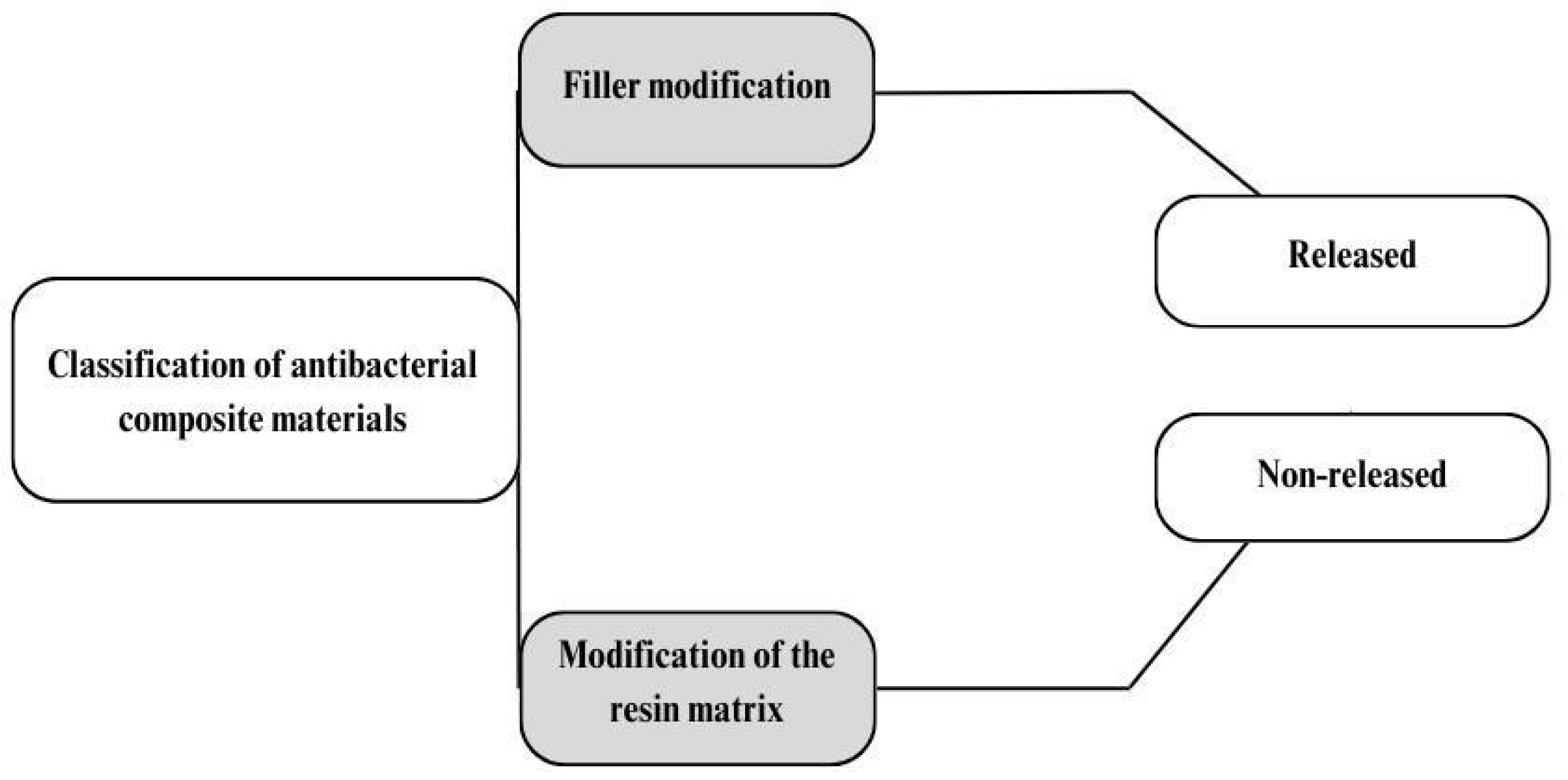
Figure 2.
Diagram of the PICO structure implemented in this review.

Figure 3.
PRISMA scheme implemented in this review.
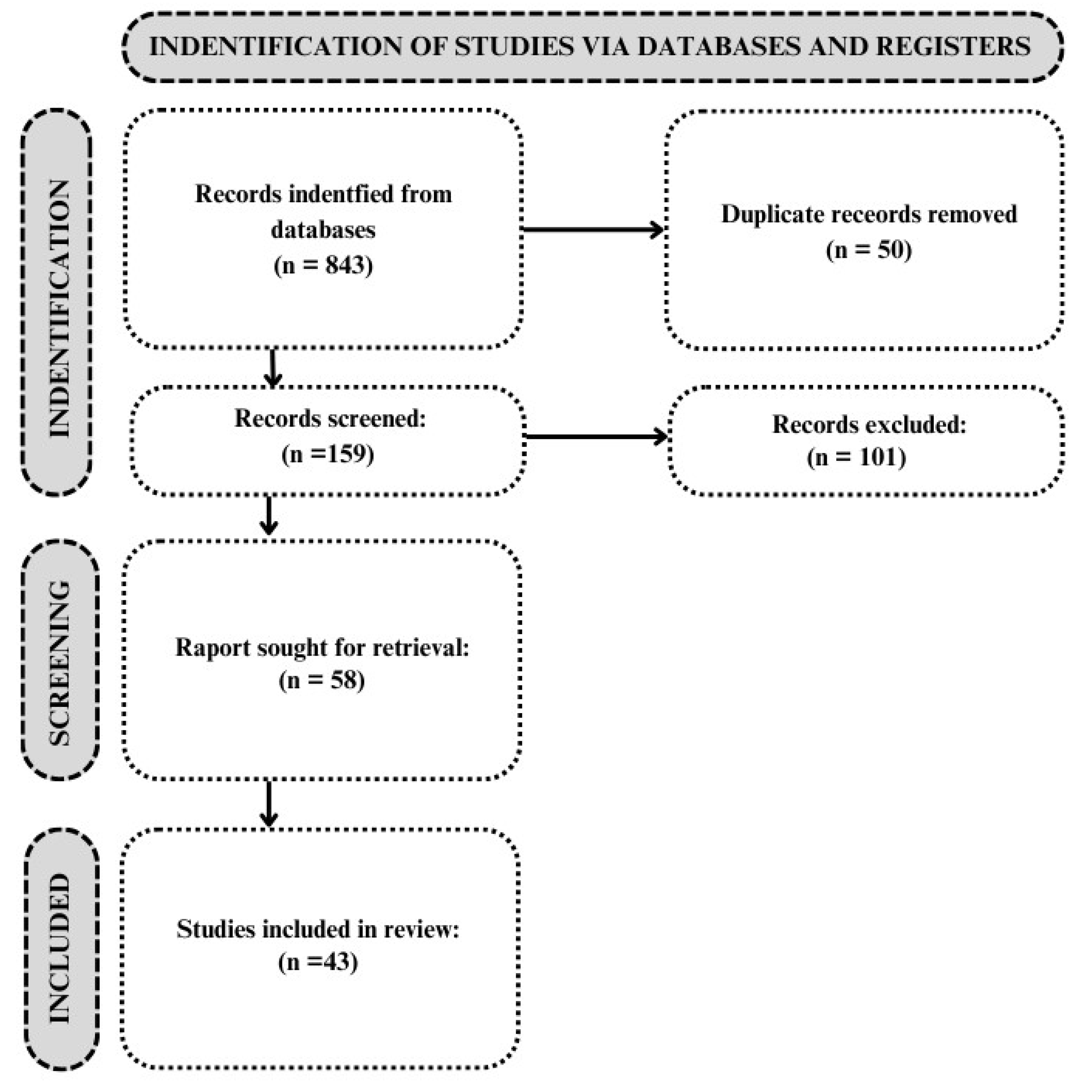
Figure 4.
Released modificator.
Figure 5.
Layers of MMT with Chlorhexidine.
Figure 6.
Dimethyl-hexadecyl-methacryloxyethyl-ammonium iodide (DHMAI).

Figure 7.
Methacryloyloxydodecylpyridinium bromide (MDPB).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The inclusion and exclusion criteria implemented in this review.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Published since 2017 Publication in English Containing the following keywords “dental AND materials AND antibacterial modifier” OR “dental AND materials AND antibacterial agent” OR “antibacterial polymer” OR “antibacterial dental resin” OR “resin composites AND antibacterial modification AND antibacterial agent OR “antimicrobial monomers AND dental resin composite” OR “dental AND composite AND antibacterial” OR “dental AND composite AND antibacterial AND properties”. | Published before 2017 Publication not in English Publications without keywords |
Table 2.
Biocidal dental resin materials.
| Modification |
Microorganisms Tested | Results | References |
|---|---|---|---|
| Triclosan-encapsulated halloysite nanotubes | Streptococcus mutans | No significant antimicrobial effect was observed between the groups for CFUs and similarly for dry mass | [18] |
| Deep eutectic solvent (DES) with benzalkonium chloride (BC) and acrylic acid (AA) | Streptococcus mutans, Staphylococcus aureus | BC-C produced a larger inhibitory halo | [19] |
| MMT loaded with chlorhexidine (CHX) | Staphylococcus aureus, Streptococcus mutans, Porphyromonas gingivalis | Among the three tested bacteria, modified composites exhibited growth inhibition at all concentrations with one exception (2.5%)—no growth inhibition of Porphyromonas gingivalis was observed | [20] |
| Core–shell AgBr/cationic polymer nanocomposite (AgBr/BHPVP) | Streptococcus mutans | Strong bactericidal effect | [21] |
| Thyme oil/TiO2 nanoparticle filler | Streptococcus mutans, Lactobacillus acidophilus, Candida albicans | The resin containing 2 wt% thyme/TiO2 exhibited the most significant inhibition zone against Streptococcus mutans. Similar trends were observed against Lactobacillus acidophilus and Candida albicans | [22] |
| Tertiary quaternary ammonium acrylamides (AMs) and methacrylamides (MAMs) with alkyl side chain lengths of 9 and 14 carbons (C9 and C14) | Streptococcus mutans | All the C14 versions demonstrated potent antibacterial properties | [23] |
| Nine monomers based on bis-quaternary ammonium salts were prepared | Streptococcus mutans, Escherichia coli, Staphylococcus aureus, Streptococcus sanguinis, Streptococcus mitis | All bis-QAMs were capable of inhibiting Streptococcus mutans biofilm formation | [24] |
| Quaternary ammonium dimethyl-hexadecyl-methacryloxyethyl-ammonium iodide (DHMAI), methacryloyloxyethylphosphorylcholine (MPC) | Streptococcus mutans | Reduction in biofilm | [25] |
| Urethane dimethacrylate quaternary ammonium compound (UDMQA-12) | Streptococcus mutans | Significant antibacterial activity | [26] |
| bi-quaternary ammonium methacrylates (biQAMA-12, biQAMA-14, and biQAMA-16) | Streptococcus mutans | BiQAMA-12 showed the greatest antimicrobial efficacy | [27] |
| Quaternary ammonium urethane-dimethacrylate derivative (QAUDMA-m (m—number of carbon atoms in the N-alkyl substituent—8, 10, 12, 14, 16, 18)) | Staphylococcus aureus, Escherichia coli | Three copolymers, BG:QA8:TEG, BG:QA10:TEG, and BG:QA12:TEG, demonstrated high antibacterial activity against both bacterial strains | [28,29] |
| Dimethylaminododecyl methacrylate (DMADDM) | Streptococcus mutans | The incorporation of 3% and 5% DMADDM resulted in a significant decrease in Streptococcus mutans biofilm colony-forming units (CFUs). Modification with DMADDM led to notable reductions in biofilm biomass and lactic acid levels | [30] |
| Dimethylaminododecyl methacrylate (DMADDM) | Helicobacter pylori | DMADDM reduced H. pylori colonization of oral origin in the stomach, thereby alleviating both local and systemic gastritis | [31] |
| Methacryloyloxydodecylpyridinium bromide (MDPB) | Enterococcus faecalis | Significant antibacterial activity | [32] |
| Myristyltrimethylammonium Bromide (MYTAB) | Streptococcus mutans | Antimicrobial activity against biofilm formation was obtained with 0.5 wt%, and activity against planktonic bacteria was obtained with 1 wt% | [33] |
| 2.5 or 5 wt % of the methacrylate monomer 1,3,5-triacryloylhexahydro-1,3,5-triazine (TAT) | Streptococcus mutans | The higher the TAT concentration, the higher the antibacterial activity | [34] |
| Methacrylated chitosan (CH-MA) | Streptococcus mutans | Reduction in biofilm formation | [35] |
| 1,2,3-triazolium-functionalized POSS | Streptococcus mutans | The nanocomposite incorporating Triazolium/POSS exhibited markedly elevated bactericidal activity | [36] |
| Fluorinated dimethacrylate FDMA was mixed with triethylene-glycol dimethacrylate (TEGDMA) and fluorinated diluent 1 H,1 H-heptafluorobutyl methacrylate (FBMA) | Streptococcus mutans | The use of fluorinated methacrylate monomers reduced the adhesion of Streptococcus mutans | [37] |
| Copper(I)-catalyzed azide-alkyne cycloaddition (CuAAC) | Streptococcus mutans | Reduction in luciferase activity and the number of viable bacteria recovered from biofilms on CuAAC-based resins | [38] |
| Nanoparticles of amorphous calcium phosphate (NACP) with dimethylaminohexadecyl methacrylate (DMAHDM) | Streptococcus mutans | Reduction in biofilm growth | [39] |
| Triethylene glycol divinylbenzyl ether (TEG-DVBE), and 3% dimethylaminohexadecyl methacrylate (DMAHDM), and 20% calcium phosphate nanoparticles (NACP) | Streptococcus mutans | Exhibited remineralizing and antibacterial properties | [40] |
| Alkaline fillers (alkasite—alkaline fillers such as barium aluminum silicate glass and ytterbium trifluoride) | Streptococcus mutans | The antibacterial effect of alkasite was lesser than that of the control group | [41] |
| Development of Chlorhexidine-loaded halloysite nanotube | Streptococcus mutans | Significant antibacterial activity | [42] |
| Core–shell chlorhexidine/amorphous calcium phosphate (CHX/ACP) nanoparticles | Streptococcus mutans | 5 wt% and more of CHX/ACP nanoparticles effectively inhibited the growth of Streptococcus mutans | [43] |
| Magnesium oxide nanoparticles (nMgO) | Streptococcus mutans | Very good antibacterial properties | [44] |
| Silver nanoparticle (AgNP)-laden HA (HA–PDA–Ag) nanowires | Streptococcus mutans | High antibacterial activity | [45] |
| Chitosan or chitosan loaded with dibasic calcium phosphate anhydrous (DCPA) particles | Streptococcus mutans | The modified composites contained about 20% less biofilm | [46] |
| TiO2 and TiO2/Ag nanoparticles | Streptococcus mutans | Modification with 2% TiO2/Ag nanoparticles significantly reduced biofilm accumulation | [47] |
| Ag–TiO2 filler particles | Streptococcus mutans | Bactericidal effect (small quantities) | [48] |
| Ag–doped sol–gel–derived bioactive glass (Ag–BG) | Streptococcus mutans | As the concentration of Ag–BG in BGCOMP increases, the number of dead bacteria in the biofilm increases | [49] |
| Ciprofloxacin–loaded silver nanoparticles (CIP–AgNPs) | Streptococcus mutans, Enterococcus faecalis, Saliva microorganism | Antimicrobial activity after CIP–AgNP modification was increased | [50] |
| Commercial barium borosilicate-based glass powders immobilized with silver sulfadiazine filler | Streptococcus mutans | Strong and effective action | [51] |
| Zinc oxide 3D microstructures filler | Streptococcus mutans, Escherichia coli, Staphylococcus aureus, Candida albicans | Low quantities of ZnO microparticles significantly inhibited the growth of Streptococcus mutans on the resin surface | [52] |
| Cellulose nanocrystal/zinc oxide nanohybrids | Streptococcus mutans | A 78% reduction in bacterial counts was achieved with the addition of 2% CNC/ZnO nanohybrids | [53] |
| Core–shell-structured ZnO@m-SiO2 | Streptococcus mutans | Superior antimicrobial activity (>99.9%) | [54] |
| Hydroxyapatite nanofibers loaded with erythromycin (s-HAFs@EM) | Streptococcus mutans | Modification with 15–20% s-HAFs@EM showed a high antibacterial rate (>85%) | [55] |
| Hydrated calcium silicate (hCS) | Streptococcus mutans | The adhesion of Streptococcus mutans decreased as the amount of hCS increased. It was found that the relative survival rates of Streptococcus mutans decreased after the addition of hCS | [56] |
| Strontium-modified phosphate-based glass (Sr–PBG) | Streptococcus mutans | A sustained in vitro bacterial resistance effect was achieved | [57] |
| Nanoparticle–modified MC with a nano–antibacterial inorganic filler (NIF) containing a quaternary ammonium salt | Streptococcus mutans | High antimicrobial activity and a corresponding self-healing efficiency of 71% were found | [58] |
| Silver sodium hydrogen zirconium phosphate (S–P) | Enterococcus faecalis | Bacterial colonies were found to be reduced when S–P concentrations ranging from 7% to 13% were used | [59] |
| Essential oils (EOs)—anise, cinnamon, citronella, clove, geranium, lavender, limette, mint, rosemary thyme | Streptococcus mutans, Lactobacillus acidophilus,
Candida albicans | Cinnamon and thyme oils showed the highest antibacterial activity against Streptococcus mutans and Lactobacillus acidophilus. The composite with 2 µL of cinnamon oil showed the best antimicrobial properties against Streptococcus mutans and Candida albicans and that with 1 µL the best antimicrobial properties against Lactobacillus acidophilus | [60] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zalega, M.; Bociong, K. Antibacterial Agents Used in Modifications of Dental Resin Composites: A Systematic Review. Appl. Sci. 2024, 14, 3710. https://doi.org/10.3390/app14093710
AMA Style
Zalega M, Bociong K. Antibacterial Agents Used in Modifications of Dental Resin Composites: A Systematic Review. Applied Sciences. 2024; 14(9):3710. https://doi.org/10.3390/app14093710
Chicago/Turabian StyleZalega, Maja, and Kinga Bociong. 2024. "Antibacterial Agents Used in Modifications of Dental Resin Composites: A Systematic Review" Applied Sciences 14, no. 9: 3710. https://doi.org/10.3390/app14093710
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.