New Instrument for Oral Hygiene of Children with Cleft Lip and Palate

 ,
,  ,
,  ,
,  ,
,  and
and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
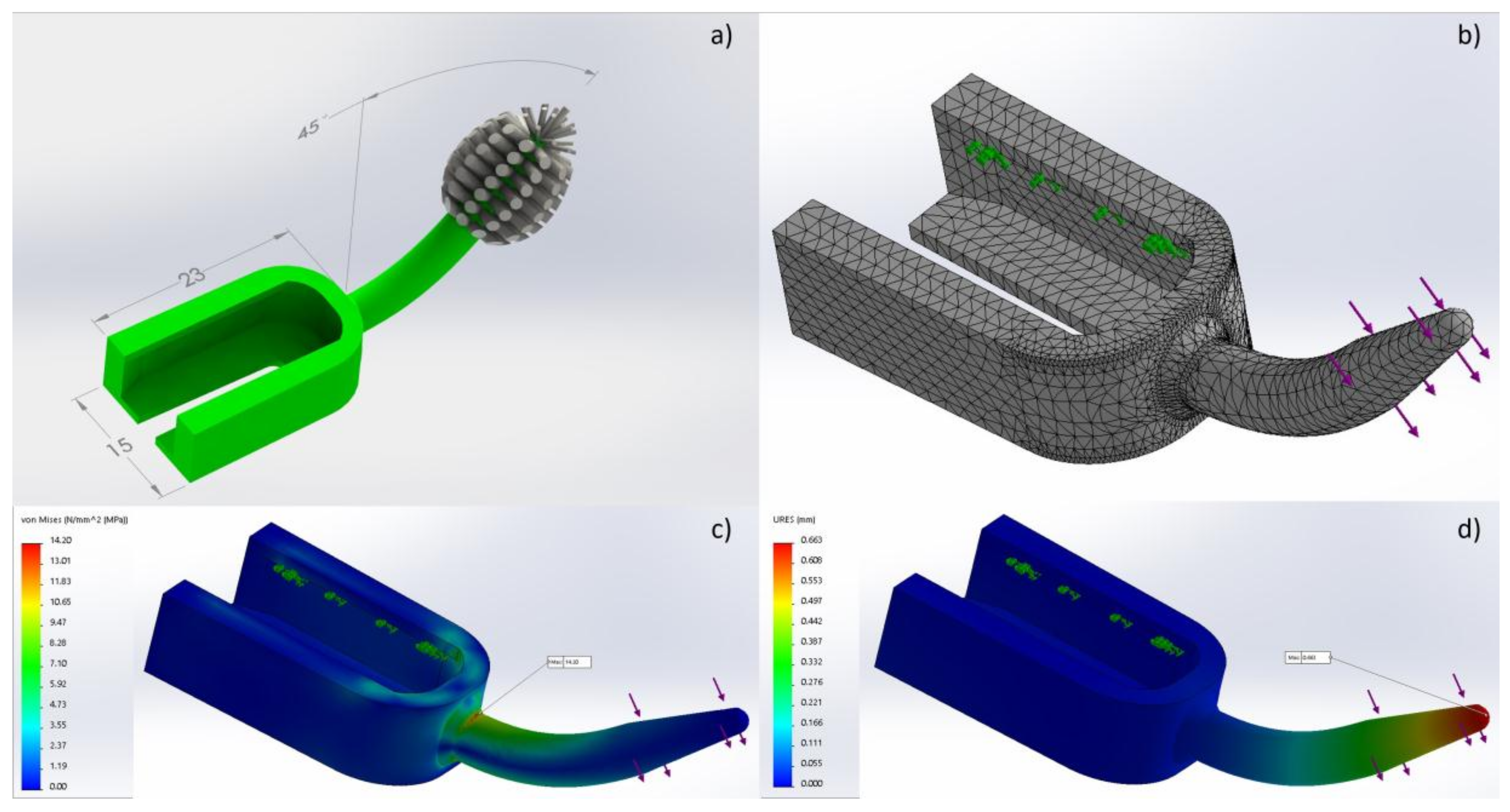
2. Design of the Cleft Toothbrush
Finite Element Simulation
3. The Efficacy of the Cleft Toothbrush
4. Discussion
5. Patent
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Maarse, W.; Rozendaal, A.M.; Pajkrt, E.; Vermeij-Keers, C.; van der Molen, A.B.M.; van den Boogaard, M.-J.H. A systematic review of associated structural and chromosomal defects in oral clefts: When is prenatal genetic analysis indicated? J. Med. Genet. 2012, 49, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Sadler, T.W.T.W.; Langman, J.M.E. Langman’s Medical Embryology, 12th ed.; Sadler, T.W., Ed.; Wolters Kluwer Health: Philadelphia, PA, USA; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Lages, E.M.B.; Marcos, B.; Pordeus, I.A. Oral health of individuals with cleft lip, cleft palate, or both. Cleft Palate-Craniofac. J. 2004, 41, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Hazza’a, A.M.; Rawashdeh, M.A.; Al-Nimri, K.; Al Habashneh, R. Dental and oral hygiene status in jordanian children with cleft lip and palate: A comparison between unilateral and bilateral clefts. Int. J. Dent. Hyg. 2011, 9, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Perdikogianni, H.; Papaioannou, W.; Nakou, M.; Oulis, C.; Papagiannoulis, L. Periodontal and microbiological parameters in children and adolescents with cleft lip and/or palate. Int. J. Paediatr. Dent. 2009, 19, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Shashni, R.; Goyal, A.; Gauba, K.; Utreja, A.K.; Ray, P.; Jena, A.K. Comparison of risk indicators of dental caries in children with and without cleft lip and palate deformities. Contemp. Clin. Dent. 2015, 6, 58–62. [Google Scholar] [PubMed]
- Worth, V.; Perry, R.; Ireland, T.; Wills, A.K.; Sandy, J.; Ness, A. Are people with an orofacial cleft at a higher risk of dental caries? A systematic review and meta-analysis. Br. Dent. J. 2017, 223, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, M.; Brailsford, S.R.; Tarelli, E.; Gilbert, S.C.; Clark, D.T.; Barnard, K.; Beighton, D. Dental caries, oral hygiene, and oral clearance in children with craniofacial disorders. J. Dent. Res. 2004, 83, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, G.; Palaska, P.-K.; Herzog, G. Caries prevalence in non-syndromic patients with cleft lip and/or palate: A meta-analysis. Caries Res. 2013, 47, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.L.; Moor, S.L.; Ho, C.T. Predisposing factors to dental caries in children with cleft lip and palate: A review and strategies for early prevention. Cleft Palate-Craniofac. J. 2007, 44, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Rivkin, C.J.; Keith, O.; Crawford, P.J.; Hathorn, I.S. Dental care for the patient with a cleft lip and palate. Part 2: The mixed dentition stage through to adolescence and young adulthood. Br. Dent. J. 2000, 188, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.L.; Davies, K.; Callery, P. Experience of maintaining tooth brushing for children born with a cleft lip and/or palate. BMC Oral Health 2017, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Gopakumar, M.; Hegde, A.M. Parental attitude towards the provision of nonsurgical oral health care to children with oral clefts: An epidemiological survey. Int. J. Clin. Pediatr. Dent. 2010, 3, 35–37. [Google Scholar] [CrossRef] [PubMed]
- van der Weijden, G.A.; Timmerman, M.F.; Reijerse, E.; Snoek, C.M.; van der Velden, U. Toothbrushing force in relation to plaque removal. J. Clin. Periodontol. 1996, 23, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Hayasaki, H.; Saitoh, I.; Nakakura-Ohshima, K.; Hanasaki, M.; Nogami, Y.; Nakajima, T.; Inada, E.; Iwasaki, T.; Iwase, Y.; Sawami, T.; et al. Tooth brushing for oral prophylaxis. Jpn. Dent. Sci. Rev. 2014, 50, 69–77. [Google Scholar] [CrossRef]
- Bizhang, M.; Schmidt, I.; Chun, Y.-H.P.; Arnold, W.H.; Zimmer, S. Toothbrush abrasivity in a long-term simulation on human dentin depends on brushing mode and bristle arrangement. PLoS ONE 2017, 12, e0172060. [Google Scholar] [CrossRef] [PubMed]
- Spina, V. A proposed modification for the classification of cleft lip and cleft palate. Cleft Palate J. 1973, 10, 251–252. [Google Scholar] [PubMed]
- Dentistry, A.A.O.P. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Pediatr. Dent. 2013, 35, E148. [Google Scholar]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ashley, P. Toothbrushing: Why, when and how? Dent. Update 2001, 28, 36–40. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, R.; Fernandes, M.H.; Bessa Monteiro, A.; Furfuro, R.; Carvalho Silva, C.; Soares, C.; Vardasca, R.; Mendes, J.; Manso, M.C. New Instrument for Oral Hygiene of Children with Cleft Lip and Palate. Appl. Sci. 2018, 8, 576. https://doi.org/10.3390/app8040576
Rodrigues R, Fernandes MH, Bessa Monteiro A, Furfuro R, Carvalho Silva C, Soares C, Vardasca R, Mendes J, Manso MC. New Instrument for Oral Hygiene of Children with Cleft Lip and Palate. Applied Sciences. 2018; 8(4):576. https://doi.org/10.3390/app8040576
Chicago/Turabian StyleRodrigues, Rita, Maria Helena Fernandes, António Bessa Monteiro, Rowney Furfuro, Cátia Carvalho Silva, César Soares, Ricardo Vardasca, Joaquim Mendes, and Maria Conceição Manso. 2018. "New Instrument for Oral Hygiene of Children with Cleft Lip and Palate" Applied Sciences 8, no. 4: 576. https://doi.org/10.3390/app8040576
APA StyleRodrigues, R., Fernandes, M. H., Bessa Monteiro, A., Furfuro, R., Carvalho Silva, C., Soares, C., Vardasca, R., Mendes, J., & Manso, M. C. (2018). New Instrument for Oral Hygiene of Children with Cleft Lip and Palate. Applied Sciences, 8(4), 576. https://doi.org/10.3390/app8040576