An Ergonomic Customized-Tool Handle Design for Precision Tools using Additive Manufacturing: A Case Study

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Introduction
2.2. Participants
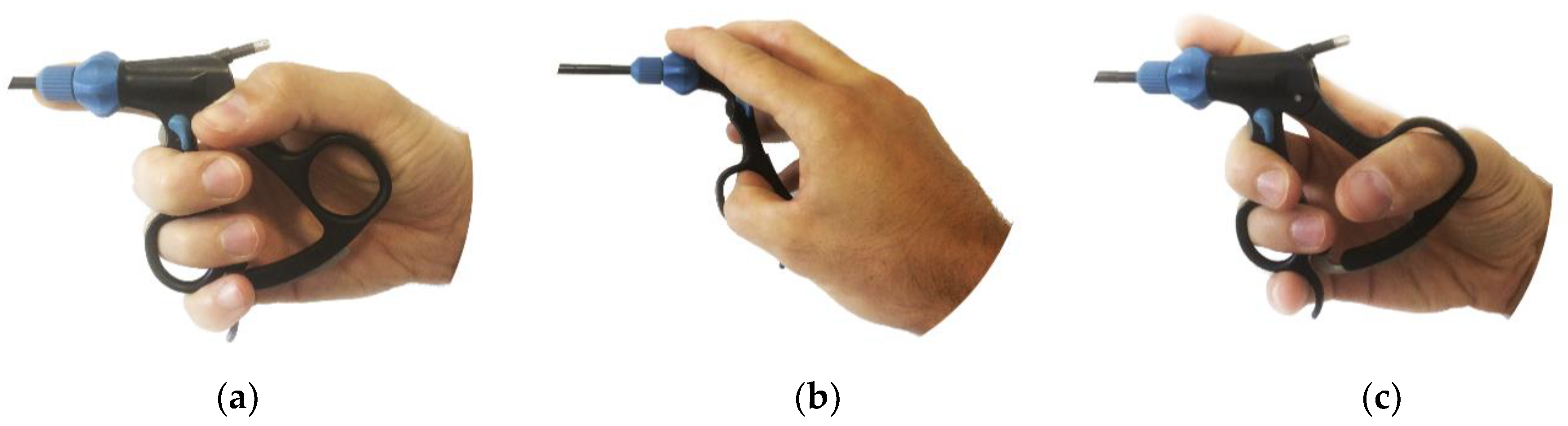
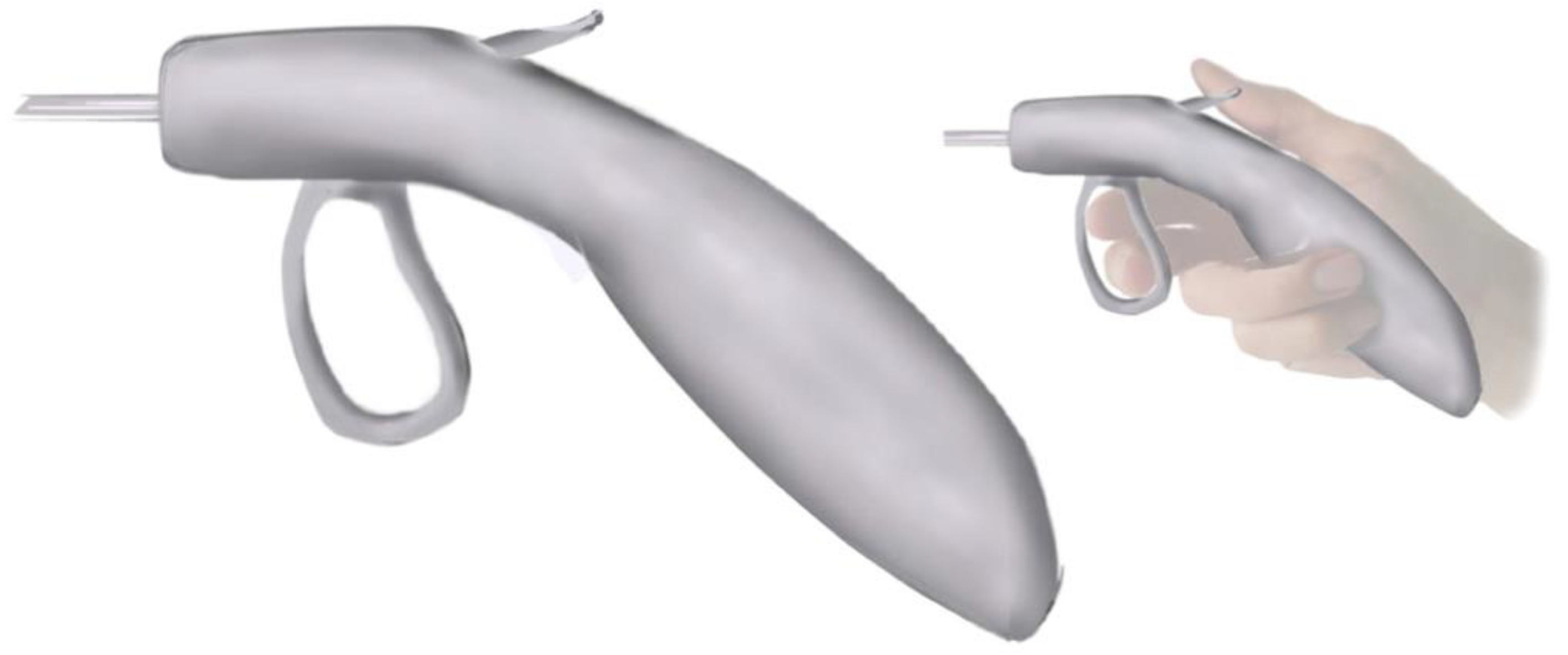
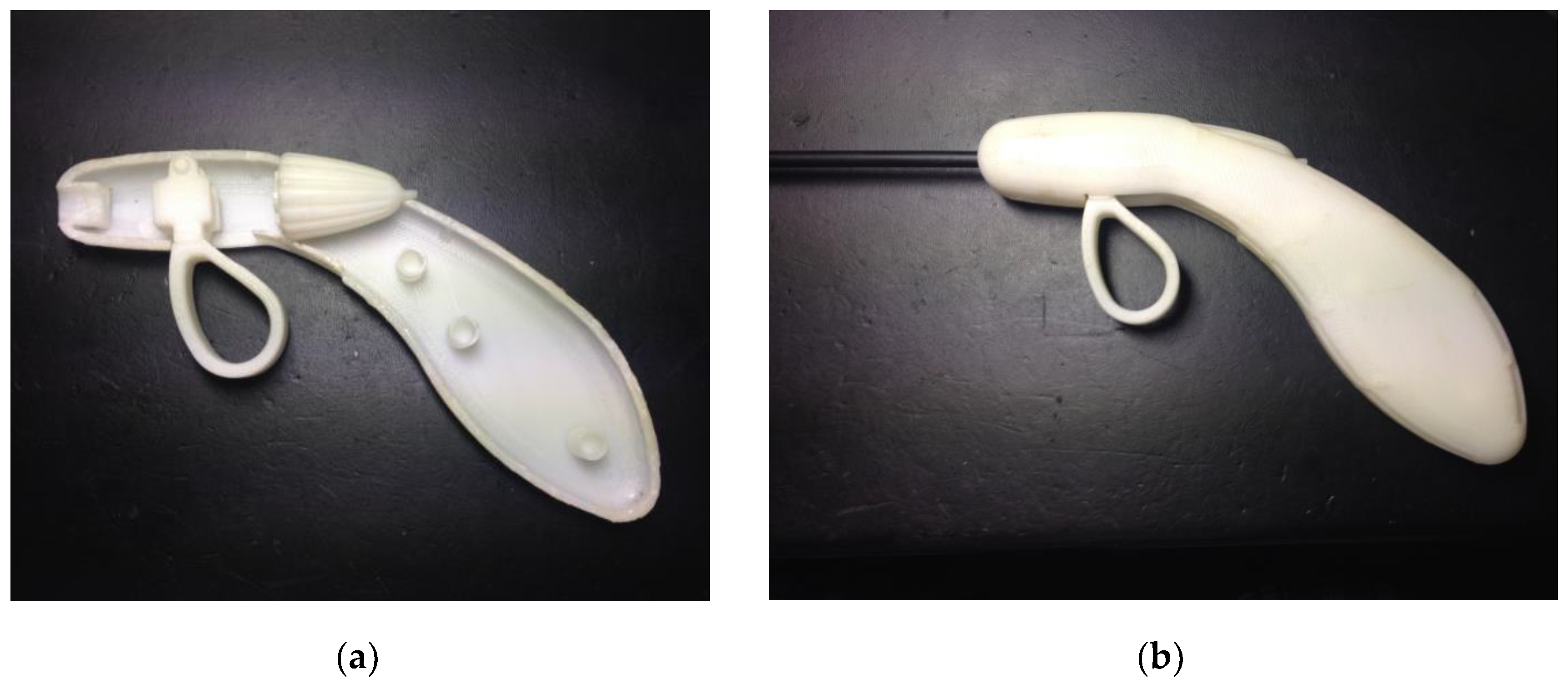
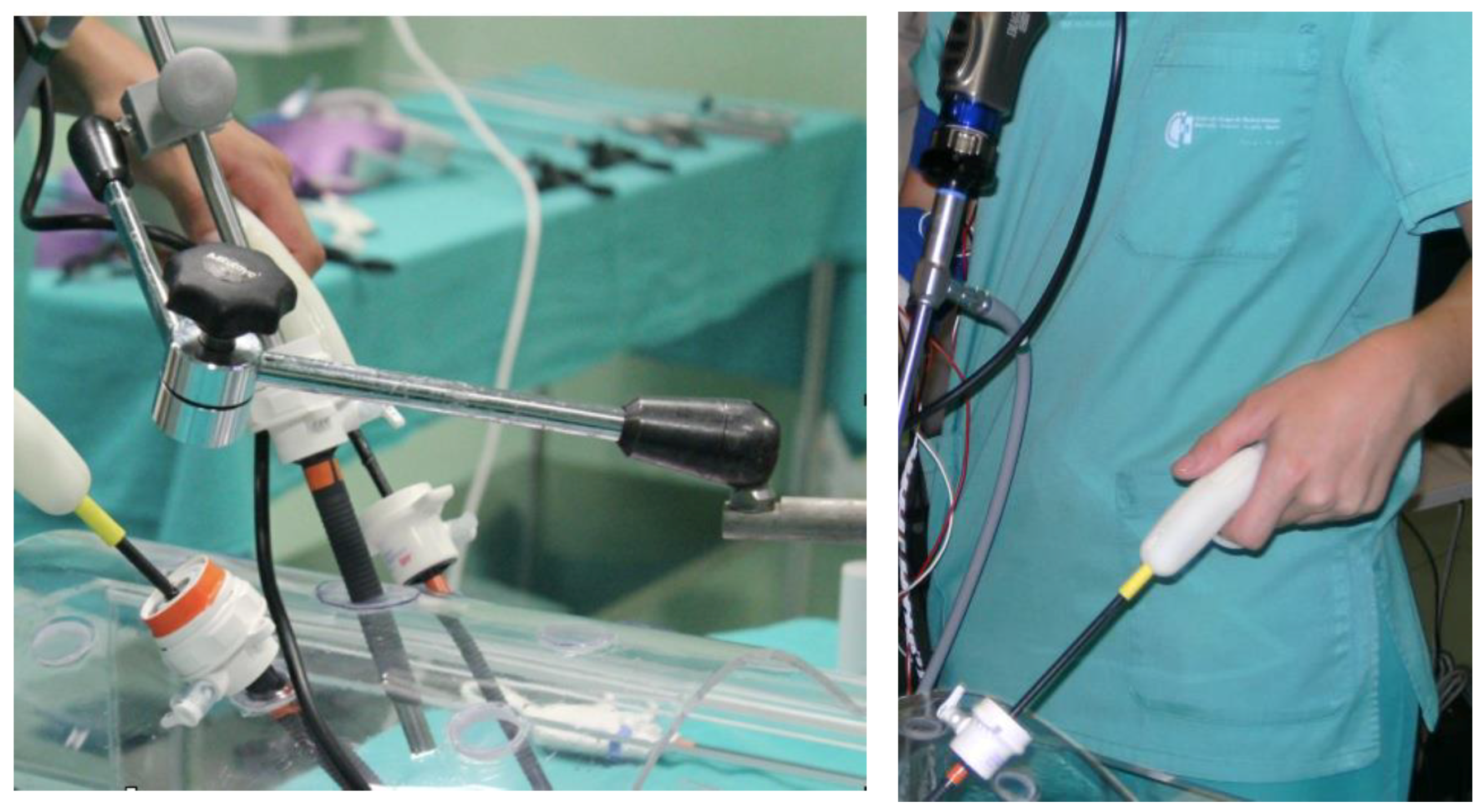
2.3. Experimental Task and the Parametric Prototype Handle
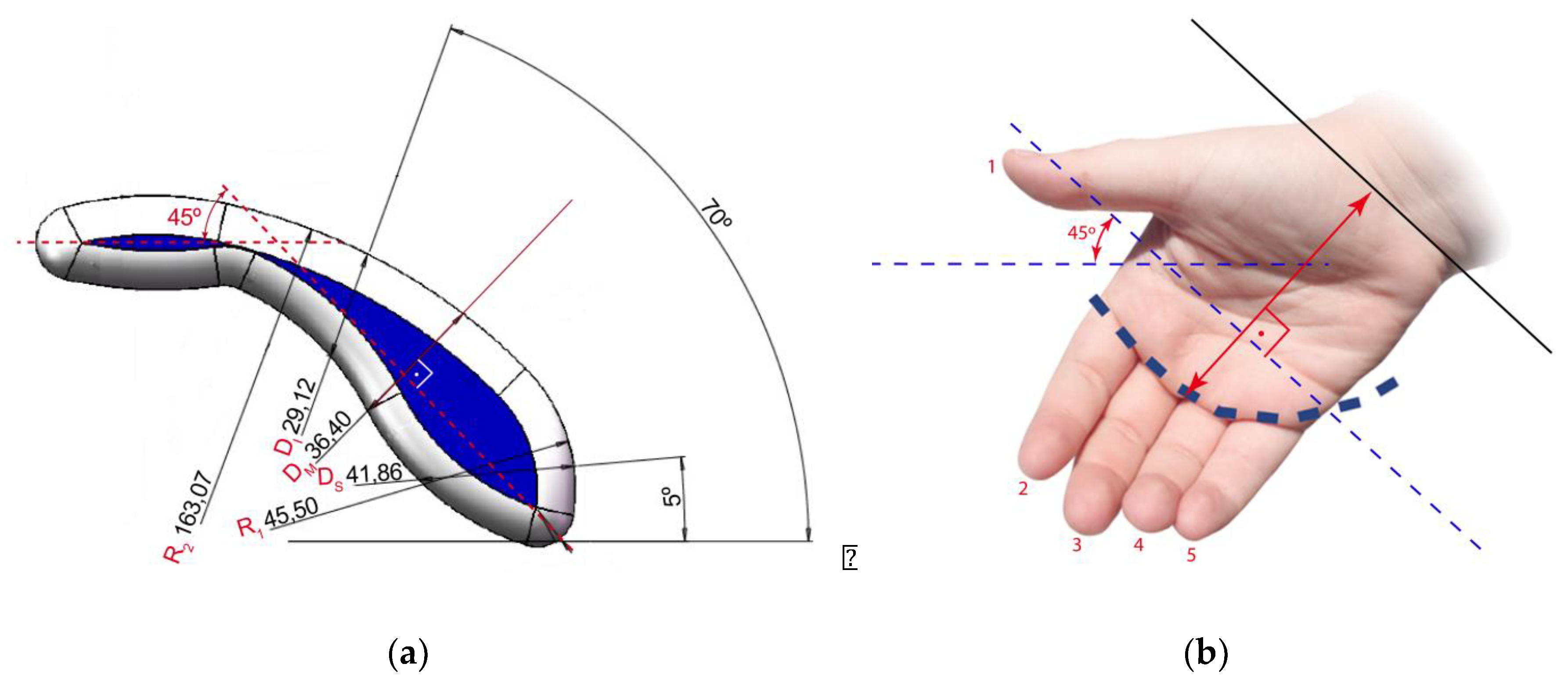
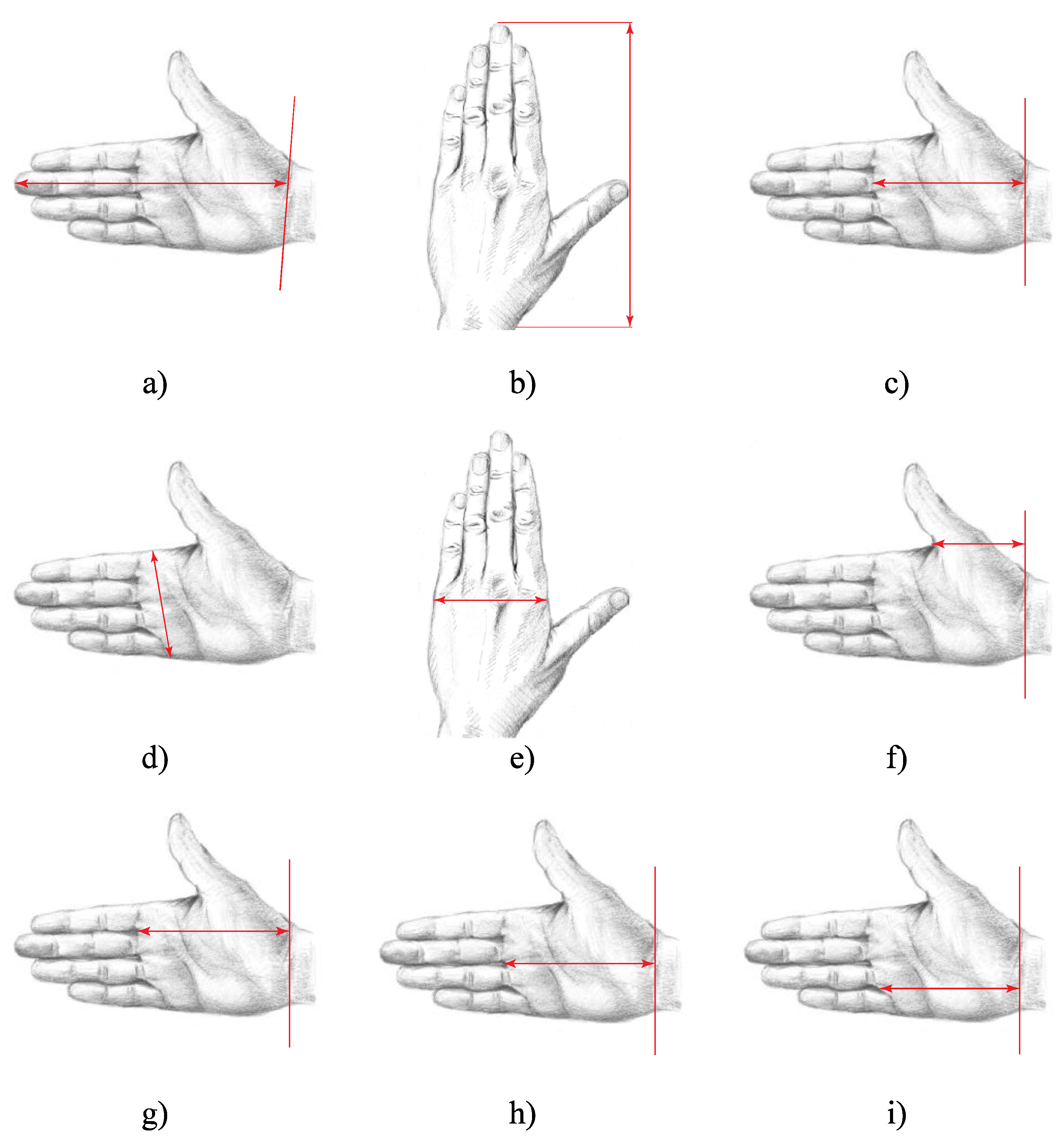
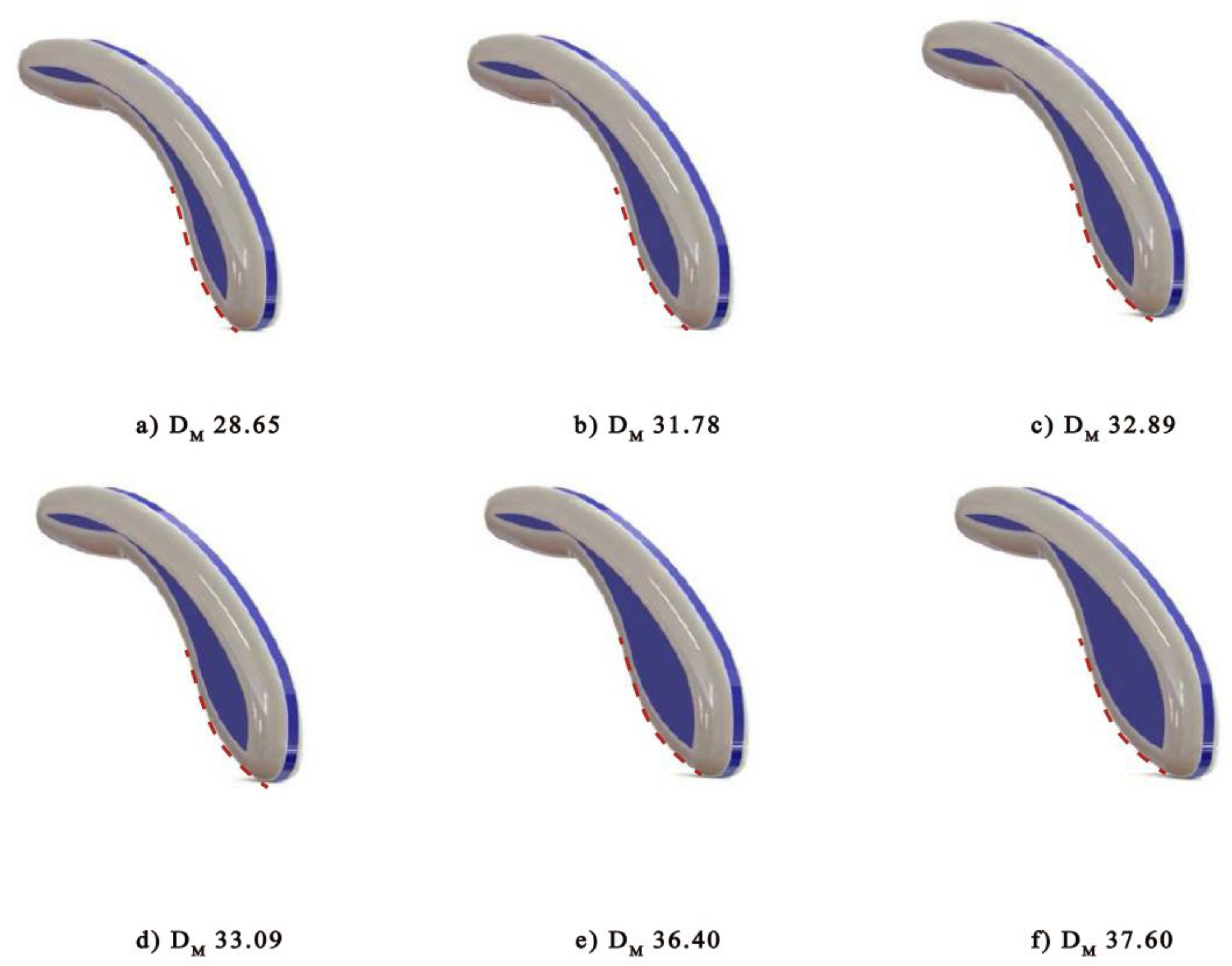
2.4. Anthropometric Relationship between the Surgeon’s Hand and the Size of the Handle
- Measurements related to the palm support of the handle—these correspond to the importance of having greater contact between hand and handle, and are therefore related to the breadth of the hand.
- Measurements related to the diameter of the handle—these correspond to the handle appropriately fitting the different types of hand, allowing the fingers to have a greater contact surface, and are therefore related to the total length of the hand and the length of the palm.
3. Results and Discussion
4. Conclusions
- A 3D parametric CAD design has been obtained for the handle of laparoscopic surgery graspers that is scalable for different hand sizes. All of the resulting models personally customized for each surgeon complied with the ergonomic criteria for their use.
- The results show that additive manufacturing and the application of ergonomics criterion provide an efficient method for the customized design and manufacture of this type of specialized tools, being possible to be applicable to other sectors.
- The relationship between the anthropometry of the surgeon’s hand and the most suitable size of the handle was determined, with the most suitable anthropometric parameter to measure being the “Palm Length Measured” (PLM).
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mace, R.L. Universal Design Universal Design: Barrier free environments for everyone. Design. West 1985, 33, 147–152. [Google Scholar]
- Mace, R.L.; Ostroff, E.; Connell, B.R.; Jones, M.; Mueller, J.; Mullick, A.; Sanford, J.; Steinfeld, E.; Follette Story, M.; Vanderheiden, G. The Principles of Universal Design; Center for Universal Design, NC State University: Raleigh, ND, USA, 1997. [Google Scholar]
- Story, M.F.; Mueller, J.L.; Mace, R.L. The Universal Design File: Designing for People of All Ages and Abilities; Center for Universal Design, NC State University: Raleigh, ND, USA, 1998. [Google Scholar]
- Clarkson, P.J.; Coleman, R. History of inclusive design in the UK. Appl. Ergon. 2015, 46, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Berguer, R.; Hreljac, A. The relationship between hand size and difficulty using surgical instruments: A survey of 726 laparoscopic surgeons. Surg. Endosc. 2004, 18, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Alleblas, C.C.J.; Vleugels, M.P.H.; Nieboer, T.E. Ergonomics of laparoscopic graspers and the importance of haptic feedback: the surgeons’ perspective. Gynecol. Surg. 2016, 13, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoklasek, P.; Mizera, A.; Maňas, M.; Maňas, D. Improvement of handle grip using reverse engineering, CAE and Rapid Prototyping. In Proceedings of the 20th International Conference on Circuits, Systems, Communications and Computers (CSCC 2016), Corfu Island, Greece, 14–17 July 2016. [Google Scholar]
- Sutton, E.; Irvin, M.; Zeigler, C.; Lee, G.; Park, A. The ergonomics of women in surgery. Surg. Endosc. 2013, 28, 1051–1055. [Google Scholar] [CrossRef] [PubMed]
- Groenesteijn, L.; Eikhout, S.M.; Vink, P. One set of pliers for more tasks in installation work: The effects on (dis)comfort and productivity. Appl. Ergon. 2004, 35, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.-K.; Lowe, B.D.; Lee, S.J.; Krieg, E.F. Evaluation of handle design characteristics in a maximum screwdriving torque task. Ergonomics 2007, 50, 1404–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harih, G.; Dolšak, B. Tool-handle design based on a digital human hand model. Int. J. Ind. Ergon. 2013, 43, 288–295. [Google Scholar] [CrossRef]
- Harih, G.; Dolšak, B. Comparison of subjective comfort ratings between anatomically shaped and cylindrical handles. Appl. Ergon. 2014, 45, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Bru, J.L.; Giurintano, D.J.; Pérez-González, A.; Vergara, M. Optimum tool handle diameter for a cylinder grip. J. Hand Ther. 2003, 16, 337–342. [Google Scholar] [CrossRef]
- Kong, Y.K.; Kim, D.M.; Lee, K.-S.; Jung, M.-C. Comparison of comfort, discomfort, and continuum ratings of force levels and hand regions during gripping exertions. Appl. Ergon. 2012, 43, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Berguer, R.; Forkey, D.L.; Smith, W.D. Ergonomic problems associated with laparoscopic surgery. Surg. Endosc. 1999, 13, 466–468. [Google Scholar] [CrossRef] [PubMed]
- DiMartino, A.; Doné, K.; Judkins, T.; Morse, J.; Melander, J. Ergonomic Laparoscopic Tool Handle Design. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, New Orleans, LA, USA, 20–24 September 2004; SAGE Publications: Los Angeles, CA, USA, 2004; pp. 1354–1358. [Google Scholar]
- Trejo, A.; Jung, M.C.; Oleynikov, D.; Hallbeck, M.S. Effect of handle design and target location on insertion and aim with a laparoscopic surgical tool. Appl. Ergon. 2007, 38, 745–753. [Google Scholar] [CrossRef] [PubMed]
- González, A.G.; Salgado, D.R.; García Moruno, L. Optimisation of a laparoscopic tool handle dimension based on ergonomic analysis. Int. J. Ind. Ergon. 2015, 48, 16–24. [Google Scholar] [CrossRef]
- Openshaw, S.; Taylor, E. Ergonomics and Design. Reference Guide; All Steel Inc.: Muscatine, IA, USA, 2006. [Google Scholar]
- Worksafe, Travail Sécuritaire. Office Ergonomics. Guidelines for Preventing Musculoskeletal Injuries; WorkSafeNB: Saint John, NB, Canada, 2010. [Google Scholar]
- Scott, P.; Kogi, K.; McPhee, B. Ergonomics Guidelines for Occupational Health Practice in Industrially Developing Countries; International Ergonomics Association: Darmtstadt, Germany, 2009. [Google Scholar]
- Chapanis, A. Ergonomics in product development: a personal view. Ergonomics 1995, 38, 1625–1638. [Google Scholar] [CrossRef]
- Van Veelen, M.A.; Meijer, D.W.; Uijttewaal, I.; Goossens, R.H.; Snijders, C.J.; Kazemier, G. Improvement of the laparoscopic needle holder based on new ergonomic guidelines. Surg. Endosc. 2003, 17, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Wauben, L.S.; Van Veelen, M.A.; Gossot, D.; Goossens, R.H. Application of ergonomic guidelines during minimally invasive surgery: A questionnaire survey of 284 surgeons. Surg. Endosc. 2006, 20, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Parekh, J.; Shepherd, D.; Hukins, D.; Maffulli, N. Ergonomic T-Handle for Minimally Invasive Surgical Instruments. Transl. Med. UniSa 2016, 14, 38–41. [Google Scholar] [PubMed]
- Berguer, R. The application of ergonomics in the work environment of general surgeons. Rev. Environ. Health 1997, 12, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Berguer, R. Surgery and ergonomics. Arch. Surg. 1999, 134, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Matern, U.; Eichenlaub, M.; Waller, P.; Ruckauer, K. MIS instruments. An experimental comparison of various ergonomic handles and their design. Surg. Endosc. 1999, 13, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Van Veelen, M.A.; Meijer, D.W. Ergonomics and design of laparoscopic instruments: results of a survey among laparoscopic surgeons. J. Laparoendosc. Adv. Surg. Tech. Part B Videoscop. 1999, 9, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Szeto, G.P.; Cheng, S.W.; Poon, J.T.; Ting, A.C.; Tsang, R.C.; Ho, P. Surgeons’ Static Posture and Movement Repetitions in Open and Laparoscopic Surgery. J. Surg. Res. 2011, 172, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Choi, S. A Review of the Ergonomic Issues in the Laparoscopic Operating Room. J. Healthc. Eng. 2012, 3, 587–603. [Google Scholar] [CrossRef]
- Berguer, R.; Chen, J.; Smith, W.D. A comparison of the physical effort required for laparoscopic and open surgical techniques. Arch. Surg. 2003, 138, 967–970. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.D.; Forkey, D.L.; Berguer, R. The Virtual Instrumentation (VI) laboratory facilitates customized on- site ergonomic analysis of minimally invasive surgery. Stud. Health Technol. Inform. 1998, 50, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Hemal, A.K.; Srinivas, M.; Charles, A.R. Ergonomic problems associated with laparoscopy. J. Endourol. 2001, 15, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Quick, N.E.; Gillette, J.C.; Shapiro, R.; Adrales, G.L.; Gerlach, D.; Park, A.E. The effect of using laparoscopic instruments on muscle activation patterns during minimally invasive surgical training procedures. Surg. Endosc. 2003, 17, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Trejo, A.; Doné, K.N.; DiMartino, A.; Oleynikov, D.; Hallbeck, M.S. Articulating vs. conventional laparoscopic grasping tools-surgeons’ opinions. Int. J. Ind. Ergon. 2006, 36, 25–35. [Google Scholar] [CrossRef]
- Park, A.; Lee, G.; Seagull, F.J.; Meenaghan, N.; Dexter, D. Patients benefit while surgeons suffer: An impending epidemic. J. Am. Coll. Surg. 2010, 210, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Ergolap Project. Obtaining Criteria for Ergonomic Design of Laparoscopic Surgery Instruments; National Project of the Spanish Gov.; Ref.: DPI2007-65902-C03-03; Ministry of Science and Innovation: Madrid, Spain, 2008–2010.
- Kong, Y.-K.; Lowe, B.D. Optimal cylindrical handle diameter for grip force tasks. Int. J. Ind. Ergon. 2005, 35, 495–507. [Google Scholar] [CrossRef]
- Kong, Y.-K.; Lowe, B.D. Evaluation of handle diameters and orientations in a maximum torque task. Int. J. Ind. Ergon. 2005, 35, 1073–1084. [Google Scholar] [CrossRef]
- Sekulova, K.; Buresa, M.; Kurkinb, O.; Simona, M. Ergonomic Analysis of a Firearm According to the Anthropometric Dimension. Procedia Eng. 2015, 100, 609–616. [Google Scholar] [CrossRef]
- Hsiao, S.W.; Chuang, J.C. A reverse engineering based approach for product form design. Des. Stud. 2003, 24, 155–171. [Google Scholar] [CrossRef]
- Zanetti, E.M.; Aldieri, A.; Terzini, M.; Calì, M.; Franceschini, G.; Bignardi, C. Additively manufactured custom loadbearing implantable devices: grounds for caution. Australas. Med. J. 2017, 10, 694. [Google Scholar] [CrossRef]
- Sass, L.; Oxman, R. Materializing design: the implications of rapid prototyping in digital design. Des. Stud. 2005, 27, 325–355. [Google Scholar] [CrossRef]
- Greiner, T.M. Hand Anthropometry of U.S. Army Personnel; Technical Report NATICK/TR-92/011; United States Army Natick Research, Development and Engineering Center: Natick, MA, USA, 1991. [Google Scholar]
- Irwin, C.B.; Radwin, R.G. A new method for estimating hand internal loads from external force measurements. Ergonomics 2008, 51, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-S.; Jung, M.-C. Ergonomic Evaluation of Biomechanical Hand Function. Saf. Health Work 2015, 6, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Radwin, R. Pistol Grip Power Tool Handle and Trigger Size Effects on Grip Exertions and Operator Preference. Hum. Factors 1993, 35, 551–569. [Google Scholar] [CrossRef] [PubMed]
- Matern, U.; Waller, P. Instruments for minimally invasive surgery: principles of ergonomic handles. Surg. Endosc. 1999, 13, 174–182. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean (SD) | Range |
|---|---|---|
| Age (years) | 39.7 (9.78) | 20–70 |
| Hand length (mm) | 178.9 (13.08) | 159.3–194.4 |
| Palm length measured (mm) | 96.5 (8.79) | 87.6–111.6 |
| Hand breadth digitized (mm) | 79.9 (6,98) | 71.1–86.5 |
| Hand Size | % | Sex | Mean Diameter (mm) |
|---|---|---|---|
| XS | 26% | Both sexes | 29.4 |
| S | 11.1% | M | 32.9 |
| 18.5% | F | 31.7 | |
| M | 24.4% | M | 36.4 |
| 6.7% | F | 33.1 | |
| L | 13.3% | Both sexes | 37.9 |
| Parameter (mm) | Parametric Ratio |
|---|---|
| DM | 1 |
| DI | 0.80 |
| DS | 1.15 |
| R1 | 1.25 |
| R2 | 4.48 |
| HSC | Sex | Hand Length from Digitizer (HLD) | Palm Length Measured (PLM) | Hand Breadth from Digitizer (HBD) | Ø Optimum Diameter of handle DM | Anthropometric Relationship Factor | ||
|---|---|---|---|---|---|---|---|---|
| Units in mm | ||||||||
 |  |  |  |  |  | |||
| XS | Both sexes | 159.3 | 87.6 | 71.1 | 29.4 | 5.418 | 2.980 | 2.418 |
| S | Male | 174.1 | 97.6 | 79.1 | 32.9 | 5.292 | 2.967 | 2.404 |
| Female | 170.2 | 94.3 | 72.5 | 31.7 | 5.369 | 2.975 | 2.287 | |
| M | Male | 188.8 | 107.8 | 86.5 | 36.4 | 5.187 | 2.962 | 2.376 |
| Female | 182.1 | 98.2 | 78.9 | 33.1 | 5.502 | 2.967 | 2.384 | |
| L | Both sexes | 194.9 | 111.6 | 86.5 | 37.9 | 5.142 | 2.945 | 2.282 |
| 5.308 | 2.967 | 2.362 | ||||||
| 0.1173040 | 0.0113021 | 0.0549504 | ||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González, A.G.; Salgado, D.R.; García Moruno, L.; Sánchez Ríos, A. An Ergonomic Customized-Tool Handle Design for Precision Tools using Additive Manufacturing: A Case Study. Appl. Sci. 2018, 8, 1200. https://doi.org/10.3390/app8071200
González AG, Salgado DR, García Moruno L, Sánchez Ríos A. An Ergonomic Customized-Tool Handle Design for Precision Tools using Additive Manufacturing: A Case Study. Applied Sciences. 2018; 8(7):1200. https://doi.org/10.3390/app8071200
Chicago/Turabian StyleGonzález, Alfonso González, David Rodríguez Salgado, Lorenzo García Moruno, and Alonso Sánchez Ríos. 2018. "An Ergonomic Customized-Tool Handle Design for Precision Tools using Additive Manufacturing: A Case Study" Applied Sciences 8, no. 7: 1200. https://doi.org/10.3390/app8071200