1. Background
Vehicular accidents and falls are the primary causes of spinal cord injuries (SCI), which are often accompanied by a second injury. Within the SCIs, falls among the elderly are increasing with the aging population [
1]. One of the most frequent complications of SCI are urinary tract infections (UTIs). Among SCI patients, 80% suffer from bladder dysfunction, out of which, 36% or more will have to be hospitalized because of complications [
2,
3]. Having lost the sensation of bladder filling, patients could not determine when and how to start urination autonomously. Consequently, indwelling catheters (IC) or CIC becomes an option to empty the bladder. Nevertheless, IC can cause bladder atrophy due to long-term poor contraction. Filth accumulated in the folds of the bladder wall can also lead to cystitis, bladder stones, smaller capacities, low-compliance bladder, low blood flow to the bladder wall, infections, and high mortality [
4,
5,
6]. The odor and unpleasant appearance of urinal collection bags also arouse the feelings of inferiority and isolation.
If the bladder of a CIC patient is overdistended before the catheterization is performed again, there would be an over-expansion of the bladder wall and the intravesical pressure would rise rapidly, resulting in a low bladder blood flow, a low-compliance bladder, and a dangerous situation for the patient. If the bladder holds more than 300 mL of urine, it will increase infection rate 4–5 times [
7,
8]. As a consequence of negligence and misjudgment of clinical infections, treatment delay is very likely to happen and thus increase hospitalization days and costs [
9]. CIC performed with voiding diary helps restore and retain the function and compliance of the bladder, as well as release the intravesical pressure and increase the blood flow of the bladder wall, enabling the bladder to perform antibacterial activities and lessen the chance of complications [
10,
11,
12,
13,
14,
15,
16,
17]. Voiding diary is a simple and primary tool used to understand urinary tract function and assess urinary symptoms, with a view to providing doctors with sufficient data for an appropriate clinical diagnosis. However, diary record with pen and paper is time-consuming and it may cause frequent omissions and increase the patients’ burden [
18,
19,
20,
21]. Furthermore, SCI patients need social support to overcome depression and neurosis derived from fear and self-imposed pressure after a sudden injury [
22,
23].
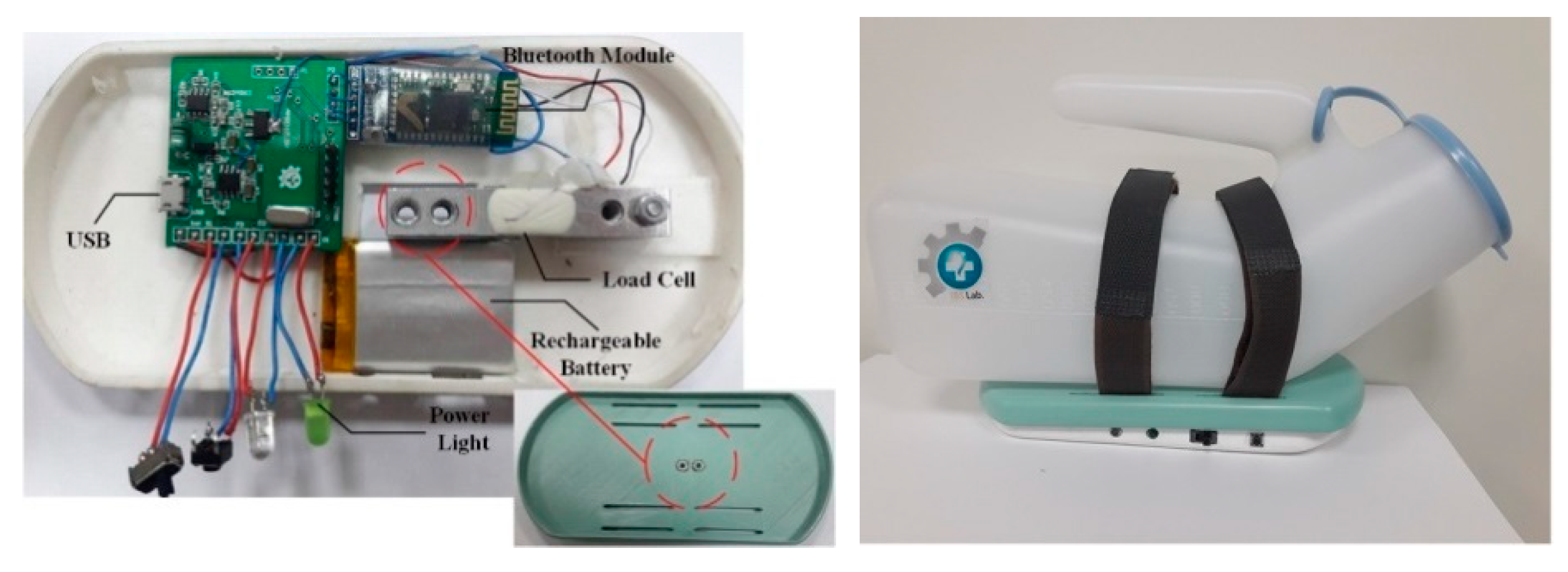
The purpose of this study is to develop a personalized assistant system for CIC patients with NBD. This system, combined with the accessible lavatory function, can automatically record individual urine voiding volume, compute bladder health status, and give feedback, so as to keep the patients from holding urine as much as possible.
3. Results
There were 12 patients, with CIC bladder management strategy, recruited as the subjects of the research under the specification of the Institutional Review Board (IRB): 10510-003 of Chi Mei Medical Center.
Table 3 is recognized as an overview of their demographic and clinical features. The age of patients ranged from 21 to 51 years old with an average of 39.25 years old. The recruited patients were interpreted by clinicians and their cytometric capacity, intravesical pressure and compliance were in the normal range, and their bladder pressure was highly correlated with the volume [
4,
24,
32]. Level of injury primarily fell on C (58.4%) and T (33.3%). The majority of these patients chose to conduct CIC indoors (91.7%) and 33.3% of them kept a record of each voided volume, while 66.7% were in fear of excess voided volume. This study observed that only 25% of the patients returned for OPD follow-up after one year or more.
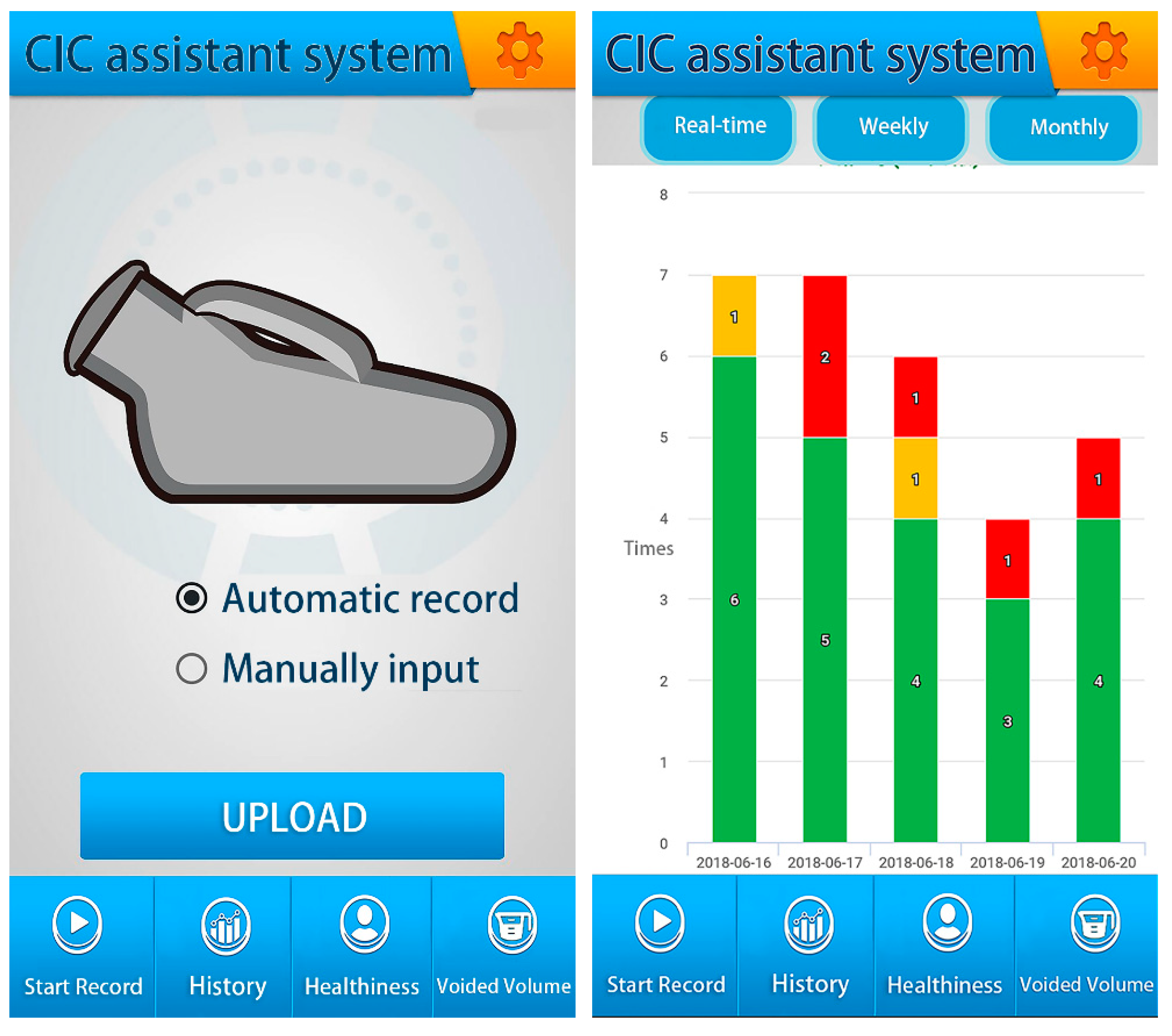
CIC assistant system automatically records and uploads the precise amount of catheterization and statistics, as shown in
Figure 5.
Figure 6 shows the regressive curve of urine volume measurement between CIC assistant device and graduated cylinder, its R-square was 0.99. Records are displayed on the app on the client’s screen. After collection and calculation, the feedback system reminds patients to modify their lifestyles or to return to the hospital for further inspection in order to reduce UTIs and other complications. Furthermore, the accessible lavatory function shows the shortest route to the most suitable lavatory after patients enter their requirements. This saves considerable time for patients when searching for a toilet.
Table 4 represents the frequency in a month for voided urine volume >550 mL of 12 patients with CIC strategy. Fewer SCI patients with bladder sensations encountered even more problems of excess voided volume in comparison with those without bladder sensations.
Figure 7 shows how the accessible lavatory function in the app provided information regarding all the nearby accessible lavatories with a filter function. Patients could also add a new lavatory on our cloud system after verification. The results of patients looking for a lavatory in an unfamiliar environment with this function were shown by the following data: unfamiliar 43.1%, semi-familiar 27.2%, and familiar 17.6%. The time spent searching for a lavatory independently was 22.5 min, 15.8 min, and 13.6 min respectively. By using the accessible lavatory function, the arrival time decreased to 12.8 min, 11.5 min, and 11.2 min respectively (
Table 5). SCI patients with CIC were inclined to perform CIC at home, or at least indoors, because of the inconvenience of searching for an accessible lavatory in an open area (
Table 3). A reduced motivation for going out could lead to social detachment, psychological disorders, and an unpleasant lifestyle [
19].
Table 6 indicates the improvement of patient intention, from 25% to 75%, through the aid of the accessible lavatory function. It is beneficial in expanding the patient’s social contact while at the same time promoting the maintenance of a healthy state of mind.
4. Discussions and Conclusion
The research developed a CIC assistant system of intermittent catheterization for neurogenic bladder dysfunction patients to record their voided volume and make suggestions. The patients with CIC bladder management strategy were recruited. The cytometric capacity, intravesical pressure, and bladder compliance of these patients were in the normal range (>40 mL/cm H
2O), and the bladder pressure of these patients was highly correlated with the urine volume [
4,
32]. A wireless urine pot measuring device is ideal for such patients to keep a record, both indoors and outdoors. By looking at the stored data, patients understand more about the history of their catheterization volume and time period. At the same time, doctors can monitor and diagnose patients despite the distance. However, the system is not suitable for the patients with abnormal bladder function, such as abnormal bladder wall compliance caused by bladder fibrosis.
By way of face-to-face discussion by clinicians under IRB’s ethical principles, the patients recruited in this study agreed that the system could effectively help them keep a record and make observations automatically. This was helpful in the bladder and urinary system care and meant the occurrence of UTIs could be decreased. The accessible lavatory function helped patients efficiently find a suitably accessible lavatory. By reducing the instance of holding urine, patients became more prepared for better social interactions. Based on the comments and scores given by experienced users, patients felt at ease to explore a new place without any psychological barrier.
A limitation of our system is that it is unable to detect the current volume of the bladder and give a catheter reminder, so the user is still troubled by drinking water, and must rely on time as the basis for catheterization. Besides this, the accessible lavatory function [
29] can only be searched for its location and route navigation. A solution would be to combine a bladder monitor device and IoT device in this system. In the future, the proposed system will integrate a wearable device, capable of bladder volume estimation non-invasively, with a reminder function. Accessible lavatory navigator function with IoT device can calculate the state and the frequency of the toilet. Therefore, it can detect toilet crowdedness and prevent patients from holding urine for a long time. It is hoped that this system could improve the quality of life of patients and reduce the chance of UTIs. Equipping SCI patients with the above system enhances their sense of happiness and encourages them to enjoy outdoor-living by contacting the crowd.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}