
A Comparison of Depression and Anxiety among University Students in Nine Countries during the COVID-19 Pandemic

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Country Differences in Depression and Anxiety
3.2. Association of Depression and Anxiety with Other Variables
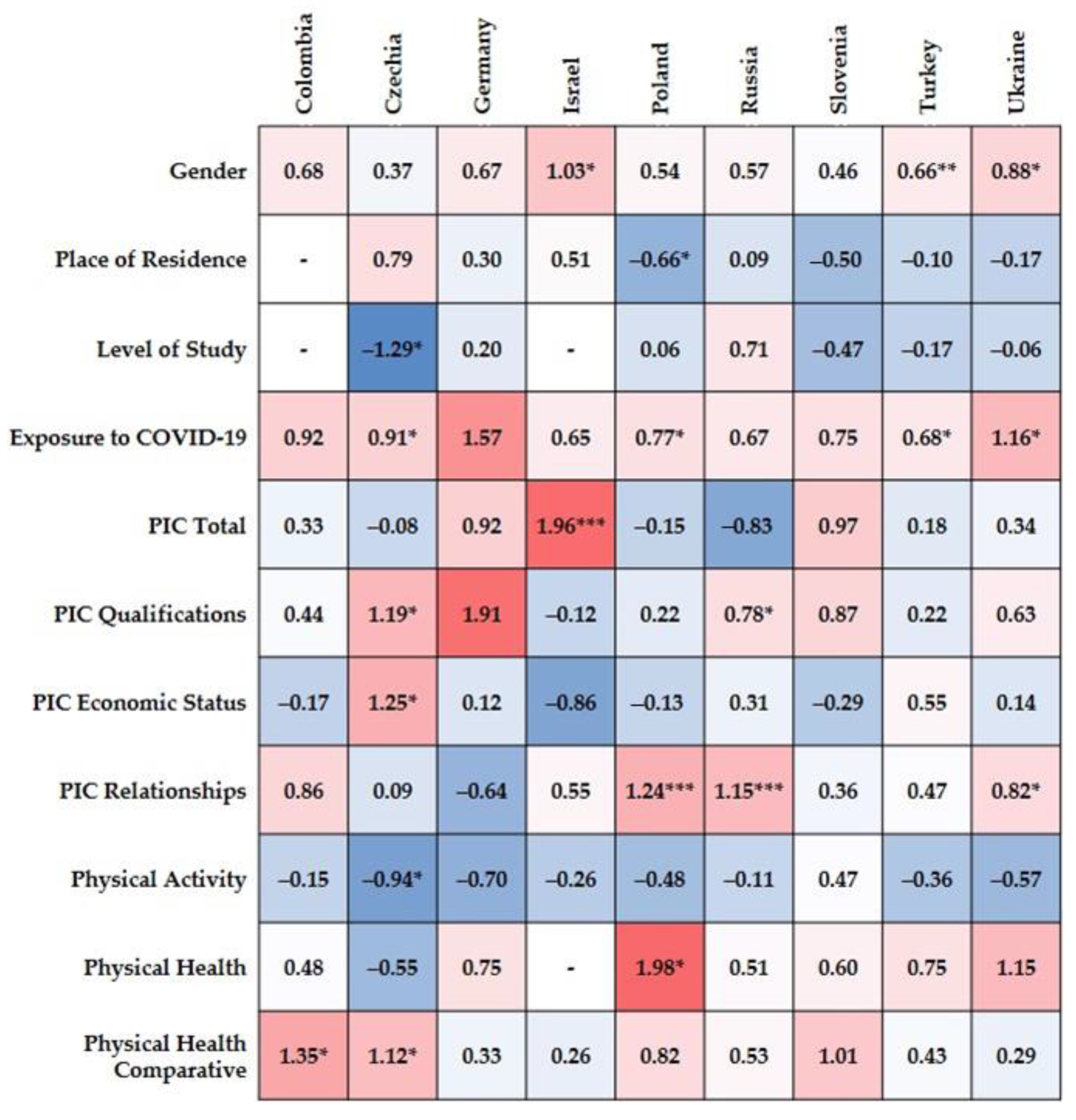
3.3. Predictors of Depression in the Nine Countries
3.4. Predictors of Anxiety in the Nine Countries
4. Discussion
4.1. Anxiety and Depression across the Nine Countries
4.2. Association of Depression and Anxiety Risk with Other Variables
4.3. Predictors of Depression and Anxiety in the Nine Countries
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baloch, S.; Baloch, M.A.; Zheng, T.; Pei, X. The coronavirus disease 2019 (COVID-19) pandemic. Tohoku J. Exp. Med. 2020, 250, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 15 March 2021).
- Rajkumar, R.P. Covid-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Lei, S.M.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional influence of the covid-19 pandemic lockdowns on health behaviors and quality of life among Chinese adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of Covid-19 epidemic declaration on psychological consequences: A study on active weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Troyer, E.A.; Kohn, J.N.; Hong, S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav. Immun. 2020, 87, 34–39. [Google Scholar] [CrossRef]
- World Bank. Global Economic Prospects, June 2020; World Bank: Washington, DC, USA, 2020. [Google Scholar] [CrossRef]
- Bartoll, X.; Palència, L.; Malmusi, D.; Suhrcke, M.; Borrell, C. The evolution of mental health in Spain during the economic crisis. Eur. J. Public Health. 2014, 24, 415–418. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.R.; Yu, Y.; Jackson, J.S.; Anderson, N.B. Racial differences in physical and mental health: Socio-economic status, stress and discrimination. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [Green Version]
- Murali, V.; Oyebode, F. Poverty, social inequality and mental health. Adv. Psychiatr. Treat. 2004, 10, 216–224. [Google Scholar] [CrossRef]
- Bonsaksen, T.; Leung, J.; Schoultz, M.; Thygesen, H.; Price, D.; Ruffolo, M.; Geirdal, A.Ø. Cross-national study of worrying, loneliness, and mental health during the COVID-19 pandemic: A comparison between individuals with and without infection in the family. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Fried, E.I.; Papanikolaou, F.; Epskamp, S. Mental Health and Social Contact during the COVID-19 Pandemic: An Ecological Momentary Assessment Study. 2020. Available online: psyarxiv.com/36xkp/ (accessed on 15 March 2021).
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the covid-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The effect of covid-19 on youth mental health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef]
- Vieira, C.M.; Franco, O.H.; Restrepo, C.G.; Abel, T. COVID-19: The forgotten priorities of the pandemic. Maturitas 2020, 136, 38–41. [Google Scholar] [CrossRef]
- Schubert, K.O.; Clark, S.R.; Van, L.K.; Collinson, J.L.; Baune, B.T. Depressive symptom trajectories in late adolescence and early adulthood: A systematic review. Aust. N. Z. J. Psychiatry 2017, 51, 477–499. [Google Scholar] [CrossRef]
- Zivin, K.; Eisenberg, D.; Gollust, S.E.; Golberstein, E. Persistence of mental health problems and needs in a college student population. J. Affect. Disord. 2009, 117, 180–185. [Google Scholar] [CrossRef]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 2013, 47, 391–400. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Evans, J.; Patterson, J.; Petersen, S.; Doll, H.; Balding, J.; Regis, D. The health of students in institutes of higher education: An important and neglected public health problem? J. Public Health Med. 2000, 22, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Vaez, M.; Ponce de Leon, A.; Laflamme, L. Health-related determinants of perceived quality of life: A comparison between first-year university students and their working peers. Work 2006, 26, 167–177. [Google Scholar]
- Andrews, B.; Wilding, J.M. The relation of depression and anxiety to life-stress and achievement in students. Br. J. Psychol. 2004, 95, 509–521. [Google Scholar] [CrossRef]
- Wege, N.; Muth, T.; Li, J.; Angerer, P. Mental health among currently enrolled medical students in Germany. Public Health 2016, 132, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Elani, H.W.; Allison, P.J.; Kumar, R.A.; Mancini, L.; Lambrou, A.; Bedos, C. A systematic review of stress in dental students. J. Dent. Educ. 2014, 78, 226–242. [Google Scholar] [CrossRef] [PubMed]
- Cook, A.F.; Arora, V.M.; Rasinski, K.A.; Curlin, F.A.; Yoon, J.D. The prevalence of medical student mistreatment and its association with burnout. Acad. Med. J. Assoc. Am. Med. Coll. 2014, 89, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Borst, J.M.; Frings-Dresen, M.H.W.; Sluiter, J.K. Prevalence and incidence of mental health problems among Dutch medical students and the study related and personal risk factors: A longitudinal study. Int. J. Adolesc. Med. Health 2016, 28, 349–355. [Google Scholar] [CrossRef]
- El-Gendawy, S.; Hadhood, M.; Shams, R.; Ibrahim, A. Epidemiological aspects of depression among Assiut University students. Assiut Med. J. 2005, 2, 81–89. [Google Scholar]
- Aristovnik, A.; Keržič, D.; Ravšelj, D.; Tomaževič, N.; Umek, L. Impacts of the COVID-19 Pandemic on Life of Higher Education Students: A Global Perspective. Sustainability 2020, 12, 8438. [Google Scholar] [CrossRef]
- Gloster, A.T.; Lamnisos, D.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; et al. Impact of COVID-19 pandemic on mental health: An international study. PLoS ONE 2020, 15, e0244809. [Google Scholar] [CrossRef]
- Adamson, M.M.; Phillips, A.; Seenivasan, S.; Martinez, J.; Grewal, H.; Kang, X.; Coetzee, J.; Luttenbacher, I.; Jester, A.; Harris, O.A.; et al. International Prevalence and Correlates of Psychological Stress during the Global COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9248. [Google Scholar] [CrossRef]
- Kavčič, T.; Avsec, A.; Kocjan, G.Z. Psychological Functioning of Slovene Adults during the COVID-19 Pandemic: Does Resilience Matter? Psychiatr. Q. 2020, 92, 207–216. [Google Scholar] [CrossRef]
- Lee, S. Subjective well-being and mental health during the pandemic outbreak: Exploring the role of institutional trust. Res. Aging 2020, 25, 164027520975145. [Google Scholar] [CrossRef]
- Tušl, M.; Brauchli, R.; Kerksieck, P.; Bauer, G.F. Impact of the COVID-19 crisis on work and private life, mental well-being and self-rated health in German and Swiss employees: A cross-sectional online survey. BMC Public Health 2021, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Almarzooq, Z.I.; Lopes, M.; Kochar, A. Virtual Learning during the COVID-19 Pandemic: A Disruptive Technology in Graduate Medical Education. J. Am. Coll. Cardiol. 2020, 75, 2635–2638. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, K.; Vishwakarma, D.K.; Singh, N. COVID-19 and its impact on education, social life and mental health of students: A survey. Child. Youth Serv. Rev. 2021, 121, 105866. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization. COVID-19 and the Education Sector. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/briefingnote/wcms_742025.pdf (accessed on 11 June 2021).
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental health problems during the COVID-19 pandemics and the mitigation effects of exercise: A longitudinal study of college students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Pavlova, I.; Kuśnierz, C.; Ochnik, D.; Bodnar, I.; Petrytsa, P. Does Physical Activity Matter for the Mental Health of University Students during the COVID-19 Pandemic? J. Clin. Med. 2020, 9, 3494. [Google Scholar] [CrossRef]
- Aslan, I.; Ochnik, D.; Çınar, O. Exploring Perceived Stress among Students in Turkey during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8961. [Google Scholar] [CrossRef]
- Juchnowicz, D.; Baj, J.; Forma, A.; Karakuła, K.; Sitarz, E.; Bogucki, J.; Karakula-Juchnowicz, H. The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown. J. Clin. Med. 2021, 10, 944. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the covid-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Islam, M.S.; Ferdous, M.Z.; Potenza, M.N. Panic and generalized anxiety during the covid-19 pandemic among Bangladeshi people: An online pilot survey early in the outbreak. J. Affect. Disord. 2020, 276, 30–37. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Schiff, M.; Zasiekina, L.; Pat-Horenczyk, R.; Benbenishty, R. COVID-Related Functional Difficulties and Concerns Among University Students during COVID-19 Pandemic: A Binational Perspective. J. Community Health 2020. [Google Scholar] [CrossRef]
- Kecojevic, A.; Basch, C.H.; Sullivan, M.; Davi, N.K. The impact of the COVID-19 epidemic on mental health of undergraduate students in New Jersey, cross-sectional study. PLoS ONE 2020, 15, e0239696. [Google Scholar] [CrossRef]
- Vigo, D.; Jones, L.; Munthali, R.; Pei, J.; Westenberg, J.; Munro, L.; Judkowicz, C.; Wang, A.Y.; Adel, B.V.D.; Dulai, J.; et al. Investigating the effect of COVID-19 dissemination on symptoms of anxiety and depression among university students. BJPsych Open 2021, 7, E69. [Google Scholar] [CrossRef]
- Cindrich, S.L.; Lansing, J.E.; Brower, C.S.; McDowell, C.P.; Herring, M.P.; Meyer, J.D. Associations Between Change in Outside Time Pre- and Post-COVID-19 Public Health Restrictions and Mental Health: Brief Research Report. Front. Public Health 2021, 9, 619129. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Coelho, C.M.; Suttiwan, P.; Arato, N.; Zsido, A.N. On the nature of fear and anxiety triggered by COVID-19. Front. Psychol. 2020, 11, 3109. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in march 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef]
- Maalouf, F.T.; Mdawar, B.; Meho, L.I.; Akl, E.A. Mental health research in response to the COVID-19, Ebola, and H1N1 outbreaks: A comparative bibliometric analysis. J. Psychiatr. Res. 2021, 132, 198–206. [Google Scholar] [CrossRef]
- Mækelæ, M.J.; Reggev, N.; Dutra, N.; Tamayo, R.M.; Silva-Sobrinho, R.A.; Klevjer, K.; Pfuhl, G. Perceived efficacy of COVID-19 restrictions, reactions and their impact on mental health during the early phase of the outbreak in six countries. R. Soc. Open Sci. 2020, 7, 200644. [Google Scholar] [CrossRef]
- Margraf, J.; Brailovskaia, J.; Schneider, S. Behavioral measures to fight COVID-19: An 8-country study of perceived usefulness, adherence and their predictors. PLoS ONE 2020, 15, e0243523. [Google Scholar] [CrossRef]
- Brailovskaia, J.; Cosci, F.; Mansueto, G.; Miragall, M.; Herrero, R.; Baños, R.M.; Krasavtseva, Y.; Kochetkov, Y.; Margraf, J. The association between depression symptoms, psychological burden caused by Covid-19 and physical activity: An investigation in Germany, Italy, Russia, and Spain. Psychiatry Res. 2021, 295, 113596. [Google Scholar] [CrossRef] [PubMed]
- Ruffolo, M.; Price, D.; Schoultz, M.; Leung, J.; Bonsaksen, T.; Thygesen, H.; Geirdal, A.Ø. Employment Uncertainty and Mental Health during the COVID-19 Pandemic Initial Social Distancing Implementation: A Cross-national Study. Glob. Soc. Welf. 2021, 8, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chudzicka-Czupała, A.; Tee, M.L.; Núñez, M.I.L.; Tripp, C.; Fardin, M.A.; Habib, H.A.; Tran, B.X.; Adamus, K.; Anlacan, J.; et al. A chain mediation model on COVID-19 symptoms and mental health outcomes in Americans, Asians and Europeans. Sci. Rep. 2021, 11, 6481. [Google Scholar] [CrossRef]
- Yehudai, M.; Bender, S.; Gritsenko, V.; Konstantinov, V.; Reznik, A.; Isralowitz, R. COVID-19 fear, mental health, and substance misuse conditions among university social work students in Israel and Russia. Int. J. Ment. Health Addict. 2020, 6, 1–8. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Yehudai, M.; Bender, S.; Shilina, I.; Isralowitz, R. First and Second Wave COVID-19 Fear Impact: Israeli and Russian Social Work Student Fear, Mental Health and Substance Use. Int. J. Ment. Health Addict. 2021, 1–8. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Leiner, D.J. SoSci Survey (Version 3.1. 06) [Computer Software]. 2019. Available online: https://www.soscisurvey.de/ (accessed on 1 April 2020).
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B.A. Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Arlington, VA, USA, 2013. [Google Scholar]
- WHO. Be Active during COVID-19. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/be-active-during-covid-19 (accessed on 15 March 2021).
- DeSalvo, K.B.; Fan, V.S.; McDonell, M.B.; Fihn, S.D. Predicting mortality and healthcare utilization with a single question. Health Serv. Res. 2005, 40, 1234–1246. [Google Scholar] [CrossRef] [Green Version]
- DeSalvo, K.B.; Fisher, W.P.; Tran, K.; Bloser, N.; Merrill, W.; Peabody, J. Assessing measurement properties of two single-item general health measures. Qual. Life Res. 2006, 15, 191–201. [Google Scholar] [CrossRef]
- Statistica. DELL Statistica (Version, 13.1) [Software for Windows]; StatSoft Polska Sp.z o.o.: Krakow, Poland, 2019. [Google Scholar]
- JASP. Team JASP (Version 0.14.1) [Computer Software]. 2020. Available online: https://jasp-stats.org/ (accessed on 15 March 2021).
- Van de Velde, S.; Bracke, P.; Levecque, K. Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc. Sci. Med. 2010, 71, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.M.; Mak, K.-K.; Chua, A.N.C.; Ho, C.S.H.; Mak, A. The effect of severity of depressive disorder on economic burden in a university hospital in Singapore. Expert Rev. Pharmacoecon. Outcomes Res. 2013, 13, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Human Development and the Antropocene. Human Development Report 2020. The Next Frontier. Available online: http://hdr.undp.org/sites/default/files/hdr2020.pdf (accessed on 15 March 2021).
- Erdin, C.; Ozkaya, G. Contribution of small and medium enterprises to economic development and quality of life in Turkey. Heliyon 2020, 6, e03215. [Google Scholar] [CrossRef] [PubMed]
- TUİK. Labor Statistics. 2020. Available online: https://data.tuik.gov.tr/ (accessed on 15 March 2021).
- TUİK. Consumer Price Index. 2021. Available online: https://data.tuik.gov.tr/ (accessed on 15 March 2021).
- Standard & Poor’s Global Ratings. Guide to Credit Rating Essentials: What Are Credit Ratings and How Do They Work? Available online: www.spglobal.com (accessed on 15 March 2021).
- Yan, J.H.; McCullagh, P. Cultural influence on youth’s motivation of participation in physical activity. J. Sport Behav. 2004, 27, 378–390. [Google Scholar]
- Judd, F.K.; Jackson, H.J.; Komiti, A.; Murray, G.; Hodgins, G.; Fraser, C. High prevalence disorders in urban and rural communities. Aust. N. Z. J. Psychiatry 2002, 36, 104–113. [Google Scholar] [CrossRef]
- Kim, H.J.; Park, E.; Storr, C.L.; Tran, K.; Juon, H.S. Depression among Asian-American Adults in the Community: Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0127760. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.G.; Shidhaye, R.; Charlson, F.; Deng, F.; Lyngdoh, T.; Chen, S.; Nanda, S.; Lacroix, K.; Baxter, A.; Whiteford, H. Social correlates of mental, neurological, and substance use disorders in China and India: A review. Lancet Psychiatry 2016, 3, 882–899. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef]
- Human Development Report 2020—Table 5: Gender Inequality Index. United Nations Development Programme. Available online: http://hdr.undp.org/en/content/table-5-gender-inequality-index-gii (accessed on 15 March 2021).
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef]
- Rosenfield, S.; Mouzon, D. Gender and Mental Health. In Handbook of the Sociology and Mental Health; Aneshensel, C.S., Phelan, J.C., Bierman, A., Eds.; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar]
- Kerč, P.; Krohne, N.; Šraj Lebar, T.; Štirn, M. Izsledki Raziskave za Oceno Potreb po Psihosocialni Podpori med Epidemijo Covida-19 [Results of a Study to Assess the Need for Psychosocial Support during the Covid-19 Epidemic]. Slovenian Psychologists’ Association. Available online: http://www.dps.si/wp-content/uploads/2021/03/Izsledki-raziskave-za-oceno-potreb.pdf (accessed on 19 April 2021).
- Levkovich, I. The Impact of Age on Negative Emotional Reactions, Compliance with Health Guidelines, and Knowledge About the Virus during the COVID-19 Epidemic: A Longitudinal Study from Israel. J. Prim. Care Community Health 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Rush, A.J.; Hiser, W.; Giles, D.E. A comparison of self-reported versus clinician-related symptoms in depression. J. Clin. Psychiatry 1987, 48, 246–248. [Google Scholar]
- Enns, M.W.; Larsen, D.K.; Cox, B.J. Discrepancies between self and observer ratings of depression—The relationship to demographic, clinical and personality variables. J. Affect. Disord. 2000, 60, 33–41. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, J.; Ma, Z.; McReynolds, L.S.; Lin, D.; Chen, Z.; Wang, T.; Wang, D.; Zhang, Y.; Zhang, J.; et al. Mental Health among College Students during the COVID-19 Pandemic in China: A 2-Wave Longitudinal Survey. J. Affect. Disord. 2021, 281, 597–604. [Google Scholar] [CrossRef]
- Debowska, A.; Horeczy, B.; Boduszek, D.; Dolinski, D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol. Med. 2020, 1–4. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Kuśnierz, C.; Ochnik, D.; Schütz, A.; Kafetsios, K.; Aslan, I.; Pavlova, I.; Benatov, J.; Arzenšek, A.; Jakubiak, M.; et al. Wellbeing of Undergraduates during the COVID-19 Pandemic: International Study; OSF: Charlottesville, VA, USA, 2020; Available online: https://osf.io/q5f4e (accessed on 15 March 2021). [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. A Comparison of Depression and Anxiety among University Students in Nine Countries during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 2882. https://doi.org/10.3390/jcm10132882
Ochnik D, Rogowska AM, Kuśnierz C, Jakubiak M, Schütz A, Held MJ, Arzenšek A, Benatov J, Berger R, Korchagina EV, et al. A Comparison of Depression and Anxiety among University Students in Nine Countries during the COVID-19 Pandemic. Journal of Clinical Medicine. 2021; 10(13):2882. https://doi.org/10.3390/jcm10132882
Chicago/Turabian StyleOchnik, Dominika, Aleksandra M. Rogowska, Cezary Kuśnierz, Monika Jakubiak, Astrid Schütz, Marco J. Held, Ana Arzenšek, Joy Benatov, Rony Berger, Elena V. Korchagina, and et al. 2021. "A Comparison of Depression and Anxiety among University Students in Nine Countries during the COVID-19 Pandemic" Journal of Clinical Medicine 10, no. 13: 2882. https://doi.org/10.3390/jcm10132882