Improvement of Overall Survival Using TKIs as Salvage Therapy in Advanced Thyroid Carcinoma: Real-Life Data on a Single Center Experience


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessments and Definitions
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. TKIs Treatment in the Entire Population
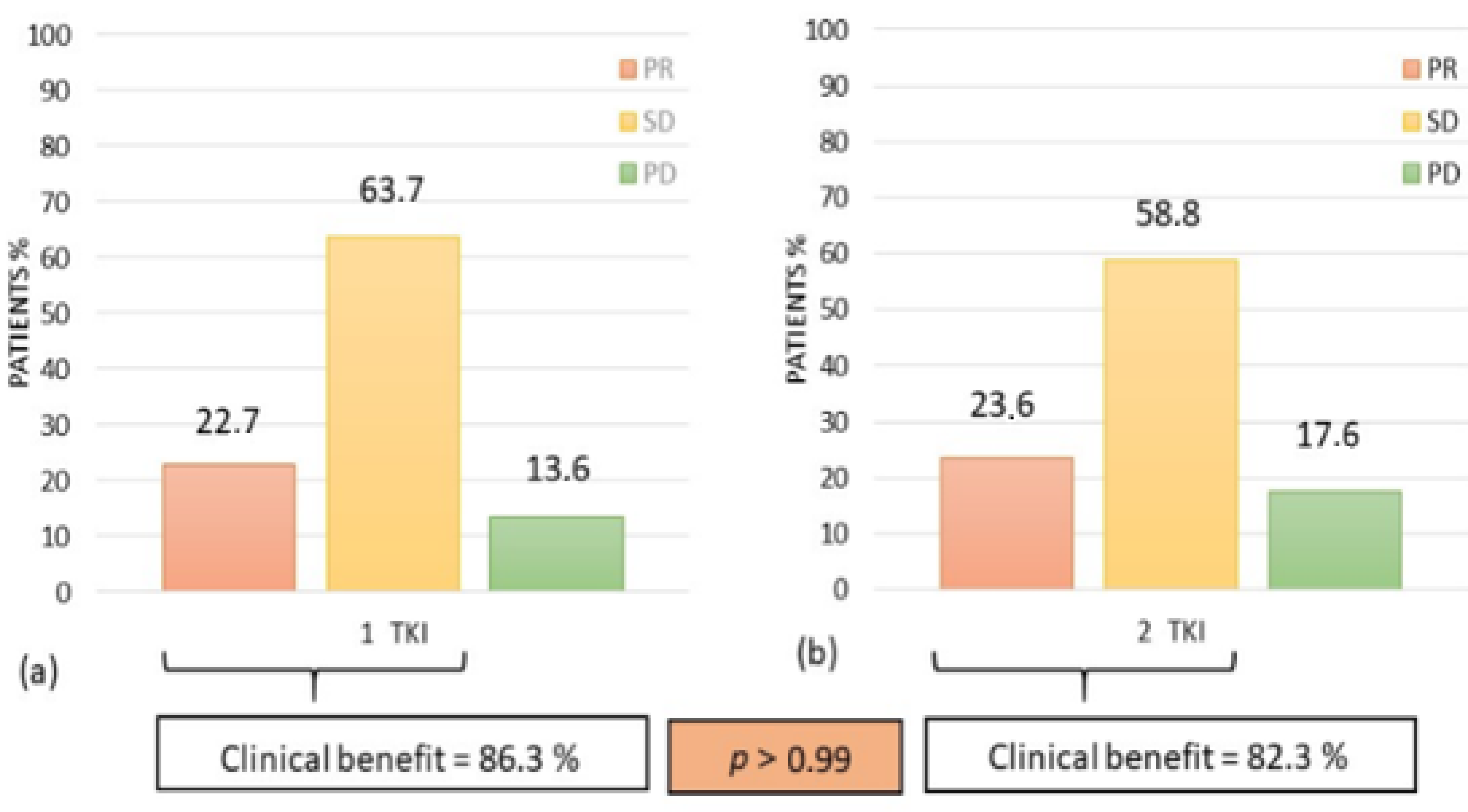
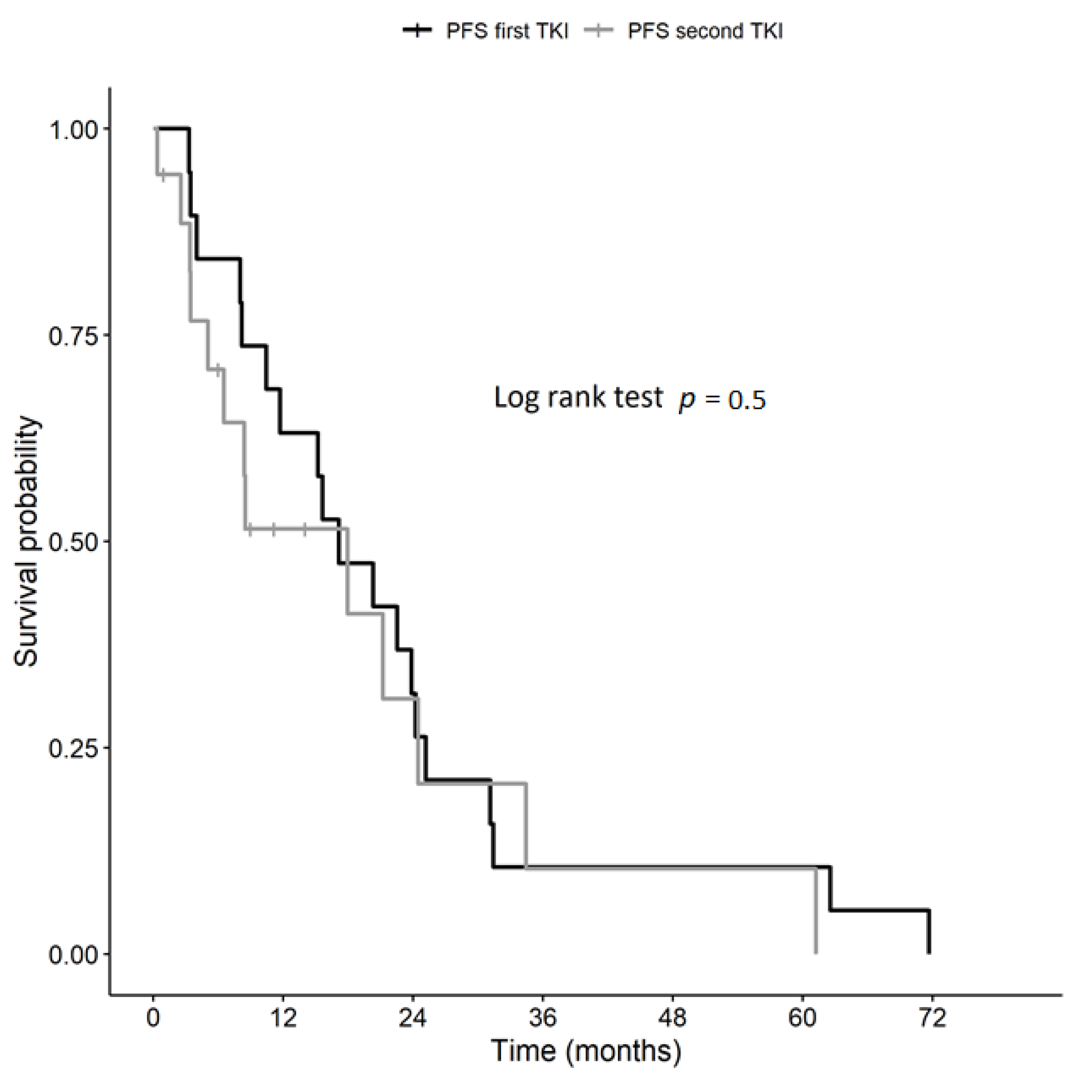
3.3. Efficacy Analysis of TKIs Treatment in the Study Group (n = 23)
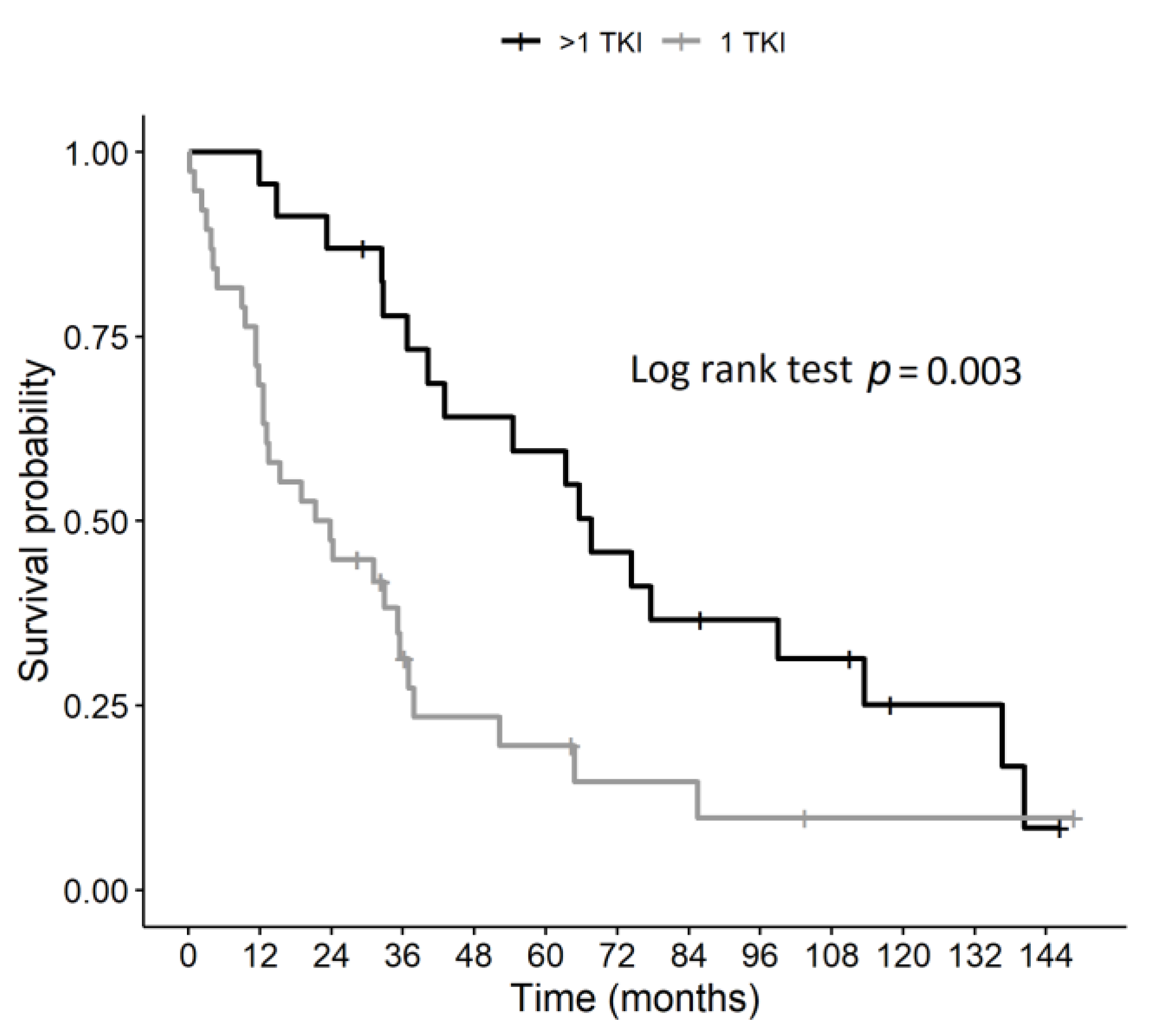
3.4. Overall Survival in the Study (n = 23) and in the Control group (n = 40)
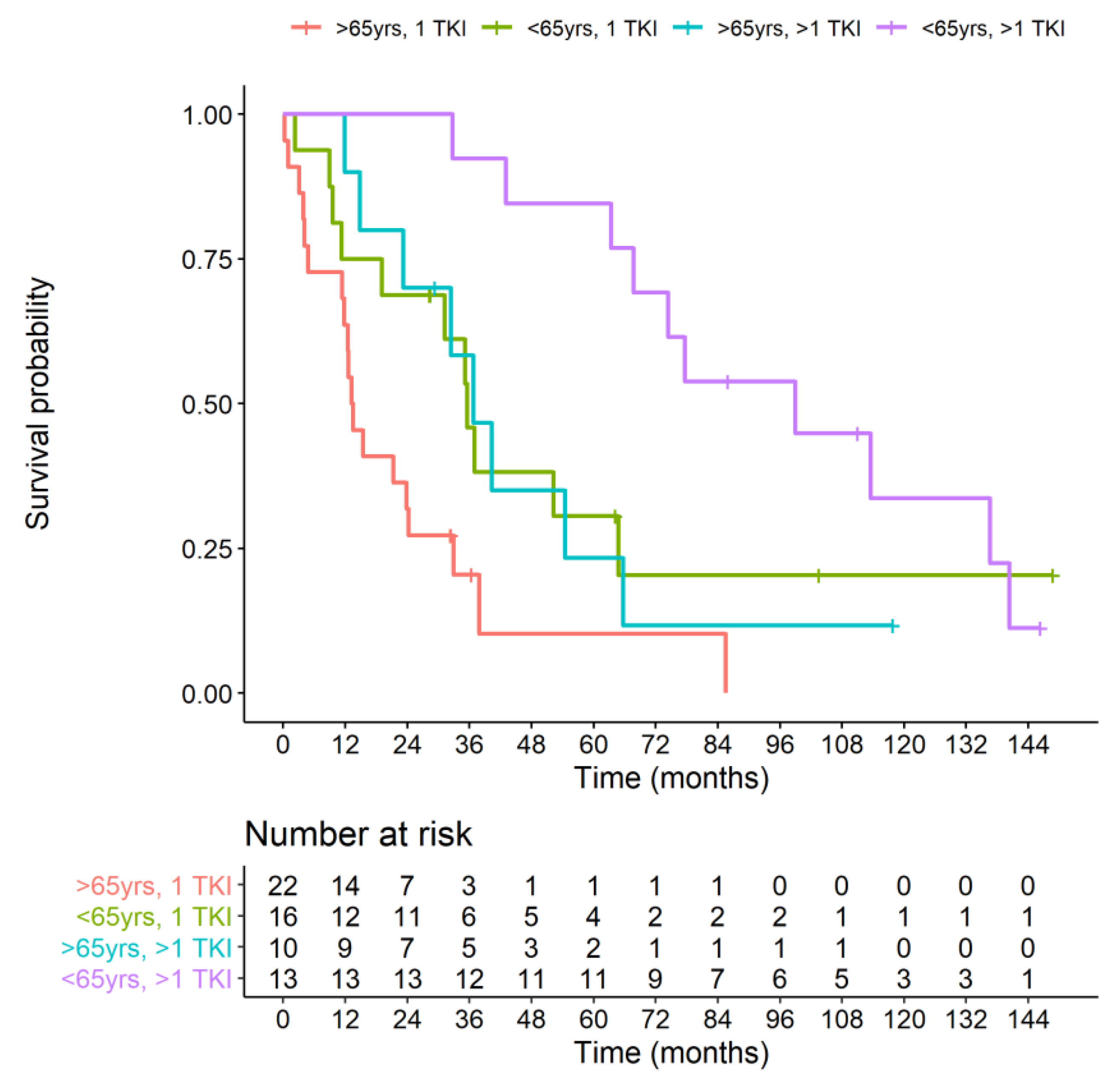
3.5. Overall Survival Based on the Age of TKI Treatment Start
3.6. Prognostic Factors Associated with Survival Benefit
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; Vathaire, F.D.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef] [PubMed]
- Fugazzola, L.; Elisei, R.; Fuhrer, D.; Jarzab, B.; Leboulleux, S.; Newbold, K.; Smit, J. 2019 European Thyroid Association Guidelines for the Treatment and Follow-Up of Advanced Radioiodine-Refractory Thyroid Cancer. Eur. Thyroid. J. 2019, 8, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Chougnet, C.; Brassard, M.; Leboulleux, S.; Baudin, E.; Schlumberger, M. Molecular targeted therapies for patients with refractory thyroid cancer. Clin. Oncol. (R. Coll. Radiol.) 2010, 22, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Araque, K.A.; Gubbi, S.; Klubo-Gwiezdzinska, J. Updates on the Management of Thyroid Cancer. Horm. Metab. Res. 2020, 52, 562–577. [Google Scholar] [CrossRef]
- Wells, S.A., Jr.; Robinson, B.G.; Gagel, R.F.; Dralle, H.; Fagin, J.A.; Santoro, M.; Baudin, E.; Elisei, R.; Jarzab, B.; Vasselli, J.R.; et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: A randomized, double-blind phase III trial. J. Clin. Oncol. 2012, 30, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Elisei, R.; Schlumberger, M.; Müller, S.P.; Schöffski, P.; Brose, M.S.; Shah, M.H.; Licitra, L.; Jarzab, B.; Medvedev, V.; Kreissl, M.C.; et al. Cabozantinib in progressive medullary thyroid cancer. J. Clin. Oncol. 2013, 31, 3639–3646. [Google Scholar] [CrossRef] [Green Version]
- Brose, M.S.; Nutting, C.M.; Jarzab, B.; Elisei, R.; Siena, S.; Bastholt, L.; Fouchardiere, C.d.l.; Pacini, F.; Paschke, R.; KeeShong, Y.; et al. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: A randomised, double-blind, phase 3 trial. Lancet 2014, 384, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, L.; Pieruzzi, L.; Biagini, A.; Sabini, E.; Valerio, L.; Giani, C.; Passannanti, P.; Pontillo-Contillo, B.; Battaglia, V.; Mazzeo, S.; et al. Lenvatinib and other tyrosine kinase inhibitors for the treatment of radioiodine refractory, advanced, and progressive thyroid cancer. OncoTargets Ther. 2016, 9, 6467–6477. [Google Scholar] [CrossRef] [Green Version]
- Kirtane, K.; Roth, M.Y. Emerging Therapies for Radioactive Iodine Refractory Thyroid Cancer. Curr. Treat. Options Oncol. 2020, 21, 18E. [Google Scholar] [CrossRef]
- Wen, T.; Xiao, H.; Luo, C.; Huang, L.; Xiong, M. Efficacy of sequential therapies with sorafenib-sunitinib versus sunitinib-sorafenib in metastatic renal cell carcinoma: A systematic review and meta-analysis. Oncotarget 2017, 8, 20441–20451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Real-life Practice Experts for HCC (RELPEC) Study Group; HCC 48 Group (hepatocellular carcinoma experts from 48 clinics in Japan). Important Clinical Factors in Sequential Therapy Including Lenvatinib against Unresectable Hepatocellular Carcinoma. Oncology 2019, 97, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Bennouna, J.; Boyer, M.; Hida, T.; Hirsh, V.; Kato, T.; Lu, S.; Mok, T.; Nakagawa, K.; O’Byrne, K.; et al. Sequencing of therapy following first-line afatinib in patients with EGFR mutation-positive non-small cell lung cancer. Lung Cancer 2019, 132, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurzrock, R.; Sherman, S.I.; Ball, D.W.; Forastiere, A.A.; Cohen, R.B.; Mehra, R.; Pfister, D.G.; Cohen, E.E.W.; Janisch, L.; Nauling, F.; et al. Activity of XL184 (Cabozantinib), an oral tyrosine kinase inhibitor, in patients with medullary thyroid cancer. J. Clin. Oncol. 2011, 29, 2660–2666. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Brose, M.S.; Holland, J.; Ferguson, K.C.; Sherman, S.I. A Phase I Study of Cabozantinib (XL184) in Patients with Differentiated Thyroid Cancer. Thyroid 2014, 24, 1508–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabanillas, M.E.; Schlumberger, M.; Jarzab, B.; Martins, R.G.; Pacini, F.; Robinson, B.; McCaffrey, J.C.; Shah, M.H.; Bodenner, D.L.; Topliss, D.; et al. A phase 2 trial of lenvatinib (E7080) in advanced, progressive, radioiodine-refractory, differentiated thyroid cancer: A clinical outcomes and biomarker assessment. Cancer 2015, 121, 2749–2756. [Google Scholar] [CrossRef]
- Bible, K.C.; Suman, V.J.; Molina, J.R.; Smallridge, R.C.; Maples, W.J.; Menefee, M.E.; Rubin, J.; Karlin, N.; Sideras, K.; Morris, J.C., III; et al. A Multicenter Phase 2 Trial of Pazopanib in Metastatic and Progressive Medullary Thyroid Carcinoma: MC057H. J. Clin. Endocrinol. Metab. 2014, 99, 1687–1693. [Google Scholar] [CrossRef]
- Atallah, V.; Hocquelet, A.; Do Cao, C.; Zerdoud, S.; De La Fouchardiere, C.; Bardet, S.; Italiano, A.; Dierick-Galet, A.; Leduc, N.; Bonichon, F.; et al. Activity and Safety of Sunitinib in Patients with Advanced Radioiodine Refractory Thyroid Carcinoma: A Retrospective Analysis of 57 Patients. Thyroid 2016, 26, 1085–1092. [Google Scholar] [CrossRef]
- Dadu, R.; Devine, C.; Hernandez, M.; Waguespack, S.G.; Busaidy, N.L.; Hu, M.I.; Jimenez, C.; Habra, M.A.; Sellin, R.V.; Ying, A.K.; et al. Role of salvage therapy in differentiated thyroid cancer patients who failed first-line sorafenib. J. Clin. Endocrinol. Metab. 2014, 99, 2086–2094. [Google Scholar] [CrossRef] [Green Version]
- Cabanillas, M.E.; de Souza, J.A.; Geyer, S.; Wirth, L.J.; Menefee, M.E.; Liu, S.V.; Shah, K.; Wright, J.; Shah, M.H. Cabozantinib As Salvage Therapy for Patients with Tyrosine Kinase Inhibitor-Refractory Differentiated Thyroid Cancer: Results of a Multicenter Phase II International Thyroid Oncology Group Trial. J. Clin. Oncol. 2017, 35, 3315–3321. [Google Scholar] [CrossRef]
- Massicotte, M.H.; Brassard, M.; Claude-Desroches, M.; Borget, I.; Bonichon, F.; Giraudet, A.-L.; Cao, C.D.; Chougnet, C.N.; Sophie Leboulleux, S.; Eric Baudin, E.; et al. Tyrosine kinase inhibitor treatments in patients with metastatic thyroid carcinomas: A retrospective study of the TUTHYREF network. Eur. J. Endocrinol. 2014, 170, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Brose, M.S.; Cabanillas, M.E.; Cohen, E.E.; Wirth, L.J.; Riehl, T.; Yue, H.; Sherman, S.I.; Sherman, E.J. Vemurafenib in patients with BRAF(V600E)-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: A non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.S.; Shin, D.Y.; Kim, M.; Park, S.Y.; Kim, T.H.; Kim, B.H.; Kim, E.Y.; Kim, W.B.; Chung, J.H.; Shong, Y.K.; et al. Extended Real-World Observation of Patients Treated with Sorafenib for Radioactive Iodine-Refractory Differentiated Thyroid Carcinoma and Impact of Lenvatinib Salvage Treatment: A Korean Multicenter Study. Thyroid 2019, 29, 1804–1810. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; M Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Chowdry, R.P.; Chen, Z.; Kim, S.; Saba, N.F.; Shin, D.M.; Khuri, F.R. Clinical efficacy of targeted biologic agents as second-line therapy of advanced thyroid cancer. Oncologist 2013, 18, 1262–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, R.L.; Qu, N.; Liao, T.; Wei, W.J.; Wang, Y.L.; Ji, Q.H. The Trend of Age-Group Effect on Prognosis in Differentiated Thyroid Cancer. Sci. Rep. 2016, 6, 27086. [Google Scholar] [CrossRef] [Green Version]
- Kauffmann, R.M.; Hamner, J.B.; Ituarte, P.H.G.; Yim, J.H. Age greater than 60 years portends a worse prognosis in patients with papillary thyroid cancer: Should there be three age categories for staging? BMC Cancer 2018, 18, 316. [Google Scholar] [CrossRef]
- Brose, M.S.; Worden, F.P.; Newbold, K.L.; Guo, M. Effect of Age on the Efficacy and Safety of Lenvatinib in Radioiodine-Refractory Differentiated Thyroid Cancer in the Phase III SELECT Trial. J. Clin. Oncol. 2017, 35, 2692–2699. [Google Scholar] [CrossRef]
- Locati, L.; Piovesan, A.; Durante, C.; Bregni, M.; Castagna, M.G.; Zovato6, S.; Giusti, M.; Ibrahim, T.; Puxeddu, E.; Fedele, G.; et al. Real-world efficacy and safety of lenvatinib: Data from a compassionate use in the treatment of radioactive iodine-refractory differentiated thyroid cancer patients in Italy. Eur. J. Cancer 2019, 118, 35–40. [Google Scholar] [CrossRef]
- Cantara, S.; Bertelli, E.; Occhini, R.; Regoli, M.; Brilli, L.; Pacini, F.; Castagna, M.G.; Toti, P. Blockade of the programmed death ligand 1 (PD-L1) as potential therapy for anaplastic thyroid cancer. Endocrine 2019, 64, 122–129. [Google Scholar] [CrossRef]
- French, J.D. Immunotherapy for advanced thyroid cancers—Rationale, current advances and future strategies. Nat. Rev. Endocrinol. 2020, 16, 629–641. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Study Group | Control Group | p Value | |
|---|---|---|---|---|
| (>1 TKI) | (1 TKI) | |||
| Patients (n) | 63 | 23 | 40 | |
| Male Sex n (%) | 33 (52.4%) | 12 (52.17%) | 21 (52.5%) | 0.99 |
| Histology n (%) | 0.6 | |||
| DTC | 42 (66.7%) | 15 (65.2%) | 27 (67.5%) | |
| PDTC | 5 (7.9%) | 1 (4.3%) | 4 (10%) | |
| MTC | 16 (25.4%) | 7 (30.5%) | 9 (22.5%) | |
| Age at cancer diagnosis (years) | 0.0046 | |||
| Mean (range) | 56.43 (23.20–85.35) | 48.56 (23.21–78.83) | 60.96 (29.88–85.35) | |
| Median | 57.56 | 53.75 | 61.07 | |
| Age at the time of TKI treatment (years) | 0.0073 | |||
| Mean (range) | 63.51 (25.57–88.01) | 56.85 (25.57–80.93) | 67.35 (32.67–88.01) | |
| Median | 65.51 | 59.18 | 68.32 | |
| Time-lapse between cancer diagnosis and TKI treatment (years) | 0.29 | |||
| Mean (range) | 7.08 (0.09–40.05) | 8.28 (0.68–40.05) | 6.39 (0.09–25.09) | |
| Median | 5.68 | 5.9 | 4.94 | |
| Time-lapse between appearance of metastases and TKI treatment (yrs) | 0.98 | |||
| Mean (range) | 3.59 (0–14.23) | 3.6 (0.05–9.79) | 3.58 (0–14.23) | |
| Median | 2.75 | 3.08 | 2.73 | |
| Numbers of anatomical site involved n (%) | 0.51 | |||
| 1 | 9 (14%) | 3 (13.5%) | 6 (15%) | |
| 2 | 18 (29%) | 4 (17%) | 14 (35%) | |
| 3 | 22 (35%) | 9 (39%) | 13 (32.5%) | |
| 4 | 7 (11%) | 4 (17%) | 3 (7.5%) | |
| >4 | 7 (11%) | 3 (13.5%) | 4 (10%) | |
| Bone metastases n (%) | 29 (46%) | 11 (48.8%) | 18 (45%) | 0.82 |
| Lung metastases n (%) | 43 (68.2%) | 18 (78.2%) | 25 (62.5%) | 0.27 |
| Sum of the target lesion diameters (mm) at baseline * | 0.25 | |||
| Mean (range) | 84.83 (17–275) | 74.32 (21–171) | 91.84 (17–275) | |
| Median | 65 | 64.65 | 65 | |
| ECOG performance status n (%) ** | 0.8 | |||
| 0–1 | 57 (93%) | 22 (95.7%) | 35 (92.1%) | |
| 2 | 4 (6.5%) | 1 (4.3%) | 3 (7.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brilli, L.; Dalmiglio, C.; Pilli, T.; Barbato, F.; Maino, F.; Capezzone, M.; Cartocci, A.; Castagna, M.G. Improvement of Overall Survival Using TKIs as Salvage Therapy in Advanced Thyroid Carcinoma: Real-Life Data on a Single Center Experience. J. Clin. Med. 2021, 10, 384. https://doi.org/10.3390/jcm10030384
Brilli L, Dalmiglio C, Pilli T, Barbato F, Maino F, Capezzone M, Cartocci A, Castagna MG. Improvement of Overall Survival Using TKIs as Salvage Therapy in Advanced Thyroid Carcinoma: Real-Life Data on a Single Center Experience. Journal of Clinical Medicine. 2021; 10(3):384. https://doi.org/10.3390/jcm10030384
Chicago/Turabian StyleBrilli, Lucia, Cristina Dalmiglio, Tania Pilli, Filomena Barbato, Fabio Maino, Marco Capezzone, Alessandra Cartocci, and Maria Grazia Castagna. 2021. "Improvement of Overall Survival Using TKIs as Salvage Therapy in Advanced Thyroid Carcinoma: Real-Life Data on a Single Center Experience" Journal of Clinical Medicine 10, no. 3: 384. https://doi.org/10.3390/jcm10030384