
Cytokine Profiles of Non-Small Cell Lung Cancer Patients Treated with Concurrent Chemoradiotherapy with Regards to Radiation Pneumonitis Severity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiation Therapy
2.3. Blood Samples
2.4. Cytokines Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients and Treatment Characteristics
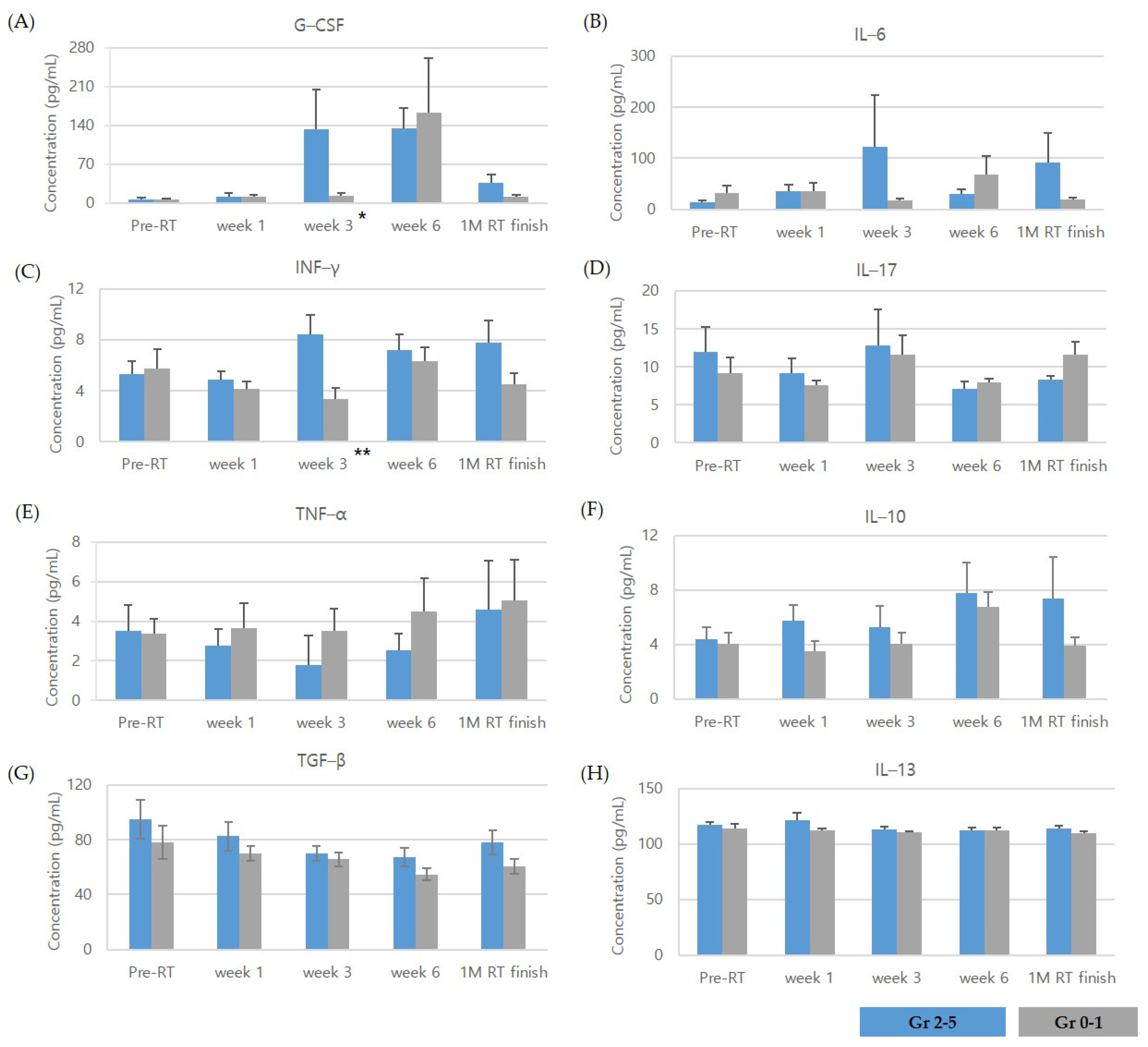
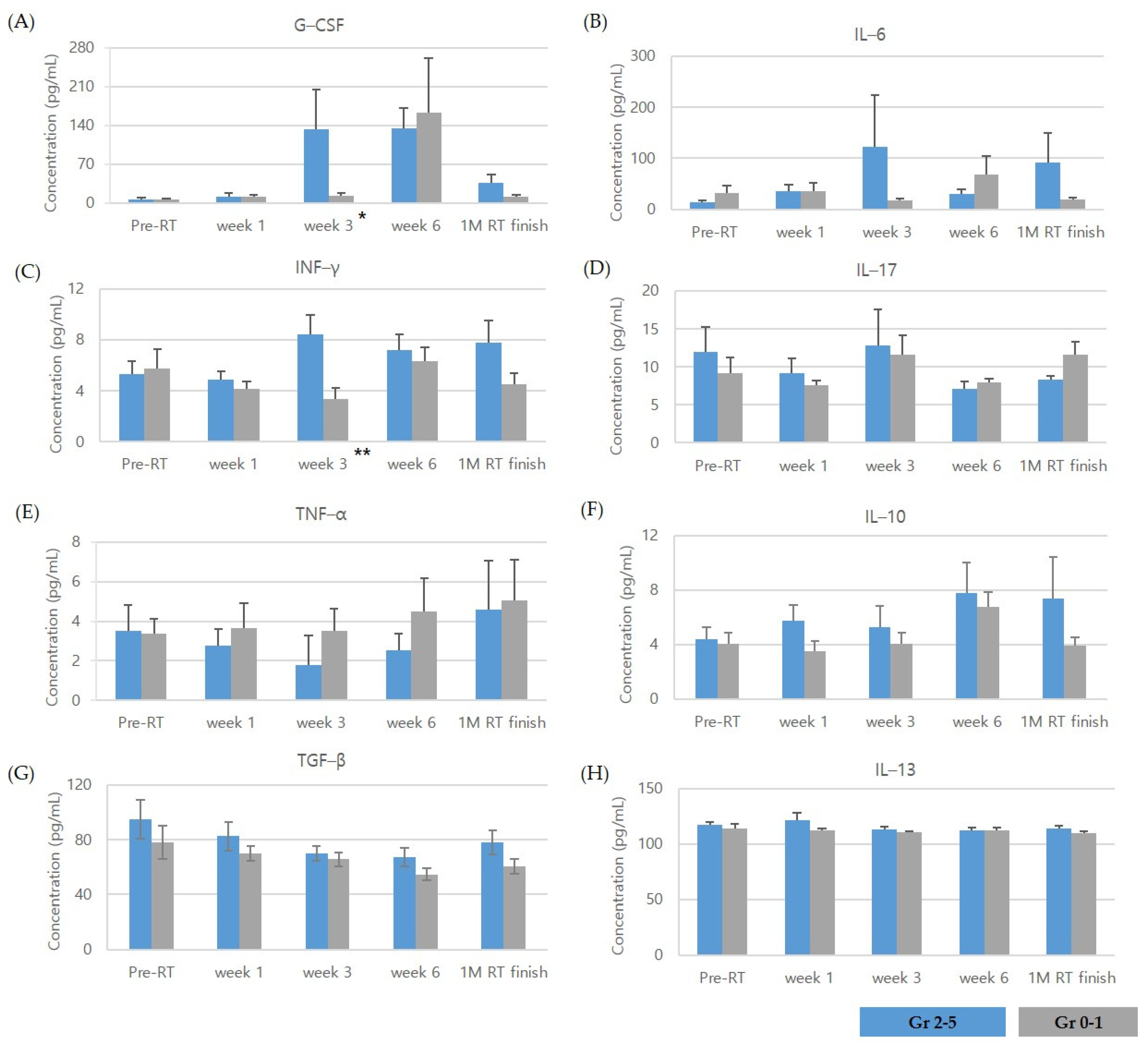
3.2. Cytokine Levels at Pre-Radiation Therapy (RT), during, and after Radiotherapy
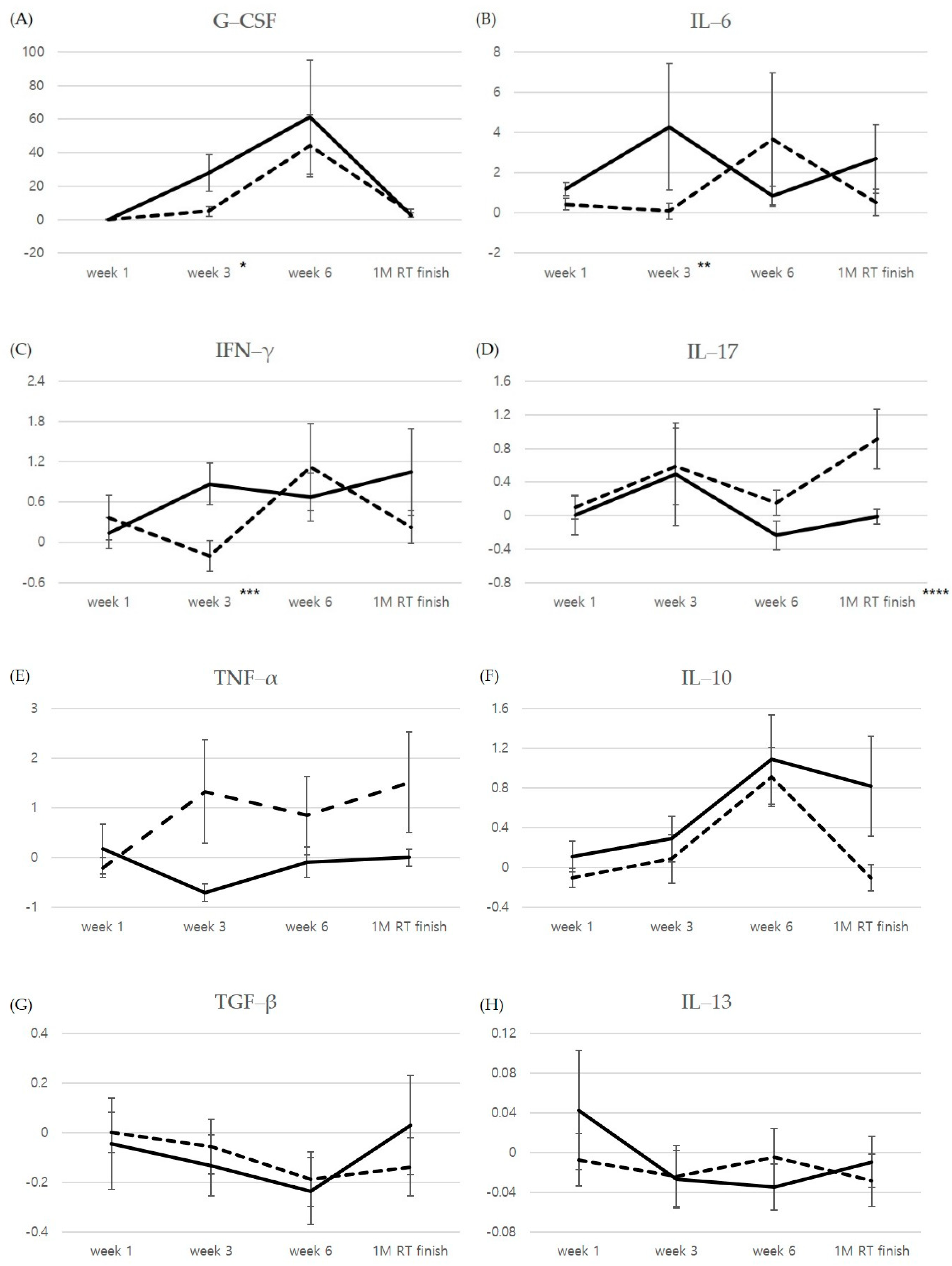
3.3. Relative Changes Compared to Pre-RT Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDonald, S.; Rubin, P.; Phillips, T.L.; Marks, L.B. Injury to the lung from cancer therapy: Clinical syndromes, measurable endpoints, and potential scoring systems. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1187–1203. [Google Scholar] [CrossRef]
- Stenmark, M.H.; Cai, X.W.; Shedden, K.; Hayman, J.A.; Yuan, S.; Ritter, T.; Ten Haken, R.K.; Lawrence, T.S.; Kong, F.M. Combining physical and biologic parameters to predict radiation-induced lung toxicity in patients with non-small-cell lung cancer treated with definitive radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e217–e222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, V. Radiation pneumonitis and pulmonary fibrosis in non-small-cell lung cancer: Pulmonary function, prediction, and prevention. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 5–24. [Google Scholar] [CrossRef]
- Lee, Y.H.; Choi, H.S.; Jeong, H.; Kang, K.M.; Song, J.H.; Lee, W.S.; Lee, G.W.; Song, H.N.; Kim, H.G.; Kang, M.H.; et al. Neutrophil-lymphocyte ratio and a dosimetric factor for predicting symptomatic radiation pneumonitis in non-small-cell lung cancer patients treated with concurrent chemoradiotherapy. Clin. Respir. J. 2018, 12, 1264–1273. [Google Scholar] [CrossRef]
- Käsmann, L.; Dietrich, A.; Staab-Weijnitz, C.A.; Manapov, F.; Behr, J.; Rimner, A.; Jeremic, B.; Senan, S.; De Ruysscher, D.; Lauber, K.; et al. Radiation-induced lung toxicity—Cellular and molecular mechanisms of pathogenesis, management, and literature review. Radiat. Oncol. 2020, 15, 214. [Google Scholar] [CrossRef]
- Kong, F.M.; Wang, S. Nondosimetric risk factors for radiation-induced lung toxicity. Semin. Radiat. Oncol. 2015, 25, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Shaverdian, N.; Thor, M.; Shepherd, A.F.; Offin, M.D.; Jackson, A.; Wu, A.J.; Gelblum, D.Y.; Yorke, E.D.; Simone, C.B., 2nd; Chaft, J.E.; et al. Radiation pneumonitis in lung cancer patients treated with chemoradiation plus durvalumab. Cancer Med. 2020, 9, 4622–4631. [Google Scholar] [CrossRef]
- Fu, Z.Z.; Peng, Y.; Cao, L.Y.; Chen, Y.S.; Li, K.; Fu, B.H. Correlations between Serum IL-6 Levels and Radiation Pneumonitis in Lung Cancer Patients: A Meta-Analysis. J. Clin. Lab. Anal. 2016, 30, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Śliwińska-Mossoń, M.; Wadowska, K.; Trembecki, Ł.; Bil-Lula, I. Markers Useful in Monitoring Radiation-Induced Lung Injury in Lung Cancer Patients: A Review. J. Pers. Med. 2020, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Ao, X.; Zhao, L.; Davis, M.A.; Lubman, D.M.; Lawrence, T.S.; Kong, F.M. Radiation produces differential changes in cytokine profiles in radiation lung fibrosis sensitive and resistant mice. J. Hematol. Oncol. 2009, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Arpin, D.; Perol, D.; Blay, J.Y.; Falchero, L.; Claude, L.; Vuillermoz-Blas, S.; Martel-Lafay, I.; Ginestet, C.; Alberti, L.; Nosov, D.; et al. Early variations of circulating interleukin-6 and interleukin-10 levels during thoracic radiotherapy are predictive for radiation pneumonitis. J. Clin. Oncol. 2005, 23, 8748–8756. [Google Scholar] [CrossRef]
- Siva, S.; MacManus, M.; Kron, T.; Best, N.; Smith, J.; Lobachevsky, P.; Ball, D.; Martin, O. A pattern of early radiation-induced inflammatory cytokine expression is associated with lung toxicity in patients with non-small cell lung cancer. PLoS ONE 2014, 9, e109560. [Google Scholar] [CrossRef]
- Lierova, A.; Jelicova, M.; Nemcova, M.; Proksova, M.; Pejchal, J.; Zarybnicka, L.; Sinkorova, Z. Cytokines and radiation-induced pulmonary injuries. J. Radiat. Res. 2018, 59, 709–753. [Google Scholar] [CrossRef]
- Hawkins, P.G.; Boonstra, P.S.; Hobson, S.T.; Hearn, J.W.D.; Hayman, J.A.; Ten Haken, R.K.; Matuszak, M.M.; Stanton, P.; Kalemkerian, G.P.; Ramnath, N.; et al. Radiation-induced lung toxicity in non-small-cell lung cancer: Understanding the interactions of clinical factors and cytokines with the dose-toxicity relationship. Radiother. Oncol. 2017, 125, 66–72. [Google Scholar] [CrossRef]
- Rübe, C.E.; Palm, J.; Erren, M.; Fleckenstein, J.; König, J.; Remberger, K.; Rübe, C. Cytokine plasma levels: Reliable predictors for radiation pneumonitis? PLoS ONE 2008, 3, e2898. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Attalah, H.; Harf, A.; Schlemmer, B.; Delclaux, C. Granulocyte colony-stimulating factor or neutrophil-induced pulmonary toxicity: Myth or reality? Systematic review of clinical case reports and experimental data. Chest 2001, 120, 1695–1701. [Google Scholar] [CrossRef] [PubMed]
- Aso, S.; Navarro-Martin, A.; Castillo, R.; Padrones, S.; Castillo, E.; Montes, A.; Martínez, J.I.; Cubero, N.; López, R.; Rodríguez, L.; et al. Severity of radiation pneumonitis, from clinical, dosimetric and biological features: A pilot study. Radiat. Oncol. 2020, 15, 246. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; Jeong, S.Y.; Song, S.Y.; Choi, E.K. The emerging role of myeloid-derived suppressor cells in radiotherapy. Radiat. Oncol. J. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Ko, E.C.; Raben, D.; Formenti, S.C. The Integration of Radiotherapy with Immunotherapy for the Treatment of Non-Small Cell Lung Cancer. Clin. Cancer Res. 2018, 24, 5792–5806. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.A.; Noh, J.M.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Pyo, H.; Ahn, Y.C.; Park, K. Real world data of durvalumab consolidation after chemoradiotherapy in stage III non-small-cell lung cancer. Lung Cancer 2020, 146, 23–29. [Google Scholar] [CrossRef]
- Schoenfeld, J.D.; Nishino, M.; Severgnini, M.; Manos, M.; Mak, R.H.; Hodi, F.S. Pneumonitis resulting from radiation and immune checkpoint blockade illustrates characteristic clinical, radiologic and circulating biomarker features. J. Immunother. Cancer 2019, 7, 112. [Google Scholar] [CrossRef]
- Christensen, E.; Pintilie, M.; Evans, K.R.; Lenarduzzi, M.; Ménard, C.; Catton, C.N.; Diamandis, E.P.; Bristow, R.G. Longitudinal cytokine expression during IMRT for prostate cancer and acute treatment toxicity. Clin. Cancer Res. 2009, 15, 5576–5583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanojković, T.P.; Matić, I.Z.; Petrović, N.; Stanković, V.; Kopčalić, K.; Besu, I.; Đorđić Crnogorac, M.; Mališić, E.; Mirjačić-Martinović, K.; Vuletić, A.; et al. Evaluation of cytokine expression and circulating immune cell subsets as potential parameters of acute radiation toxicity in prostate cancer patients. Sci. Rep. 2020, 10, 19002. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.S.W.; Zhang, H.; Wang, L.; Citrin, D.; Dawson, L.A. Association of pro-inflammatory soluble cytokine receptors early during hepatocellular carcinoma stereotactic radiotherapy with liver toxicity. NPJ Precis. Oncol. 2020, 4, 17. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | All Patients (n = 15) | Gr ≥ 2 (n = 6) | Gr 0–1 (n = 9) | p-Value | |
|---|---|---|---|---|---|
| Sex | male | 13 | 5 | 8 | 1.0 |
| female | 2 | 1 | 1 | ||
| Age | years, median (range) | 70 (54–76) | 71.5 (58–75) | 60 (54–76) | 0.456 |
| ECOG | 0 | 3 | 0 | 3 | 0.229 |
| 1 | 12 | 6 | 6 | ||
| Smoking history | none | 4 | 1 | 3 | 0.604 |
| yes | 11 | 5 | 6 | ||
| Underlying lung disease | none | 5 | 1 | 4 | 0.580 |
| yes | 10 | 5 | 5 | ||
| Clinical stage (7th edition) | IIIA | 6 | 1 | 5 | 0.287 |
| IIIB | 9 | 5 | 4 | ||
| Histology | SqCC | 11 | 5 | 6 | 0.604 |
| adenocarcinoma | 4 | 1 | 3 | ||
| Chemotherapy regimen | Paclitaxel-cisplatin | 8 | 4 | 4 | 0.608 |
| Paclitaxel-carboplatin | 7 | 2 | 5 | ||
| Total RT dose | Gy, median (range) | 59.4 (55.8–66) | 59.4 (59.4–66) | 63 (54.8–66) | 0.388 |
| RT technique | 3D CRT | 7 | 1 | 6 | 0.119 |
| IMRT | 8 | 5 | 3 |
| Gr ≥ 2 | Gr 0–1 | p Value | |||
|---|---|---|---|---|---|
| Mean | SE | Mean | SE | ||
| G-CSF | |||||
| Week1 | −0.035 | 0.227 | −0.018 | 0.361 | 0.456 |
| Week3 | 27.732 | 10.849 | 5.077 | 3.020 | 0.026 |
| Week6 | 61.257 | 34.150 | 44.268 | 18.680 | 0.607 |
| 1M RT F | 2.801 | 1.157 | 4.064 | 2.341 | 0.529 |
| IL-6 | |||||
| Week1 | 1.196 | 0.32 | 0.434 | 0.29 | 0.145 |
| Week3 | 4.276 | 3.14 | 0.089 | 0.39 | 0.050 |
| Week6 | 0.834 | 0.49 | 3.679 | 3.30 | 0.864 |
| 1M RT F | 2.696 | 1.71 | 0.528 | 0.65 | 0.147 |
| IFN-γ | |||||
| Week1 | 0.138 | 0.23 | 0.366 | 0.33 | 0.776 |
| Week3 | 0.872 | 0.31 | −0.203 | 0.23 | 0.026 |
| Week6 | 0.674 | 0.36 | 1.120 | 0.65 | 0.955 |
| 1M RT F | 1.048 | 0.65 | 0.226 | 0.25 | 0.438 |
| IL-17 | |||||
| Week1 | 0.002 | 0.23 | 0.099 | 0.14 | 0.607 |
| Week3 | 0.491 | 0.61 | 0.586 | 0.46 | 0.414 |
| Week6 | −0.238 | 0.17 | 0.147 | 0.15 | 0.088 |
| 1M RT F | −0.010 | 0.09 | 0.916 | 0.35 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, B.K.; Kim, J.H.; Jung, M.H.; Kang, K.M.; Lee, Y.H. Cytokine Profiles of Non-Small Cell Lung Cancer Patients Treated with Concurrent Chemoradiotherapy with Regards to Radiation Pneumonitis Severity. J. Clin. Med. 2021, 10, 699. https://doi.org/10.3390/jcm10040699
Jeong BK, Kim JH, Jung MH, Kang KM, Lee YH. Cytokine Profiles of Non-Small Cell Lung Cancer Patients Treated with Concurrent Chemoradiotherapy with Regards to Radiation Pneumonitis Severity. Journal of Clinical Medicine. 2021; 10(4):699. https://doi.org/10.3390/jcm10040699
Chicago/Turabian StyleJeong, Bae Kwon, Jin Hyun Kim, Myeong Hee Jung, Ki Mun Kang, and Yun Hee Lee. 2021. "Cytokine Profiles of Non-Small Cell Lung Cancer Patients Treated with Concurrent Chemoradiotherapy with Regards to Radiation Pneumonitis Severity" Journal of Clinical Medicine 10, no. 4: 699. https://doi.org/10.3390/jcm10040699