
Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis

 ,
,  ,
, 
 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
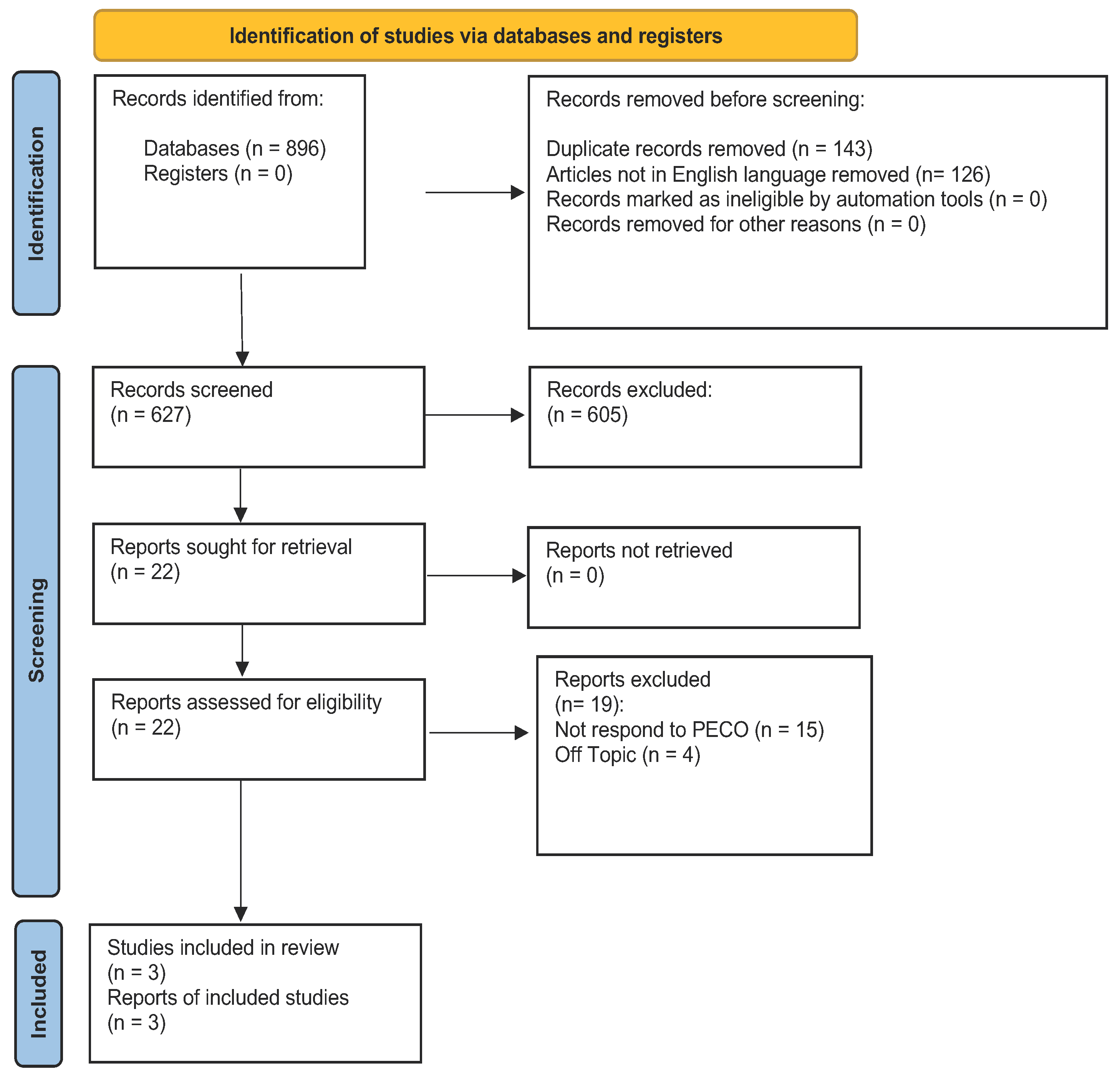
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Main Findings
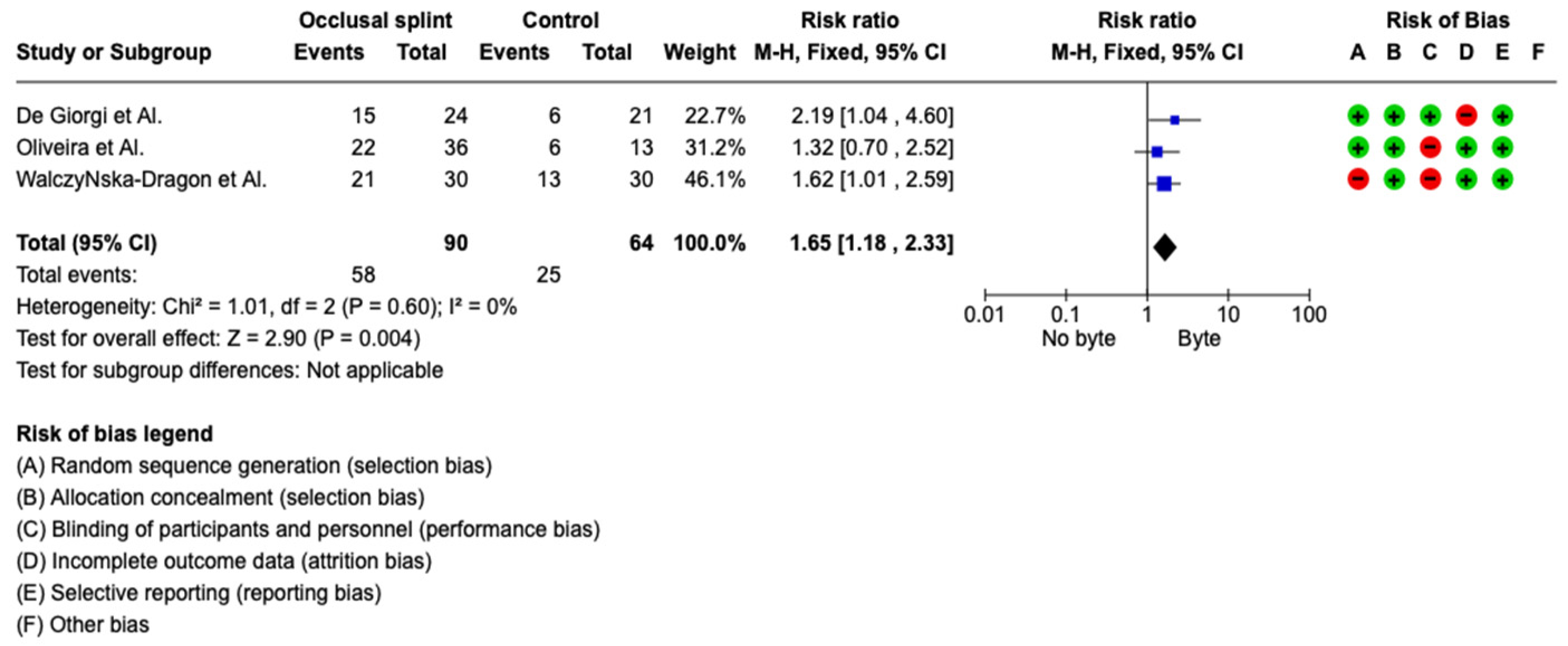
3.3. Metanalysis
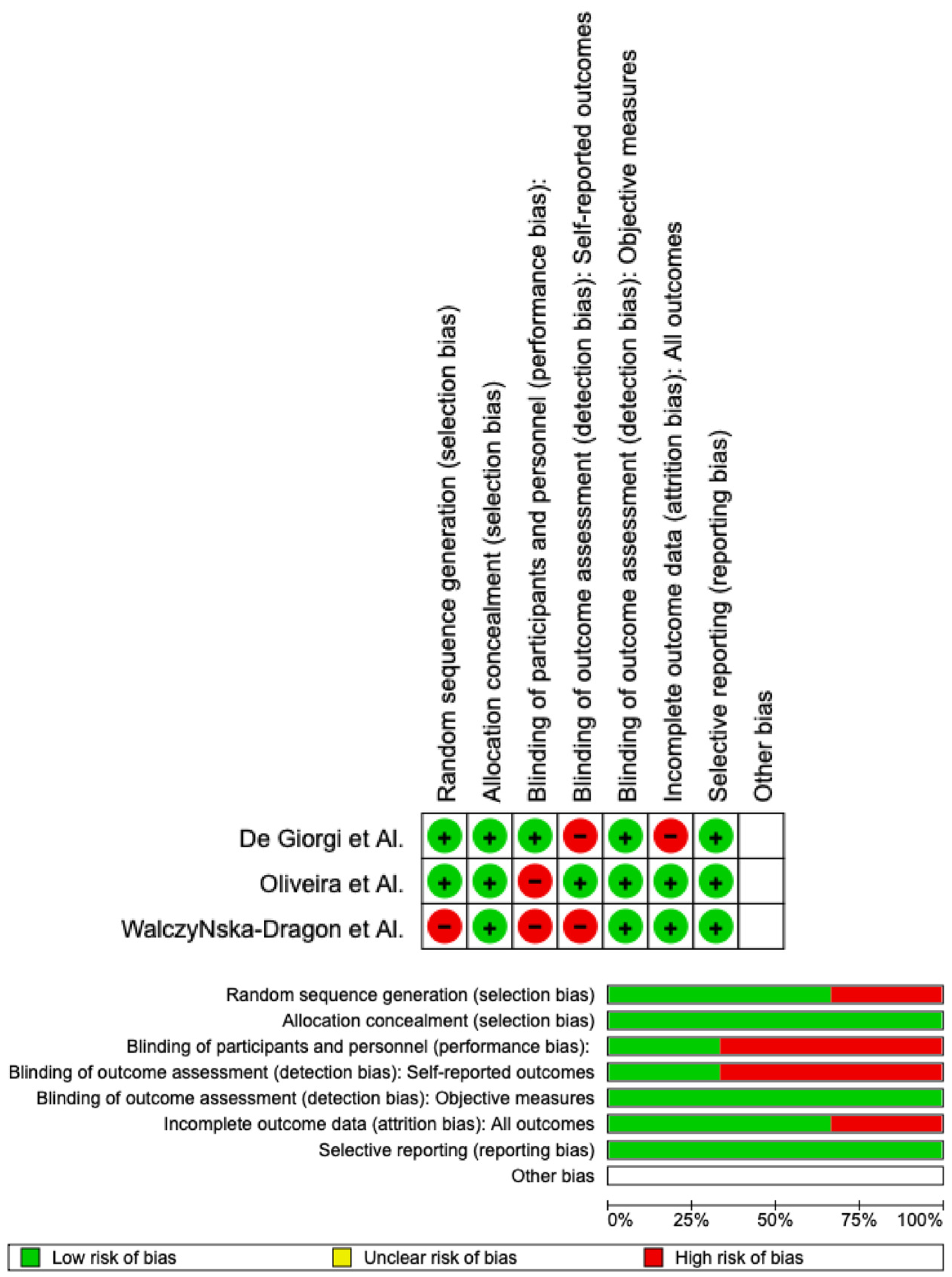
3.4. Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMD | temporomandibular disorders |
| TMJ | temporomandibular joint |
| PECO | patients, exposure, comparison, outcome |
| DC/TMD | diagnostic criteria for temporomandibular disorders |
| RCT | randomized clinical trial |
| MeSh | Medical Subject Headings |
| ROM | range of motion |
References
- Di Francesco, F.; Lanza, A.; Di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Appl. Sci. 2022, 12, 12409. [Google Scholar] [CrossRef]
- la Touche, R.; París-Alemany, A.; von Piekartz, H.; Mannheimer, J.S.; Fernández-Carnero, J.; Rocabado, M. The Influence of Cranio-cervical Posture on Maximal Mouth Opening and Pressure Pain Threshold in Patients with Myofascial Temporomandibular Pain Disorders. Clin. J. Pain 2011, 27, 48–55. [Google Scholar] [CrossRef]
- Tallarico, M.; Meloni, S.M.; Park, C.-J.; Zadrożny; Scrascia, R.; Cicciù, M. Implant Fracture: A Narrative Literature Review. Prosthesis 2021, 3, 267–279. [Google Scholar] [CrossRef]
- Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- Saccomanno, S.; Quinzi, V.; D’Andrea, N.; Albani, A.; Paskay, L.C.; Marzo, G. Traumatic Events and Eagle Syndrome: Is There Any Correlation? A Systematic Review. Healthcare 2021, 9, 825. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; D’amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofacial Surg. 2022, 1097. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Diaz-Betancourt, M.; Cagetti, M.; Carvalho, J.; Carvalho, T.; Cortés-Martinicorena, J.; Deschner, J.; Douglas, G.; Giacaman, R.; Machiulskiene, V.; et al. Study Protocol for an Online Questionnaire Survey on Symptoms/Signs, Protective Measures, Level of Awareness and Perception Regarding COVID-19 Outbreak among Dentists. A Global Survey. Int. J. Environ. Res. Public Health 2020, 17, 5598. [Google Scholar] [CrossRef]
- Chakraborty, T.; Jamal, R.; Battineni, G.; Teja, K.; Marto, C.; Spagnuolo, G. A Review of Prolonged Post-COVID-19 Symptoms and Their Implications on Dental Management. Int. J. Environ. Res. Public Health 2021, 18, 5131. [Google Scholar] [CrossRef]
- Soltani, P.; Baghaei, K.; Tafti, K.T.; Spagnuolo, G. Science Mapping Analysis of COVID-19 Articles Published in Dental Journals. Int. J. Environ. Res. Public Health 2021, 18, 2110. [Google Scholar] [CrossRef] [PubMed]
- Sycinska-Dziarnowska, M.; Maglitto, M.; Woźniak, K.; Spagnuolo, G. Oral Health and Teledentistry Interest during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 3532. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Prevalence of Temporomandibular Disorders in Children and Adolescents Evaluated with Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-analysis. J. Oral Rehabil. 2023. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Laino, L.; Fiorillo, L. Oral signs and symptoms of COVID-19 affected patients: Dental practice as prevention method. Minerva Dent. Oral Sci. 2020, 71, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Qazi, N.; Pawar, M.; Padhly, P.P.; Pawar, V.; Mehta, V.; D’Amico, C.; Nicita, F.; Fiorillo, L.; Alushi, A.; Minervini, G.; et al. Teledentistry: Evaluation of Instagram Posts Related to Bruxism. Technol. Health Care 2023, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bellini, P.; Iani, C.; Zucchelli, G.; Franchi, M.; Mattioli, A.V.; Consolo, U. Impact of the COVID-19 pandemic on dental hygiene students in the Italian region of Emilia-Romagna. Minerva Dent. Oral Sci. 2022, 71, 180–191. [Google Scholar] [CrossRef]
- Wadhokar, O.C.; Patil, D.S. Current Trends in the Management of Temporomandibular Joint Dysfunction: A Review. Cureus 2022, 14, e29314. [Google Scholar] [CrossRef]
- An, J.-S.; Jeon, D.-M.; Jung, W.-S.; Yang, I.-H.; Lim, W.H.; Ahn, S.-J. Influence of temporomandibular joint disc displacement on craniocervical posture and hyoid bone position. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 72–79. [Google Scholar] [CrossRef]
- Lee, W.Y.; Okeson, J.P.; Lindroth, J. The relationship between forward head posture and temporomandibular disorders. J. Orofac. Pain 1995, 9. [Google Scholar]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. CRANIO® 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.D.; Del Mondo, D.D.; Russo, D.D.; Cervino, G.D.; D’Amico, C.D.; Fiorillo, L.D. Stem Cells in Temporomandibular Joint Engineering: State of Art and Future Persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. [Google Scholar] [CrossRef]
- Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Per-spectives for the Management of Orofacial Pain. Molecules 2022, 28, 106. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-H. Effects on migraine, neck pain, and head and neck posture, of temporomandibular disorder treatment: Study of a retrospective cohort. Arch. Oral Biol. 2020, 114, 104718. [Google Scholar] [CrossRef]
- Perinetti, G. Correlations Between the Stomatognathic System and Body Posture: Biological or Clinical Impli-cations? Clinics 2009, 64, 77–78. [Google Scholar] [CrossRef] [Green Version]
- Quinzi, V.; Paskay, L.C.; Manenti, R.J.; Giancaspro, S.; Marzo, G.; Saccomanno, S. Telemedicine for a multidisciplinary as-sessment of orofacial pain in a patient affected by eagle’s syndrome: A clinical case report. Open Dent. J. 2021, 15, 102–110. [Google Scholar] [CrossRef]
- Abe, S.; Kawano, F.; Matsuka, Y.; Masuda, T.; Okawa, T.; Tanaka, E. Relationship between Oral Parafunctional and Postural Habits and the Symptoms of Temporomandibular Disorders: A Survey-Based Cross-Sectional Cohort Study Using Propensity Score Matching Analysis. J. Clin. Med. 2022, 11, 6396. [Google Scholar] [CrossRef]
- Miranda, L.S.; Graciosa, M.D.; Puel, A.N.; de Oliveira, L.R.; Sonza, A. Masticatory muscles electrical activity, stress and posture in preadolescents and adolescents with and without temporomandibular dysfunction. Int. J. Pediatr. Otorhinolaryngol. 2020, 141, 110562. [Google Scholar] [CrossRef]
- de Giorgi, I.; Castroflorio, T.; Cugliari, G.; Deregibus, A. Does occlusal splint affect posture? A randomized controlled trial. CRANIO® 2020, 38, 264–272. [Google Scholar] [CrossRef]
- Oliveira, S.S.I.; Pannuti, C.M.; Paranhos, K.S.; Tanganeli, J.P.C.; Laganá, D.C.; Sesma, N.; Duarte, M.; Frigerio, M.L.M.A.; Cho, S. Effect of occlusal splint and therapeutic exercises on postural balance of patients with signs and symptoms of temporo-mandibular disorder. Clin. Exp. Den.t Res. 2019, 5, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walczyńska-Dragon, K.; Baron, S.; Nitecka-Buchta, A.; Tkacz, E. Correlation between TMD and Cervical Spine Pain and Mobility: Is the Whole Body Balance TMJ Related? Biomed Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Faulin, E.F.; Guedes, C.G.; Feltrin, P.P.; Joffiley, C.M.M.S.C. Association between temporomandibular disorders and abnormal head postures. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef]
- Mehta, N.R.; Correa, L.P. Oral Appliance Therapy and Temporomandibular Disorders. Sleep Med. Clin. 2018, 13, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Franco, R.; Basili, M.; Venditti, A.; Chiaramonte, C.; Ottria, L.; Barlattani, A.; Bollero, P. Statistical analysis of the frequency distribution of signs and symptoms of patients with temporomandibular disorders. Oral Implant. 2016, 9, 190–201. [Google Scholar] [CrossRef]
- Saddu, S.C. The Evaluation of Head and Craniocervical Posture among Patients with and without Temporomandibular Joint Disorders- A Comparative Study. J. Clin. Diagn. Res. 2015, 9, ZC55–ZC58. [Google Scholar] [CrossRef]
- Fagundes, N.C.F.; Minervini, G.; Alonso, B.F.; Nucci, L.; Grassia, V.; d’Apuzzo, F.; Puigdollers, A.; Perillo, L.; Flores-Mir, C. Patient-reported outcomes while managing obstructive sleep apnea with oral appliances: A scoping review. J. Evid. -Based Dent. Pract. 2022, 23, 101786. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Lippi, L.; Giudice, A.; Calafiore, D.; Paolucci, T.; Renò, F.; Migliario, M.; Fortunato, L.; Invernizzi, M.; de Sire, A. Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Sys-tematic Review. J. Clin. Med. 2022, 11, 6231. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sci. 2023, 13, 481. [Google Scholar] [CrossRef] [PubMed]
- Câmara-Souza, M.B.; Bracci, A.; Colonna, A.; Ferrari, M.; Garcia, R.C.M.R.; Manfredini, D. Ecological Momentary Assessment of Awake Bruxism Frequency in Patients with Different Temporomandibular Disorders. J. Clin. Med. 2023, 12, 501. [Google Scholar] [CrossRef] [PubMed]
- Arribas-Pascual, M.; Hernández-Hernández, S.; Jiménez-Arranz, C.; Grande-Alonso, M.; Angulo-Díaz-Parreño, S.; La Touche, R.; Paris-Alemany, A. Effects of Physiotherapy on Pain and Mouth Opening in Temporomandibular Disorders: An Umbrella and Mapping Systematic Review with Meta-Meta-Analysis. J. Clin. Med. 2023, 12, 788. [Google Scholar] [CrossRef]
- Almeida, L.E.; Doetzer, A.; Beck, M.L. Immunohistochemical Markers of Temporomandibular Disorders: A Review of the Literature. J. Clin. Med. 2023, 12, 789. [Google Scholar] [CrossRef]
- Winocur, E.; Wieckiewicz, M. Temporomandibular Disorders Related Pain among Sleep & Awake Bruxers: A Comparison among Sexes and Age. J. Clin. Med. 2023, 12, 1364. [Google Scholar] [CrossRef]
- Chęciński, M.; Chęcińska, K.; Turosz, N.; Sikora, M.; Chlubek, D. Intra-Articular Injections into the Inferior versus Superior Compartment of the Temporomandibular Joint: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1664. [Google Scholar] [CrossRef]
- Colonna, A.; Bracci, A.; Ahlberg, J.; Câmara-Souza, M.B.; Bucci, R.; Conti, P.C.R.; Dias, R.; Emodi-Perlmam, A.; Favero, R.; Häggmän-Henrikson, B.; et al. Ecological Momentary Assessment of Awake Bruxism Behaviors: A Scoping Review of Findings from Smartphone-Based Studies in Healthy Young Adults. J. Clin. Med. 2023, 12, 1904. [Google Scholar] [CrossRef] [PubMed]
- Nota, A.; Tecco, S.; Ehsani, S.; Padulo, J.; Baldini, A. Postural stability in subjects with temporomandibular disorders and healthy controls: A comparative assessment. J. Electromyogr. Kinesiol. 2017, 37, 21–24. [Google Scholar] [CrossRef] [PubMed]
- di Giacomo, P.; Ferrara, V.; Accivile, E.; Ferrato, G.; Polimeni, A.; di Paolo, C. Relationship between Cervical Spine and Skeletal Class II in Subjects with and without Temporomandibular Disorders. Pain Res. Manag. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Chaves, P.J.; de Oliveira, F.E.M.; Damázio, L.C.M. Incidence of postural changes and temporoman-dibular disorders in students. Acta Ortop. Bras. 2017, 25, 162–164. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.C.; Grossi, D.; Dach, F.; Speciali, J.G.; Gonçalves, M.C.; Chaves, T.C. Body posture changes in women with migraine with or without temporomandibular disorders. Braz. J. Phys. Ther. 2014, 18, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Paço, M.; Duarte, J.; Pinho, T. Orthodontic Treatment and Craniocervical Posture in Patients with Temporomandibular Disorders: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 3295. [Google Scholar] [CrossRef]
- Ekici Camcı, H. Relationship of temporomandibular joint disorders with cervical posture and hyoid bone position. Cranio® 2021, 1–10. [Google Scholar] [CrossRef]
- Cortese, S.; Mondello, A.; Galarza, R.; Biondi, A. Postural alterations as a risk factor for temporomandibular disorders. Acta Odontol. Latinoam. 2017, 30, 57–61. [Google Scholar]
- Cuccia, A.; Caradonna, C. The Relationship Between the Stomatognathic System and Body Posture. Clinics 2009, 64, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, D.; Castroflorio, T.; Perinetti, G.; Guardanardini, L. Dental occlusion, body posture and temporomandibular disorders: Where we are now and where we are heading for. J. Oral Rehabil. 2012, 39, 463–471. [Google Scholar] [CrossRef]
- Carini, F.; Mazzola, M.; Fici, C.; Palmeri, S.; Messina, M.; Damiani, P.; Tomasello, G. Posture and posturology, anatomical and physiological profiles: Overview and current state of art. Acta Biomed. 2017, 88, 11–16. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PubMed ((temporomandibular disorders) OR (TMD)) AND (POSTURE) |
| Lilacs temporomandibular disorders [Palavras] or tmd [Palavras] and posture [Palavras] |
| Web of Science ((ALL=(temporomandibular disorders)) OR ALL=(tmd)) AND ALL=(posture) |
| Author | Year | Sample | Diagnostic Criteria | Type of Byte | Treatment Duration | Exams to Evaluate Effect on Posture | Results |
|---|---|---|---|---|---|---|---|
| De Giorgi et al. [26] | 2020 | 45 women: 24 test 21 control | DC/TMD | 2 mm with posterior contact | 1, 2, 3 months | Evaluation of VAS Rasterstereography Cephalometric analysis | Significant differences concerning the cervical arrow, the kyphotic and lordotic angles |
| Oliveira et al. [27] | 2019 | 49 patients: 36 test 13 control | DC/TMD | 1.5 mm with simultaneous bilateral contact | 12 weeks | Stabilometry test with the eye open and closed | Study group had increased anteroposterior velocity with eyes closed and eyes open |
| WalczyNska-Dragon et al. [28] | 2014 | 60 patients: 30 test 30 control | DC/TMD | Byte only with anterior contact | Evaluation after 3 weeks and 3 months | Evaluation of VAS Evaluation of mandibular movement with JMT Evaluation of cervical spine movement with MCS | Test group: improvement in TMJ movement and cervical spinal movement Diminutions of VAS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minervini, G.; Franco, R.; Marrapodi, M.M.; Crimi, S.; Badnjević, A.; Cervino, G.; Bianchi, A.; Cicciù, M. Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis. J. Clin. Med. 2023, 12, 2652. https://doi.org/10.3390/jcm12072652
Minervini G, Franco R, Marrapodi MM, Crimi S, Badnjević A, Cervino G, Bianchi A, Cicciù M. Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2652. https://doi.org/10.3390/jcm12072652
Chicago/Turabian StyleMinervini, Giuseppe, Rocco Franco, Maria Maddalena Marrapodi, Salvatore Crimi, Almir Badnjević, Gabriele Cervino, Alberto Bianchi, and Marco Cicciù. 2023. "Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2652. https://doi.org/10.3390/jcm12072652