
Should Trazodone Be First-Line Therapy for Insomnia? A Clinical Suitability Appraisal
 , , and
, , and 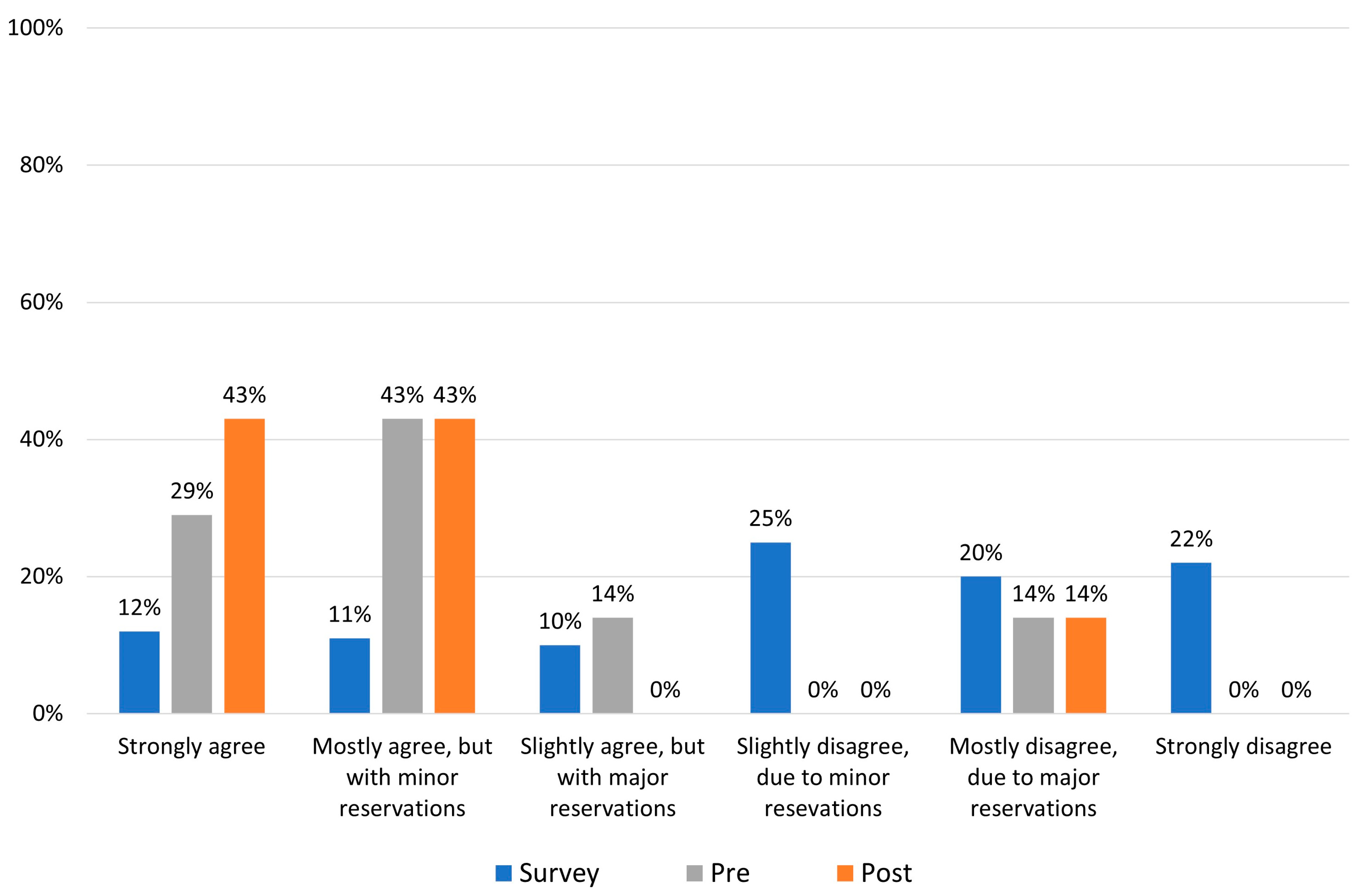{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
- Strongly agree;
- Mostly agree, but with minor reservations;
- Slightly agree, but with major reservations;
- Slightly disagree, due to minor reservations;
- Mostly disagree, due to major reservations;
- Strongly disagree
- Evidence obtained from meta-analysis, including at least one large, randomized control trial (RCT);
- Evidence obtained from either meta-analysis, including at least one small RCT, or from at least one well-designed large RCT;
- Evidence obtained from a well-designed cohort or from case-controlled studies;
- Evidence obtained from case series, case reports, or flawed clinical trials;
- Opinions of respected authorities based on clinical experience, descriptive studies, or reports of expert committees;
- Insufficient evidence to form an opinion.
3. Results
3.1. Literature Review
3.1.1. Rationale and Definition of the Statement
3.1.2. Literature Search Criteria
3.1.3. Literature in Support of the Statement: Key Studies
3.1.4. Literature in Opposition to the Statement: Key Studies
3.1.5. Grading of Literature Evidence and Level of Statement Support
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Centers for Disease Control and Prevention of Sleep and Sleep Disorders: Data and Statistics. Available online: https://www.cdc.gov/sleep/data_statistics.html (accessed on 10 December 2022).
- Chattu, V.K.; Manzar, M.D.; Kumary, S.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The Global Problem of Insufficient Sleep and Its Serious Public Health Implications. Healthcare 2018, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: An American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. 2021, 17, 263–298. [Google Scholar] [CrossRef]
- Streatfeild, J.; Smith, J.; Mansfield, D.; Pezzullo, L.; Hillman, D. The social and economic cost of sleep disorders. Sleep 2021, 44, zsab132. [Google Scholar] [CrossRef]
- Sharma, M.P.; Andrade, C. Behavioral interventions for insomnia: Theory and practice. Indian J. Psychiatry 2012, 54, 359–366. [Google Scholar] [CrossRef]
- Stahl, S.M. Mechanism of action of trazodone: A multifunctional drug. CNS Spectr. 2009, 14, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Murray Horwitz, M.; Bertisch, S.M.; Herzig, S.J.; Buysse, D.J.; Toh, S. Trends in Dispensing of Zolpidem and Low-Dose Trazodone Among Commercially Insured Adults in the United States, 2011-2018. JAMA 2020, 324, 2211–2213. [Google Scholar] [CrossRef] [PubMed]
- Roch, C.; Bergamini, G.; Steiner, M.A.; Clozel, M. Nonclinical pharmacology of daridorexant: A new dual orexin receptor antagonist for the treatment of insomnia. Psychopharmacology 2021, 238, 2693–2708. [Google Scholar] [CrossRef]
- Ufer, M.; Kelsh, D.; Schoedel, K.A.; Dingemanse, J. Abuse potential assessment of the new dual orexin receptor antagonist daridorexant in recreational sedative drug users as compared to suvorexant and zolpidem. Sleep 2022, 45, zsab224. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.F.; Chung, K.F.; Yung, K.P.; Ng, T.H. Doxepin for insomnia: A systematic review of randomized placebo-controlled trials. Sleep Med. Rev. 2015, 19, 75–83. [Google Scholar] [CrossRef]
- Everitt, H.; Baldwin, D.S.; Stuart, B.; Lipinska, G.; Mayers, A.; Malizia, A.L.; Manson, C.C.; Wilson, S. Antidepressants for insomnia in adults. Cochrane Database Syst. Rev. 2018, 5, CD010753. [Google Scholar] [CrossRef]
- McCall, W.V.; Ahuja, A.; Olivieri, A.; Busser, A.; Grandner, M. Trazodone Prescribing in Insomnia: A Real-World Cohort Study American Psychiatric Association Annual Meeting. 2022. Available online: https://www.psychiatry.org/getattachment/4352f445-d10a-4f14-80aa-a5e4457042f2/am-newresearch-2022.pdf (accessed on 3 February 2023).
- Bertisch, S.M.; Herzig, S.J.; Winkelman, J.W.; Buettner, C. National use of prescription medications for insomnia: NHANES 1999–2010. Sleep 2014, 37, 343–349. [Google Scholar] [CrossRef]
- Roehrs, T.; Roth, T. ‘Hypnotic’ prescription patterns in a large managed-care population. Sleep Med. 2004, 5, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Madari, S.; Golebiowski, R.; Mansukhan, I.M.P.; Kolla, B.P. Pharmacological Management of Insomnia. Neurotherapeutics 2021, 18, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Clinical Guidelines Committee of the American College of Physicians. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef]
- Mysliwiec, V.; Martin, J.L.; Ulmer, C.S.; Chowdhuri, S.; Brock, M.S.; Spevak, C.; Sall, J. The Management of Chronic Insomnia Disorder and Obstructive Sleep Apnea: Synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guidelines. Ann Intern Med. 2020, 172, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Camargos, E.F.; Louzada, L.L.; Quintas, J.L.; Naves, J.O.; Louzada, F.M.; Nóbrega, O.T. Trazodone improves sleep parameters in Alzheimer disease patients: A randomized, double-blind, and placebo-controlled study. Am. J. Geriatr. Psychiatry 2014, 22, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Puzino, K.; Fernandez-Mendoza, J.; Krishnamurthy, V.B.; Basta, M.; Bixler, E.O. Effects of trazodone versus cognitive behavioral therapy in the insomnia with short sleep duration phenotype: A preliminary study. J. Clin. Sleep Med. 2020, 16, 2009–2019. [Google Scholar] [CrossRef]
- Morin, C.M.; Edinger, J.D.; Beaulieu-Bonneau, S.; Ivers, H.; Krystal, A.D.; Guay, B.; Bélanger, L.; Cartwright, A.; Simmons, B.; Lamy, M.; et al. Effectiveness of Sequential Psychological and Medication Therapies for Insomnia Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2020, 77, 1107–1115. [Google Scholar] [CrossRef]
- Amari, D.T.; Juday, T.R.; Frech, F.H.; Wang, W.; Gor, D.; Atkins, N., Jr.; Wickwire, E.M. Fall Risk, Healthcare Resource Use, and Costs Among Adult Patients in the United States Treated for Insomnia with Zolpidem, Trazodone, or Benzodiazepines: A Retrospective Cohort Study. Adv. Ther. 2022, 39, 1324–1340. [Google Scholar] [CrossRef]
- Haria, M.; Fitton, A.; McTavish, D. Trazodone. A review of its pharmacology, therapeutic use in depression and therapeutic potential in other disorders. Drugs Aging 1994, 4, 331–355. [Google Scholar] [CrossRef] [PubMed]
- Warner, M.D.; Peabody, C.A.; Whiteford, H.A.; Hollister, L.E. Trazodone and priapism. J. Clin. Psychiatry 1987, 48, 244–245. [Google Scholar] [PubMed]
- Shah, T.; Deolanker, J.; Luu, T.; Sadeghi-Nejad, H. Pretreatment screening and counseling on prolonged erections for patients prescribed trazodone. Investig. Clin. Urol. 2021, 62, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Practice Guideline for the Treatment of Patients with Major Depressive Disorder American Psychiatric Association: American Psychiatric Association. 2010. Available online: https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf (accessed on 10 December 2022).
- Hoffmann, P.; Neu, E.T.; Neu, D. Penile amputation after trazodone-induced priapism: A case report. Prim. Care Companion J. Clin. Psychiatry 2010, 12, 27092. [Google Scholar] [CrossRef] [PubMed]
- Matz, A.; Ambinder, D.; Spencer, E.; Phillips, J.; Wong, N.C. Review of Priapism Litigation in the United States. Urology 2021, 156, 169–172. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelayo, R.; Bertisch, S.M.; Morin, C.M.; Winkelman, J.W.; Zee, P.C.; Krystal, A.D. Should Trazodone Be First-Line Therapy for Insomnia? A Clinical Suitability Appraisal. J. Clin. Med. 2023, 12, 2933. https://doi.org/10.3390/jcm12082933
Pelayo R, Bertisch SM, Morin CM, Winkelman JW, Zee PC, Krystal AD. Should Trazodone Be First-Line Therapy for Insomnia? A Clinical Suitability Appraisal. Journal of Clinical Medicine. 2023; 12(8):2933. https://doi.org/10.3390/jcm12082933
Chicago/Turabian StylePelayo, Rafael, Suzanne M. Bertisch, Charles M. Morin, John W. Winkelman, Phyllis C. Zee, and Andrew D. Krystal. 2023. "Should Trazodone Be First-Line Therapy for Insomnia? A Clinical Suitability Appraisal" Journal of Clinical Medicine 12, no. 8: 2933. https://doi.org/10.3390/jcm12082933