
Recent Advances and Future Directions in Syncope Management: A Comprehensive Narrative Review
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
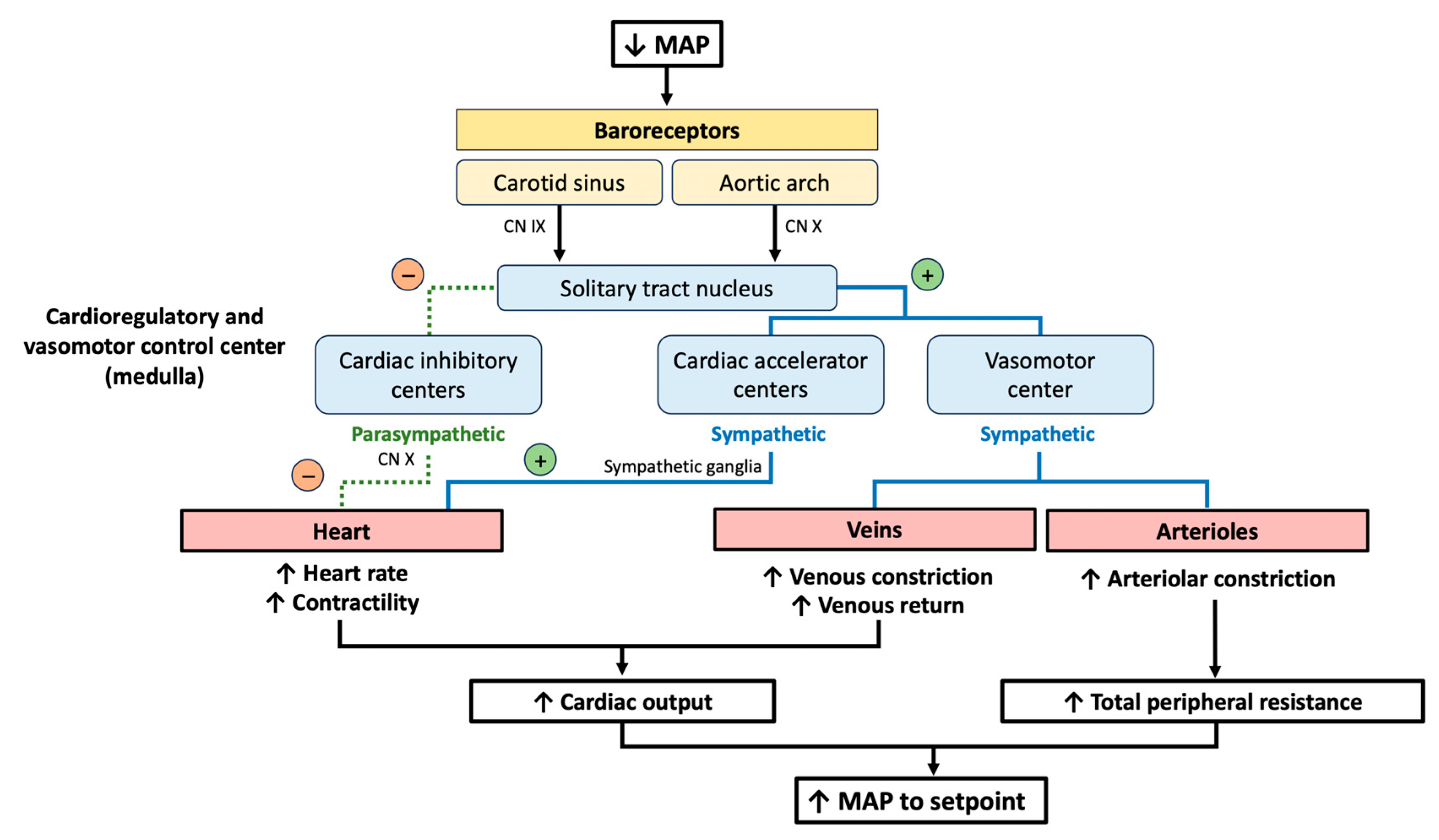
2. The Baroreceptor Reflex
3. Etiological Classification
3.1. Non-Cardiac Syncope
3.2. Cardiac Syncope
4. Diagnostic Approach
4.1. Initial Assessment
4.2. Differential Diagnoses
4.3. Risk Stratification
4.3.1. Diagnosis of Non-Cardiac Syncope
4.3.2. Diagnosis of Cardiac Syncope
5. Treatment
5.1. Treatment of Reflex Syncope
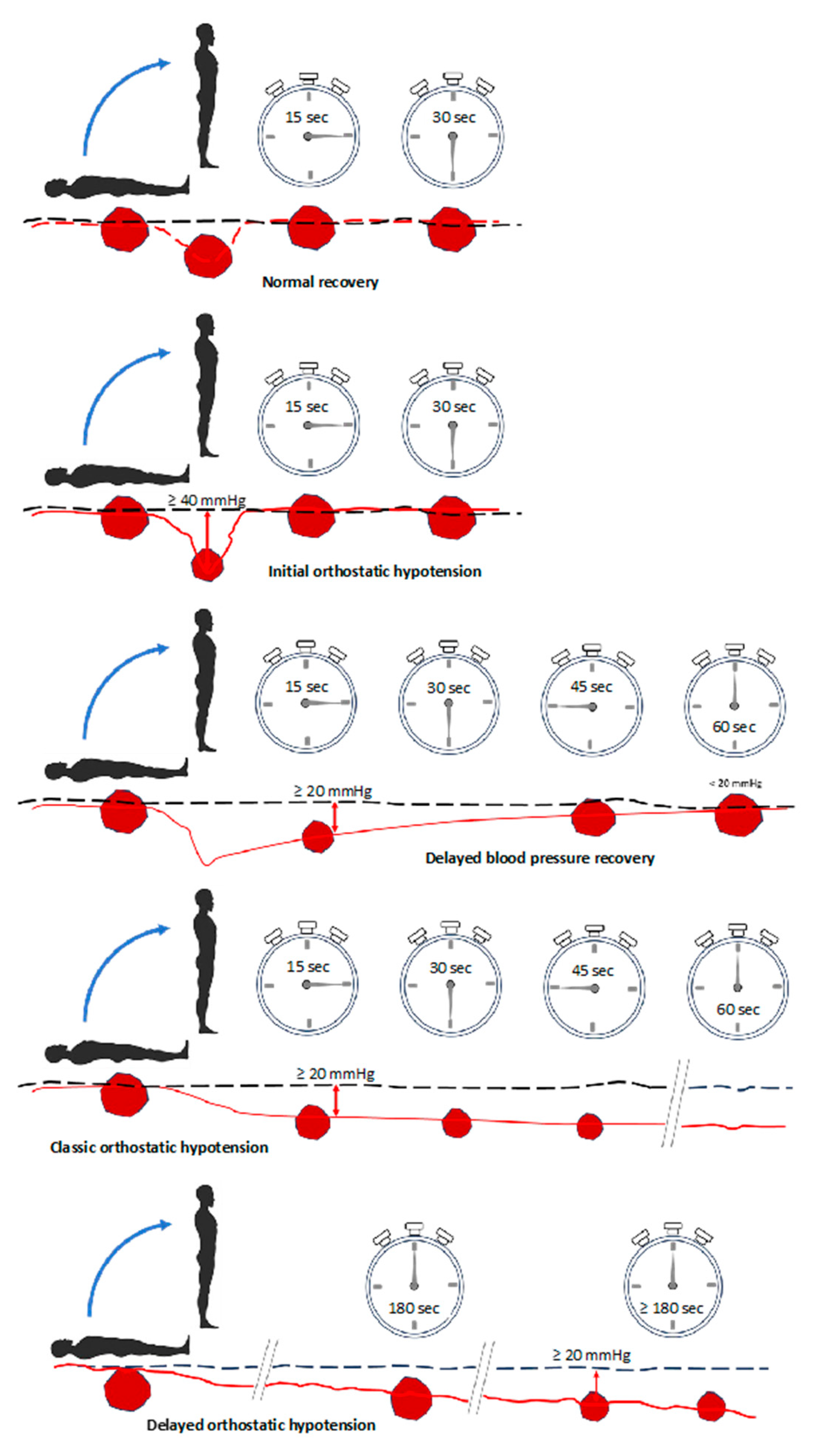
5.2. Treatment of Orthostatic Hypotension and Orthostatic Intolerance
5.3. Treatment of Cardiac Syncope
6. Management of Syncope in Older Adults
Syncope Unit
7. Future Directions in the Management of Syncope: A Little Help from New Technologies?
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martin, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Ruwald, M.H.; Hansen, M.L.; Lamberts, M.; Hansen, C.M.; Hojgaard, M.V.; Kober, L.; Torp-Pedersen, C.; Hansen, J.; Gislason, G.H. The relation between age, sex, comorbidity, and pharmacotherapy and the risk of syncope: A Danish nationwide study. Europace 2012, 14, 1506–1514. [Google Scholar] [CrossRef]
- Ganzeboom, K.S.; Mairuhu, G.; Reitsma, J.B.; Linzer, M.; Wieling, W.; van Dijk, N. Lifetime cumulative incidence of syncope in the general population: A study of 549 Dutch subjects aged 35–60 years. J. Cardiovasc. Electrophysiol. 2006, 17, 1172–1176. [Google Scholar] [CrossRef]
- Canakci, M.E.; Sevik, O.E.; Acar, N. How Should We Approach Syncope in the Emergency Department? Current Perspectives. Open Access Emerg. Med. 2022, 14, 299–309. [Google Scholar] [CrossRef]
- Probst, M.A.; Kanzaria, H.K.; Gbedemah, M.; Richardson, L.D.; Sun, B.C. National trends in resource utilization associated with ED visits for syncope. Am. J. Emerg. Med. 2015, 33, 998–1001. [Google Scholar] [CrossRef]
- Barbic, F.; Dipaola, F.; Casazza, G.; Borella, M.; Minonzio, M.; Solbiati, M.; Raj, S.R.; Sheldon, R.; Quinn, J.; Costantino, G.; et al. Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors. J. Clin. Med. 2019, 8, 150. [Google Scholar] [CrossRef]
- Saklani, P.; Krahn, A.; Klein, G. Syncope. Circulation 2013, 127, 1330–1339. [Google Scholar] [CrossRef]
- Torabi, P.; Rivasi, G.; Hamrefors, V.; Ungar, A.; Sutton, R.; Brignole, M.; Fedorowski, A. Early and late-onset syncope: Insight into mechanisms. Eur. Heart J. 2022, 43, 2116–2123. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2017, 136, e60–e122. [Google Scholar] [CrossRef] [PubMed]
- Numeroso, F.; Casagranda, I.; Lerza, R.; Ungar, A.; Gruppo Italiano Multidisciplinare per lo Studio della Sincope (GIMSI). Current ED syncope management in Italian hospitals and prospects for optimization: A national survey. Intern. Emerg. Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Van Wijnen, V.K.; Gans, R.O.B.; Wieling, W.; Ter Maaten, J.C.; Harms, M.P.M. Diagnostic accuracy of evaluation of suspected syncope in the emergency department: Usual practice vs. ESC guidelines. BMC Emerg. Med. 2020, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Ghitani, N.; Chesler, A.T. The anatomy of the baroreceptor reflex. Cell Rep. 2019, 29, 2121–2122. [Google Scholar] [CrossRef] [PubMed]
- Bencivenga, L.; De Souto Barreto, P.; Rolland, Y.; Hanon, O.; Vidal, J.S.; Cestac, P.; Vellas, B.; Rouch, L. Blood pressure variability: A potential marker of aging. Ageing Res. Rev. 2022, 80, 101677. [Google Scholar] [CrossRef] [PubMed]
- Schumann, A.; Gupta, Y.; Gerstorf, D.; Demuth, I.; Bar, K.J. Sex differences in the age-related decrease of spontaneous baroreflex function in healthy individuals. Am. J. Physiol. Heart Circ. Physiol. 2024, 326, H158–H165. [Google Scholar] [CrossRef] [PubMed]
- Tedla, Y.G.; Yano, Y.; Carnethon, M.; Greenland, P. Association Between Long-Term Blood Pressure Variability and 10-Year Progression in Arterial Stiffness: The Multiethnic Study of Atherosclerosis. Hypertension 2017, 69, 118–127. [Google Scholar] [CrossRef]
- Cremer, A.; Boutouyrie, P.; Laurent, S.; Gosse, P.; Tzourio, C. Orthostatic hypotension: A marker of blood pressure variability and arterial stiffness: A cross-sectional study on an elderly population: The 3-City study. J. Hypertens. 2020, 38, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P. Arterial Stiffness and Hypertension in the Elderly. Front. Cardiovasc. Med. 2020, 7, 544302. [Google Scholar] [CrossRef] [PubMed]
- Donato, A.J.; Machin, D.R.; Lesniewski, L.A. Mechanisms of Dysfunction in the Aging Vasculature and Role in Age-Related Disease. Circ. Res. 2018, 123, 825–848. [Google Scholar] [CrossRef]
- Zhou, T.L.; Henry, R.M.A.; Stehouwer, C.D.A.; van Sloten, T.T.; Reesink, K.D.; Kroon, A.A. Blood Pressure Variability, Arterial Stiffness, and Arterial Remodeling. Hypertension 2018, 72, 1002–1010. [Google Scholar] [CrossRef]
- Cacciatore, S.; Spadafora, L.; Bernardi, M.; Galli, M.; Betti, M.; Perone, F.; Nicolaio, G.; Marzetti, E.; Martone, A.M.; Landi, F.; et al. Management of Coronary Artery Disease in Older Adults: Recent Advances and Gaps in Evidence. J. Clin. Med. 2023, 12, 5233. [Google Scholar] [CrossRef]
- Palatini, P. Short-term blood pressure variability: Does its prognostic value increase with ageing? J. Hypertens. 2018, 36, 1795–1797. [Google Scholar] [CrossRef] [PubMed]
- Buto, M.S.S.; Catai, A.M.; Vassimon-Barroso, V.; Gois, M.O.; Porta, A.; Takahashi, A.C.M. Baroreflex sensitivity in frailty syndrome. Braz. J. Med. Biol. Res. 2019, 52, e8079. [Google Scholar] [CrossRef] [PubMed]
- Maciorowska, M.; Krzesinski, P.; Wierzbowski, R.; Uzieblo-Zyczkowska, B.; Gielerak, G. Associations between Heart Rate Variability Parameters and Hemodynamic Profiles in Patients with Primary Arterial Hypertension, Including Antihypertensive Treatment Effects. J. Clin. Med. 2022, 11, 3767. [Google Scholar] [CrossRef]
- Diaconu, C.C.; Cozma, M.A.; Dobrica, E.C.; Gheorghe, G.; Jichitu, A.; Ionescu, V.A.; Nicolae, A.C.; Dragoi, C.M.; Gaman, M.A. Polypharmacy in the Management of Arterial Hypertension-Friend or Foe? Medicina 2021, 57, 1288. [Google Scholar] [CrossRef]
- Coon, E.A.; Singer, W.; Low, P.A. Pure Autonomic Failure. Mayo Clin. Proc. 2019, 94, 2087–2098. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.S.; Dev, V.; Khandelwal, E. Cardiac Autonomic Neuropathy in Newly Diagnosed Patients with Type 2 Diabetes Mellitus. Cureus 2023, 15, e47366. [Google Scholar] [CrossRef]
- Gertz, M.A. Immunoglobulin light chain amyloidosis: 2024 update on diagnosis, prognosis, and treatment. Am. J. Hematol. 2023, 99, 309–324. [Google Scholar] [CrossRef]
- Underwood, C.F.; Hildreth, C.M.; Wyse, B.F.; Boyd, R.; Goodchild, A.K.; Phillips, J.K. Uraemia: An unrecognized driver of central neurohumoral dysfunction in chronic kidney disease? Acta Physiol. 2017, 219, 305–323. [Google Scholar] [CrossRef]
- Ortiz-Guzman, J.E.; Molla-Casanova, S.; Serra-Ano, P.; Arias-Mutis, O.J.; Calvo, C.; Bizy, A.; Alberola, A.; Chorro, F.J.; Zarzoso, M. Short-Term Heart Rate Variability in Metabolic Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6051. [Google Scholar] [CrossRef]
- Hashemi, D.; Blum, M.; Mende, M.; Stork, S.; Angermann, C.E.; Pankuweit, S.; Tahirovic, E.; Wachter, R.; Pieske, B.; Edelmann, F.; et al. Syncopes and clinical outcome in heart failure: Results from prospective clinical study data in Germany. ESC Heart Fail. 2020, 7, 942–952. [Google Scholar] [CrossRef]
- Ferreira, M.; Laranjo, S.; Cunha, P.; Geraldes, V.; Oliveira, M.; Rocha, I. Orthostatic Stress and Baroreflex Sensitivity: A Window into Autonomic Dysfunction in Lone Paroxysmal Atrial Fibrillation. J. Clin. Med. 2023, 12, 5857. [Google Scholar] [CrossRef]
- Saramet, E.E.; Pomirleanu, C.; Mastaleru, A.; Oancea, A.; Cojocaru, D.C.; Russu, M.; Negru, R.D.; Ancuta, C. Autonomic Dysfunction and Cardiovascular Risk in Patients with Rheumatoid Arthritis: Can Heart Rate Variability Analysis Contribute to a Better Evaluation of the Cardiovascular Profile of a Patient? J. Clin. Med. 2023, 12, 7736. [Google Scholar] [CrossRef]
- Bhanu, C.; Nimmons, D.; Petersen, I.; Orlu, M.; Davis, D.; Hussain, H.; Magammanage, S.; Walters, K. Drug-induced orthostatic hypotension: A systematic review and meta-analysis of randomised controlled trials. PLoS Med. 2021, 18, e1003821. [Google Scholar] [CrossRef]
- Scala, I.; Rizzo, P.A.; Bellavia, S.; Brunetti, V.; Colo, F.; Broccolini, A.; Della Marca, G.; Calabresi, P.; Luigetti, M.; Frisullo, G. Autonomic Dysfunction during Acute SARS-CoV-2 Infection: A Systematic Review. J. Clin. Med. 2022, 11, 3883. [Google Scholar] [CrossRef] [PubMed]
- Jamal, S.M.; Landers, D.B.; Hollenberg, S.M.; Turi, Z.G.; Glotzer, T.V.; Tancredi, J.; Parrillo, J.E. Prospective Evaluation of Autonomic Dysfunction in Post-Acute Sequela of COVID-19. J. Am. Coll. Cardiol. 2022, 79, 2325–2330. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Wang, H.; Kline, G.; Ding, Y.; Ross, S.E.; Davis, S.; Mallet, R.T.; Shi, X. Habitual physical activity improves vagal cardiac modulation and carotid baroreflex function in elderly women. Exp. Biol. Med. 2023, 248, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Massimo Massetti, M.; Rambaldi, P.; Gatta, G.; Cappabianca, S.; Sasso, F.C.; Santamaria, M.; Volpicelli, M.; Ducceschi, V.; Signoriello, G.; et al. SGLT2-inhibitors reduce the cardiac autonomic neuropathy dysfunction and vaso-vagal syncope recurrence in patients with type 2 diabetes mellitus: The SCAN study. Metabolism 2022, 137, 155243. [Google Scholar] [CrossRef] [PubMed]
- Balcioglu, A.S.; Celik, E.; Aksu, E.; Aykan, A.C. Impact of Sodium-Glucose Cotransporter-2 Inhibitors on Sympathetic Nervous System Activity Detected by Sympathetic Activity Index and LF/HF Ratio in Patients with Type 2 Diabetes Mellitus. Turk. Kardiyol. Dern. Ars. 2022, 50, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Lim, V.G.; He, H.; Lachlan, T.; Ng, G.A.; Kyrou, I.; Randeva, H.S.; Osman, F. Impact of sodium-glucose co-transporter inhibitors on cardiac autonomic function and mortality: No time to die. Europace 2022, 24, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Vernino, S.; Bourne, K.M.; Stiles, L.E.; Grubb, B.P.; Fedorowski, A.; Stewart, J.M.; Arnold, A.C.; Pace, L.A.; Axelsson, J.; Boris, J.R.; et al. Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting—Part 1. Auton. Neurosci. 2021, 235, 102828. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Rivasi, G.; Sutton, R.; Kenny, R.A.; Morillo, C.A.; Sheldon, R.; Raj, S.R.; Ungar, A.; Furlan, R.; van Dijk, G.; et al. Low-blood pressure phenotype underpins the tendency to reflex syncope. J. Hypertens. 2021, 39, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Rivasi, G. New insights in diagnostics and therapies in syncope: A novel approach to non-cardiac syncope. Heart 2021, 107, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Rivasi, G.; Ungar, A.; Moya, A.; Brignole, M.; Sutton, R.; Fedorowski, A. Syncope: New solutions for an old problem. Kardiol. Pol. 2021, 79, 1068–1078. [Google Scholar] [CrossRef] [PubMed]
- Francisco Pascual, J.; Jordan Marchite, P.; Rodriguez Silva, J.; Rivas Gandara, N. Arrhythmic syncope: From diagnosis to management. World J. Cardiol. 2023, 15, 119–141. [Google Scholar] [CrossRef] [PubMed]
- Koene, R.J.; Adkisson, W.O.; Benditt, D.G. Syncope and the risk of sudden cardiac death: Evaluation, management, and prevention. J. Arrhythm. 2017, 33, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Francis-Morel, G. Impact of Admission of Patients With Syncope in Non-Teaching Hospitals Versus Teaching Hospitals: A Nationwide Analysis. Cureus 2023, 15, e39545. [Google Scholar] [CrossRef] [PubMed]
- Joy, P.S.; Kumar, G.; Olshansky, B. Syncope: Outcomes and Conditions Associated with Hospitalization. Am. J. Med. 2017, 130, 699–706.e6. [Google Scholar] [CrossRef] [PubMed]
- Tajdini, M.; Khalaji, A.; Behnoush, A.H.; Tavolinejad, H.; Jalali, A.; Sadeghian, S.; Vasheghani-Farahani, A.; Yadangi, S.; Masoudkabir, F.; Bozorgi, A. Brain MRI and EEG overemployment in patients with vasovagal syncope: Results from a tertiary syncope unit. BMC Cardiovasc. Disord. 2023, 23, 576. [Google Scholar] [CrossRef]
- Costantino, G.; Dipaola, F.; Solbiati, M.; Bulgheroni, M.; Barbic, F.; Furlan, R. Is hospital admission valuable in managing syncope? Results from the STePS study. Cardiol. J. 2014, 21, 606–610. [Google Scholar] [CrossRef]
- Wood, B.S.; Craig, M.J.; Williamson, M.; Gehi, A.K. A Systematic Emergency Department Care Protocol for Syncope Patients Reduces Admissions. Am. J. Cardiol. 2023, 202, 160–162. [Google Scholar] [CrossRef]
- Mechanic, O.J.; Pascheles, C.Y.; Lopez, G.J.; Winans, A.M.; Shapiro, N.I.; Tibbles, C.; Wolfe, R.E.; Grossman, S.A. Using the Boston Syncope Observation Management Pathway to Reduce Hospital Admission and Adverse Outcomes. West. J. Emerg. Med. 2019, 20, 250–255. [Google Scholar] [CrossRef]
- Bayard, M.; Gerayli, F.; Holt, J. Syncope: Evaluation and Differential Diagnosis. Am. Fam. Physician 2023, 108, 454–463. [Google Scholar]
- France, C.R.; France, J.L.; Conatser, R.; Lux, P.; McCullough, J.; Erickson, Y. Predonation fears identify young donors at risk for vasovagal reactions. Transfusion 2019, 59, 2870–2875. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, C.; McCrory, C.; O’Leary, N.; O’Brien, H.; Kenny, R.A. Childhood trauma and lifetime syncope burden among older adults. J. Psychosom. Res. 2017, 97, 63–69. [Google Scholar] [CrossRef]
- Russo, V.; AlTurki, A.; Rago, A.; Proietti, R.; Chausse, G.; Monteleone, A.M.; Scognamiglio, P.; Monteleone, P.; Nigro, G. Temperament and character personality dimensions in nitrate-tilt-induced vasovagal syncope patients. Hellenic J. Cardiol. 2017, 58, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Sheldon, R.S.; Ritchie, D.; Raj, V.; Raj, S.R. Reduced quality of life and greater psychological distress in vasovagal syncope patients compared to healthy individuals. Pacing Clin. Electrophysiol. 2019, 42, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Atici, A.; Asoglu, R.; Demirkiran, A.; Serbest, N.G.; Emektas, B.; Sarikaya, R.; Yeldan, I.; Bilge, A.K. The relationship between clinical characteristics and psychological status and quality of life in patients with vasovagal syncope. North. Clin. Istanb. 2020, 7, 237–245. [Google Scholar] [CrossRef]
- Sutton, R.; Ricci, F.; Fedorowski, A. Risk stratification of syncope: Current syncope guidelines and beyond. Auton. Neurosci. 2021, 238, 102929. [Google Scholar] [CrossRef]
- Martin, T.P.; Hanusa, B.H.; Kapoor, W.N. Risk stratification of patients with syncope. Ann. Emerg. Med. 1997, 29, 459–466. [Google Scholar] [CrossRef]
- Colivicchi, F.; Ammirati, F.; Melina, D.; Guido, V.; Imperoli, G.; Santini, M.; Investigators, O.S. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: The OESIL risk score. Eur. Heart J. 2003, 24, 811–819. [Google Scholar] [CrossRef]
- Quinn, J.; McDermott, D.; Stiell, I.; Kohn, M.; Wells, G. Prospective validation of the San Francisco Syncope Rule to predict patients with serious outcomes. Ann. Emerg. Med. 2006, 47, 448–454. [Google Scholar] [CrossRef]
- Probst, M.A.; Gibson, T.; Weiss, R.E.; Yagapen, A.N.; Malveau, S.E.; Adler, D.H.; Bastani, A.; Baugh, C.W.; Caterino, J.M.; Clark, C.L.; et al. Risk Stratification of Older Adults Who Present to the Emergency Department With Syncope: The FAINT Score. Ann. Emerg. Med. 2020, 75, 147–158. [Google Scholar] [CrossRef]
- Zimmermann, T.; du Fay de Lavallaz, J.; Walter, J.E.; Strebel, I.; Nestelberger, T.; Joray, L.; Badertscher, P.; Flores, D.; Widmer, V.; Geigy, N.; et al. Development of an electrocardiogram-based risk calculator for a cardiac cause of syncope. Heart 2021, 107, 1796–1804. [Google Scholar] [CrossRef]
- de Sousa Bispo, J.; Azevedo, P.; Mota, T.; Fernandes, R.; Guedes, J.; Candeias, R.; Marques, N.S.; Camacho, A.; Jesus, I. EGSYS score for the prediction of cardiac etiology in syncope: Is it useful in an outpatient setting? Rev. Port. Cardiol. 2020, 39, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Claesson, J.E.; Kristensson, B.E.; Edvardsson, N.; Wahrborg, P. Less syncope and milder symptoms in patients treated with pacing for induced cardioinhibitory carotid sinus syndrome: A randomized study. Europace 2007, 9, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Fischer, C.; Lipsitz, L.A.; Mottley, L.; Sands, K.; Thompson, S.; Zimetbaum, P.; Shapiro, N.I. Predicting adverse outcomes in syncope. J. Emerg. Med. 2007, 33, 233–239. [Google Scholar] [CrossRef]
- Brignole, M.; Kessisoglu, F.; Croci, F.; Solano, A.; Donateo, P.; Maggi, R.; Solari, D.; Bertolone, C.; Fontana, D.; Oddone, D.; et al. Complementary effectiveness of carotid sinus massage and tilt testing for the diagnosis of reflex syncope in patients older than 40 years: A cohort study. Europace 2020, 22, 1737–1741. [Google Scholar] [CrossRef]
- Kerr, S.R.; Pearce, M.S.; Brayne, C.; Davis, R.J.; Kenny, R.A. Carotid sinus hypersensitivity in asymptomatic older persons: Implications for diagnosis of syncope and falls. Arch. Intern. Med. 2006, 166, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Ungar, A.; Rivasi, G.; Rafanelli, M.; Toffanello, G.; Mussi, C.; Ceccofiglio, A.; McDonagh, R.; Drumm, B.; Marchionni, N.; Alboni, P.; et al. Safety and tolerability of Tilt Testing and Carotid Sinus Massage in the octogenarians. Age Ageing 2016, 45, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Menozzi, C.; Lolli, G.; Bottoni, N.; Gaggioli, G. Long-term outcome of paced and nonpaced patients with severe carotid sinus syndrome. Am. J. Cardiol. 1992, 69, 1039–1043. [Google Scholar] [CrossRef]
- Menozzi, C.; Brignole, M.; Lolli, G.; Bottoni, N.; Oddone, D.; Gianfranchi, L.; Gaggioli, G. Follow-up of asystolic episodes in patients with cardioinhibitory, neurally mediated syncope and VVI pacemaker. Am. J. Cardiol. 1993, 72, 1152–1155. [Google Scholar] [CrossRef]
- Maggi, R.; Menozzi, C.; Brignole, M.; Podoleanu, C.; Iori, M.; Sutton, R.; Moya, A.; Giada, F.; Orazi, S.; Grovale, N. Cardioinhibitory carotid sinus hypersensitivity predicts an asystolic mechanism of spontaneous neurally mediated syncope. Europace 2007, 9, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Harms, M.P.M.; Finucane, C.; Perez-Denia, L.; Juraschek, S.P.; van Wijnen, V.K.; Lipsitz, L.A.; van Lieshout, J.J.; Wieling, W. Systemic and cerebral circulatory adjustment within the first 60 s after active standing: An integrative physiological view. Auton. Neurosci. 2021, 231, 102756. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Rivasi, G.; Fedorowski, A.; Stahlberg, M.; Groppelli, A.; Ungar, A. Tests for the identification of reflex syncope mechanism. Expert. Rev. Med. Devices 2023, 20, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Flevari, P.; Leftheriotis, D.; Komborozos, C.; Fountoulaki, K.; Dagres, N.; Theodorakis, G.; Kremastinos, D. Recurrent vasovagal syncope: Comparison between clomipramine and nitroglycerin as drug challenges during head-up tilt testing. Eur. Heart J. 2009, 30, 2249–2253. [Google Scholar] [CrossRef] [PubMed]
- Ungar, A.; Sgobino, P.; Russo, V.; Vitale, E.; Sutton, R.; Melissano, D.; Beiras, X.; Bottoni, N.; Ebert, H.H.; Gulizia, M.; et al. Diagnosis of neurally mediated syncope at initial evaluation and with tilt table testing compared with that revealed by prolonged ECG monitoring. An analysis from the Third International Study on Syncope of Uncertain Etiology (ISSUE-3). Heart 2013, 99, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, J.G.; van Rossum, I.A.; Thijs, R.D. The pathophysiology of vasovagal syncope: Novel insights. Auton. Neurosci. 2021, 236, 102899. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, J.G.; Ghariq, M.; Kerkhof, F.I.; Reijntjes, R.; van Houwelingen, M.J.; van Rossum, I.A.; Saal, D.P.; van Zwet, E.W.; van Lieshout, J.J.; Thijs, R.D.; et al. Novel Methods for Quantification of Vasodepression and Cardioinhibition During Tilt-Induced Vasovagal Syncope. Circ. Res. 2020, 127, e126–e138. [Google Scholar] [CrossRef]
- Van Dijk, J.G.; van Rossum, I.A.; van Houwelingen, M.; Ghariq, M.; Saal, D.P.; de Lange, F.J.; Thijs, R.D.; Sutton, R.; Benditt, D.G. Influence of Age on Magnitude and Timing of Vasodepression and Cardioinhibition in Tilt-Induced Vasovagal Syncope. JACC Clin. Electrophysiol. 2022, 8, 997–1009. [Google Scholar] [CrossRef]
- Rivasi, G.; Groppelli, A.; Brignole, M.; Soranna, D.; Zambon, A.; Bilo, G.; Pengo, M.; Sharad, B.; Hamrefors, V.; Rafanelli, M.; et al. Association between hypotension during 24 h ambulatory blood pressure monitoring and reflex syncope: The SynABPM 1 study. Eur. Heart J. 2022, 43, 3765–3776. [Google Scholar] [CrossRef]
- Freund, O.; Caspi, I.; Shacham, Y.; Frydman, S.; Biran, R.; Abu Katash, H.; Zornitzki, L.; Bornstein, G. Holter ECG for Syncope Evaluation in the Internal Medicine Department-Choosing the Right Patients. J. Clin. Med. 2022, 11, 4781. [Google Scholar] [CrossRef]
- Yasa, E.; Intzilakis, T.; Ricci, F.; Melander, O.; Hamrefors, V.; Sutton, R.; Fedorowski, A. Outcomes of Primary vs. Delayed Strategy of Implanting a Cardiac Monitor for Unexplained Syncope. J. Clin. Med. 2022, 11, 1819. [Google Scholar] [CrossRef]
- Doundoulakis, I.; Soulaidopoulos, S.; Arsenos, P.; Dilaveris, P.; Tsiachris, D.; Antoniou, C.-K.; Sideris, S.; Kordalis, A.; Laina, A.; Kallinikidis, S.; et al. Unexplained Syncope: The Importance of the Electrophysiology Study. Hearts 2021, 2, 495–504. [Google Scholar] [CrossRef]
- Ghani, A.R.; Ullah, W.; Abdullah, H.M.A.; Sattar, Y.; Sarwar, U.; Ahsan, I.; Humayun, W. The role of echocardiography in diagnostic evaluation of patients with syncope-a retrospective analysis. Am. J. Cardiovasc. Dis. 2019, 9, 78–83. [Google Scholar] [PubMed]
- Lacewell, A.N.; Buck, T.M.; Romero, S.A.; Halliwill, J.R. Postexercise syncope: Wingate syncope test and effective countermeasure. Exp. Physiol. 2014, 99, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Jang, H.J.; Kim, S.; Cho, S.Y.; Song, K.S.; Pickett, C.; Schmitt, H.J.; Lee, J. A new test for diagnosing vasovagal syncope: Standing after treadmill test with sublingual nitrate administration. PLoS ONE 2017, 12, e0179631. [Google Scholar] [CrossRef] [PubMed]
- Mitrani, R.D.; Hendel, R.C. The appropriateness of an ischemia evaluation for syncope. Circ. Cardiovasc. Imaging 2013, 6, 358–359. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, P.; Dell’Era, G.; Pellegrino, P.L.; Ammendola, E.; Ziacchi, M.; Guerra, F.; Aspromonte, V.; Laffi, M.; Pimpini, L.; Santoro, F.; et al. Causes of syncopal recurrences in patients treated with permanent pacing for bradyarrhythmic syncope: Findings from the SYNCOPACED registry. Heart Rhythm. 2021, 18, 770–777. [Google Scholar] [CrossRef]
- Fedorowski, A.; Ricci, F.; Hamrefors, V.; Sandau, K.E.; Hwan Chung, T.; Muldowney, J.A.S.; Gopinathannair, R.; Olshansky, B. Orthostatic Hypotension: Management of a Complex, But Common, Medical Problem. Circ. Arrhythm. Electrophysiol. 2022, 15, e010573. [Google Scholar] [CrossRef] [PubMed]
- Aydin, M.A.; Salukhe, T.V.; Wilke, I.; Willems, S. Management and therapy of vasovagal syncope: A review. World J. Cardiol. 2010, 2, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Behnoush, A.H.; Yazdani, K.; Khalaji, A.; Tavolinejad, H.; Aminorroaya, A.; Jalali, A.; Tajdini, M. Pharmacologic prevention of recurrent vasovagal syncope: A systematic review and network meta-analysis of randomized controlled trials. Heart Rhythm. 2023, 20, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Sutton, R.; de Jong, J.S.Y.; Stewart, J.M.; Fedorowski, A.; de Lange, F.J. Pacing in vasovagal syncope: Physiology, pacemaker sensors, and recent clinical trials-Precise patient selection and measurable benefit. Heart Rhythm. 2020, 17, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Pachon, J.C.; Pachon, E.I.; Pachon, J.C.; Lobo, T.J.; Pachon, M.Z.; Vargas, R.N.; Jatene, A.D. “Cardioneuroablation”--new treatment for neurocardiogenic syncope, functional AV block and sinus dysfunction using catheter RF-ablation. Europace 2005, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vandenberk, B.; Lei, L.Y.; Ballantyne, B.; Vickers, D.; Liang, Z.; Sheldon, R.S.; Chew, D.S.; Aksu, T.; Raj, S.R.; Morillo, C.A. Cardioneuroablation for vasovagal syncope: A systematic review and meta-analysis. Heart Rhythm. 2022, 19, 1804–1812. [Google Scholar] [CrossRef] [PubMed]
- Pachon, M.J.; Pachon, M.E.; Pachon, C.T.C.; Santillana, P.T.; Lobo, T.J.; Pachon, M.J.; Higuti, C.; Zerpa, A.J.; Pachon, M.Z.C.; Ortencio, F.A.; et al. Long-term outcomes of cardioneuroablation with and without extra-cardiac vagal stimulation confirmation in severe cardioinhibitory neurocardiogenic syncope. J. Cardiovasc. Electrophysiol. 2024, 42, 821–829. [Google Scholar] [CrossRef]
- Brignole, M.; Aksu, T.; Calo, L.; Debruyne, P.; Deharo, J.C.; Fanciulli, A.; Fedorowski, A.; Kulakowski, P.; Morillo, C.; Moya, A.; et al. Clinical controversy: Methodology and indications of cardioneuroablation for reflex syncope. Europace 2023, 25, euad033. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, R.S.; Raj, S.R. Cardioneuroablation for vasovagal syncope: Sober second thoughts. Heart Rhythm. 2023. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, A.; Abdelazeim, B.; Mattar, O.; Gadelkarim, M.; Salah, R.; Negida, A. Meta-analysis of the safety and efficacy of droxidopa for neurogenic orthostatic hypotension. Clin. Auton. Res. 2016, 26, 171–180. [Google Scholar] [CrossRef]
- Kaufmann, H.; Norcliffe-Kaufmann, L.; Palma, J.A. Droxidopa in neurogenic orthostatic hypotension. Expert. Rev. Cardiovasc. Ther. 2015, 13, 875–891. [Google Scholar] [CrossRef]
- Biaggioni, I.; Arthur Hewitt, L.; Rowse, G.J.; Kaufmann, H. Integrated analysis of droxidopa trials for neurogenic orthostatic hypotension. BMC Neurol. 2017, 17, 90. [Google Scholar] [CrossRef]
- Amjad, F.; Polenchar, B.; Favit, A. Droxidopa Persistence in Neurogenic Orthostatic Hypotension May Be Affected by Titration Approach. Int. J. Gen. Med. 2021, 14, 4485–4490. [Google Scholar] [CrossRef]
- Hauser, R.A.; Favit, A.; Hewitt, L.A.; Lindsten, A.; Gorny, S.; Kymes, S.; Isaacson, S.H. Durability of the Clinical Benefit of Droxidopa for Neurogenic Orthostatic Hypotension During 12 Weeks of Open-Label Treatment. Neurol. Ther. 2022, 11, 459–469. [Google Scholar] [CrossRef]
- Ungar, A.; Mussi, C.; Del Rosso, A.; Noro, G.; Abete, P.; Ghirelli, L.; Cellai, T.; Landi, A.; Salvioli, G.; Rengo, F.; et al. Diagnosis and characteristics of syncope in older patients referred to geriatric departments. J. Am. Geriatr. Soc. 2006, 54, 1531–1536. [Google Scholar] [CrossRef]
- Galizia, G.; Abete, P.; Mussi, C.; Noro, G.; Morrione, A.; Langellotto, A.; Landi, A.; Cacciatore, F.; Masotti, G.; Rengo, F.; et al. Role of early symptoms in assessment of syncope in elderly people: Results from the Italian group for the study of syncope in the elderly. J. Am. Geriatr. Soc. 2009, 57, 18–23. [Google Scholar] [CrossRef]
- Chiara, M.; Gianluigi, G.; Pasquale, A.; Alessandro, M.; Alice, M.; Gabriele, N.; Paolo, C.; Loredana, G.; Giovanni, T.; Franco, R.; et al. Unexplained Falls Are Frequent in Patients with Fall-Related Injury Admitted to Orthopaedic Wards: The UFO Study (Unexplained Falls in Older Patients). Curr. Gerontol. Geriatr. Res. 2013, 2013, 928603. [Google Scholar] [CrossRef]
- Ungar, A.; Mussi, C.; Nicosia, F.; Ceccofiglio, A.; Bellelli, G.; Bo, M.; Riccio, D.; Landi, F.; Martone, A.M.; Langellotto, A.; et al. The “syncope and dementia” study: A prospective, observational, multicenter study of elderly patients with dementia and episodes of “suspected” transient loss of consciousness. Aging Clin. Exp. Res. 2015, 27, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.; Gallagher, C.; Linz, D.; Elliott, A.D.; Emami, M.; Kadhim, K.; Mishima, R.; Hendriks, J.M.L.; Mahajan, R.; Arnolda, L.; et al. Atrial Fibrillation Is Associated With Syncope and Falls in Older Adults: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 676–687. [Google Scholar] [CrossRef] [PubMed]
- Francisco-Pascual, J.; Rivas-Gandara, N. Syncope in Patients With Aortic Stenosis: Does Investigating the Cause Affect Prognosis? Can. J. Cardiol. 2023, 39, 909. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, F.; Colaceci, R.; Cesario, A.; Strano, S.; Della Scala, A.; Colangelo, I.; De Santo, T.; Toscano, E.; Ricci, R.; Santini, M. Management of syncope: Clinical and economic impact of a Syncope Unit. Europace 2008, 10, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Van Zanten, S.; de Jong, J.S.Y.; Scheffer, M.G.; Kaal, E.C.A.; de Groot, J.R.; de Lange, F.J. A cross-sectional nationwide survey of guideline based syncope units in the Netherlands: The SU-19 score-a novel validation for best practices. Europace 2023, 26, euae002. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, T.; D’Ascenzo, F.; Pepe, M.; Bonsignore Zanghi, S.; Bernardi, M.; Spadafora, L.; Frati, G.; Peruzzi, M.; De Ferrari, G.M.; Biondi-Zoccai, G. Unsupervised Machine Learning with Cluster Analysis in Patients Discharged after an Acute Coronary Syndrome: Insights from a 23,270-Patient Study. Am. J. Cardiol. 2023, 193, 44–51. [Google Scholar] [CrossRef]
- Statz, G.M.; Evans, A.Z.; Johnston, S.L.; Adhaduk, M.; Mudireddy, A.R.; Sonka, M.; Lee, S.; Barsotti, E.J.; Ricci, F.; Dipaola, F.; et al. Can Artificial Intelligence Enhance Syncope Management? JACC Adv. 2023, 2, 100323. [Google Scholar] [CrossRef]
- Dipaola, F.; Shiffer, D.; Gatti, M.; Mene, R.; Solbiati, M.; Furlan, R. Machine Learning and Syncope Management in the ED: The Future Is Coming. Medicina 2021, 57, 351. [Google Scholar] [CrossRef]
- Goh, C.H.; Ferdowsi, M.; Gan, M.H.; Kwan, B.H.; Lim, W.Y.; Tee, Y.K.; Rosli, R.; Tan, M.P. Assessing the efficacy of machine learning algorithms for syncope classification: A systematic review. MethodsX 2024, 12, 102508. [Google Scholar] [CrossRef] [PubMed]
- Everson, J.; Adler-Milstein, J. Sharing information electronically with other hospitals is associated with increased sharing of patients. Health Serv. Res. 2020, 55, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Everson, J.; Adler-Milstein, J. Gaps in health information exchange between hospitals that treat many shared patients. J. Am. Med. Inform. Assoc. 2018, 25, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Warren, L.R.; Clarke, J.; Arora, S.; Darzi, A. Improving data sharing between acute hospitals in England: An overview of health record system distribution and retrospective observational analysis of inter-hospital transitions of care. BMJ Open 2019, 9, e031637. [Google Scholar] [CrossRef] [PubMed]
- Spadafora, L.; Comandini, G.L.; Giordano, S.; Polimeni, A.; Perone, F.; Sabouret, P.; Leonetti, M.; Cacciatore, S.; Cacia, M.; Betti, M.; et al. Blockchain technology in Cardiovascular Medicine: A glance to the future? Results from a social media survey and future perspectives. Minerva Cardiol. Angiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C.; Aydar, M.; Hassan Virk, H.U.; Kumar, A.; Kaplin, S.; Guimaraes, L.; Wang, Z.; Halperin, J.L. Artificial Intelligence-Powered Blockchains for Cardiovascular Medicine. Can. J. Cardiol. 2022, 38, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Ojha, U.; Ayathamattam, J.; Okonkwo, K.; Ogunmwonyi, I. Recent Updates and Technological Developments in Evaluating Cardiac Syncope in the Emergency Department. Curr. Cardiol. Rev. 2022, 18, e210422203887. [Google Scholar] [CrossRef] [PubMed]
- Duncker, D.; Ding, W.Y.; Etheridge, S.; Noseworthy, P.A.; Veltmann, C.; Yao, X.; Bunch, T.J.; Gupta, D. Smart Wearables for Cardiac Monitoring-Real-World Use beyond Atrial Fibrillation. Sensors 2021, 21, 2539. [Google Scholar] [CrossRef] [PubMed]
- Groppelli, A.; Rafanelli, M.; Testa, G.D.; Agusto, S.; Rivasi, G.; Ungar, A.; Carbone, E.; Soranna, D.; Zambon, A.; Brignole, M.; et al. Feasibility of Blood Pressure Measurement With a Wearable (Watch-Type) Monitor During Impending Syncopal Episodes. J. Am. Heart Assoc. 2022, 11, e026420. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subtype | Etiology | Features |
|---|---|---|
| Vasovagal | Emotional distress (e.g., pain and fear). | Usually occurs at a younger age |
| Situational | Coughing, sneezing, swallowing, defecation, and micturition after exercise | |
| Carotid sinus syndrome | Vagal hyperactivation due to accidental stimulation of carotid sinus baroreceptors | People ≥ 40 years old with increased baroreceptor sensitivity due to atherosclerosis and arterial stiffness |
| Atypical forms | No identifiable triggers |
| Syncope | Epilepsy |
|---|---|
| Before TLOC | |
|
|
| During TLOC | |
Myoclonia (rare, <60% of cases)
|
|
| After TLOC | |
|
|
| Other features | |
| Fecal/urine release, open eyes during TLOC, fatigue, and sleepiness are common in both conditions. Cyanotic face is common in epilepsy but rare in syncope | |
| High-Risk Syncope |
|
| Low-risk syncope |
|
| Test | Method | Results |
| Active standing test | Measure the BP in clinostatism and after rapid orthostatism at minute 0, minute 1, and minute 3 |
|
| Tilt test |
|
|
| Valsalva maneuver | Indicated in patients with suspected reflex syncope or to confirm the tendency of hypotension induced by situational syncope | Results can help diagnose neurogenic syncope or confirm hypotension tendency induced with situational syncope |
| Deep breathing test | Indicated in patients with OH of suspected neurogenic origin | Results can provide information about reflex syncope |
| ABPM | Identifies any drops in BP occurring in the 24 h. | Can identify different patterns: dipping (BP falls > 10% at night compared with daytime) or non-dipping (BP falls < 10% at night), or reverse dipping (BP rises at night) |
| Test | Methods | Results |
| Telemetry ECG monitoring | Used in the acute phase (within 72 h after TLOC) in high-risk patients |
|
| 24-h Holter ECG | Indicated in patients with very frequent syncope or presyncope (>1/week) |
|
| Event recorder | External
|
|
| EPS | Recommended for:
|
|
| Echocardiography | Useful for diagnosing structural heart disease and assessing the prognosis |
|
| Exercise testing | Indicated in patients with syncope on exertion | Positive if syncope is reproduced during or immediately after exertion with associated ECG changes. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martone, A.M.; Parrini, I.; Ciciarello, F.; Galluzzo, V.; Cacciatore, S.; Massaro, C.; Giordano, R.; Giani, T.; Landi, G.; Gulizia, M.M.; et al. Recent Advances and Future Directions in Syncope Management: A Comprehensive Narrative Review. J. Clin. Med. 2024, 13, 727. https://doi.org/10.3390/jcm13030727
Martone AM, Parrini I, Ciciarello F, Galluzzo V, Cacciatore S, Massaro C, Giordano R, Giani T, Landi G, Gulizia MM, et al. Recent Advances and Future Directions in Syncope Management: A Comprehensive Narrative Review. Journal of Clinical Medicine. 2024; 13(3):727. https://doi.org/10.3390/jcm13030727
Chicago/Turabian StyleMartone, Anna Maria, Iris Parrini, Francesca Ciciarello, Vincenzo Galluzzo, Stefano Cacciatore, Claudia Massaro, Rossella Giordano, Tommaso Giani, Giovanni Landi, Michele Massimo Gulizia, and et al. 2024. "Recent Advances and Future Directions in Syncope Management: A Comprehensive Narrative Review" Journal of Clinical Medicine 13, no. 3: 727. https://doi.org/10.3390/jcm13030727