

The Skeletal Stability of Combined Surgery First Approach and Clear Aligners in Skeletal Class III Malocclusion Correction: A Randomized Controlled Trial
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Interventions
2.2.1. Experimental Group
2.2.2. Control Group
2.3. Stability Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baik, H.S.; Han, H.K.; Kim, D.J.; Proffit, W.R. Cephalometric characteristics of Korean Class III surgical patients and their relationship to plans for surgical treatment. Int. J. Adult Orthod. Orthognath. Surg. 2000, 15, 119–128. [Google Scholar]
- Insawak, R.; Lin, C.-H.; Chen, Y.-A.; Ko, E.W.-C. Comparison of 3-dimensional postoperative dental movement in Class III surgical correction with and without presurgical orthodontic treatment. Biomed. J. 2020, 44, S282–S295. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Yang, Z.; Qi, Y.; Peng, J.; Li, Z.; Liu, X.; Yi, B.; Wang, X.; Chen, G.; Han, B.; et al. Early and 1-year postsurgical stability and its factors in patients with complicated skeletal Class Ⅲ malocclusion treated by conventional and surgery-first approach: A prospective cohort study. Am. J. Orthod. Dentofac. Orthop. 2023, 164, 728–740. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-F.; Chiu, Y.-T.; Huang, C.-S.; Ko, E.W.-C.; Chen, Y.-R. Presurgical orthodontics versus no presurgical orthodontics: Treatment outcome of surgical-orthodontic correction for skeletal class III open bite. Plast. Reconstr. Surg. 2010, 126, 2074–2083. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-F.; Chen, Y.-F.; Yao, C.-F.; Chen, Y.-A.; Chen, Y.-R. Long-term outcomes of bimaxillary surgery for treatment of asymmetric skeletal class III deformity using surgery-first approach. Clin. Oral Investig. 2018, 23, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Millesi, G.A.; Zimmermann, M.; Eltz, M. Surgery First and Surgery Early Treatment Approach in Orthognathic Surgery. Oral Maxillofac. Surg. Clin. North Am. 2023, 35, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Peiró-Guijarro, M.A.; Guijarro-Martínez, R.; Hernández-Alfaro, F. Surgery first in orthognathic surgery: A systematic review of the literature. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.F.; Willershausen, B. Braces versus Invisalign®: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef]
- Fujiyama, K.; Kera, Y.; Yujin, S.; Tanikawa, C.; Yamashiro, T.; Guo, X.; Ni, A.; Deguchi, T. Comparison of clinical outcomes between Invisalign and conventional fixed appliance therapies in adult patients with severe deep overbite treated with nonextraction. Am. J. Orthod. Dentofac. Orthop. 2021, 161, 542–547. [Google Scholar] [CrossRef]
- Soverina, D.; Gasparini, G.; Pelo, S.; Doneddu, P.; Todaro, M.; Boniello, R.; Azzuni, C.; Grippaudo, C.; Saponaro, G.; D’amato, G.; et al. Skeletal stability in orthognathic surgery with the surgery first approach: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 930–940. [Google Scholar] [CrossRef]
- Li, M.; Shen, S.; Zhao, Z.; Wang, B.; Yu, H. The application of a fully digital approach in the treatment of skeletal class III malocclusion: A preliminary study. BMC Oral Health 2023, 23, 237. [Google Scholar] [CrossRef]
- Stokbro, K.; Aagaard, E.; Torkov, P.; Bell, R.B.; Thygesen, T. Surgical accuracy of three-dimensional virtual planning: A pilot study of bimaxillary orthognathic procedures including maxillary segmentation. Int. J. Oral Maxillofac. Surg. 2016, 45, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F.; Christensen, A.M.; Lasky, R.E.; Lemoine, J.J.; Liebschner, M.A. Accuracy of the computer-aided surgical simulation (CASS) system in the treatment of patients with complex craniomaxillofacial deformity: A Pilot Study. J. Oral Maxillofac. Surg. 2007, 65, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Bell, W.H.; Creekmore, T.D. Surgical-orthodontic correction of mandibular prognathism. Am. J. Orthod. 1973, 63, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Seifi, M.; Matini, N.S.; Motabar, A.R.; Motabar, M. Dentoskeletal Stability in Conventional Orthognathic Surgery, Presurgical Orthodontic Treatment and Surgery-First Approach in Class-III Patients. World J. Plast. Surg. 2018, 7, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.S.; Choi, J.W.; Lee, J.Y.; Kwon, S.M. Can a surgery-first orthognathic approach reduce the total treatment time? Int. J. Oral Maxillofac. Surg. 2017, 46, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Keser, E.; Naini, F.B. Accelerated orthodontic tooth movement: Surgical techniques and the regional acceleratory phe-nomenon. Maxillofac. Plast. Reconstr. Surg. 2022. 44, 1. [CrossRef]
- Liou, E.J.; Chen, P.-H.; Wang, Y.-C.; Yu, C.-C.; Huang, C.; Chen, Y.-R. Surgery-First accelerated orthognathic surgery: Postoperative rapid orthodontic tooth movement. J. Oral Maxillofac. Surg. 2011, 69, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Liou, E.J.; Chen, P.-H.; Wang, Y.-C.; Yu, C.-C.; Huang, C.; Chen, Y.-R. Surgery-First accelerated orthognathic surgery: Orthodontic guidelines and setup for model surgery. J. Oral Maxillofac. Surg. 2011, 69, 771–780. [Google Scholar] [CrossRef]
- Mah, D.-H.; Kim, S.-G.; Oh, J.-S.; You, J.-S.; Jung, S.-Y.; Kim, W.-G.; Yu, K.-H. Comparative study of postoperative stability between conventional orthognathic surgery and a surgery-first orthognathic approach after bilateral sagittal split ramus osteotomy for skeletal class III correction. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 23–28. [Google Scholar] [CrossRef]
- Hu, J.; Jiang, Y.; Wang, D.; Guo, S.; Li, S.; Jiang, H.; Cheng, J. Comparison of cost-effectiveness and benefits of surgery-first versus orthodontics-first orthognathic correction of skeletal class III malocclusion. Int. J. Oral Maxillofac. Surg. 2020, 50, 367–372. [Google Scholar] [CrossRef]
- Choi, B.-J.; Lee, B.-S.; Kwon, Y.-D.; Lee, J.-W.; Yun, S.-U.; Ryu, K.-S.; Ohe, J.-Y. Correlation between intraoperative proximal segment rotation and post-sagittal split ramus osteotomy relapse: A three-dimensional cone beam computed tomography study. Int. J. Oral Maxillofac. Surg. 2018, 47, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Vongkamolchoon, S.; Sinha, S.; Liao, Y.-F.; Chen, Y.-R.; Huang, C. The impact of a surgery-first approach on oral health-related quality of life. Int. J. Oral Maxillofac. Surg. 2021, 50, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Shokeen, B.; Viloria, E.; Duong, E.; Rizvi, M.; Murillo, G.; Mullen, J.; Shi, B.; Dinis, M.; Li, H.; Tran, N.C.; et al. The impact of fixed orthodontic appliances and clear aligners on the oral microbiome and the association with clinical parameters: A longitudinal comparative study. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e475–e485. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.T.; Hajeer, M.Y.; Burhan, A.S.; Latifeh, Y. The Effect of Treatment With Clear Aligners Versus Fixed Appliances on Oral Health-Related Quality of Life in Patients With Severe Crowding: A One-Year Follow-Up Randomized Controlled Clinical Trial. Cureus 2022, 14, e25472. [Google Scholar] [CrossRef]
- Moon, C.; Sándor, G.K.; Ko, E.C.; Kim, Y.-D. Postoperative Stability of Patients Undergoing Orthognathic Surgery with Orthodontic Treatment Using Clear Aligners: A Preliminary Study. Appl. Sci. 2021, 11, 11216. [Google Scholar] [CrossRef]
- Jaber, S.T.; Hajeer, M.Y.; Burhan, A.S.; Alam, M.K.; Al-Ibrahim, H.M. Treatment effectiveness of young adults using clear aligners versus buccal fixed appliances in class I malocclusion with first premolar extraction using the ABO-Objective Grading System: A randomized controlled clinical trial. Int. Orthod. 2023, 21, 100817. [Google Scholar] [CrossRef]
- Jaber, S.T.; Hajeer, M.Y.; Burhan, A.S. The Effectiveness of In-house Clear Aligners and Traditional Fixed Appliances in Achieving Good Occlusion in Complex Orthodontic Cases: A Randomized Control Clinical Trial. Cureus 2022, 14, e30147. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Vu, T.T.; Nguyen, Q.N. Advanced Digital 3D Technology in the Combined Surgery-First Orthognathic and Clear Aligner Orthodontic Therapy for Dentofacial Deformity Treatment. Processes 2021, 9, 1609. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Experimental Group | Control Group | p Value |
|---|---|---|---|
| Sex (%) | |||
| Male | 40.5 | 43.2 | 0.814 |
| Female | 59.5 | 56.8 | |
| Age (mean ± SD, years) | 24.62 ± 3.89 | 25.73 ± 4.64 | 0.269 |
| Treatment time | 18.05 ± 2.53 | 22.83 ± 3.60 | 0.000 * |
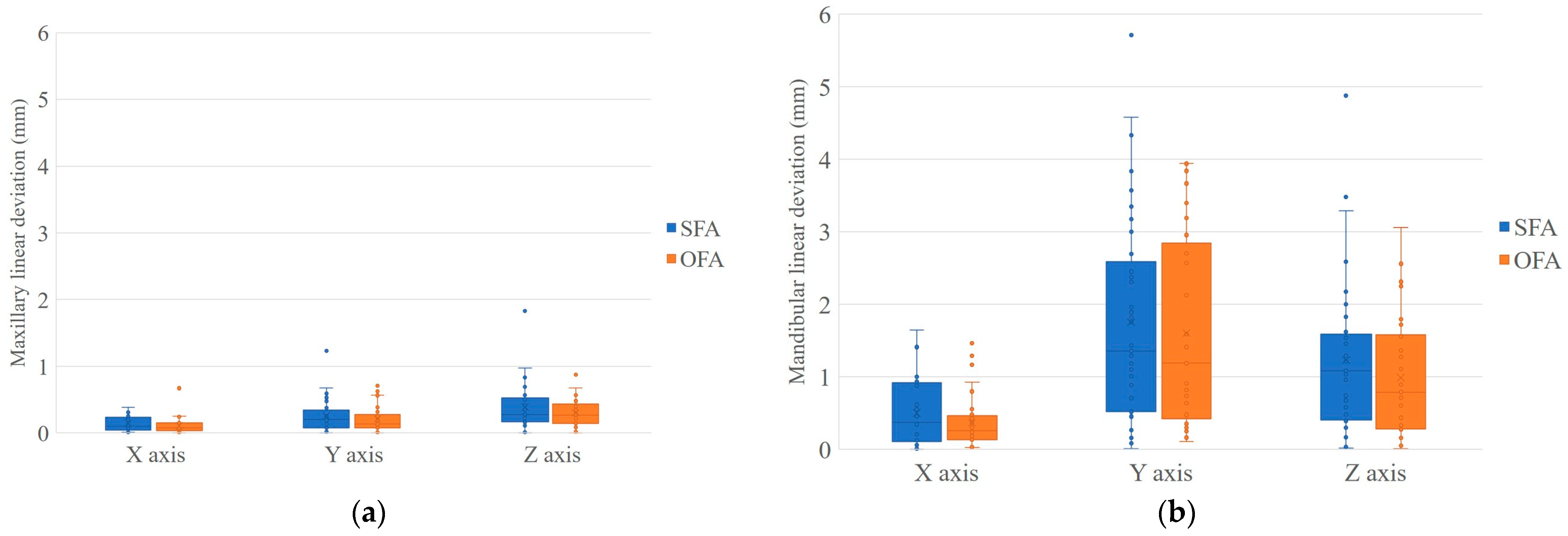
| Dimension | Segment | Median | IQR | p Value | |
|---|---|---|---|---|---|
| Linear deviation (mm) | x axis | SFA | 0.10 | 0.04–0.23 | 0.208 |
| OFA | 0.08 | 0.03–0.15 | |||
| y axis | SFA | 0.20 | 0.07–0.34 | 0.361 | |
| OFA | 0.13 | 0.08–0.27 | |||
| z axis | SFA | 0.28 | 0.16–0.52 | 0.378 | |
| OFA | 0.27 | 0.14–1.43 | |||
| Angular deviation (°) | yaw | SFA | 0.29 | 0.11–0.51 | 0.005 * |
| OFA | 0.16 | 0.06–0.23 | |||
| roll | SFA | 0.26 | 0.10–0.58 | 0.893 | |
| OFA | 0.28 | 0.16–0.49 | |||
| pitch | SFA | 0.71 | 0.34–1.30 | 0.2 | |
| OFA | 0.57 | 0.14–1.10 |
| Dimension | Segment | Median | IQR | p Value | |
|---|---|---|---|---|---|
| Linear deviation (mm) | x axis | SFA | 0.37 | 0.11–0.92 | 0.466 |
| OFA | 0.26 | 0.13–0.46 | |||
| y axis | SFA | 1.36 | 0.52–2.59 | 0.758 | |
| OFA | 1.19 | 0.42–2.85 | |||
| z axis | SFA | 1.08 | 0.41–1.59 | 0.402 | |
| OFA | 0.79 | 0.28–1.58 | |||
| Angular deviation (°) | yaw | SFA | 0.37 | 0.23–0.67 | 0.075 |
| OFA | 0.30 | 0.13–0.42 | |||
| roll | SFA | 0.31 | 0.19–0.62 | 0.056 | |
| OFA | 0.23 | 0.11–0.38 | |||
| pitch | SFA | 0.96 | 0.47–1.50 | 0.6 | |
| OFA | 0.95 | 0.47–1.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Shen, S.; Huang, J.; Wang, Y.; Bao, J.; Wang, B.; Yu, H. The Skeletal Stability of Combined Surgery First Approach and Clear Aligners in Skeletal Class III Malocclusion Correction: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 872. https://doi.org/10.3390/jcm13030872
Li M, Shen S, Huang J, Wang Y, Bao J, Wang B, Yu H. The Skeletal Stability of Combined Surgery First Approach and Clear Aligners in Skeletal Class III Malocclusion Correction: A Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(3):872. https://doi.org/10.3390/jcm13030872
Chicago/Turabian StyleLi, Meng, Shunyao Shen, Jingyang Huang, Yiming Wang, Jiahao Bao, Bo Wang, and Hongbo Yu. 2024. "The Skeletal Stability of Combined Surgery First Approach and Clear Aligners in Skeletal Class III Malocclusion Correction: A Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 3: 872. https://doi.org/10.3390/jcm13030872
APA StyleLi, M., Shen, S., Huang, J., Wang, Y., Bao, J., Wang, B., & Yu, H. (2024). The Skeletal Stability of Combined Surgery First Approach and Clear Aligners in Skeletal Class III Malocclusion Correction: A Randomized Controlled Trial. Journal of Clinical Medicine, 13(3), 872. https://doi.org/10.3390/jcm13030872