
Comparison of Cervical Biportal Endoscopic Spine Surgery and Anterior Cervical Discectomy and Fusion in Patients with Symptomatic Cervical Disc Herniation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
2.3. Surgical Techniques: ACDF
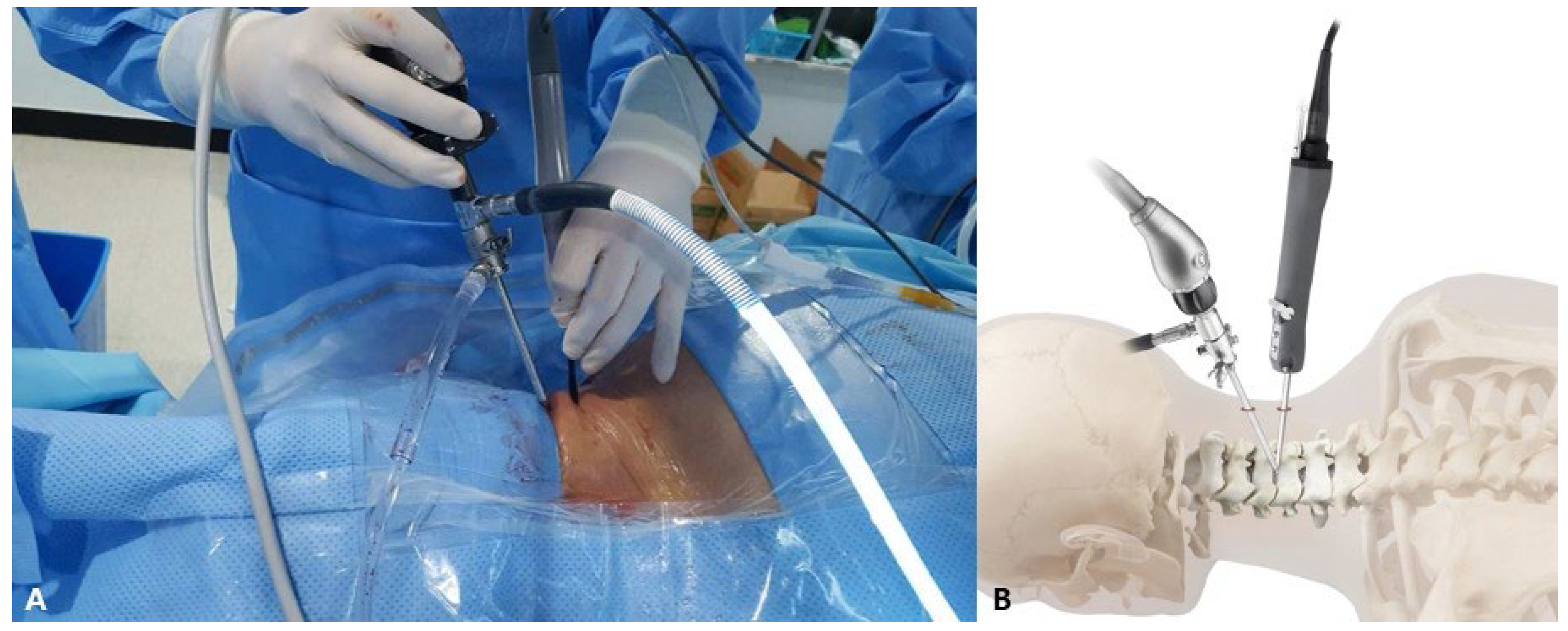
2.4. Surgical Techniques: C-BESS
2.5. Postoperative Care
2.6. Outcome Evaluation
2.7. Statistics
3. Results
3.1. Demographic Characteristics
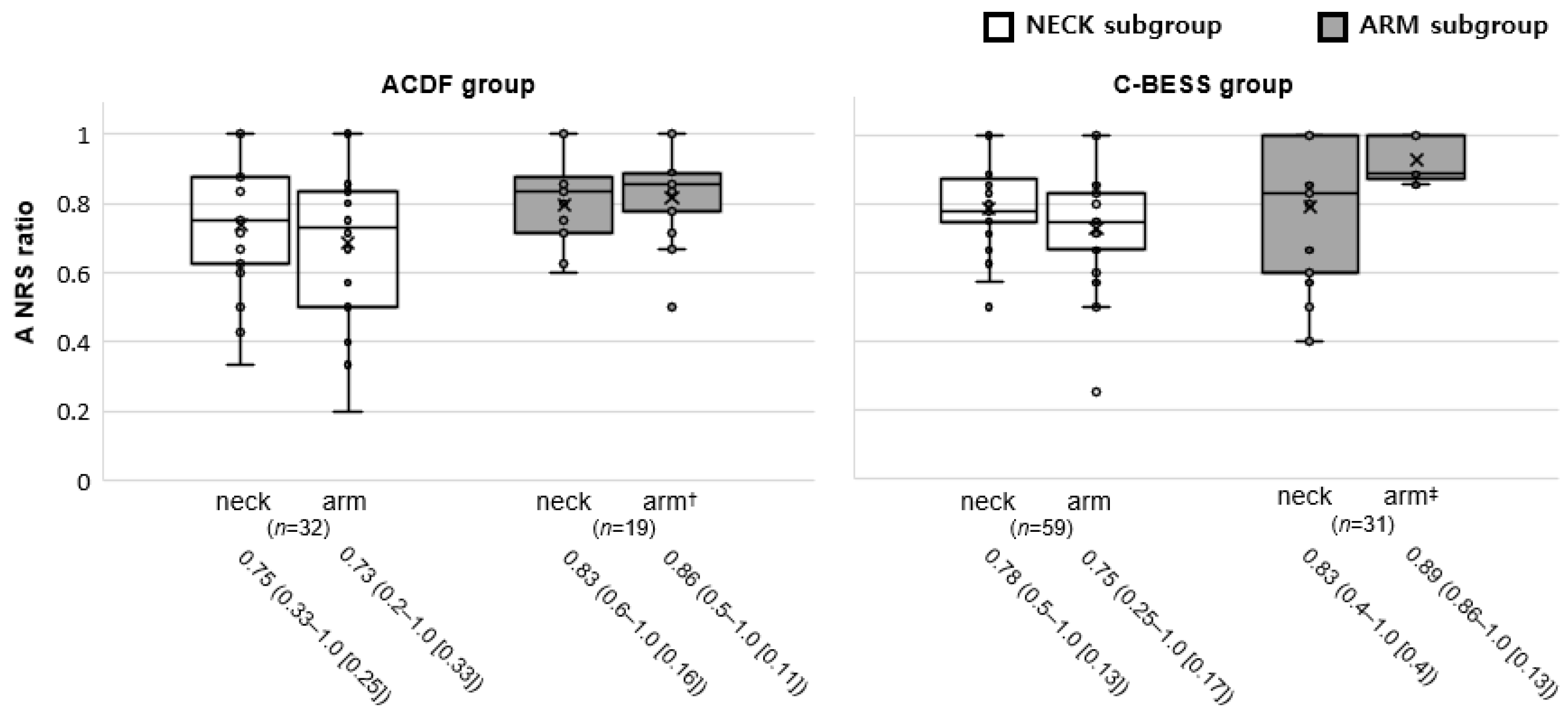
3.2. Outcome Measures
3.3. Perioperative Data
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carette, S.; Fehlings, M.G. Clinical practice. Cervical radiculopathy. N. Engl. J. Med. 2005, 353, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; George, A.A.; Bader, J.O.; Caram, P.M., Jr. Incidence and epidemiology of cervical radiculopathy in the United States military: 2000 to 2009. J. Spinal Disord. Tech. 2012, 25, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Vergroesen, P.P.; Bochyn Ska, A.I.; Emanuel, K.S.; Sharifi, S.; Kingma, I.; Grijpma, D.W.; Smit, T.H. A biodegradable glue for annulus closure: Evaluation of strength and endurance. Spine 2015, 40, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. A Review of Complication Rates for Anterior Cervical Diskectomy and Fusion (ACDF). Surg. Neurol. Int. 2019, 10, 100. [Google Scholar] [CrossRef]
- Lawrence, B.D.; Shamji, M.F.; Traynelis, V.C.; Yoon, S.T.; Rhee, J.M.; Chapman, J.R.; Brodke, D.S.; Fehlings, M.G. Surgical management of degenerative cervical myelopathy: A consensus statement. Spine 2013, 38, S171–S172. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. Dynamic Plating for Single Level Anterior Diskectomy/Fusion: A Study Comparing Morbidity with Single Level Anterior Corpectomy/Fusion. Spinal Surg. 2007, 21, 91–100. [Google Scholar] [CrossRef]
- Zhao, T.; Liu, Y.; Li, F.; Zhang, Y.; Zhang, S.; Zhang, B.; Gao, J. The safety and efficacy of percutaneous transforaminal endoscopic discectomy and fenestration discectomy in the treatment of lumbar disc herniation. Cir. Cir. 2023, 91, 153–161. [Google Scholar] [CrossRef]
- Zheng, B.; Hao, D.; Guo, H.; He, B. ACDF vs TDR for patients with cervical spondylosis—An 8 year follow up study. BMC Surg. 2017, 17, 113. [Google Scholar] [CrossRef]
- Pointillart, V.; Castelain, J.E.; Coudert, P.; Cawley, D.T.; Gille, O.; Vital, J.M. Outcomes of the Bryan cervical disc replacement: Fifteen year follow-up. Int. Orthop. 2018, 42, 851–857. [Google Scholar] [CrossRef]
- Song, Z.; Zhang, Z.; Hao, J.; Shen, J.; Zhou, N.; Xu, S.; Ni, W.; Hu, Z. Microsurgery or open cervical foraminotomy for cervical radiculopathy? A systematic review. Int. Orthop. 2016, 40, 1335–1343. [Google Scholar] [CrossRef]
- Zdeblick, T.A.; Zou, D.; Warden, K.E.; McCabe, R.; Kunz, D.; Vanderby, R. Cervical stability after foraminotomy. A biomechanical in vitro analysis. J. Bone Jt. Surg. Am. 1992, 74, 22–27. [Google Scholar] [CrossRef]
- Sakhrekar, R.; Ha, J.S.; Han, H.D.; Kim, D.H.; Kim, C.W.; Kulkarni, S. The Past, Present, and Future of Unilateral Biportal Endoscopy with a Technical Note on Novel Endoscopic Visualization Pedicle Screw Insertion Technique and UBE-transforaminal Lumbar Interbody Fusion Technique with Literature Review. J. Orthop. Case Rep. 2023, 13, 165–171. [Google Scholar] [CrossRef]
- Jung, S.B.; Kim, N. Biportal endoscopic spine surgery for cervical disk herniation: A technical notes and preliminary report. Medicine 2022, 101, e29751. [Google Scholar] [CrossRef]
- Zhu, C.; Zhou, X.; Ge, G.; Wang, C.; Zhuang, X.; Cheng, W.; Wang, D.; Zhu, H.; Pan, H.; Zhang, W. Unilateral Biportal Endoscopic Laminectomy for Treating Cervical Stenosis: A Technical Note and Preliminary Results. Medicina 2023, 59, 305. [Google Scholar] [CrossRef]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Ward, C.; Meathe, E.; Benumof, J.; Trousdale, F. A computer nomogram for blood loss replacement. J. Am. Soc. Anesthesiol. 1980, 53, S126. [Google Scholar] [CrossRef]
- Furman, E.B. Intraoperative fluid therapy. Int. Anesthesiol. Clin. 1975, 13, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Picado, A.; Albinarrate, A.; Barrachina, B. Determination of Perioperative Blood Loss: Accuracy or Approximation? Anesth. Analg. 2017, 125, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Keum, H.J.; Shin, S.H. Percutaneous Endoscopic Cervical Discectomy Versus Anterior Cervical Discectomy and Fusion: A Comparative Cohort Study with a Five-Year Follow-Up. J. Clin. Med. 2020, 9, 371. [Google Scholar] [CrossRef] [PubMed]
- Maguire, T.; Mayne, C.J.; Terry, T.; Tincello, D.G. Analysis of the surgical learning curve using the cumulative sum (CUSUM) method. Neurourol. Urodyn. 2013, 32, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Thoomes, E.J.; Scholten-Peeters, G.G.; de Boer, A.J.; Olsthoorn, R.A.; Verkerk, K.; Lin, C.; Verhagen, A.P. Lack of uniform diagnostic criteria for cervical radiculopathy in conservative intervention studies: A systematic review. Eur. Spine J. 2012, 21, 1459–1470. [Google Scholar] [CrossRef]
- Maharaj, M.M.; Mobbs, R.J.; Hogan, J.; Zhao, D.F.; Rao, P.J.; Phan, K. Anterior cervical disc arthroplasty (ACDA) versus anterior cervical discectomy and fusion (ACDF): A systematic review and meta-analysis. J. Spine Surg. 2015, 1, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Yee, T.J.; Swong, K.; Park, P. Complications of anterior cervical spine surgery: A systematic review of the literature. J. Spine Surg. 2020, 6, 302–322. [Google Scholar] [CrossRef] [PubMed]
- Dohrmann, G.J.; Hsieh, J.C. Long-term results of anterior versus posterior operations for herniated cervical discs: Analysis of 6,000 patients. Med. Princ. Pract. 2014, 23, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B.; Xu, S.; Guo, C.; Jin, L.; Liu, C.; Liu, H. Efficacy and safety of unilateral biportal endoscopy versus other spine surgery: A systematic review and meta-analysis. Front. Surg. 2022, 9, 911914. [Google Scholar] [CrossRef]
- Passias, P.G.; Hasan, S.; Radcliff, K.; Isaacs, R.; Bianco, K.; Jalai, C.M.; Poorman, G.W.; Worley, N.J.; Horn, S.R.; Boniello, A.; et al. Arm Pain Versus Neck Pain: A Novel Ratio as a Predictor of Post-Operative Clinical Outcomes in Cervical Radiculopathy Patients. Int. J. Spine Surg. 2018, 12, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.H.; Natarajan, R.N.; An, H.S.; Andersson, G.B. Comparison of biomechanical response to surgical procedures used for cervical radiculopathy: Posterior keyhole foraminotomy versus anterior foraminotomy and discectomy versus anterior discectomy with fusion. J. Spinal Disord. 2001, 14, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Raynor, R.B.; Pugh, J.; Shapiro, I. Cervical facetectomy and its effect on spine strength. J. Neurosurg. 1985, 63, 278–282. [Google Scholar] [CrossRef]
- Li, C.; Ju, F.; Li, W.; Gao, S.; Cao, C.; Li, C.; He, L.; Ma, X.; Li, M. Efficacy and safety of unilateral biportal endoscopy compared with microscopic decompression in the treatment of lumbar spinal stenosis: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e27970. [Google Scholar] [CrossRef]
- Chen, L.; Zhu, B.; Zhong, H.Z.; Wang, Y.G.; Sun, Y.S.; Wang, Q.F.; Liu, J.J.; Tian, D.S.; Jing, J.H. The Learning Curve of Unilateral Biportal Endoscopic (UBE) Spinal Surgery by CUSUM Analysis. Front. Surg. 2022, 9, 873691. [Google Scholar] [CrossRef]
- Son, S.; Ahn, Y.; Lee, S.G.; Kim, W.K.; Yoo, B.R.; Jung, J.M.; Cho, J. Learning curve of percutaneous endoscopic transforaminal lumbar discectomy by a single surgeon. Medicine 2021, 100, e24346. [Google Scholar] [CrossRef] [PubMed]
- You, K.H.; Kang, M.S.; Lee, W.M.; Hwang, J.Y.; Hyun, J.T.; Yang, I.; Park, S.M.; Park, H.J. Biportal endoscopic paraspinal decompressive foraminotomy for lumbar foraminal stenosis: Clinical outcomes and factors influencing unsatisfactory outcomes. Acta Neurochir. 2023, 165, 2153–2163. [Google Scholar] [CrossRef] [PubMed]
- Lange, N.; Stadtmüller, T.; Scheibel, S.; Reischer, G.; Wagner, A.; Meyer, B.; Gempt, J. Analysis of risk factors for perioperative complications in spine surgery. Sci. Rep. 2022, 12, 14350. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.T.; Kim, J.S.; Huang, A.P.; Lin, M.H.; Chen, C.M. Current Indications for Spinal Endoscopic Surgery and Potential for Future Expansion. Neurospine 2023, 20, 33–42. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | ACDF 1 (n = 156) | C-BESS 2 (n = 162) | p-Value |
|---|---|---|---|
| Sex, male: female | 101: 55 | 113: 49 | 0.3 |
| Age, years | 52 (34–83), [15] | 54 (29–81), [16] | 0.4 |
| Symptom duration, months | 12 (6–60), [8] | 12 (6–52), [12.5] | 0.8 |
| Initial neck NRS 3 | 8 (4–9), [1] | 8 (5–9), [2] | 0.8 |
| Initial arm NRS | 7 (4–9), [2] | 7 (4–9), [2] | 0.8 |
| Initial NDI 4, % | 42 (20–78), [14] | 40 (20–78), [26] | 0.1 |
| Herniation levels, % | |||
| C3/4 | 1.9, n = 3 | 3.7, n = 6 | 0.1 |
| C4/5 | 19.2, n = 30 | 17.9, n = 19 | |
| C5/6 | 60.3, n = 94 | 52.5, n = 85 | |
| C6/7 | 18.6, n = 29 | 21.6, n = 35 | |
| C7/T1 | 0.0, n = 0 | 4.3, n = 7 |
| Group/Variables | Preoperative | Postoperative One Year |
|---|---|---|
| ACDF 1 | ||
| neck NRS 3 | 7.3 (5–9), SD 1.0, (7.1 to 7.5) | 1.6 (0–4), SD 1.0, (1.4 to 1.8) |
| arm NRS 3 | 7.0 (4–9), SD 1.5, (6.7 to 7.2) | 1.5 (0–4), SD 0.9, (1.4 to 1.7) |
| NDI | 42.2 (20–78), SD 14.2, (43.0 to 47.5) | 14.3 (4–38), SD 8.2, (13.0 to 15.6) |
| C-BESS 2 | ||
| neck NRS 3 | 7.2 (5–9), SD 1.2, (7.1 to 7.4) | 1.4 (0–4), SD 0.9, (1.3 to 1.5) |
| arm NRS 3 | 6.9 (4–9), SD 1.5, (6.7 to 7.1) | 1.3 (0–4), SD 0.8, (1.1 to 1.4) |
| NDI 4 | 42.9 (19–80), SD 15.1, (40.6 to 45.3) | 14.9 (4–36), SD 8.8, (13.5 to 16.2) |
| Variables | ACDF 1 (n = 156) | C-BESS 2 (n = 162) | p-Value |
|---|---|---|---|
| Operative time, minutes | 35 (30–90) [10] | 55 (40–100) [15] | <0.001 |
| Estimated blood loss, mL | 78.6 (13.4–190.4) [29.7] | 88.5 (45.9–205.3) [21.1] | <0.001 |
| Length of hospitalization, days | 2 (1–7) [1] | 3 (1–8) [1] | 0.4 |
| Variables | ACDF 1 (n = 156) | C-BESS 2 (n = 162) |
|---|---|---|
| neck NRS ratio 3 ≤ 0.2 4 | 1 | 5 |
| arm NRS ratio 3 ≤ 0.2 4 | 4 | 1 |
| Complications [%] (details) | 4 [2.6] (hoarseness 2, dysphagia 1, screw loosening 1) | 3 [1.9] (motor weakness 2, muscle soreness 1) |
| Revision | 1 | 1 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.-B.; Gunadala, I.; Kim, N. Comparison of Cervical Biportal Endoscopic Spine Surgery and Anterior Cervical Discectomy and Fusion in Patients with Symptomatic Cervical Disc Herniation. J. Clin. Med. 2024, 13, 1823. https://doi.org/10.3390/jcm13061823
Jung S-B, Gunadala I, Kim N. Comparison of Cervical Biportal Endoscopic Spine Surgery and Anterior Cervical Discectomy and Fusion in Patients with Symptomatic Cervical Disc Herniation. Journal of Clinical Medicine. 2024; 13(6):1823. https://doi.org/10.3390/jcm13061823
Chicago/Turabian StyleJung, Seok-Bong, Ishant Gunadala, and Nackhwan Kim. 2024. "Comparison of Cervical Biportal Endoscopic Spine Surgery and Anterior Cervical Discectomy and Fusion in Patients with Symptomatic Cervical Disc Herniation" Journal of Clinical Medicine 13, no. 6: 1823. https://doi.org/10.3390/jcm13061823