
The Obesity Mortality Paradox in Patients with Pulmonary Embolism: Insights from a Tertiary Care Center

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Statistical Analysis
2.2. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.; Goldenberg, I.; Schleede, S.; McNitt, S.; Gosev, I.; Elbadawi, A.; Pietropaoli, A.; Barrus, B.; Chen, Y.L.; Mazzillo, J.; et al. Effect of a Multidisciplinary Pulmonary Embolism Response Team on Patient Mortality. Am. J. Cardiol. 2021, 161, 102–107. [Google Scholar] [CrossRef]
- Chaudhury, P.; Gadre, S.K.; Schneider, E.; Renapurkar, R.D.; Gomes, M.; Haddadin, I.; Heresi, G.A.; Tong, M.Z.; Bartholomew, J.R. Impact of Multidisciplinary Pulmonary Embolism Response Team Availability on Management and Outcomes. Am. J. Cardiol. 2019, 124, 1465–1469. [Google Scholar] [CrossRef] [PubMed]
- Fleitas Sosa, D.; Lehr, A.L.; Zhao, H.; Roth, S.; Lakhther, V.; Bashir, R.; Cohen, G.; Panaro, J.; Maldonado, T.S.; Horowitz, J.; et al. Impact of pulmonary embolism response teams on acute pulmonary embolism: A systematic review and meta-analysis. Eur. Respir. Rev. 2022, 31, 220023. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief 2020, 1–8. [Google Scholar]
- Gregson, J.; Kaptoge, S.; Bolton, T.; Pennells, L.; Willeit, P.; Burgess, S.; Bell, S.; Sweeting, M.; Rimm, E.B.; Kabrhel, C.; et al. Cardiovascular Risk Factors Associated with Venous Thromboembolism. JAMA Cardiol. 2019, 4, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Kabrhel, C.; Varraso, R.; Goldhaber, S.Z.; Rimm, E.B.; Camargo, C.A. Prospective study of BMI and the risk of pulmonary embolism in women. Obesity 2009, 17, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, E.; Teal, N.; Dudley, J.; May, W.; Bower, J.D.; Salahudeen, A.K. Influence of excess weight on mortality and hospital stay in 1346 hemodialysis patients. Kidney Int. 1999, 55, 1560–1567. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; De Schutter, A.; Patel, D.A.; Romero-Corral, A.; Artham, S.M.; Milani, R.V. Body composition and survival in stable coronary heart disease: Impact of lean mass index and body fat in the “obesity paradox”. J. Am. Coll. Cardiol. 2012, 60, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Horwich, T.B.; Fonarow, G.C.; Clark, A.L. Obesity and the Obesity Paradox in Heart Failure. Prog. Cardiovasc. Dis. 2018, 61, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Chittal, P.; Babu, A.S.; Lavie, C.J. Obesity paradox: Does fat alter outcomes in chronic obstructive pulmonary disease? COPD 2015, 12, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Barba, R.; Zapatero, A.; Losa, J.E.; Valdés, V.; Todolí, J.A.; Di Micco, P.; Monreal, M. Body mass index and mortality in patients with acute venous thromboembolism: Findings from the RIETE registry. J. Thromb. Haemost. JTH 2008, 6, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Hobohm, L.; Münzel, T.; Ostad, M.A.; Espinola-Klein, C.; Lavie, C.J.; Konstantinides, S.; Lankeit, M. Survival Benefit of Obese Patients with Pulmonary Embolism. Mayo Clin. Proc. 2019, 94, 1960–1973. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. JTH 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Barrachina, M.N.; Hermida-Nogueira, L.; Moran, L.A.; Casas, V.; Hicks, S.M.; Sueiro, A.M.; Di, Y.; Andrews, R.K.; Watson, S.P.; Gardiner, E.E.; et al. Phosphoproteomic Analysis of Platelets in Severe Obesity Uncovers Platelet Reactivity and Signaling Pathways Alterations. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.D.; Matta, F.; Goldman, J. Obesity and pulmonary embolism: The mounting evidence of risk and the mortality paradox. Thromb. Res. 2011, 128, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Chahal, H.; McClelland, R.L.; Tandri, H.; Jain, A.; Turkbey, E.B.; Hundley, W.G.; Barr, R.G.; Kizer, J.; Lima, J.A.C.; Bluemke, D.A.; et al. Obesity and right ventricular structure and function: The MESA-Right Ventricle Study. Chest 2012, 141, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, J.M.; Zhao, H.; Moores, L.K.; Rali, P. Obesity Paradox in VTE Outcomes: An Evolving Concept. Chest 2020, 158, 1290–1291. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ren, J. Obesity Paradox in Aging: From Prevalence to Pathophysiology. Prog. Cardiovasc. Dis. 2018, 61, 182–189. [Google Scholar] [CrossRef] [PubMed]
- McAuley, P.A.; Beavers, K.M. Contribution of cardiorespiratory fitness to the obesity paradox. Prog. Cardiovasc. Dis. 2014, 56, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Goldhaber, S.Z. Obesity and Pulmonary Embolism: Can We Dismantle the “Obesity Paradox”. Thromb. Haemost. 2023, 124, 058–060. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Chong, M.; Le, A.; Mohammadi-Shemirani, P.; Morton, R.; Brinza, C.; Kiflen, M.; Narula, S.; Akhabir, L.; Mao, S.; et al. Surrogate Adiposity Markers and Mortality. JAMA Netw. Open 2023, 6, e2334836. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | BMI ≥ 30 (N = 150) | BMI 18.5–29.9 (N = 98) | p-Value | |
|---|---|---|---|---|
| Male | 70 (46.7%) | 55 (56.1%) | 0.15 | |
| Age, mean (SD) | 59.9 (15.3) | 65.5 (15.2) | 0.005 | |
| Prior VTE | 7 (4.7%) | 4 (4.1%) | 0.83 | |
| Recent COVID infection | 20 (13.3%) | 4 (4.1%) | 0.016 | |
| History of cancer | 33 (22.0%) | 39 (39.8%) | 0.003 | |
| History of heart failure | 26 (17.3%) | 15 (15.3%) | 0.67 | |
| History of chronic lung disease | 29 (19.3%) | 24 (24.5%) | 0.33 | |
| Smoking | 19 (12.7%) | 15 (15.8%) | 0.49 | |
| Hypoxia (defined as requiring oxygen) | 116 (77.3%) | 76 (78.4%) | 0.85 | |
| Hypotension | 13 (8.7%) | 13 (13.4%) | 0.24 | |
| European Society of Cardiology PE Mortality Risk | Intermediate–Low | 30 (20.0%) | 27 (27.6%) | 0.38 |
| Intermediate–High | 85 (56.7%) | 51 (52.0%) | ||
| High | 35 (23.3%) | 20 (20.4%) | ||
| Catheter thrombectomy | 80 (53.7%) | 46 (46.9%) | 0.30 | |
| Systemic thrombolysis | 13 (8.7%) | 8 (8.2%) | 0.89 | |
| Hazard Ratio | p-Value | 95% Confidence Interval | |
|---|---|---|---|
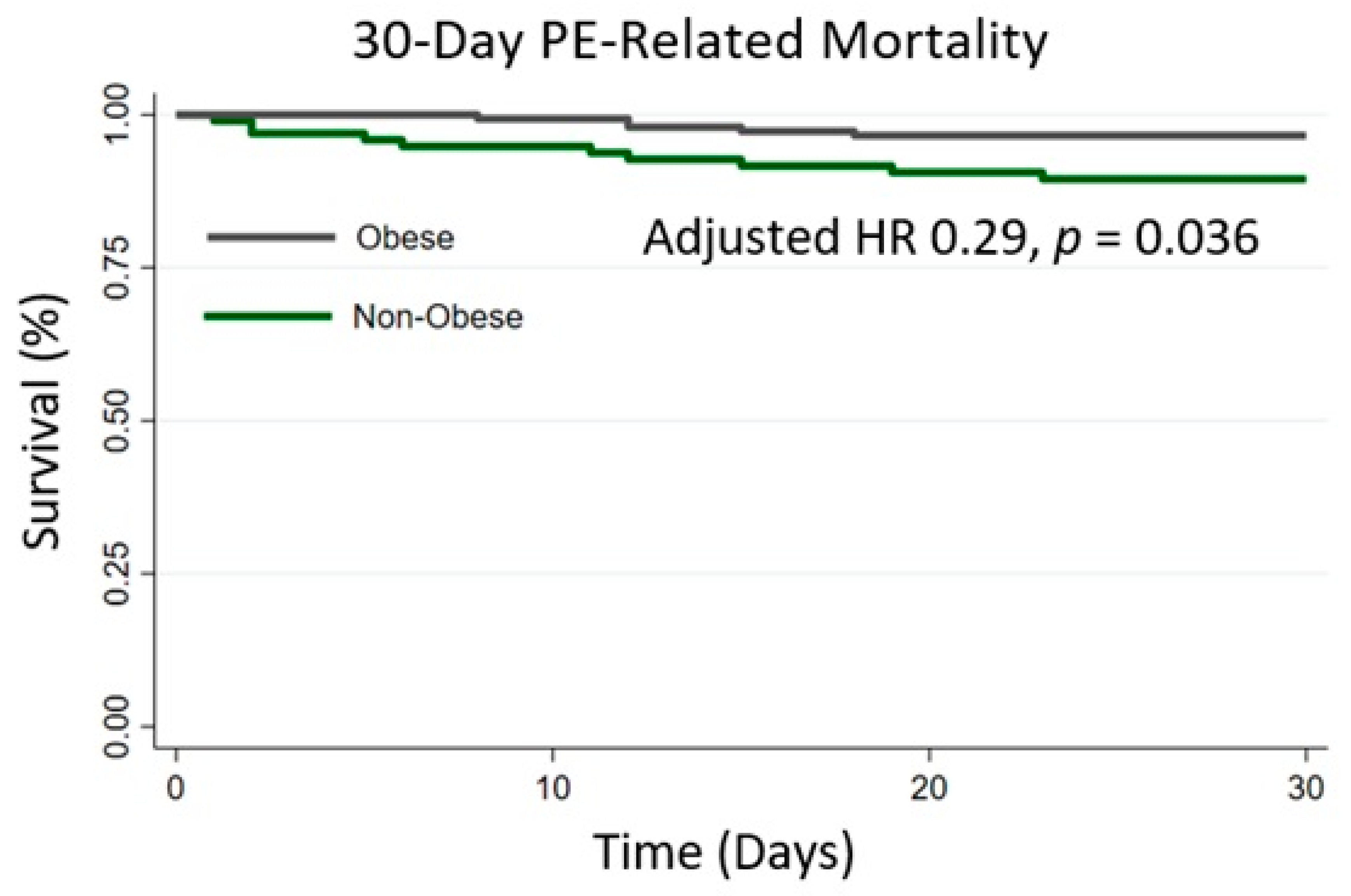
| Obesity (BMI ≥ 30 vs. BMI 18.5–29.9) | 0.29 | 0.04 | 0.09–0.92 |
| Male | 0.54 | 0.27 | 0.18–1.60 |
| Age (per 1 year) | 1.02 | 0.27 | 0.98–1.06 |
| History of Heart Failure | 1.98 | 0.23 | 0.65–6.04 |
| History of Chronic Lung Disease | 2.09 | 0.18 | 0.72–6.05 |
| Recent COVID Infection | 2.56 | 0.25 | 0.52–12.6 |
| Systemic Thrombolysis | 3.14 | 0.12 | 0.76–13.0 |
| ESC Mortality Risk (Baseline: Intermediate–Low Risk) | |||
| Intermediate–High Risk | 0.29 | 0.06 | 0.08–1.06 |
| High Risk | 0.61 | 0.46 | 0.17–2.22 |
| Hazard Ratio | p-Value | 95% Confidence Interval | |
|---|---|---|---|
| BMI (per 1 kg/m2) | 0.91 | 0.049 | 0.83–0.999 |
| Male | 0.53 | 0.30 | 0.16–1.74 |
| Age (per 1 year) | 1.01 | 0.47 | 0.98–1.05 |
| History of Heart Failure | 2.40 | 0.14 | 0.75–7.72 |
| History of Chronic Lung Disease | 2.04 | 0.23 | 0.64–6.50 |
| Recent COVID Infection | 2.58 | 0.25 | 0.52–12.9 |
| Systemic Thrombolysis | 3.09 | 0.12 | 0.75–12.7 |
| ESC Mortality Risk (Baseline: Intermediate–Low Risk) | |||
| Intermediate–High Risk | 0.43 | 0.22 | 0.11–1.66 |
| High Risk | 0.64 | 0.53 | 0.16–2.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkhalfan, F.; Bukhari, S.; Rosenzveig, A.; Moudgal, R.; Khan, S.Z.; Ghoweba, M.; Chaudhury, P.; Cameron, S.J.; Tefera, L. The Obesity Mortality Paradox in Patients with Pulmonary Embolism: Insights from a Tertiary Care Center. J. Clin. Med. 2024, 13, 2375. https://doi.org/10.3390/jcm13082375
Alkhalfan F, Bukhari S, Rosenzveig A, Moudgal R, Khan SZ, Ghoweba M, Chaudhury P, Cameron SJ, Tefera L. The Obesity Mortality Paradox in Patients with Pulmonary Embolism: Insights from a Tertiary Care Center. Journal of Clinical Medicine. 2024; 13(8):2375. https://doi.org/10.3390/jcm13082375
Chicago/Turabian StyleAlkhalfan, Fahad, Syed Bukhari, Akiva Rosenzveig, Rohitha Moudgal, Syed Zamrak Khan, Mohamed Ghoweba, Pulkit Chaudhury, Scott J. Cameron, and Leben Tefera. 2024. "The Obesity Mortality Paradox in Patients with Pulmonary Embolism: Insights from a Tertiary Care Center" Journal of Clinical Medicine 13, no. 8: 2375. https://doi.org/10.3390/jcm13082375