
Intraoperative Fracture during the Insertion of Advanced Locking Screws (T2 Alpha Femur Retrograde Intramedullary Nailing System): Report of Two Cases and Identifying Causes and Prevention
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
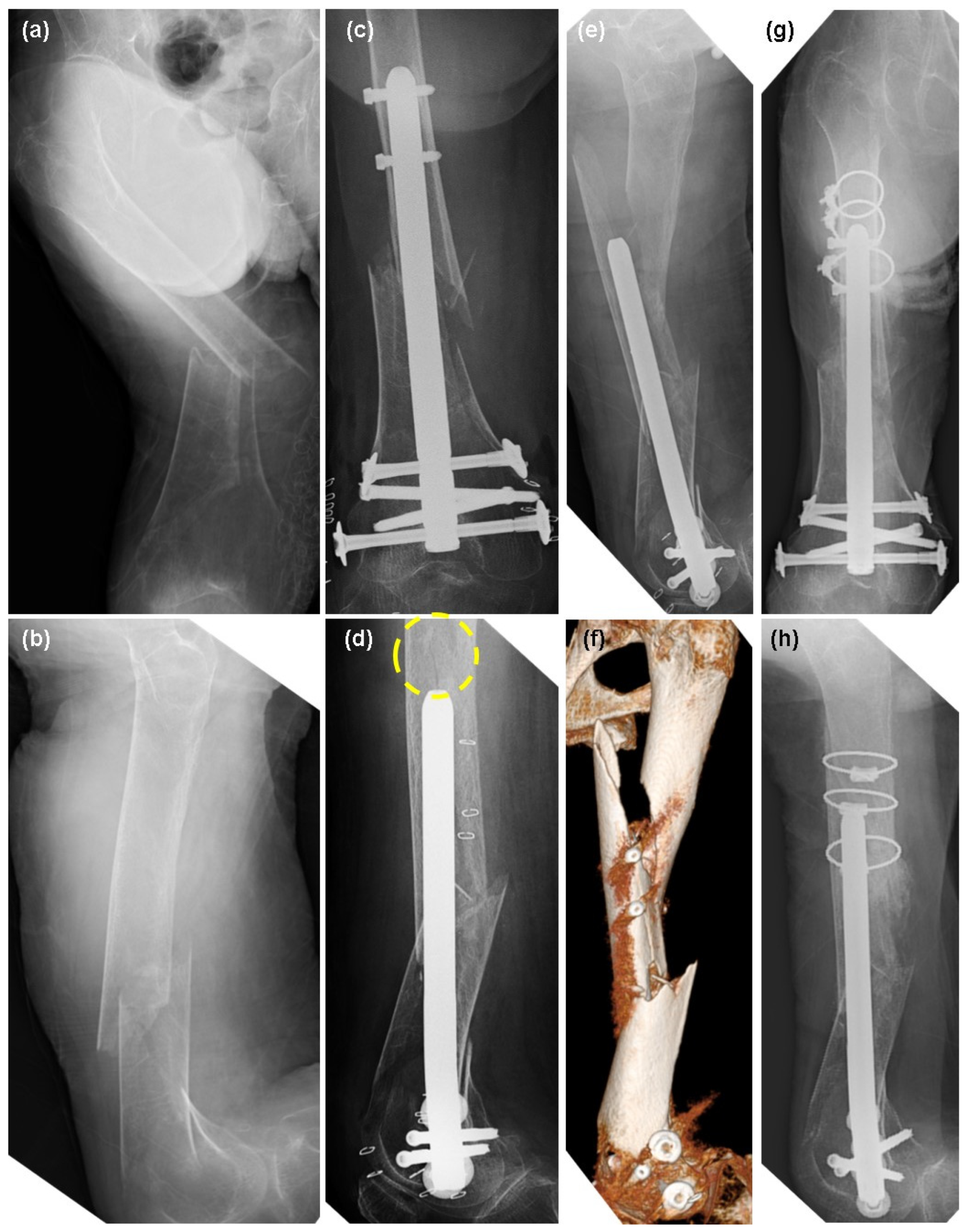
2. Case Presentation
2.1. Patient 1
2.2. Patient 2
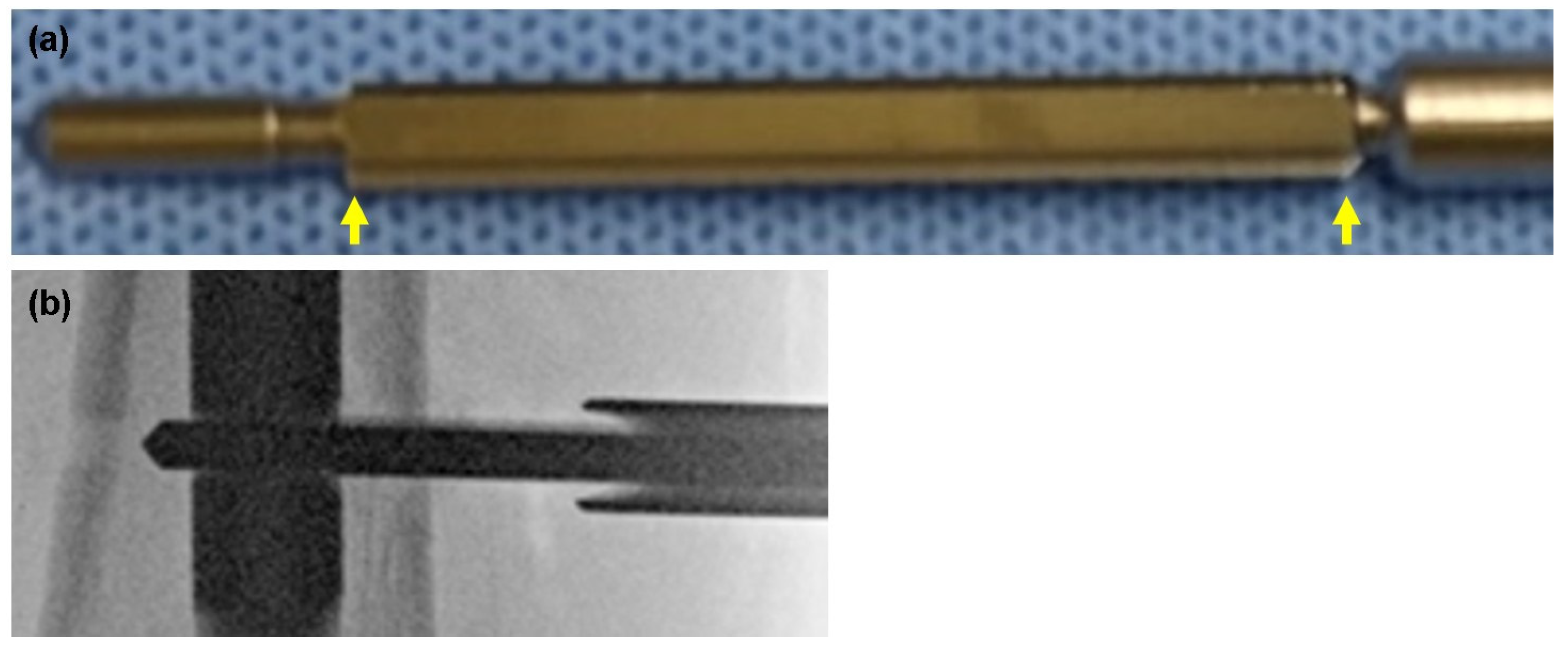
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elbarbary, A.N.; Hassen, S.; Badr, I.T. Outcome of Intramedullary Nail for Fixation of Osteoporotic Femoral Shaft Fractures in the Elderly above 60. Injury 2021, 52, 602–605. [Google Scholar] [CrossRef] [PubMed]
- Rosa, N.; Marta, M.; Vaz, M.; Tavares, S.M.O.; Simoes, R.; Magalhães, F.D.; Marques, A.T. Recent Developments on Intramedullary Nailing: A Biomechanical Perspective. Ann. N. Y. Acad. Sci. 2017, 1408, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, Y.N.; Bava, S.S.; Phunde, R.; Soni, H.; Haider, H. Windshield Wiper Effect in Human Bone-Peri-Implant Benign Diaphyseal Expansile Lesion with Humerus Shaft Fracture Non-Union with Implant in Situ—Case Report. J. Orthop. Case Rep. 2023, 13, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Brinker, M.R.; O’Connor, D.P. Exchange Nailing of Ununited Fractures. J. Bone Jt. Surg. Am. 2007, 89, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Nester, M.; Borrelli, J., Jr. Distal Femur Fractures Management and Evolution in the Last Century. Int. Orthop. 2023, 47, 2125–2135. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.J.; Kim, M.S.; Kim, T.H.; Kim, M.W.; Kweon, S.H. Fractures of the Distal Femur in Elderly Patients: Retrospective Analysis of a Case Series Treated with Single or Double Plate. J. Orthop. Surg. Res. 2022, 17, 55. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Mittal, A.; Raj, M.; Singh, P.; Singh, J.; Kumar, S. Extra Articular Supracondylar Femur Fractures Managed with Locked Distal Femoral Plate or Supracondylar Nailing: A Comparative Outcome Study. J. Clin. Diagn. Res. 2017, 11, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.; Rajnish, R.K.; Kumar, P.; Srivastava, A.; Rathor, K.; Haq, R.U. Comparison of Outcomes of Retrograde Intramedullary Nailing Versus Locking Plate Fixation in Distal Femur Fractures: A Systematic Review and Meta-Analysis of 936 Patients in 16 Studies. J. Orthop. 2023, 36, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.R.; Ma, J.X.; Wang, S.; Sun, L.; Wang, Y.; Lu, B.; Bai, H.H.; Hu, Y.C.; Ma, X.L. Comparison of Less Invasive Stabilization System Plate and Retrograde Intramedullary Nail in the Fixation of Femoral Supracondylar Fractures in the Elderly: A Biomechanical Study. Orthop. Surg. 2019, 11, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Ohbe, H.; Tomita, Y.; Yorifuji, T.; Nakajima, M.; Sasabuchi, Y.; Miyamoto, Y.; Matsui, H.; Noda, T.; Yasunaga, H. Associations between Early Surgery and Postoperative Outcomes in Elderly Patients with Distal Femur Fracture: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 5800. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Langen, M.V.; Sontheimer, V.; Borchert, G.H.; Izadpanah, K.; Schmal, H.; Kubosch, E.J. Outcome Evaluation of Distal Femoral Fractures Following Surgical Management: A Retrospective Cohort Study. J. Pers. Med. 2023, 13, 350. [Google Scholar] [CrossRef] [PubMed]
- Paulsson, M.; Ekholm, C.; Tranberg, R.; Rolfson, O.; Geijer, M. Using a Traction Table for Fracture Reduction during Minimally Invasive Plate Osteosynthesis (MIPO) of Distal Femoral Fractures Provides Anatomical Alignment. J. Clin. Med. 2023, 12, 4044. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, K.C.; Lim, S.J.; Kwon, K.B.; Kim, J.W. Surgical outcomes of simple distal femur fractures in elderly patients treated with the minimally invasive plate osteosynthesis technique: Can percutaneous cerclage wiring reduce the fracture healing time? Arch. Orthop. Trauma Surg. 2020, 140, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Kwak, D.; Kim, J.; Kwon, S.; Kwon, J.; Hwang, J. Risk Factors of Proximal Screw Breakage of Locking Plate (ZPLP®) after MIPO for Distal Femur Fractures -Analysis of Patients with Plate Removal after Bony Union-. J. Clin. Med. 2023, 12, 6345. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F. Sterile Inflammatory Response and Surgery-Related Trauma in Elderly Patients with Subtrochanteric Fractures. Biomedicines 2024, 12, 354. [Google Scholar] [CrossRef] [PubMed]
- Herrera, A.; Albareda, J.; Gabarre, S.; Ibarz, E.; Puertolas, S.; Mateo, J.; Gracia, L. Comparative Analysis of the Biomechanical Behavior of Anterograde/Retrograde Nailing in Supracondylar Femoral Fractures. Injury 2020, 51 (Suppl. S1), S80–S88. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higuchi, T.; Taninaka, A.; Yoshimizu, R.; Hayashi, K.; Miwa, S.; Yamamoto, N.; Tsuchiya, H.; Demura, S. Intraoperative Fracture during the Insertion of Advanced Locking Screws (T2 Alpha Femur Retrograde Intramedullary Nailing System): Report of Two Cases and Identifying Causes and Prevention. J. Clin. Med. 2024, 13, 2393. https://doi.org/10.3390/jcm13082393
Higuchi T, Taninaka A, Yoshimizu R, Hayashi K, Miwa S, Yamamoto N, Tsuchiya H, Demura S. Intraoperative Fracture during the Insertion of Advanced Locking Screws (T2 Alpha Femur Retrograde Intramedullary Nailing System): Report of Two Cases and Identifying Causes and Prevention. Journal of Clinical Medicine. 2024; 13(8):2393. https://doi.org/10.3390/jcm13082393
Chicago/Turabian StyleHiguchi, Takashi, Atsushi Taninaka, Rikuto Yoshimizu, Katsuhiro Hayashi, Shinji Miwa, Norio Yamamoto, Hiroyuki Tsuchiya, and Satoru Demura. 2024. "Intraoperative Fracture during the Insertion of Advanced Locking Screws (T2 Alpha Femur Retrograde Intramedullary Nailing System): Report of Two Cases and Identifying Causes and Prevention" Journal of Clinical Medicine 13, no. 8: 2393. https://doi.org/10.3390/jcm13082393