
A Novel Surgical Treatment Management Algorithm for Elbow Posterolateral Rotatory Instability (PLRI) Based on the Common Extensor Origin Integrity
 ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Anatomy and Considerations
3. Clinical Presentation and Diagnosis
4. Unique Features
- It is straightforward to grasp.
- It directly applies to clinical settings without requiring complex procedures.
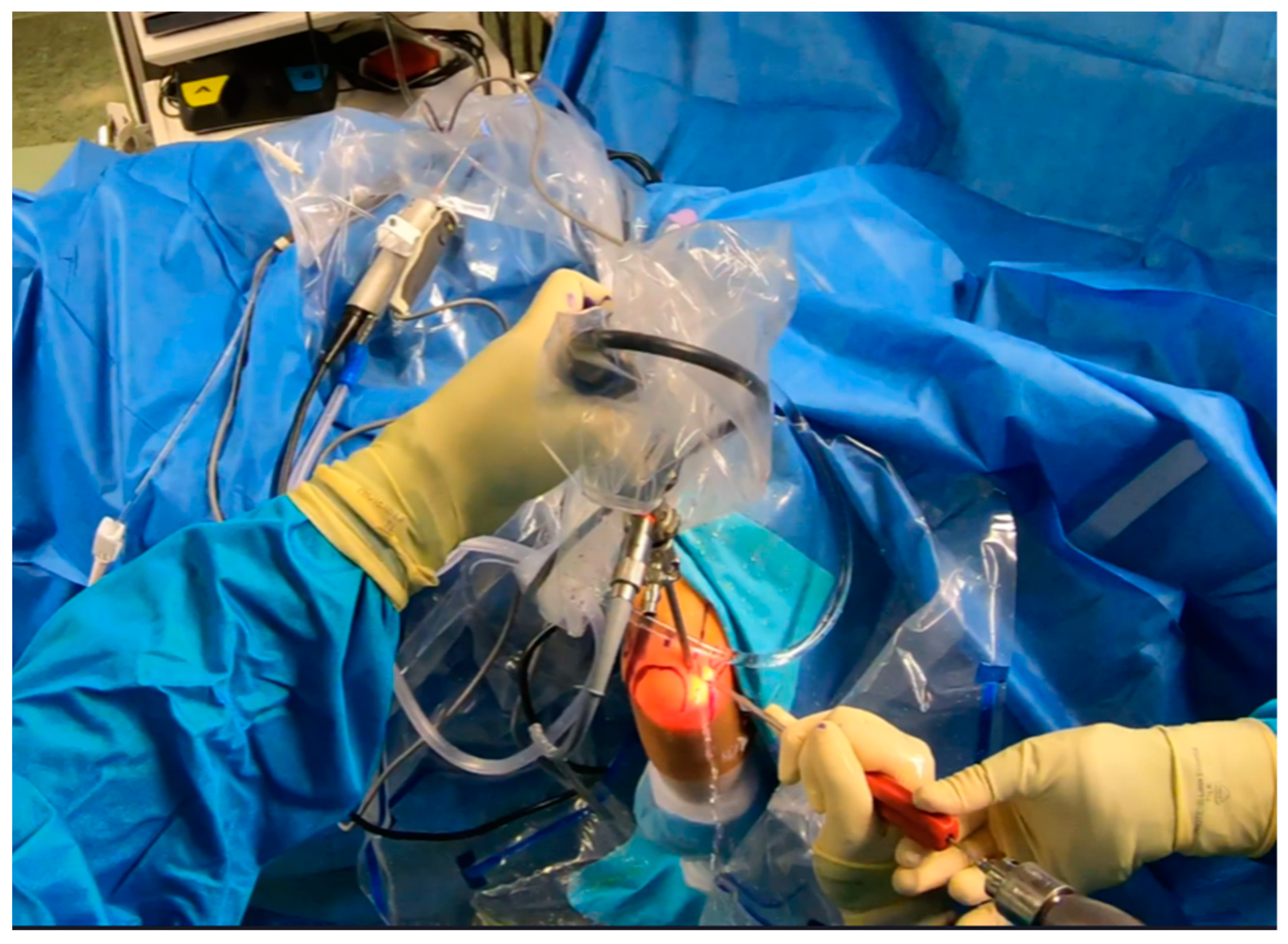
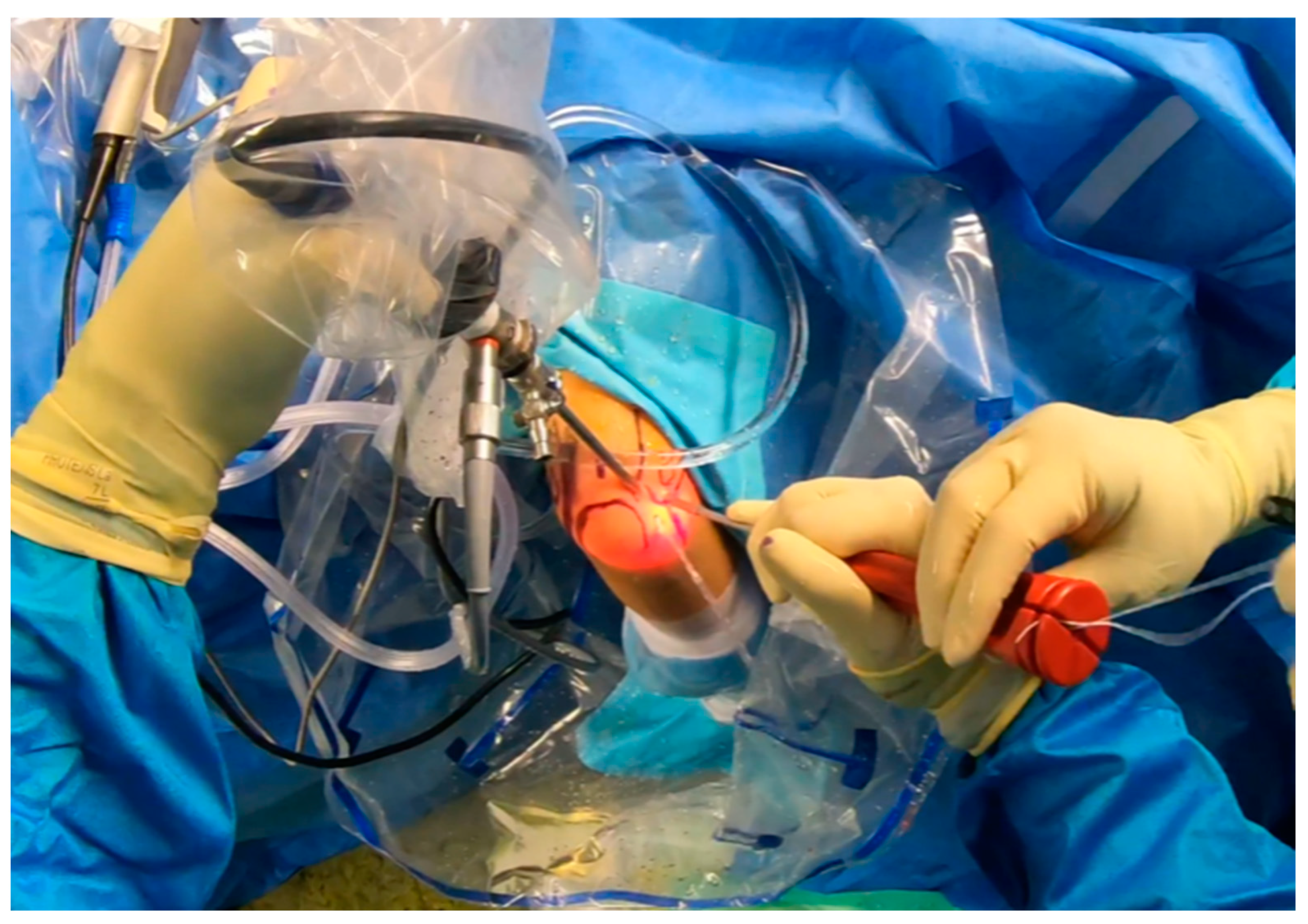
- It utilizes arthroscopic minimally invasive techniques, which minimize potential iatrogenic instability; in contrast, open procedures can exacerbate elbow instability, which is challenging to rectify [38].
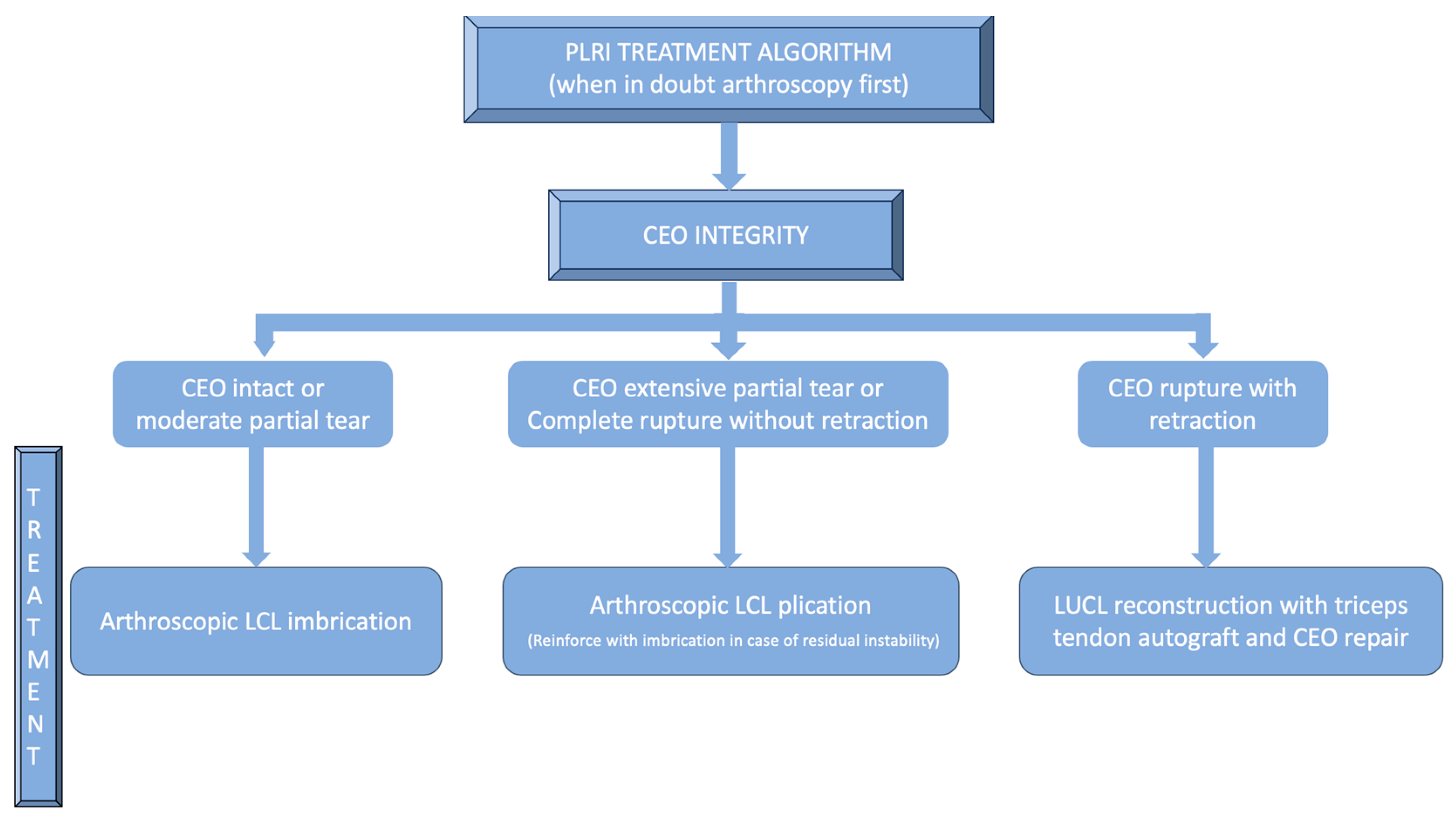
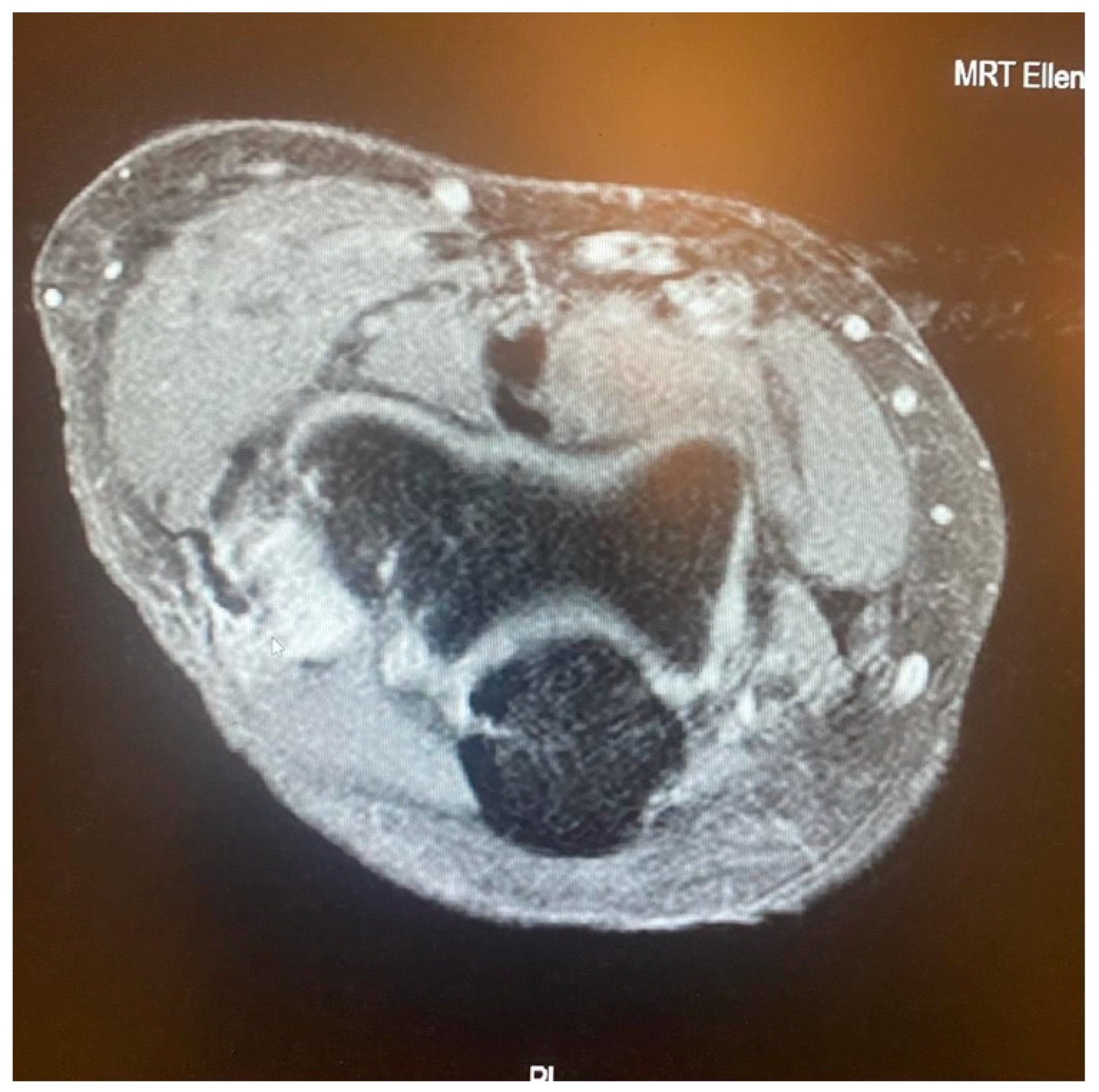
- It is contingent on the integrity of the CEO, whether it is intact, has a moderate or extensive partial tear, or is completely ruptured with or without retraction. This evaluation can be conveniently conducted via MRI.
5. PLRI Treatment
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marinelli, A.; Graves, B.R.; Bain, G.I.; Pederzini, L. Treatment of elbow instability: State of the art. J. ISAKOS 2021, 6, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Carlier, Y.; Soubeyrand, M. Chronic elbow instability in adults: The why, when and how of ligament reconstruction. Orthop. Traumatol. Surg. Res. 2023, 109, 103449. [Google Scholar] [CrossRef] [PubMed]
- Kohlprath, R.; Vuylsteke, K.; van Riet, R. Arthroscopic lateral collateral ligament imbrication of the elbow: Short-term clinical results. J. Shoulder Elb. Surg. 2022, 31, 2316–2321. [Google Scholar] [CrossRef] [PubMed]
- Badhrinarayanan, S.; Desai, A.; Watson, J.J.; White, C.H.R.; Phadnis, J. Indications, Outcomes, and Complications of Lateral Ulnar Collateral Ligament Reconstruction of the Elbow for Chronic Posterolateral Rotatory Instability: A Systematic Review. Am. J. Sports Med. 2021, 49, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Amarasooriya, M.; Phadnis, J. Arthroscopic Diagnosis of Posterolateral Rotatory Instability of the Elbow. Arthrosc. Tech. 2020, 9, e1951–e1956. [Google Scholar] [CrossRef]
- Noriego, D.; Carrera, A.; Tubbs, R.S.; Guibernau, J.; San Millán, M.; Iwanaga, J.; Cateura, A.; Sañudo, J.; Reina, F. The lateral ulnar collateral ligament: Anatomical and structural study for clinical application in the diagnosis and treatment of elbow lateral ligament injuries. Clin. Anat. 2023, 36, 866–874. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Morrey, B.F.; Korinek, S.; An, K.N. Elbow subluxation and dislocation. A spectrum of instability. Clin. OrthopRelat Res. 1992, 280, 186–197. [Google Scholar] [PubMed]
- O’Driscoll, S.W.; Bell, D.F.; Morrey, B.F. Posterolateral rotatory instability of the elbow. J. Bone Jt. Surg. Am. 1991, 73, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, P.; Cucchi, D.; D’Ambrosi, R.; Butt, U.; Safran, M.R.; Denard, P.; Randelli, P. Intra-articular findings in symptomatic minor instability of the lateral elbow (SMILE). Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Chaney, G.K. Preoperative and operative risk factors for failed lateral collateral ligament reconstruction. JSES Int. 2023, 7, 2578–2586. [Google Scholar] [CrossRef]
- Dunning, C.E.; Zarzour, Z.D.; Patterson, S.D.; Johnson, J.A.; King, G.J. Ligamentous stabilizers against posterolateral rotatory instability of the elbow. J. Bone Jt. Surg. Am. 2001, 83, 1823–1828. [Google Scholar] [CrossRef] [PubMed]
- Imatani, J.; Ogura, T.; Morito, Y.; Hashizume, H.; Inoue, H. Anatomic and histologic studies of lateral collateral ligament complex of the elbow joint. J. Shoulder Elb. Surg. 1999, 8, 625–627. [Google Scholar] [CrossRef] [PubMed]
- Anakwenze, O.A.; Kwon, D.; O’Donnell, E.; Levine, W.N.; Ahmad, C.S. Surgical treatment of posterolateral rotatory instability of the elbow. Arthrosc. J. Arthrosc. Relat. Surg. 2014, 30, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, D.; Dynin, M.; MacDonnell, J.R.; Kessler, M.W. The role of arthroscopy in chronic elbow instability. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 2029–2036. [Google Scholar] [CrossRef] [PubMed]
- Scheiderer, B.; Imhoff, F.B.; Kia, C.; Aglio, J.; Morikawa, D.; Obopilwe, E.; Cote, M.P.; Lacheta, L.; Imhoff, A.B.; Mazzocca, A.D.; et al. LUCL internal bracing restores posterolateral rotatory stability of the elbow. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Conti Mica, M.; Caekebeke, P.; van Riet, R. Lateral collateral ligament injuries of the elbow—Chronic posterolateral rotatory instability (PLRI). EFORT Open Rev. 2017, 1, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Sachinis, N.P.; Yiannakopoulos, C.K.; Beitzel, K.; Koukos, C. Arthroscopic Modified Elbow Lateral Collateral Ligament Imbrication: An Operative Technique. Arthrosc. Tech. 2023, 12, e709–e714. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.E.; Shamrock, A.G.; Wolf, B.R. Posterolateral Rotary Instability of the Elbow in Adolescents: A Report of 2 Cases and Review of the Literature. JBJS Case Connect. 2019, 9, e0504. [Google Scholar] [CrossRef] [PubMed]
- Kholinne, E.; Liu, H.; Kim, H.; Kwak, J.M.; Koh, K.H.; Jeon, I.H. Systematic Review of Elbow Instability in Association With Refractory Lateral Epicondylitis: Myth or Fact? Am. J. Sports Med. 2021, 49, 2542–2550. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.M.; Müller, K.; Hollinger, B.; Nietschke, R.; Zimmerer, A.; Ries, C.; Burkhart, K.J. Lateral Ulnar Collateral Ligament Reconstruction for Posterolateral Rotatory Instability after Failed Common Extensor Origin Release: Outcomes at Minimum 2-Year Follow-up. Orthop. J. Sports Med. 2022, 10, 23259671211069340. [Google Scholar] [CrossRef]
- Schnetzke, M.; Ellwein, A.; Maier, D.; Wagner, F.C.; Grützner, P.A.; Guehring, T. Injury patterns following simple elbow dislocation: Radiological analysis implies existence of a pure valgus dislocation mechanism. Arch. Orthop. Trauma Surg. 2021, 141, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Kim, S.T.; Lee, K.H.; Ahn, J.M.; Gong, H.S. Radiocapitellar incongruity of the radial head in magnetic resonance imaging correlates with pathologic changes of the lateral elbow stabilizers in lateral epicondylitis. PLoS ONE 2021, 16, e0254037. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.Y.; Lee, M.H.; Jeon, I.H.; Chung, H.W.; Lee, S.H.; Shin, M.J. Lateral epicondylitis: Associations of MR imaging and clinical assessments with treatment options in patients receiving conservative and arthroscopic managements. Eur. Radiol. 2018, 28, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Fedorka, C.J.; Oh, L.S. Posterolateral rotatory instability of the elbow. Curr. Rev. Musculoskelet. Med. 2016, 9, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Seki, A.; Olsen, B.S.; Jensen, S.L.; Eygendaal, D.; Søjbjerg, J.O. Functional anatomy of the lateral collateral ligament complex of the elbow: Configuration of Y and its role. J. Shoulder Elb. Surg. 2002, 11, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.A.; Bain, G.I. Posterolateral rotatory instability of the elbow. J. Am. Acad. Orthop. Surg. 2004, 12, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Regan, W.; Lapner, P.C. Prospective evaluation of two diagnostic apprehension signs for posterolateral instability of the elbow. J. Shoulder Elb. Surg. 2006, 15, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Hackl, M.; Wegmann, K.; Ries, C.; Leschinger, T.; Burkhart, K.J.; Müller, L.P. Reliability of Magnetic Resonance Imaging Signs of Posterolateral Rotatory Instability of the Elbow. J. Hand Surg. Am. 2015, 40, 1428–1433. [Google Scholar] [CrossRef] [PubMed]
- Pierreux, P.; Caekebeke, P.; van Riet, R. The role of arthroscopy in instability of the elbow. JSES Int. 2022, 7, 2594–2599. [Google Scholar] [CrossRef]
- Mahasupachai, N.; Samathi, N.; Premsiri, A.; Chanlalit, C. The sonographic posterolateral rotatory stress test: Normal ulnohumeral gap difference in healthy volunteers. J. Orthop. Surg. 2022, 30, 1–7. [Google Scholar] [CrossRef]
- Walz, D.M.; Newman, J.S.; Konin, G.P.; Ross, G. Epicondylitis: Pathogenesis, imaging, and treatment. Radiographics 2010, 30, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Bredella, M.A.; Tirman, P.F.; Fritz, R.C.; Feller, J.F.; Wischer, T.K.; Genant, H.K. MR imaging findings of lateral ulnar collateral ligament abnormalities in patients with lateral epicondylitis. AJR Am. J. Roentgenol. 1999, 173, 1379–1382. [Google Scholar] [CrossRef] [PubMed]
- Savoie, F.H., 3rd; Field, L.D.; Gurley, D.J. Arthroscopic and open radial ulnohumeral ligament reconstruction for posterolateral rotatory instability of the elbow. Hand Clin. 2009, 25, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Badre, A.; Axford, D.T.; Banayan, S.; Johnson, J.A.; King, G.J.W. Role of the anconeus in the stability of a lateral ligament and common extensor origin-deficient elbow: An in vitro biomechanical study. J. Shoulder Elb. Surg. 2019, 28, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.L., Jr.; Murphy, K.P.; Gottlob, C.A.; Curd, D.T. Arthroscopic classification and treatment of lateral epicondylitis: Two-year clinical results. J. Shoulder Elb. Surg. 2000, 9, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Savoie, F.H., 3rd; O’Brien, M.J.; Field, L.D.; Gurley, D.J. Arthroscopic and open radial ulnohumeral ligament reconstruction for posterolateral rotatory instability of the elbow. Clin. Sports Med. 2010, 29, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Caekebeke, P.; Mica, M.A.C.; van Riet, R. Evaluation and Management of Posterolateral Rotatory Instability (PLRI). In The Unstable Elbow; Tashjian, R., Ed.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Daniels, S.D.; France, T.J.; Peek, K.J.; Tucker, N.J.; Baldini, T.; Catalano, L.W.; Lauder, A. Posterolateral Rotatory Instability Develops Following the Modified Kocher Approach and Does Not Resolve Following Interval Repair. J. Bone Jt. Surg. Am. 2023, 105, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Schoch, C.; Dittrich, M.; Seilern Und Aspang, J.; Geyer, M.; Geyer, S. Autologous triceps tendon graft for LUCL reconstruction of the elbow: Clinical outcome after 7.5 years. Eur. J. Orthop. Surg. Traumatol. 2022, 32, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Dehlinger, F.; Ries, C.; Hollinger, B. LUCL-Bandplastik mit Trizepssehnentransplantat zur Therapie der posterolateralen Rotationsinstabilität am Ellenbogen. Oper. Orthop. Traumatol. 2014, 26, 414–429. [Google Scholar] [CrossRef] [PubMed]
- Chanlalit, C.; Mahasupachai, N.; Sakdapanichkul, C. Arthroscopic lateral collateral ligament imbrication for treatment of atraumatic posterolateral rotatory instability. J. Orthop. Surg. 2022, 30, 1–7. [Google Scholar] [CrossRef]
- Lannes, X.; Traverso, A.; Wehrli, L.; Goetti, P. Douleurs latérales du coude chez l’adulte: Algorithme de prise en charge [Support algorithm for lateral elbow pain syndrome in adults]. Rev. Med. Suisse 2023, 19, 2336–2343. (In French) [Google Scholar] [CrossRef] [PubMed]
- Eigenschink, M.; Pauzenberger, L.; Laky, B.; Ostermann, R.C.; Anderl, W.; Heuberer, P.R. Lateral ulnar collateral ligament reconstruction using an autologous triceps tendon graft for subclinical posterolateral rotatory instability in recalcitrant lateral epicondylitis. J. Shoulder Elb. Surg. 2023, 32, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Tranier, M.; Bacle, G.; Marteau, E.; Sos, C.; Laulan, J.; Roulet, S. Lateral elbow ligament reconstruction for posterolateral rotatory instability: 10 years follow-up in 32 patients. JSES Int. 2022, 7, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.P. Revisiting the anatomy and biomechanics of the anconeus muscle and its role in elbow stability. Ann. Anat. 2013, 195, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Delgove, A.; Weigert, R.; Casoli, V. Evaluation of donor site morbidity after medial triceps brachii free flap for lower limb reconstruction. Arch. Orthop. Trauma Surg. 2017, 137, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Chow, H.Y.; Eygendaal, D.; The, B. Elbow arthroscopy—Indications and technique. J. Clin. Orthop. Trauma 2021, 19, 147–153. [Google Scholar] [CrossRef] [PubMed]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koukos, C.; Kotsapas, M.; Sidiropoulos, K.; Traverso, A.; Bilsel, K.; Montoya, F.; Arrigoni, P. A Novel Surgical Treatment Management Algorithm for Elbow Posterolateral Rotatory Instability (PLRI) Based on the Common Extensor Origin Integrity. J. Clin. Med. 2024, 13, 2411. https://doi.org/10.3390/jcm13082411
Koukos C, Kotsapas M, Sidiropoulos K, Traverso A, Bilsel K, Montoya F, Arrigoni P. A Novel Surgical Treatment Management Algorithm for Elbow Posterolateral Rotatory Instability (PLRI) Based on the Common Extensor Origin Integrity. Journal of Clinical Medicine. 2024; 13(8):2411. https://doi.org/10.3390/jcm13082411
Chicago/Turabian StyleKoukos, Christos, Michail Kotsapas, Konstantinos Sidiropoulos, Aurélien Traverso, Kerem Bilsel, Fredy Montoya, and Paolo Arrigoni. 2024. "A Novel Surgical Treatment Management Algorithm for Elbow Posterolateral Rotatory Instability (PLRI) Based on the Common Extensor Origin Integrity" Journal of Clinical Medicine 13, no. 8: 2411. https://doi.org/10.3390/jcm13082411