
Fluorescence-Guided Laparoscopy after Oral Hypericin Administration for Staging of Locally Advanced Gastric Cancer—A Pilot Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Drug Treatment
2.3. Inclusion/Exclusion Criteria
2.4. Trial Approval and Consent to Participate
2.5. Study Conduct
2.6. Laparoscopy
2.7. Determination of Hypericin
2.8. Statistical Analysis and Data Availability
2.9. Safety Analysis
3. Results
3.1. Study Enrollment and Patient Characteristics
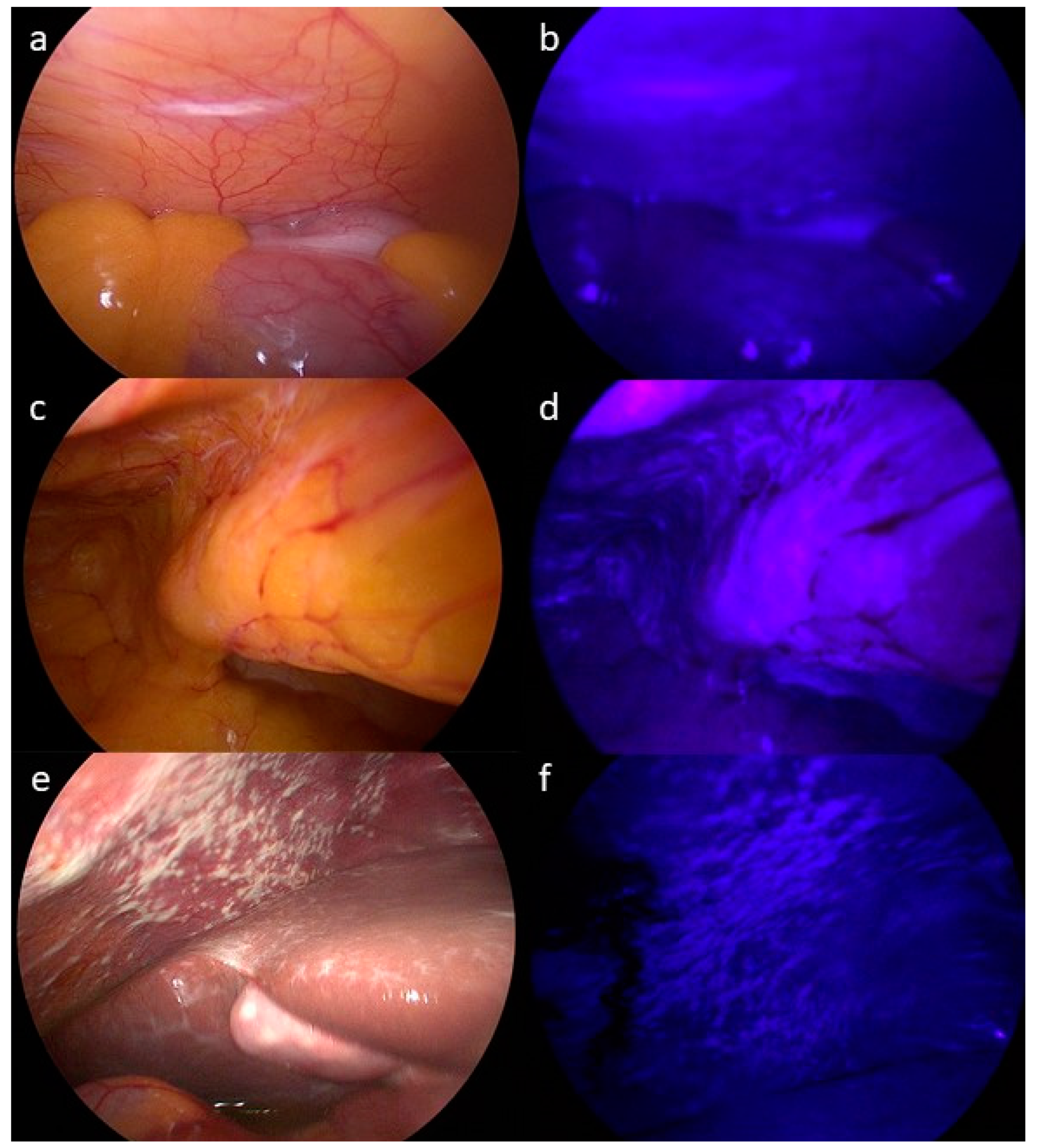
3.2. Assessment of PM by CT, White Light (WLL) and Fluorescence-Guided Laparoscopy (FGL)
3.3. Accuracy of CT, WLL and FGL in Detecting PM
3.4. Safety Assessment
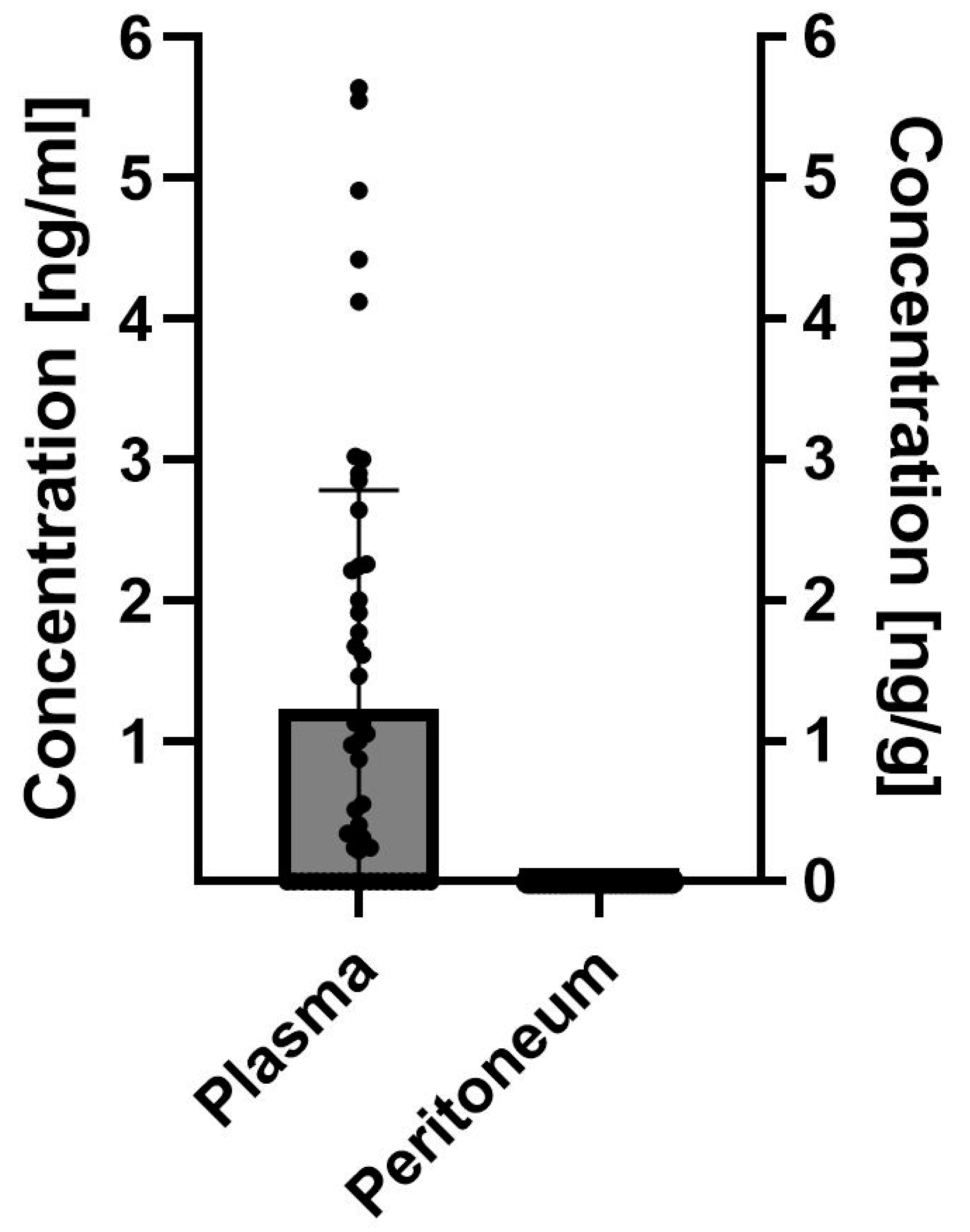
3.5. Determination of Hypericin in Serum and Peritoneal Tissue Samples
3.6. Photodynamic Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yarema, R.; Ohorchak, M.; Hyrya, P.; Kovalchuk, Y.; Safiyan, V.; Karelin, I.; Ferneza, S.; Fetsych, M.; Matusyak, M.; Oliynyk, Y.; et al. Gastric cancer with peritoneal metastases: Efficiency of standard treatment methods. World J. Gastrointest. Oncol. 2020, 12, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Koemans, W.J.; Lurvink, R.J.; Grootscholten, C.; Verhoeven, R.H.A.; de Hingh, I.H.; van Sandick, J.W. Synchronous peritoneal metastases of gastric cancer origin: Incidence, treatment and survival of a nationwide Dutch cohort. Gastric Cancer 2021, 24, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, H.H.; Kim, Y.H.; Hwang, S.H.; Lee, H.S.; Park, D.J.; Kim, S.Y.; Lee, K.H. Peritoneal metastasis: Detection with 16- or 64-detector row CT in patients undergoing surgery for gastric cancer. Radiology 2009, 253, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; Committee, E.G. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.F.; Scalon, F.M.; Scalon, M.M.; Dias, D.I. Staging laparoscopy in gastric cancer to detect peritoneal metastases: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1315–1321. [Google Scholar] [CrossRef]
- Xu, S.; Bulin, A.L.; Hurbin, A.; Elleaume, H.; Coll, J.L.; Broekgaarden, M. Photodynamic Diagnosis and Therapy for Peritoneal Carcinomatosis: Emerging Perspectives. Cancers 2020, 12, 2491. [Google Scholar] [CrossRef] [PubMed]
- Casas, A. Clinical uses of 5-aminolaevulinic acid in photodynamic treatment and photodetection of cancer: A review. Cancer Lett. 2020, 490, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.; Arend, J.; Wolff, S.; Perrakis, A.; Rahimli, M.; Negrini, V.R.; Stockheim, J.; Lorenz, E.; Croner, R. Tumor visualization and fluorescence angiography with indocyanine green (ICG) in laparoscopic and robotic hepatobiliary surgery—Valuation of early adopters from Germany. Innov. Surg. Sci. 2021, 6, 59–66. [Google Scholar] [CrossRef]
- Harada, Y.; Murayama, Y.; Takamatsu, T.; Otsuji, E.; Tanaka, H. 5-Aminolevulinic Acid-Induced Protoporphyrin IX Fluorescence Imaging for Tumor Detection: Recent Advances and Challenges. Int. J. Mol. Sci. 2022, 23, 6478. [Google Scholar] [CrossRef]
- Inoue, K.; Fukuhara, H.; Yamamoto, S.; Karashima, T.; Kurabayashi, A.; Furihata, M.; Hanazaki, K.; Lai, H.W.; Ogura, S.I. Current status of photodynamic technology for urothelial cancer. Cancer Sci. 2022, 113, 392–398. [Google Scholar] [CrossRef]
- McCracken, D.J.; Schupper, A.J.; Lakomkin, N.; Malcolm, J.; Painton Bray, D.; Hadjipanayis, C.G. Turning on the light for brain tumor surgery: A 5-aminolevulinic acid story. Neuro Oncol. 2022, 24, S52–S61. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Roskams, T.; de Witte, P.A. Antivascular tumor eradication by hypericin-mediated photodynamic therapy. Photochem. Photobiol. 2002, 76, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Kamuhabwa, A.A.; Di Mavungu, J.D.; Baert, L.; D’Hallewin, M.A.; Hoogmartens, J.; de Witte, P.A. Determination of hypericin in human plasma by high-performance liquid chromatography after intravesical administration in patients with transitional cell carcinoma of the bladder. Eur. J. Pharm. Biopharm. 2005, 59, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Sarissky, M.; Lavicka, J.; Kocanova, S.; Sulla, I.; Mirossay, A.; Miskovsky, P.; Gajdos, M.; Mojzis, J.; Mirossay, L. Diazepam enhances hypericin-induced photocytotoxicity and apoptosis in human glioblastoma cells. Neoplasma 2005, 52, 352–359. [Google Scholar] [PubMed]
- Seitz, G.; Warmann, S.W.; Armeanu, S.; Heitmann, H.; Ruck, P.; Hoffman, R.M.; Fuchs, J.; Wessels, J.T. In vitro photodynamic therapy of childhood rhabdomyosarcoma. Int. J. Oncol. 2007, 30, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Tian, R.; Koyabu, N.; Morimoto, S.; Shoyama, Y.; Ohtani, H.; Sawada, Y. Functional induction and de-induction of P-glycoprotein by St. John’s wort and its ingredients in a human colon adenocarcinoma cell line. Drug Metab. Dispos. 2005, 33, 547–554. [Google Scholar] [CrossRef] [PubMed]
- VanderWerf, Q.M.; Saxton, R.E.; Chang, A.; Horton, D.; Paiva, M.B.; Anderson, J.; Foote, C.; Soudant, J.; Mathey, A.; Castro, D.J. Hypericin: A new laser phototargeting agent for human cancer cells. Laryngoscope 1996, 106, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Yee, K.K.; Soo, K.C.; Olivo, M. Anti-angiogenic effects of Hypericin-photodynamic therapy in combination with Celebrex in the treatment of human nasopharyngeal carcinoma. Int. J. Mol. Med. 2005, 16, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Naderi, M.; Rahmani Cherati, M.; Mohammadian, A.; Baghery Bidhendy, M.; Ghiasvand, S.; Zare Marzouni, H.; Aryan, H.; Jangholi, E.; Javidi, M.A. Hypericin Induces Apoptosis in AGS Cell Line with No Significant Effect on Normal Cells. Iran. J. Pharm. Res. 2020, 19, 349–357. [Google Scholar] [CrossRef]
- Buľková, V.; Vargová, J.; Babinčák, M.; Jendželovský, R.; Zdráhal, Z.; Roudnický, P.; Košuth, J.; Fedoročko, P. New findings on the action of hypericin in hypoxic cancer cells with a focus on the modulation of side population cells. Biomed. Pharmacother. 2023, 163, 114829. [Google Scholar] [CrossRef]
- Ritz, R.; Muller, M.; Weller, M.; Dietz, K.; Kuci, S.; Roser, F.; Tatagiba, M. Hypericin: A promising fluorescence marker for differentiating between glioblastoma and neurons in vitro. Int. J. Oncol. 2005, 27, 1543–1549. [Google Scholar] [PubMed]
- Schempp, C.M.; Muller, K.A.; Winghofer, B.; Schopf, E.; Simon, J.C. St. John’s wort (Hypericum perforatum L.). A plant with relevance for dermatology. Hautarzt 2002, 53, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Schulz, V. Incidence and clinical relevance of the interactions and side effects of Hypericum preparations. Phytomedicine 2001, 8, 152–160. [Google Scholar] [PubMed]
- Jichlinski, P.; Leisinger, H.J. Fluorescence cystoscopy in the management of bladder cancer: A help for the urologist! Urol. Int. 2005, 74, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Olivo, M. Bio-distribution and subcellular localization of Hypericin and its role in PDT induced apoptosis in cancer cells. Int. J. Oncol. 2002, 21, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Buytaert, E.; Callewaert, G.; Hendrickx, N.; Scorrano, L.; Hartmann, D.; Missiaen, L.; Vandenheede, J.R.; Heirman, I.; Grooten, J.; Agostinis, P. Role of endoplasmic reticulum depletion and multidomain proapoptotic BAX and BAK proteins in shaping cell death after hypericin-mediated photodynamic therapy. FASEB J. 2006, 20, 756–758. [Google Scholar] [CrossRef] [PubMed]
- Du, H.Y.; Olivo, M.; Tan, B.K.; Bay, B.H. Hypericin-mediated photodynamic therapy induces lipid peroxidation and necrosis in nasopharyngeal cancer. Int. J. Oncol. 2003, 23, 1401–1405. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.D.; Krysko, D.V.; Verfaillie, T.; Kaczmarek, A.; Ferreira, G.B.; Marysael, T.; Rubio, N.; Firczuk, M.; Mathieu, C.; Roebroek, A.J.; et al. A novel pathway combining calreticulin exposure and ATP secretion in immunogenic cancer cell death. EMBO J. 2012, 31, 1062–1079. [Google Scholar] [CrossRef]
- Mikes, J.; Koval, J.; Jendzelovsky, R.; Sackova, V.; Uhrinova, I.; Kello, M.; Kulikova, L.; Fedorocko, P. The role of p53 in the efficiency of photodynamic therapy with hypericin and subsequent long-term survival of colon cancer cells. Photochem. Photobiol. Sci. 2009, 8, 1558–1567. [Google Scholar] [CrossRef]
- Rubio, N.; Coupienne, I.; Di Valentin, E.; Heirman, I.; Grooten, J.; Piette, J.; Agostinis, P. Spatiotemporal autophagic degradation of oxidatively damaged organelles after photodynamic stress is amplified by mitochondrial reactive oxygen species. Autophagy 2012, 8, 1312–1324. [Google Scholar] [CrossRef]
- Diwu, Z.; Lown, J.W. Photosensitization with anticancer agents. 17. EPR studies of photodynamic action of hypericin: Formation of semiquinone radical and activated oxygen species on illumination. Free Radic. Biol. Med. 1993, 14, 209–215. [Google Scholar] [CrossRef]
- Delaey, E.; Vandenbogaerde, A.; Merlevede, W.; de Witte, P. Photocytotoxicity of hypericin in normoxic and hypoxic conditions. J. Photochem. Photobiol. B 2000, 56, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Kamuhabwa, A.R.; Agostinis, P.M.; D’Hallewin, M.A.; Baert, L.; de Witte, P.A. Cellular photodestruction induced by hypericin in AY-27 rat bladder carcinoma cells. Photochem. Photobiol. 2001, 74, 126–132. [Google Scholar] [CrossRef]
- Blank, M.; Kostenich, G.; Lavie, G.; Kimel, S.; Keisari, Y.; Orenstein, A. Wavelength-dependent properties of photodynamic therapy using hypericin in vitro and in an animal model. Photochem. Photobiol. 2002, 76, 335–340. [Google Scholar] [CrossRef]
- Theodossiou, T.A.; Hothersall, J.S.; De Witte, P.A.; Pantos, A.; Agostinis, P. The multifaceted photocytotoxic profile of hypericin. Mol. Pharm. 2009, 6, 1775–1789. [Google Scholar] [CrossRef] [PubMed]
- Alecu, M.; Ursaciuc, C.; Halalau, F.; Coman, G.; Merlevede, W.; Waelkens, E.; de Witte, P. Photodynamic treatment of basal cell carcinoma and squamous cell carcinoma with hypericin. Anticancer. Res. 1998, 18, 4651–4654. [Google Scholar] [PubMed]
- Kacerovska, D.; Pizinger, K.; Majer, F.; Smid, F. Photodynamic therapy of nonmelanoma skin cancer with topical hypericum perforatum extract--a pilot study. Photochem. Photobiol. 2008, 84, 779–785. [Google Scholar] [CrossRef]
- Rook, A.H.; Wood, G.S.; Duvic, M.; Vonderheid, E.C.; Tobia, A.; Cabana, B. A phase II placebo-controlled study of photodynamic therapy with topical hypericin and visible light irradiation in the treatment of cutaneous T-cell lymphoma and psoriasis. J. Am. Acad. Dermatol. 2010, 63, 984–990. [Google Scholar] [CrossRef]
- Bhuvaneswari, R.; Gan, Y.Y.; Lucky, S.S.; Chin, W.W.; Ali, S.M.; Soo, K.C.; Olivo, M. Molecular profiling of angiogenesis in hypericin mediated photodynamic therapy. Mol. Cancer 2008, 7, 56. [Google Scholar] [CrossRef]
- Kamuhabwa, A.A.; Cosserat-Gerardin, I.; Didelon, J.; Notter, D.; Guillemin, F.; Roskams, T.; D’Hallewin, M.A.; Baert, L.; de Witte, P.A. Biodistribution of hypericin in orthotopic transitional cell carcinoma bladder tumors: Implication for whole bladder wall photodynamic therapy. Int. J. Cancer 2002, 97, 253–260. [Google Scholar] [CrossRef]
- Kamuhabwa, A.A.; Roskams, T.; D’Hallewin, M.A.; Baert, L.; Van Poppel, H.; de Witte, P.A. Whole bladder wall photodynamic therapy of transitional cell carcinoma rat bladder tumors using intravesically administered hypericin. Int. J. Cancer 2003, 107, 460–467. [Google Scholar] [CrossRef]
- Urla, C.; Armeanu-Ebinger, S.; Fuchs, J.; Seitz, G. Successful in vivo tumor visualization using fluorescence laparoscopy in a mouse model of disseminated alveolar rhabdomyosarcoma. Surg. Endosc. 2015, 29, 1105–1114. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Peritoneal-plasma barrier. Cancer Treat. Res. 1996, 82, 53–63. [Google Scholar] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 2010, 1, 100–107. [Google Scholar] [CrossRef]
- Staffeldt, B.; Kerb, R.; Brockmoller, J.; Ploch, M.; Roots, I. Pharmacokinetics of hypericin and pseudohypericin after oral intake of the hypericum perforatum extract LI 160 in healthy volunteers. J. Geriatr. Psychiatry Neurol. 1994, 7 (Suppl. S1), S47–S53. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Wang, J.; Ni, Y.; Chen, F. Necrosis avidity: A newly discovered feature of hypericin and its preclinical applications in necrosis imaging. Theranostics 2013, 3, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Orth, K.; Russ, D.; Steiner, R.; Beger, H.G. Fluorescence detection of small gastrointestinal tumours: Principles, technique, first clinical experience. Langenbecks Arch. Surg. 2000, 385, 488–494. [Google Scholar] [CrossRef]
- Ladner, D.P.; Steiner, R.A.; Allemann, J.; Haller, U.; Walt, H. Photodynamic diagnosis of breast tumours after oral application of aminolevulinic acid. Br. J. Cancer 2001, 84, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Matsuyama, H.; Kawai, T.; Ikeda, A.; Miyake, M.; Nishimoto, K.; Matsushita, Y.; Komura, K.; Abe, T.; Kume, H.; et al. Bladder cancer prospective cohort study on high-risk non-muscle invasive bladder cancer after photodynamic diagnosis-assisted transurethral resection of the bladder tumor (BRIGHT study). Int. J. Urol. 2022, 29, 632–638. [Google Scholar] [CrossRef]
- Kobayashi, K.; Matsuyama, H.; Oka, S.; Nakamura, K.; Misumi, T.; Hiroyoshi, T.; Ito, H.; Isoyama, N.; Hirata, H.; Matsumoto, H.; et al. Risks and benefits of transurethral resection of the bladder tumor using photodynamic diagnosis with oral 5-aminolevulinic acid hydrochloride according to age and history of recurrence in patients with non-muscle invasive bladder cancer. Photodiagn. Photodyn. Ther. 2023, 41, 103294. [Google Scholar] [CrossRef]
- Taoka, R.; Matsuoka, Y.; Yamasaki, M.; Kani, N.; Honda, T.; Harada, S.; Tohi, Y.; Kato, T.; Okazoe, H.; Tsunemori, H.; et al. Photodynamic diagnosis-assisted transurethral resection using oral 5-aminolevulinic acid decreases residual cancer and improves recurrence-free survival in patients with non-muscle-invasive bladder cancer. Photodiagn. Photodyn. Ther. 2022, 38, 102838. [Google Scholar] [CrossRef] [PubMed]
- Kishi, K.; Fujiwara, Y.; Yano, M.; Motoori, M.; Sugimura, K.; Ohue, M.; Noura, S.; Marubashi, S.; Takahashi, H.; Sakon, M. Diagnostic laparoscopy with 5-aminolevulinic-acid-mediated photodynamic diagnosis enhances the detection of peritoneal micrometastases in advanced gastric cancer. Oncology 2014, 87, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Wurglics, M.; Schubert-Zsilavecz, M. Hypericum perforatum: A ‘modern’ herbal antidepressant: Pharmacokinetics of active ingredients. Clin. Pharmacokinet. 2006, 45, 449–468. [Google Scholar] [CrossRef] [PubMed]
- Wagner, B.R.; Adamus, A.L.; Hempfling, L.; Vahdad, R.; Haap-Hoff, A.; Heinrich, B.; Vázquez, O.; Jank, P.; Denkert, C.; Seitz, G. Increasing the efficiency of hyperthermic intraperitoneal chemotherapy (HIPEC) by combination with a photosensitive drug in pediatric rhabdomyosarcoma in an animal model. Pediatr. Blood Cancer 2022, 69, e29864. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Treated Per Protocol [PP] (n = 50) | |
|---|---|
| Sex—n (%) | |
| Female | 17 (34) |
| Male | 33 (66) |
| Age–Median (min–max) | |
| Years | 62.7 (27–86) |
| Ethnicity—n (%) | |
| Caucasian | 50 (100) |
| Location of tumor—n (%) | |
| Esophagogastric junction | 22 (44) |
| Corpus ventriculi | 24 (48) |
| Antrum ventriculi | 4 (8) |
| Tumor extension—n (%) | |
| cT1 | 0 (0) |
| cT2 | 5 (10) |
| cT3 | 26 (52) |
| cT4 | 1 (2) |
| cTx | 18 (36) |
| Nodal status—n (%) | |
| cN0 | 6 (12) |
| cN+ | 43 (86) |
| cNx | 1 (2) |
| Metastasis—n (%) | |
| cM0 | 42 (84) |
| cM1 | 8 (16) |
| Grade of differentiation—n (%) | |
| G1 | 0 (0) |
| G2 | 14 (28) |
| G3 | 32 (64) |
| Gx | 4 (8) |
| Neoadjuvant chemotherapy prior to laparoscopy—n (%) | |
| Yes | 10 (20) |
| No | 40 (80) |
| Sensitivity | Specificity | |
|---|---|---|
| Computed tomography (CT) | 6 of 16 (37.5%) | 32 of 34 (94.1%) |
| White light laparoscopy (WLL) | 16 of 16 (100%) | 23 of 34 (67.6%) |
| Fluorescence-guided laparoscopy (FGL) | 13 of 16 (81.3%) | 22 of 34 (64.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yurttas, C.; Horvath, P.; Fischer, I.; Wagner, S.; Thiel, K.; Ladurner, R.; Königsrainer, I.; Königsrainer, A.; Schwab, M.; Beckert, S.; et al. Fluorescence-Guided Laparoscopy after Oral Hypericin Administration for Staging of Locally Advanced Gastric Cancer—A Pilot Study. J. Clin. Med. 2024, 13, 2422. https://doi.org/10.3390/jcm13082422
Yurttas C, Horvath P, Fischer I, Wagner S, Thiel K, Ladurner R, Königsrainer I, Königsrainer A, Schwab M, Beckert S, et al. Fluorescence-Guided Laparoscopy after Oral Hypericin Administration for Staging of Locally Advanced Gastric Cancer—A Pilot Study. Journal of Clinical Medicine. 2024; 13(8):2422. https://doi.org/10.3390/jcm13082422
Chicago/Turabian StyleYurttas, Can, Philipp Horvath, Imma Fischer, Silvia Wagner, Karolin Thiel, Ruth Ladurner, Ingmar Königsrainer, Alfred Königsrainer, Matthias Schwab, Stefan Beckert, and et al. 2024. "Fluorescence-Guided Laparoscopy after Oral Hypericin Administration for Staging of Locally Advanced Gastric Cancer—A Pilot Study" Journal of Clinical Medicine 13, no. 8: 2422. https://doi.org/10.3390/jcm13082422