
Usefulness of Combined Measurement of Surfactant Protein D, Thrombin–Antithrombin III Complex, D-Dimer, and Plasmin–α2 Plasmin Inhibitor Complex in Acute Exacerbation of Interstitial Lung Disease: A Retrospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
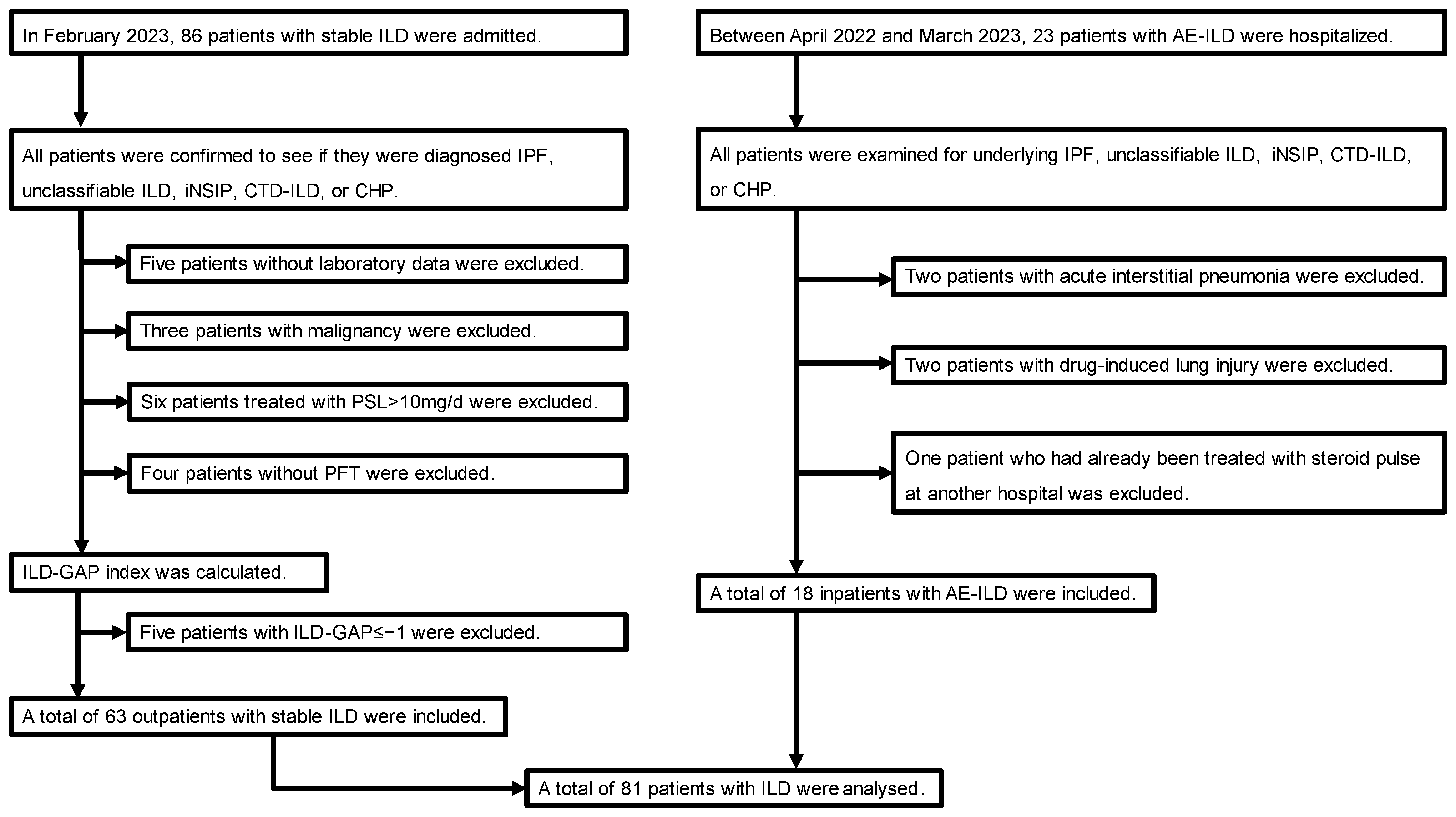
2.1. Study Design and Patients
2.2. Definition of AE-ILD
2.3. Definition of Disseminated Intravascular Coagulation (DIC)
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Patient Background
3.2. Comparison of Laboratory Findings between the Stable ILD and AE-ILD Groups
3.3. Characteristics of Patients with AE-ILD
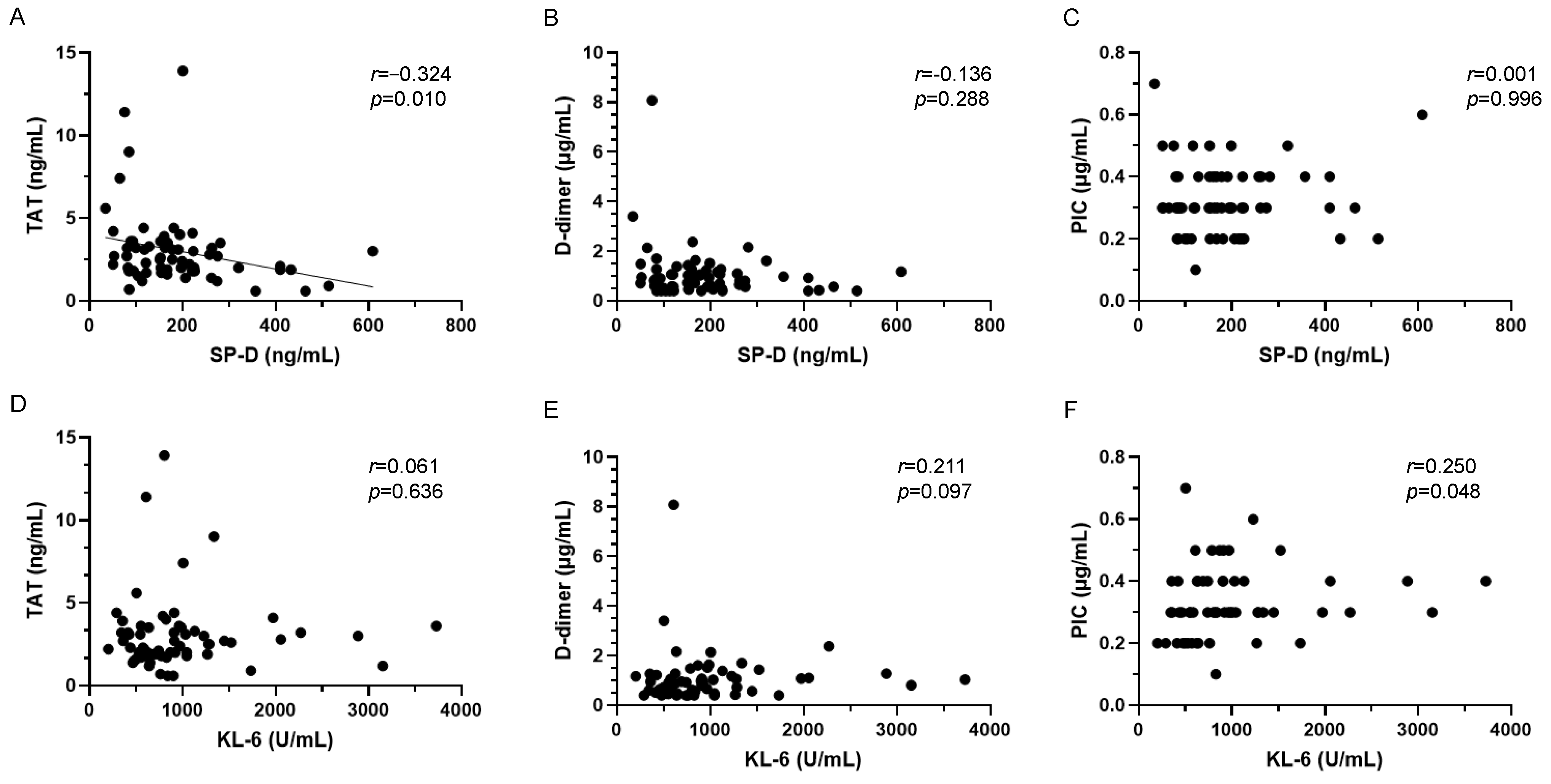
3.4. Relationships between Alveolar Epithelial Injury and Coagulopathy Markers in AE-ILD
3.5. Relationships between Alveolar Epithelial Injury and Coagulopathy Markers in Stable ILD
3.6. AE-ILD Diagnostic Accuracy of Alveolar Epithelial Injury and Coagulopathy Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leuschner, G.; Behr, J. Acute exacerbation in interstitial lung disease. Front. Med. 2017, 4, 176. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, C.D.; Batra, K.; Torrealba, J.R.; Terada, L.S. Characteristics and evaluation of acute exacerbations in chronic interstitial lung diseases. Respir. Med. 2021, 183, 106400. [Google Scholar] [CrossRef] [PubMed]
- José, R.J.; Williams, A.E.; Chambers, R.C. Proteinase-activated receptors in fibroproliferative lung disease. Thorax 2014, 69, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Borensztajn, K.; Spek, C.A. Targeting coagulation factor receptors–protease-activated receptors in idiopathic pulmonary fibrosis. J. Thromb. Haemost. 2017, 15, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Fujii, M.; Hayakawa, H.; Urano, T.; Sato, A.; Chida, K.; Nakamura, H.; Takada, A. Relevance of tissue factor and tissue factor pathway inhibitor for hypercoagulable state in the lungs of patients with idiopathic pulmonary fibrosis. Thromb. Res. 2000, 99, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Navaratnam, V.; Fogarty, A.W.; McKeever, T.; Thompson, N.; Jenkins, G.; Johnson, S.R.; Dolan, G.; Kumaran, M.; Pointon, K.; Hubbard, R.B. Presence of a prothrombotic state in people with idiopathic pulmonary fibrosis: A population-based case-control study. Thorax 2014, 69, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, G.; Acquah, S.O.; Salvatore, M.; Padilla, M.L. Elevated serum D-dimer level is associated with an increased risk of acute exacerbation in interstitial lung disease. Respir. Med. 2017, 128, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Song, J.W.; Hong, S.B.; Lim, C.M.; Koh, Y.; Kim, D.S. Acute exacerbation of idiopathic pulmonary fibrosis: Incidence, risk factors and outcome. Eur. Respir. J. 2011, 37, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, K.; Yamaguchi, K.; Kono, Y.; Yokoyama, T.; Kubo, K.; Matsumura, T.; Ichimura, Y.; Abe, M.; Terada, J.; Tatsumi, K. Thrombomodulin for acute exacerbations of idiopathic pulmonary fibrosis: A proof of concept study. Pulm. Pharmacol. Ther. 2014, 29, 233–240. [Google Scholar] [CrossRef]
- Imokawa, S.; Sato, A.; Hayakawa, H.; Kotani, M.; Urano, T.; Takada, A. Tissue factor expression and fibrin deposition in the lungs of patients with idiopathic pulmonary fibrosis and systemic sclerosis. Am. J. Respir. Crit. Care Med. 1997, 156, 631–636. [Google Scholar] [CrossRef]
- Koyama, K.; Katayama, S.; Tonai, K.; Shima, J.; Koinuma, T.; Nunomiya, S. Biomarker profiles of coagulopathy and alveolar epithelial injury in acute respiratory distress syndrome with idiopathic/immune-related disease or common direct risk factors. Crit. Care 2019, 23, 283. [Google Scholar] [CrossRef] [PubMed]
- Ohshimo, S.; Ishikawa, N.; Horimasu, Y.; Hattori, N.; Hirohashi, N.; Tanigawa, K.; Kohno, N.; Bonella, F.; Guzman, J.; Costabel, U. Baseline KL-6 predicts increased risk for acute exacerbation of idiopathic pulmonary fibrosis. Respir. Med. 2014, 108, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Collard, H.R.; Calfee, C.S.; Wolters, P.J.; Song, J.W.; Hong, S.B.; Brady, S.; Ishizaka, A.; Jones, K.D.; King, T.E., Jr.; Matthay, M.A.; et al. Plasma biomarker profiles in acute exacerbation of idiopathic pulmonary fibrosis. Am. J. Physiol. Lung Cell. Mol. Physiol. 2010, 299, L3–L7. [Google Scholar] [CrossRef]
- Ryerson, C.J.; Vittinghoff, E.; Ley, B.; Lee, J.S.; Mooney, J.J.; Jones, K.D.; Elicker, B.M.; Wolters, P.J.; Koth, L.L.; King, T.E., Jr.; et al. Predicting survival across chronic interstitial lung disease: The ILD-GAP model. Chest 2014, 145, 723–728. [Google Scholar] [CrossRef]
- Collard, H.R.; Ryerson, C.J.; Corte, T.J.; Jenkins, G.; Kondoh, Y.; Lederer, D.J.; Lee, J.S.; Maher, T.M.; Wells, A.U.; Antoniou, K.M.; et al. Acute exacerbation of idiopathic pulmonary fibrosis. An international working group report. Am. J. Respir. Crit. Care Med. 2016, 194, 265–275. [Google Scholar] [CrossRef]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef]
- Patel, P.; Walborn, A.; Rondina, M.; Fareed, J.; Hoppensteadt, D. Markers of inflammation and infection in sepsis and disseminated intravascular coagulation. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619843338. [Google Scholar] [CrossRef] [PubMed]
- Nahm, F.S. Receiver operating characteristic curve: Overview and practical use for clinicians. Korean J. Anesthesiol. 2022, 75, 25–36. [Google Scholar] [CrossRef]
- Muller, M.P.; Tomlinson, G.; Marrie, T.J.; Tang, P.; McGeer, A.; Low, D.E.; Detsky, A.S.; Gold, W.L. Can routine laboratory tests discriminate between severe acute respiratory syndrome and other causes of community-acquired pneumonia? Clin. Infect. Dis. 2005, 40, 1079–1086. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, P.; Badagabettu, S.N.; Lewis, M.G.; Adiga, M.; Padur, A.A. Determination of Spearman correlation coefficient (r) to evaluate the linear association of dermal collagen and elastic fibers in the perspectives of skin injury. Dermatol. Res. Pract. 2018, 2018, 4512840. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Levi, M.; Toh, C.H. Disseminated intravascular coagulation. Nat. Rev. Dis. Primers 2016, 2, 16037. [Google Scholar] [CrossRef] [PubMed]
- Giustozzi, M.; Ehrlinder, H.; Bongiovanni, D.; Borovac, J.A.; Guerreiro, R.A.; Gąsecka, A.; Papakonstantinou, P.E.; Parker, W.A.E. Coagulopathy and sepsis: Pathophysiology, clinical manifestations and treatment. Blood Rev. 2021, 50, 100864. [Google Scholar] [CrossRef] [PubMed]
- Oda, K.; Ishimoto, H.; Yamada, S.; Kushima, H.; Ishii, H.; Imanaga, T.; Harada, T.; Ishimatsu, Y.; Matsumoto, N.; Naito, K.; et al. Autopsy analyses in acute exacerbation of idiopathic pulmonary fibrosis. Respir. Res. 2014, 15, 109. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Kida, H.; Ogata, Y.; Marumo, S.; Matsuoka, H.; Gohma, I.; Yamamoto, S.; Mori, M.; Sugimoto, C.; Tachibana, K.; et al. Efficacy of recombinant thrombomodulin for poor prognostic cases of acute exacerbation in idiopathic interstitial pneumonia: Secondary analysis of the SETUP trial. BMJ Open Respir. Res. 2020, 7, e000558. [Google Scholar] [CrossRef] [PubMed]
- Borensztajn, K.; Crestani, B.; Kolb, M. Idiopathic pulmonary fibrosis: From epithelial injury to biomarkers–insights from the bench side. Respiration 2013, 86, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Sokai, A.; Tanizawa, K.; Handa, T.; Kanatani, K.; Kubo, T.; Ikezoe, K.; Nakatsuka, Y.; Tokuda, S.; Oga, T.; Hirai, T.; et al. Importance of serial changes in biomarkers in idiopathic pulmonary fibrosis. ERJ Open Res. 2017, 3, 00019-2016. [Google Scholar] [CrossRef] [PubMed]
- Drakopanagiotakis, F.; Markart, P.; Steiropoulos, P. Acute exacerbations of interstitial lung diseases: Focus on biomarkers. Int. J. Mol. Sci. 2023, 24, 10196. [Google Scholar] [CrossRef] [PubMed]
- Nishikiori, H.; Chiba, H.; Ariki, S.; Kuronuma, K.; Otsuka, M.; Shiratori, M.; Ikeda, K.; Watanabe, A.; Kuroki, Y.; Takahashi, H. Distinct compartmentalization of SP-A and SP-D in the vasculature and lungs of patients with idiopathic pulmonary fibrosis. BMC Pulm. Med. 2014, 14, 196. [Google Scholar] [CrossRef]
- Rai, M.; Parthasarathi, A.; Beeraka, N.M.; Kaleem Ullah, M.; Malamardi, S.; Padukudru, S.; Siddaiah, J.B.; Uthaiah, C.A.; Vishwanath, P.; Chaya, S.K.; et al. Circulatory Serum Krebs von Den Lungen-6 and Surfactant Protein-D Concentrations Predict Interstitial Lung Disease Progression and Mortality. Cells 2023, 12, 1281. [Google Scholar] [CrossRef]
- Zhong, D.; Wu, C.; Bai, J.; Hu, C.; Xu, D.; Wang, Q.; Zeng, X. Comparative diagnostic efficacy of serum Krebs von den Lungen-6 and surfactant D for connective tissue disease-associated interstitial lung diseases: A meta-analysis. Medicine 2020, 99, e19695. [Google Scholar] [CrossRef] [PubMed]
- Awano, N.; Jo, T.; Yasunaga, H.; Inomata, M.; Kuse, N.; Tone, M.; Morita, K.; Matsui, H.; Fushimi, K.; Nagase, T.; et al. Body mass index and in-hospital mortality in patients with acute exacerbation of idiopathic pulmonary fibrosis. ERJ Open Res. 2021, 7, 00037-2021. [Google Scholar] [CrossRef] [PubMed]
- Natsuizaka, M.; Chiba, H.; Kuronuma, K.; Otsuka, M.; Kudo, K.; Mori, M.; Bando, M.; Sugiyama, Y.; Takahashi, H. Epidemiologic survey of Japanese patients with idiopathic pulmonary fibrosis and investigation of ethnic differences. Am. J. Respir. Crit. Care Med. 2014, 190, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Homma, S.; Suda, T.; Hongo, Y.; Yoshida, M.; Hiroi, S.; Iwasaki, K.; Takeshima, T.; Kondoh, Y. Incidence and changes in treatment of acute exacerbation of idiopathic pulmonary fibrosis in Japan: A claims-based retrospective study. Respir. Investig. 2022, 60, 798–805. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | Points |
|---|---|---|
| Plt (×103/μL) | >100 | 0 |
| 50–100 | 1 | |
| <50 | 2 | |
| PT-INR | <1.3 | 0 |
| 1.3–1.7 | 1 | |
| >1.7 | 2 | |
| D-dimer (μg/mL) | <0.4 | 0 |
| 0.4–4.0 | 2 | |
| >4.0 | 3 | |
| Fibrinogen (mg/dL) | >100 | 0 |
| <100 | 1 |
| Variables | Stable ILD | AE-ILD | p-Value |
|---|---|---|---|
| (n = 63) | (n = 18) | ||
| Demographic | |||
| Age (years) | 75.0 (72.0, 80.5) | 76.0 (74.0, 80.0) | 0.645 |
| Male sex (%) | 37 (58.7) | 13 (72.2) | 0.412 |
| BMI (kg/m2) | 24.48 (22.30, 25.85) (N/A = 14) | 20.66 (19.63, 23.85) (N/A = 1) | 0.004 |
| Smoking history (%) | 36 (63.2) (N/A = 6) | 15 (83.3) | 0.150 |
| Baseline ILD | |||
| IPF (%) | 37 (58.7) | 14 (77.8) | 0.174 |
| Unclassifiable ILD (%) | 8 (12.7) | 0 (0.0) | 0.189 |
| iNSIP (%) | 8 (12.7) | 2 (11.1) | >0.999 |
| CTD-ILD (%) | 7 (11.1) | 1 (5.6) | 0.677 |
| CHP (%) | 3 (4.8) | 1 (5.6) | >0.999 |
| Baseline treatment | |||
| Corticosteroids (%) | 22 (34.9) | 3 (16.7) | 0.162 |
| Immunosuppressants (%) | 1 (1.6) | 2 (11.1) | 0.123 |
| Antifibrosis drugs (%) | 36 (57.1) | 9 (50.0) | 0.603 |
| Anticoagulant drugs (%) | 3 (4.8) | 6 (33.3) | 0.003 |
| Home oxygen therapy (%) | 14 (22.2) | 7 (38.9) | 0.221 |
| Laboratory Findings | Stable ILD | AE-ILD | p-Value |
|---|---|---|---|
| (n = 63) | (n = 18) | ||
| CRP (mg/dL) | 0.16 (0.11, 0.63) | 12.45 (5.94, 17.27) | <0.001 |
| LDH (U/L) | 229 (196, 262) | 387 (272, 478) (N/A = 1) | <0.001 |
| PCT (ng/mL) | 0.05 (0.03, 0.06) | 0.16 (0.12, 0.47) (N/A = 1) | <0.001 |
| IL-6 (pg/mL) | 3.7 (2.3, 7.5) | 28.5 (6.8, 125.7) | <0.001 |
| KL-6 (U/mL) | 803 (562, 1043) | 1132 (687, 1651) (N/A = 1) | 0.068 |
| SP-D (ng/mL) | 167 (102, 224) | 386 (172, 461) | 0.005 |
| Plt (×103/μL) | 221 (181, 262) | 217 (204, 276) | 0.725 |
| PT-INR (s) | 0.94 (0.92, 0.97) | 1.07 (1.00, 1.13) | <0.001 |
| Fibrinogen (mg/dL) | 353 (313, 404) | 564 (470, 693) (N/A = 1) | <0.001 |
| TAT (ng/mL) | 2.5 (1.9, 3.4) | 10.6 (3.3, 17.8) | <0.001 |
| D-dimer (μg/mL) | 0.88 (0.57, 1.20) | 3.57 (2.07, 7.81) | <0.001 |
| PIC (μg/mL) | 0.3 (0.3, 0.4) | 0.5 (0.4, 0.6) | <0.001 |
| P | Baseline | Hospitalization | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age (y) | Sex | ILD | ILD Treatment | DIC Score | Code Status | Treatment in Combination with Steroid Pulse | Oxygen Device | Hospitalization (Days) | Outcome | |
| 1 | 81 | M | CHP | None | 3 | DNI | – | HFOT | 22 | Survivor |
| 2 | 72 | M | IPF | None | 2 | Full | – | HFOT | 12 | |
| 3 | 79 | F | IPF | Nintedanib | 0 | Full | – | None | 10 | |
| 4 | 83 | F | iNSIP | None | 3 | DNI | – | HFOT | 23 | |
| 5 | 75 | M | IPF | None | 3 | DNI | Tacrolimus | HFOT | 35 | |
| 6 | 76 | F | iNSIP | None | 2 | DNI | Tacrolimus | NPPV | 36 | |
| 7 | 76 | M | IPF | Nintedanib | 2 | DNI | PMX-DHP | HFOT | 20 | |
| 8 | 74 | F | IPF | Pirfenidone + PSL (9 mg/d) | 4 | DNI | Tacrolimus | HFOT | 19 | |
| 9 | 73 | M | IPF | Nintedanib | 2 | Full | – | COT | 11 | |
| 10 | 71 | M | IPF | Pirfenidone | 3 | DNI | Tacrolimus + PMX-DHP | HFOT | 40 | Non-survivor |
| 11 | 80 | M | IPF | Nintedanib | 3 | DNI | Tacrolimus + PMX-DHP | HFOT | 23 | |
| 12 | 80 | F | IPF | Tacrolimus | 3 | DNI | Tacrolimus + PMX-DHP | HFOT | 16 | |
| 13 | 75 | M | IPF | Nintedanib | 5 | DNI | Tacrolimus + PMX-DHP | NPPV | 38 | |
| 14 | 74 | M | IPF | None | 2 | Full | – | MV | 33 | |
| 15 | 80 | M | CTD-ILD | Azathioprine + PSL (5 mg/d) | 2 | DNI | Tacrolimus + PMX-DHP | HFOT | 8 | |
| 16 | 82 | M | IPF | Nintedanib | 2 | DNI | Tacrolimus | HFOT | 27 | |
| 17 | 79 | M | IPF | None | 3 | Full | Tacrolimus + PMX-DHP | MV | 23 | |
| 18 | 56 | M | IPF | Pirfenidone + PSL (20 mg) | 3 | DNI | Tacrolimus + PMX-DHP | NPPV | 11 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeshita, Y.; To, M.; Kurosawa, Y.; Furusho, N.; Kinouchi, T.; Tsushima, K.; Tada, Y.; To, Y.; Sakao, S. Usefulness of Combined Measurement of Surfactant Protein D, Thrombin–Antithrombin III Complex, D-Dimer, and Plasmin–α2 Plasmin Inhibitor Complex in Acute Exacerbation of Interstitial Lung Disease: A Retrospective Cohort Study. J. Clin. Med. 2024, 13, 2427. https://doi.org/10.3390/jcm13082427
Takeshita Y, To M, Kurosawa Y, Furusho N, Kinouchi T, Tsushima K, Tada Y, To Y, Sakao S. Usefulness of Combined Measurement of Surfactant Protein D, Thrombin–Antithrombin III Complex, D-Dimer, and Plasmin–α2 Plasmin Inhibitor Complex in Acute Exacerbation of Interstitial Lung Disease: A Retrospective Cohort Study. Journal of Clinical Medicine. 2024; 13(8):2427. https://doi.org/10.3390/jcm13082427
Chicago/Turabian StyleTakeshita, Yuichiro, Masako To, Yusuke Kurosawa, Naho Furusho, Toru Kinouchi, Kenji Tsushima, Yuji Tada, Yasuo To, and Seiichiro Sakao. 2024. "Usefulness of Combined Measurement of Surfactant Protein D, Thrombin–Antithrombin III Complex, D-Dimer, and Plasmin–α2 Plasmin Inhibitor Complex in Acute Exacerbation of Interstitial Lung Disease: A Retrospective Cohort Study" Journal of Clinical Medicine 13, no. 8: 2427. https://doi.org/10.3390/jcm13082427