
Enhancing Cranio-Maxillofacial Fracture Care in Low- and Middle-Income Countries: A Systematic Review

 , , , ,
, , , , {kind=link}
Abstract
:1. Introduction
2. Material and Methods
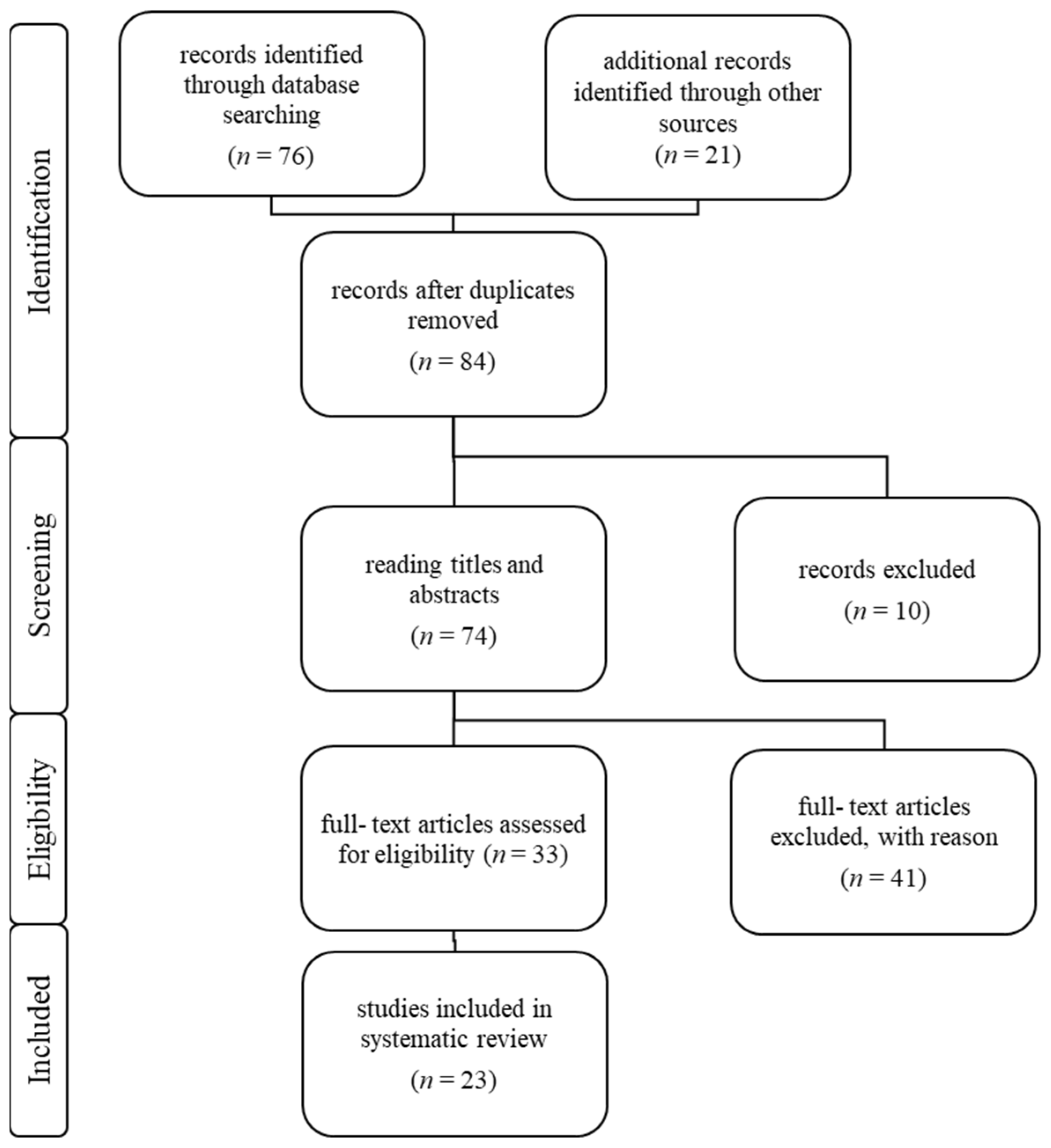
2.1. Literature Search
2.2. Study Selection
2.3. Risk of Bias [37]
2.4. Data Extraction and Categorization
- Category I: Teaching.
- Digital teaching;
- On-site teaching;
- Fellowships abroad.
- Category II: Transfer of the patient to specialized national clinics.
- Category III: Off-label and non-operative solutions.
3. Results of the Literature Search by Category
3.1. Category 1: Digital Teaching
3.1.1. Digital Teaching Platforms
3.1.2. On-Site Teaching
3.1.3. Fellowships Abroad
3.2. Category II: Transfer of the Patient to Specialized National Clinics
3.3. Category III: Off-Label and Non-Operative Solutions
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Rossiter, N.D. Trauma—The forgotten pandemic? Int. Orthop. 2022, 46, 3–11. [Google Scholar] [CrossRef] [PubMed]
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 21 June 2023).
- Available online: https://data.worldbank.org/indicator/SH.MED.SAOP.P5?end=2018&name_desc=false&start=2008&view=chart (accessed on 21 June 2023).
- Ibrahim, N.A.; Ajani, A.W.O.; Mustafa, I.A.; Balogun, R.A.; Oludara, M.A.; Idowu, O.E.; Solagberu, B.A. Road Traffic Injury in Lagos, Nigeria: Assessing Prehospital Care. Prehosp. Disaster Med. 2017, 32, 424–430. [Google Scholar] [CrossRef]
- Nielsen, K.; Mock, C.; Joshipura, M.; Rubiano, A.M.; Zakariah, A.; Rivara, F. Assessment of the status of prehospital care in 13 low- and middle-income countries. Prehosp. Emerg. Care 2012, 16, 381–389. [Google Scholar] [CrossRef]
- Quake, S.Y.L.; Khoda, F.; Rad, A.A.; Ponniah, H.S.; Vardanyan, R.; Frisoni, P.; Rad, H.A.; Brasesco, M.; Mustoe, S.; Godfrey, J.; et al. The Current Status and Challenges of Prehospital Trauma Care in Low- and Middle-Income Countries: A Systematic Review. Prehosp. Emerg. Care 2023, 28, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Marin, F. Access to oral & maxillofacial surgery in Sub-Saharan African countries. J. Oral Biol. Craniofac. Res. 2021, 11, 608–611. [Google Scholar] [CrossRef]
- Tissingh, E.K.; Marais, L.; Loro, A.; Bose, D.; Paner, N.T.; Ferguson, J.; Morgensten, M.; McNally, M. Management of fracture-related infection in low resource settings: How applicable are the current consensus guidelines? EFORT Open Rev. 2022, 7, 422–432. [Google Scholar] [CrossRef]
- ORCA Study Group. Open tibial shaft fractures: Treatment patterns in sub-Saharan Africa. OTA Int. 2023, 6, e228. [Google Scholar] [CrossRef]
- Kurdin, A.; Caines, A.; Boone, D.; Furey, A. TEAM: A Low-Cost Alternative to ATLS for Providing Trauma Care Teaching in Haiti. J. Surg. Educ. 2018, 75, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Kim, J.; Heo, J.; Nguyen, D.T.N.; Nguyen, S.H.; Kim, W.H. Outcomes of trauma education workshop in Vietnam: Improving diagnostic and surgical skills. BMC Med. Educ. 2020, 20, 267. [Google Scholar] [CrossRef]
- Callese, T.E.; Richards, C.T.; Shaw, P.; Schuetz, S.J.; Issa, N.; Paladino, L.; Swaroop, M. Layperson trauma training in low- and middle-income countries: A review. J. Surg. Res. 2014, 190, 104–110. [Google Scholar] [CrossRef]
- Anderson, G.A.; Kayima, P.; Ilcisin, L.; Benitez, N.P.; Albutt, K.H.; Briggs, S.M.; Nehra, D. Development of a Comprehensive Trauma Training Curriculum for the Resource-Limited Environment. J. Surg. Educ. 2018, 75, 1317–1324. [Google Scholar] [CrossRef]
- Jaber, M.A.; AlQahtani, F.; Bishawi, K.; Kuriadom, S.T. Patterns of Maxillofacial Injuries in the Middle East and North Africa: A Systematic Review. Int. Dent. J. 2021, 71, 292–299. [Google Scholar] [CrossRef]
- Kanala, S.; Gudipalli, S.; Perumalla, P.; Jagalanki, K.; Polamarasetty, P.V.; Guntaka, S.; Gudala, A.; Boyapati, R.P. Aetiology, prevalence, fracture site and management of maxillofacial trauma. Ann. R. Coll. Surg. Engl. 2021, 103, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Adeleke, A.I.; Hlongwa, M.; Makhunga, S.; Ginindza, T.G. Epidemiology of maxillofacial injury among adults in sub-Saharan Africa: A scoping review. Inj. Epidemiol. 2023, 10, 58. [Google Scholar] [CrossRef]
- Vu, H.M.; Dang, A.K.; Tran, T.T.; Vu, G.T.; Truong, N.T.; Nguyen, C.T.; Van Doan, A.; Pham, K.T.H.; Tran, T.H.; Tran, B.X.; et al. Health-Related Quality of Life Profiles among Patients with Different Road Traffic Injuries in an Urban Setting of Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 1462. [Google Scholar] [CrossRef]
- Lalloo, R.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; Roberts, N.L.S.; Sylte, D.O.; et al. Epidemiology of facial fractures: Incidence, prevalence and years lived with disability estimates from the Global Burden of Disease 2017 study. Inj. Prev. 2020, 26 (Suppl. S1), i27–i35. [Google Scholar] [CrossRef]
- Das, D.; Salazar, L. Maxillofacial Trauma: Managing Potentially Dangerous And Disfiguring Complex Injuries. Emerg. Med. Pract. 2017, 19, 1–24. [Google Scholar] [PubMed]
- Bhattacharya, K.K.; Mittal, S.T.; Shetty, S.; Rajagopal, R. Diplopia in blow out fractures. Indian J. Ophthalmol. 2013, 61, 85–86. [Google Scholar] [CrossRef]
- Chang, Y.B.; Xia, J.J.; Gateno, J.; Xiong, Z.; Zhou, X.; Wong, S.T. An automatic and robust algorithm of reestablishment of digital dental occlusion. IEEE Trans. Med. Imaging 2010, 29, 1652–1663. [Google Scholar] [CrossRef]
- Farber, S.J.; Kantar, R.S.; Rodriguez, E.D. Facial Trauma Care in the Austere Environment. J. Spec. Oper. Med. 2018, 18, 62–66. [Google Scholar] [CrossRef]
- Deininger, C.; Hofmann, V.; Necchi, M.; Deininger, S.; Wichlas, F. Off-Label Treatment for Severe Craniomaxillofacial Fractures in Low-Income Countries-A Novel Operation Method with the External Face Fixator. J. Clin. Med. 2022, 11, 1488. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.B.; Choi, S.Y.; Kwon, T.G.; Kim, J.W. Concomitant injuries and complications according to categories of pan-facial fracture: A retrospective study. J. Craniomaxillofac. Surg. 2020, 48, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Moshy, J.R.; Msemakweli, B.S.; Owibingire, S.S.; Sohal, K.S. Pattern of mandibular fractures and helmet use among motorcycle crash victims in Tanzania. Afr. Health Sci. 2020, 20, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Bouguila, J.; Zairi, I.; Khonsari, R.H.; Lankriet, C.; Mokhtar, M.; Adouani, A. Mandibular fracture: A 10-year review of 685 cases treated in Charles-Nicolle Hospital (Tunis-Tunisia). Rev. Stomatol. Chir. Maxillofac. 2009, 110, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Anyanechi, C.E.; Saheeb, B.D. Mandibular sites prone to fracture: Analysis of 174 cases in a Nigerian tertiary hospital. Ghana Med. J. 2011, 45, 111–114. [Google Scholar] [PubMed]
- Goguet, Q.; Lee, S.H.; Longis, J.; Corre, P.; Bertin, H. Intraoperative imaging and navigation with mobile cone-beam CT in maxillofacial surgery. Oral Maxillofac. Surg. 2019, 23, 487–491. [Google Scholar] [CrossRef]
- Avery, L.L.; Susarla, S.M.; Novelline, R.A. Multidetector and three-dimensional CT evaluation of the patient with maxillofacial injury. Radiol. Clin. N. Am. 2011, 49, 183–203. [Google Scholar] [CrossRef]
- Thapliyal, S.; Mowar, A.; Bansal, V. Comparison Between Conventional Titanium Miniplates and Indigenous Detachable Custom made 3D Titanium Plates (VAS 3D Bone Plate) for Fixation of Mandibular Fracture in Mental Foramen Region: A Randomized Clinical Trial and Finite Element Analysis. J. Maxillofac. Oral Surg. 2022, 21, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Schuknecht, B.; Graetz, K. Radiologic assessment of maxillofacial, mandibular, and skull base trauma. Eur. Radiol. 2005, 15, 560–568. [Google Scholar] [CrossRef]
- Yabe, T.; Ozawa, T. Treatment of nasoethmoid-orbital fractures using Kirschner wire fixation of the nasal septum. J. Craniofac. Surg. 2011, 22, 1510–1512. [Google Scholar] [CrossRef]
- Giudice, A.; Colangeli, W.; Cristofaro, M.G. Percutaneous reduction of an isolated zygomatic fracture using a wire suture. Br. J. Oral Maxillofac. Surg. 2013, 51, e201–e202. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.M.; Douglas, P.S. The Kirschner wire guide. Br. J. Oral Maxillofac. Surg. 1994, 32, 48–49. [Google Scholar] [CrossRef]
- Thomaidis, V.; Tsoucalas, G.; Fiska, A. The Hippocratic Method for the Reduction of the Mandibular Dislocation, an Ancient Greek Procedure Still in Use in Maxillofacial Surgery. Acta Med. Acad. 2018, 47, 139–143. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Acero, J. International transfer of knowledge: Training and education in craniomaxillofacial surgery. Contributing to humanitarian aid by teaching the teachers. J. Oral Biol. Craniofac. Res. 2021, 11, 643–651. [Google Scholar] [CrossRef]
- EACMFS. Available online: https://www.eacmfs.org/information/european-lecture-series-2/european-lecture-series-2022-2023-pg1/ (accessed on 17 March 2024).
- IAOMS. Available online: https://www.iaoms.org/nextgen/ (accessed on 17 March 2024).
- Surgicalcore. Available online: https://www.surgicalcore.org/ (accessed on 17 March 2024).
- School for Surgeons. Available online: https://www.schoolforsurgeons.net/ (accessed on 17 March 2024).
- Goldstein, S.D.; Papandria, D.; Linden, A.; Azzie, G.; Borgstein, E.; Calland, J.F.; Finlayson, S.R.; Jani, P.; Klingensmith, M.; Labib, M.; et al. A pilot comparison of standardized online surgical curricula for use in low- and middle-income countries. JAMA Surg. 2014, 149, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Derbew, M.; Beveridge, M.; Howard, A.; Byrne, N. Building surgical research capacity in Africa: The Ptolemy Project. PLoS Med. 2006, 3, e305. [Google Scholar] [CrossRef] [PubMed]
- Ptolemy. Available online: www.ptolemy.ca (accessed on 17 March 2024).
- Harris, J.A.; Beck, N.A.; Niedziela, C.J.; Alvarez, G.A.; Danquah, S.A.; Afshar, S. The global reach of social media in oral and maxillofacial surgery. Oral Maxillofac. Surg. 2022, 27, 513–517. [Google Scholar] [CrossRef]
- Ambroise, B.; Benateau, H.; Prevost, R.; Traore, H.; Hauchard, K.; Dia, H.; Veyssiere, A. The contribution of telemedicine to humanitarian surgery. J. Craniomaxillofac. Surg. 2018, 46, 1368–1372. [Google Scholar] [CrossRef]
- Mohan, H.M.; Fitzgerald, E.; Gokani, V.; Sutton, P.; Harries, R.; Bethune, R.; McDermott, F.D.; Ahmad, J.; Akerele, E.; Ashken, L.; et al. Engagement and role of surgical trainees in global surgery: Consensus statement and recommendations from the Association of Surgeons in Training. Int. J. Surg. 2018, 52, 366–370. [Google Scholar] [CrossRef]
- Taub, P.J.; Lin, A.Y.; Cladis, F.P.; Baker, S.B.; Gooden, C.K.; Kumar, A.; Losee, J.E.; Menard, R.; Starks, R.; Duncan, J.A.; et al. Development of Volunteer International Craniofacial Surgery Missions: The Komedyplast Protocol. J. Craniofac. Surg. 2015, 26, 1151–1155. [Google Scholar] [CrossRef]
- Nagengast, E.S.; Munabi, N.C.O.; Xepoleas, M.; Auslander, A.; Magee, W.P., 3rd; Chong, D. The Local Mission: Improving Access to Surgical Care in Middle-Income Countries. World J. Surg. 2021, 45, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.; Howard, B.M.; Yu, A.; Grey, D.; Hofmann, P.B.; Moren, A.M.; McHembe, M.; Essajee, A.; Mndeme, O.; Peck, J.; et al. A Consortium Approach to Surgical Education in a Developing Country: Educational Needs Assessment. JAMA Surg. 2015, 150, 1074–1078. [Google Scholar] [CrossRef]
- Riviello, R.; Ozgediz, D.; Hsia, R.Y.; Azzie, G.; Newton, M.; Tarpley, J. Role of collaborative academic partnerships in surgical training, education, and provision. World J. Surg. 2010, 34, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Guntaka, P.K.; Harris, J.A.; Niedziela, C.J.; Bass, M.; Afshar, S. The landscape of international oral and maxillofacial surgery collaborations from 1996 to 2020: A scoping review of the published literature. Int. J. Oral Maxillofac. Surg. 2022, 51, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Shaye, D.A.; Tollefson, T.; Shah, I.; Krishnan, G.; Matic, D.; Figari, M.; Lim, T.C.; Aniruth, S.; Schubert, W. Backward Planning a Craniomaxillofacial Trauma Curriculum for the Surgical Workforce in Low-Resource Settings. World J. Surg. 2018, 42, 3514–3519. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, K. One-Year Craniofacial Surgery Fellowship at Chang Gung Memorial Hospital. J. Craniofac. Surg. 2021, 32, e582–e583. [Google Scholar] [CrossRef]
- Porter, M.; Lownie, M.; Cleaton-Jones, P. Maxillofacial injury: A retrospective analysis of time lapse between injury and treatment in a South African academic maxillofacial and oral surgery unit. S. Afr. J. Surg. 2013, 51, 138–142. [Google Scholar] [CrossRef]
- Stanford-Moore, G.B.; Niyigaba, G.; Tuyishimire, G.; Yau, J.; Kulkrani, A.; Nyabyenda, V.; Ncogoza, I.; Shaye, D.A. Effect of Delay of Care for Patients with Craniomaxillofacial Trauma in Rwanda. OTO Open 2022, 6, 2473974X221096032. [Google Scholar] [CrossRef]
- Styazhkin, N. Surgeon Ilizarov and his method. Australas. Nurses J. 1973, 2, 8. [Google Scholar] [PubMed]
- Hihara, M.; Yagura, T.; Takegawa, M.; Kakudo, N.; Morimoto, N.; Kusumoto, K. A novel fixation method for panfacial fracture using an Ilizarov-type external fixator. Trauma Case Rep. 2019, 22, 100214. [Google Scholar] [CrossRef] [PubMed]
- Béogo, R.; Bouletreau, P.; Konsem, T.; Traoré, I.; Coulibaly, A.T.; Ouédraogo, D. Wire internal fixation: An obsolete, yet valuable method for surgical management of facial fractures. Pan Afr. Med. J. 2014, 17, 219. [Google Scholar] [CrossRef] [PubMed]
- Cienfuegos, R.; Sierra, E.; Ortiz, B.; Fernandez, G. Treatment of Palatal Fractures by Osteosynthesis with 2.0-mm Locking Plates as External Fixator. Craniomaxillofac. Trauma Reconstr. 2010, 3, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Moroz, P.J.; Spiegel, D.A. The World Health Organization’s action plan on the road traffic injury pandemic: Is there any action for orthopaedic trauma surgeons? J. Orthop. Trauma 2014, 28 (Suppl. S1), S11–S14. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, P.; Meyer, F.J.; Gajic, O. Successful implementation of modern critical care in the low-resources country Bosnia and Herzegovina: Single-center experience. Med. Klin. Intensivmed. Notfmed. 2022, 117, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Andrews, R.J.; Quintana, L.M. Unpredictable, unpreventable and impersonal medicine: Global disaster response in the 21st century. EPMA J. 2015, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Aguilera, S.; Quintana, L.; Khan, T.; Garcia, R.; Shoman, H.; Caddell, L.; Latifi, R.; Park, K.B.; Garcia, P.; Dempsey, R.; et al. Global health, global surgery and mass casualties: II. Mass casualty centre resources, equipment and implementation. BMJ Glob. Health 2020, 5, e001945. [Google Scholar] [CrossRef] [PubMed]
- O’Flynn, E.; Danial, A.; Gajewski, J. Global Surgery Education and Training Programmes—A Scoping Review and Taxonomy. Indian J. Surg. 2022, 84 (Suppl. S1), 193–206. [Google Scholar] [CrossRef]
- Chawla, S.; Kurani, S.; Wren, S.M.; Stewart, B.; Burnham, G.; Kushner, A.; McIntyre, T. Electricity and generator availability in LMIC hospitals: Improving access to safe surgery. J. Surg. Res. 2018, 223, 136–141. [Google Scholar] [CrossRef]
- Lepard, J.R.; Akbari, S.H.A.; Haji, F.; Davis, M.C.; Harkness, W.; Johnston, J.M. The initial experience of InterSurgeon: An online platform to facilitate global neurosurgical partnerships. Neurosurg. Focus 2020, 48, E15. [Google Scholar] [CrossRef] [PubMed]
- Dyke, C.; Franklin, B.R.; Sweeney, W.B.; Ritter, E.M. Early implementation of Fundamentals of Endoscopic Surgery training using a simulation-based mastery learning curriculum. Surgery 2021, 169, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Toal, G.G.; Gisondi, M.A.; Miller, N.M.; Sebok-Syer, S.S.; Avedian, R.S.; Dixon, W.W. Simulation-Based Mastery Learning to Teach Distal Radius Fracture Reduction. Simul. Healthc. 2021, 16, e176–e180. [Google Scholar] [CrossRef] [PubMed]
- Kryklywy, J.H.; Roach, V.A.; Todd, R.M. Assessing the efficacy of tablet-based simulations for learning pseudo-surgical instrumentation. PLoS ONE 2021, 16, e0245330. [Google Scholar] [CrossRef] [PubMed]
- McGann, K.C.; Melnyk, R.; Saba, P.; Joseph, J.; Glocker, R.J.; Ghazi, A. Implementation of an E-Learning Academic Elective for Hands-On Basic Surgical Skills to Supplement Medical School Surgical Education. J. Surg. Educ. 2021, 78, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, P.; Dragic, S.; Kovacevic, T.; Momcicevic, D.; Festic, E.; Kashyap, R.; Niven, A.S.; Dong, Y.; Gajic, O. Impact of weekly case-based tele-education on quality of care in a limited resource medical intensive care unit. Crit. Care 2019, 23, 220. [Google Scholar] [CrossRef] [PubMed]
- Baird, R.; Kisa, P.; Muzira, A.; Wesonga, A.S.; Sekabira, J.; Butterworth, S.; MacNeily, A.E.; Duffy, D.; Blair, G. Training low-middle-income (LMIC) pediatric surgeons in a high-income country (HIC) program. Pediatr. Surg. Int. 2022, 38, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Merchant, A.I.; Walters, C.B.; Valenzuela, J.; McQueen, K.A.; May, A.K. Creating a Global Acute Care Surgery Fellowship to Meet International Need. J. Surg. Educ. 2017, 74, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Maistry, N.; Patel, N.; Govender, T.; Grieve, A. Voyaging through the paediatric surgical maze: A multi-centre analysis of inter-hospital referrals to Johannesburg, South Africa. J. Pediatr. Surg. 2023, 58, 282–286. [Google Scholar] [CrossRef]
- Conyers, J. Dealing with the Sick Rural Surgery Patient in Need of Transfer. Surg. Clin. N. Am. 2020, 100, 921–936. [Google Scholar] [CrossRef]
- Rai, A.; Jain, A.; Datarkar, A.; Mandora, D. Intermaxillary fixation with two loop wires: The Rai technique. Br. J. Oral Maxillofac. Surg. 2020, 58, 613–614. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deininger, C.; Wichlas, F.; Necchi, M.; Deluca, A.; Deininger, S.; Trieb, K.; Tempfer, H.; Kriechbaumer, L.; Traweger, A. Enhancing Cranio-Maxillofacial Fracture Care in Low- and Middle-Income Countries: A Systematic Review. J. Clin. Med. 2024, 13, 2437. https://doi.org/10.3390/jcm13082437
Deininger C, Wichlas F, Necchi M, Deluca A, Deininger S, Trieb K, Tempfer H, Kriechbaumer L, Traweger A. Enhancing Cranio-Maxillofacial Fracture Care in Low- and Middle-Income Countries: A Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2437. https://doi.org/10.3390/jcm13082437
Chicago/Turabian StyleDeininger, Christian, Florian Wichlas, Marco Necchi, Amelie Deluca, Susanne Deininger, Klemens Trieb, Herbert Tempfer, Lukas Kriechbaumer, and Andreas Traweger. 2024. "Enhancing Cranio-Maxillofacial Fracture Care in Low- and Middle-Income Countries: A Systematic Review" Journal of Clinical Medicine 13, no. 8: 2437. https://doi.org/10.3390/jcm13082437