
The Association of Serum Profile of Transferrin Isoforms with COVID-19 Disease Severity

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients Quantification
2.3. Analysis
2.4. Transferrin Isoforms Determination
2.5. Statistics
3. Results
3.1. Transferrin Isoforms between Samples
3.2. Total Transferrin between Samples
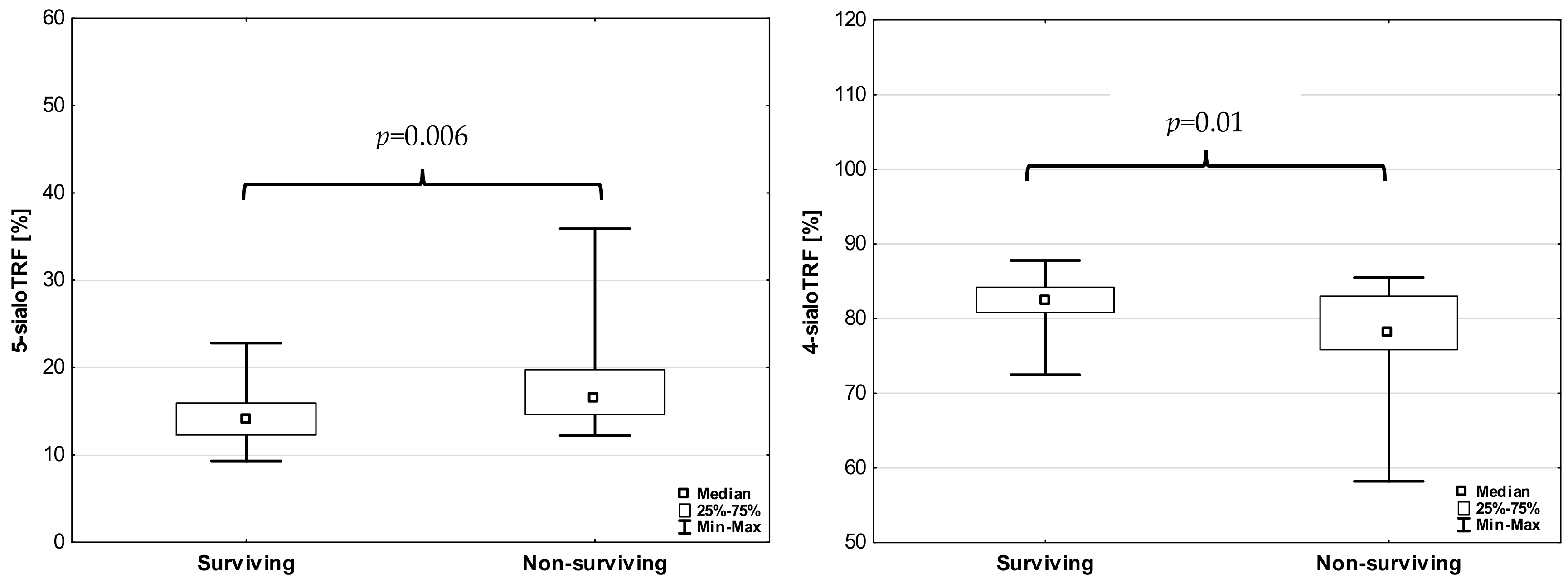
3.3. Transferrin Isoforms According to the Severity of Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umar, A.; Ashraf, M.A.A.; Khan, M.S.; Jafar, K.; Ahmad, S.; Ulfat, Z.; Aslam, M.W.; Waheed, A.; Akmal, H.; Zafar, W.; et al. Clinical investigation of COVID-19 related pneumonia through HRCT chest scan. Biomed. Lett. 2022, 8, 28–33. [Google Scholar] [CrossRef]
- Umar, A.; Ulfat, Z.; Aslam, M.W.; Waheed, A.; Ali, N.; Parveen, S.; Amjad, N.; Wajid, M.; Zafar, A.; Akhtar, M.S.; et al. A mini review on omicron variant of SARS-COV: A new variant of concern (VOC). GSC Biol. Pharm. Sci. 2022, 19, 001–004. [Google Scholar] [CrossRef]
- Zheng, J.; Miao, J.; Guo, R.; Guo, J.; Fan, Z.; Kong, X.; Gao, R.; Yang, L. Mechanism of COVID-19 Causing ARDS: Exploring the Possibility of Preventing and Treating SARS-CoV-2. Front. Cell Infect. Microbiol. 2022, 12, 931061. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A.; Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand. J. Immunol. 2021, 93, e12998. [Google Scholar] [CrossRef] [PubMed]
- de Jong, G.; van Dijk, J.P.; van Eijk, H.G. The biology of transferrin. Clin. Chim. Acta 1990, 190, 1–46. [Google Scholar] [CrossRef]
- van Eijk, H.G.; de Jong, G. The physiology of iron, transferrin, and ferritin. Biol. Trace Elem. Res. 1992, 35, 13–24. [Google Scholar] [CrossRef] [PubMed]
- de Jong, G.; van Eijk, H.G. Microheterogeneity of human serum transferrin: A biological phenomenon studied by isoelectric focusing in immobilized pH gradients. Electrophoresis 1988, 9, 589–598. [Google Scholar] [CrossRef] [PubMed]
- van Pelt, J.; Bakker, J.A.; Velmans, M.H.; Spaapen, L.J. Carbohydrate-deficient transferrin values in neonatal and umbilical cord blood. J. Inherit. Metab. Dis. 1996, 19, 253–266. [Google Scholar] [CrossRef]
- Yang, Z.; Hancock, W.S. Monitoring glycosylation pattern changes of glycoproteins using multi-lectin affinity chromatography. J. Chromatogr. A 2005, 1070, 57–64. [Google Scholar] [CrossRef]
- van Eijk, H.G.; van Noort, W.L.; de Jong, G.; Koster, J.F. Human serum sialo transferrins in diseases. Clin. Chim. Acta 1987, 165, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.; Campion, B.; Decottignies, J.-P.; Montreuil, J.; Spik, G. Physiological significance of the marked increased branching of the glycans of human serotransferrin during pregnancy. Biochem. J. 1989, 257, 231–238. [Google Scholar] [CrossRef] [PubMed]
- de Jong, G.; van Noort, W.L.; Feelders, R.A.; de Jeu-Jaspars, C.M.; van Eijk, H.G. Adaptation of transferrin protein and glycan synthesis. Clin. Chim. Acta 1992, 212, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Gruys, E.; Toussaint, M.J.; Niewold, T.A.; Koopmans, S.J. Acute phase reaction and acute phase proteins. J. Zhejiang Univ. Sci. B 2005, 6, 1045–1056. [Google Scholar] [CrossRef]
- Li, L.; Chen, C. Contribution of acute-phase reaction proteins to the diagnosis and treatment of 2019 novel coronavirus disease (COVID-19). Epidemiol. Infect. 2020, 148, e164. [Google Scholar] [CrossRef] [PubMed]
- Gruszewska, E.; Wrona, A.; Gudowska, M.; Panasiuk, A.; Cylwik, B.; Lipartowska-Klimuk, K.; Flisiak, R.; Chrostek, L. The transferrin isoforms in chronic hepatitis. Clin. Biochem. 2017, 50, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Gudowska, M.; Gruszewska, E.; Wrona, A.; Gindzienska-Sieskiewicz, E.; Domyslawska, I.; Lipartowska-Klimuk, K.; Cylwik, B.; Sierakowski, S.; Chrostek, L. The Profile of Serum Transferrin Isoforms in Rheumatoid Arthritis. J. Clin. Rheumatol. 2019, 25, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Grytczuk, A.; Bauer, A.; Gruszewska, E.; Cylwik, B.; Chrostek, L. Changed profile of serum transferrin isoforms in Primary Biliary Cholangitis. J. Clin. Med. 2020, 9, 2894. [Google Scholar] [CrossRef]
- Mucha, A.; Zaczek, M.; Kralisz, M.; Gruszewska, E.; Cylwik, B.; Panasiuk, A.; Chrostek, L. The serum profile of transferrin isoforms in pancreatitis. J. Clin. Med. 2022, 11, 1638. [Google Scholar] [CrossRef]
- World Health Organization Working Group on the Clinical Characterisation and management of COVID-19 infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Al-Salman, J.; Sanad Salem Alsabea, A.; Alkhawaja, S.; Al Balooshi, A.M.; Alalawi, M.; Abdulkarim Ebrahim, B.; Hasan Zainaldeen, J.; Al Sayyad, A.S. Evaluation of an adjusted MEWS (Modified Early Warning Score) for COVID-19 patients to identify risk of ICU admission or death in the Kingdom of Bahrain. J. Infect. Public Health 2023, 16, 1773–1777. [Google Scholar] [CrossRef] [PubMed]
- Ehlting, C.; Wolf, S.D.; Bode, J. G: Acute-phase protein synthesis: A key feature of innate immune functions of the liver. Biol. Chem. 2021, 402, 1129–1145. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef] [PubMed]
- Sayit, A.T.; Elmali, M.; Deveci, A.; Gedikli, O. Relationship between acute phase reactants and prognosis in patients with or without COVID-19 pneumonia. Rev. Inst. Med. Trop. Sao Paulo 2021, 63, e51. [Google Scholar] [CrossRef] [PubMed]
- Orhan, S.; Mecit, B.B.T.; Kazan, E.D.; Kazan, S.; Konya, P.S.; Gulsoy, K.Y. The Effect of Acute Phase Reactants on the Survival of COVID-19 Patients in Intensive Care. Prog. Nutr. 2021, 23 (Suppl. S2), e2021268. [Google Scholar] [CrossRef]
- Mehmood, R.; Mansoor, Z.; Atanasov, G.P.; Cheian, A.; Davletova, A.; Patel, A.; Ahmed, D. High-Flow Nasal Oxygenation and Its Applicability in COVID Patients. SN Compr. Clin. Med. 2022, 4, 49. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group | Sample 1 | Sample 2 | ||||
|---|---|---|---|---|---|---|
| Test | Median | IQR | Median | IQR | Median | IQR |
| pH | 7.405 | 0.50 | 7.457 * | 0.058 | 7.459 * | 0.052 |
| pO2 [mmHg] | 97.0 | 8.0 | 83.6 * | 43.0 | 82.6 * | 38.1 |
| pCO2 [mmHg] | 39.0 | 4.0 | 36.1 * | 5.8 | 38.5 | 6.4 |
| SatO2 [%] | 97.0 | 1.0 | 96.8 | 5.8 | 96.7 * | 3.2 |
| BE [mEq/L] | 0.33 | 2.05 | 2.50 * | 5.60 | 3.00 *# | 4.10 |
| IL6 [pg/mL] | 1.5 | 0.32 | 42.0 * | 107.6 | 24.6 * | 53.1 |
| Fibrinogen [mg/dL] | 294.0 | 86.0 | 393.0 * | 351.0 | 315.5 | 1714 |
| Creatinin [mg/dL] | 0.86 | 0.18 | 0.85 | 0.53 | 0.77 *# | 0.35 |
| CK [IU/L] | 89.0 | 71.0 | 93.0 * | 145.0 | 32.0 *# | 43.0 |
| ALT [IU/L] | 10.20 | 68.0 | 30.75 * | 40.75 | 35.00 * | 36.0 |
| AST [IU/L] | 20.0 | 6.0 | 42.0 * | 47.25 | 33.3 *# | 30.2 |
| GGT [IU/L] | 14.5 | 10.0 | 53.5 * | 87.5 | 75.0 * | 119.0 |
| LDH [IU/L] | 155.0 | 42.0 | 268.5 * | 195.0 | 182.0 *# | 92.0 |
| Bilirubin [mg/dL] | 0.46 | 0.23 | 0.52 | 0.38 | 0.447 | 0.626 |
| Glucose [mg/dL] | 86.4 | 11.6 | 109.0 * | 42.0 | 105.5 * | 39.3 |
| HBG [g/dL] | 13.70 | 1.60 | 12.95 * | 2.80 | 12.60 * | 2.90 |
| HCT [%] | 39.15 | 5.25 | 38.40 * | 7.90 | 37.60 * | 7.30 |
| RBC [×106/μL] | 4.59 | 0.605 | 4.275 * | 0.97 | 4.130 * | 0.855 |
| MCV [fl] | 86.55 | 5.85 | 89.20 | 8.55 | 89.55 # | 7.55 |
| WBC [×103/μL] | 6.49 | 1.75 | 7.20 | 4.35 | 6.95 # | 4.73 |
| PLT [×103/μL] | 243.0 | 55.0 | 205.5 | 107 | 254.0 # | 187.0 |
| INR | 0.93 | 0.065 | 1.145 * | 0.29 | 1.18 * | 0.35 |
| PT [s] | 12.40 | 0.70 | 13.75 * | 3.40 | 14.00 *# | 3.70 |
| Cholesterol [mg/dL] | 197.65 | 57.2 | 141.65 * | 62.65 | 140.70 * | 72.4 |
| TG [mg/dL] | 91.20 | 54.40 | 137.60 * | 75.9 | 164.35 * | 106.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrostek, L.; Gan, K.; Kazberuk, M.; Kralisz, M.; Janicka, K.; Gruszewska, E.; Panasiuk, A.; Cylwik, B. The Association of Serum Profile of Transferrin Isoforms with COVID-19 Disease Severity. J. Clin. Med. 2024, 13, 2446. https://doi.org/10.3390/jcm13082446
Chrostek L, Gan K, Kazberuk M, Kralisz M, Janicka K, Gruszewska E, Panasiuk A, Cylwik B. The Association of Serum Profile of Transferrin Isoforms with COVID-19 Disease Severity. Journal of Clinical Medicine. 2024; 13(8):2446. https://doi.org/10.3390/jcm13082446
Chicago/Turabian StyleChrostek, Lech, Kacper Gan, Marcin Kazberuk, Michal Kralisz, Katarzyna Janicka, Ewa Gruszewska, Anatol Panasiuk, and Bogdan Cylwik. 2024. "The Association of Serum Profile of Transferrin Isoforms with COVID-19 Disease Severity" Journal of Clinical Medicine 13, no. 8: 2446. https://doi.org/10.3390/jcm13082446