
The Reduction of Anastomosis-Related Morbidity Using the Kono-S Anastomosis in Patients with Crohn’s Disease: A Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Study Protocol
2.2. Endpoints
2.3. Eligibility Criteria
2.4. Literature Search
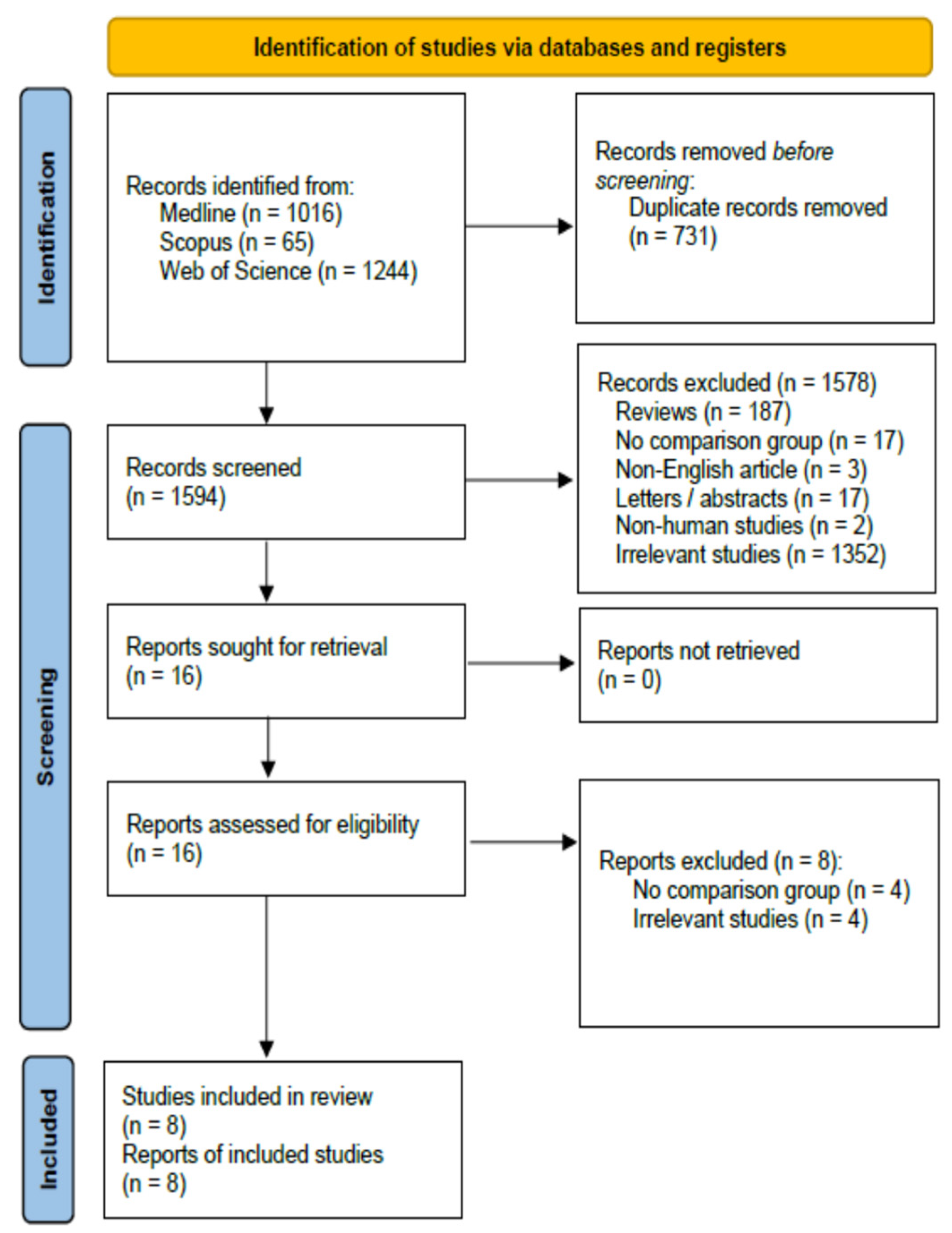
2.5. Study Selection and Data Collection
2.6. Statistical Analysis
2.7. Risk of Bias across Studies
3. Results
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef]
- Meima-van Praag, E.M.; Buskens, C.J.; Hompes, R.; Bemelman, W.A. Surgical Management of Crohn’s Disease: A State of the Art Review. Int. J. Color. Dis. 2021, 36, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Van der Have, M.; van der Aalst, K.S.; Kaptein, A.A.; Leenders, M.; Siersema, P.D.; Oldenburg, B.; Fidder, H.H. Determinants of Health-Related Quality of Life in Crohn’s Disease: A Systematic Review and Meta-Analysis. J. Crohns Colitis 2014, 8, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Luglio, G.; Rispo, A.; Imperatore, N.; Giglio, M.C.; Amendola, A.; Tropeano, F.P.; Peltrini, R.; Castiglione, F.; De Palma, G.D.; Bucci, L. Surgical Prevention of Anastomotic Recurrence by Excluding Mesentery in Crohn’s Disease: The SuPREMe-CD Study—A Randomized Clinical Trial. Ann. Surg. 2020, 272, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Shimada, N.; Ohge, H.; Kono, T.; Sugitani, A.; Yano, R.; Watadani, Y.; Uemura, K.; Murakami, Y.; Sueda, T. Surgical Recurrence at Anastomotic Site after Bowel Resection in Crohn’s Disease: Comparison of Kono-S and End-to-End Anastomosis. J. Gastrointest. Surg. 2019, 23, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Colombo, F.; Frontali, A.; Baldi, C.; Cigognini, M.; Lamperti, G.; Manzo, C.A.; Maconi, G.; Ardizzone, S.; Foschi, D.; Sampietro, G.M. Repeated Surgery for Recurrent Crohn’s Disease: Does the Outcome Keep Worsening Operation after Operation? A Comparative Study of 1224 Consecutive Procedures. Updates Surg. 2022, 74, 73. [Google Scholar] [CrossRef]
- De Cruz, P.; Hamilton, A.L.; Burrell, K.J.; Gorelik, A.; Liew, D.; Kamm, M.A. Endoscopic Prediction of Crohn’s Disease Postoperative Recurrence. Inflamm. Bowel Dis. 2022, 28, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Navaratne, L.; Hurndall, K.H.; Richardson, D.M.; Stephenson, R.; Power, N.; Gillott, H.; Ruiz Sánchez, S.; Khodatars, K.; Chan, C.L.H. Risk Factors for Symptomatic Anastomotic Postoperative Recurrence Following Ileo-Colic Resection in Crohn’s Disease. Color. Dis. 2021, 23, 1184–1192. [Google Scholar] [CrossRef]
- Aaltonen, G.; Keränen, I.; Carpelan-Holmström, M.; Lepistö, A. Risk Factors for Anastomotic Recurrence after Primary Ileocaecal Resection in Crohn’s Disease. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1143–1147. [Google Scholar] [CrossRef]
- Gklavas, A.; Dellaportas, D.; Papaconstantinou, I. Risk Factors for Postoperative Recurrence of Crohn’s Disease with Emphasis on Surgical Predictors. Ann. Gastroenterol. 2017, 30, 598–612. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.H.; Chin, Y.H.; Lin, S.Y.; Koh, J.W.H.; Lieske, B.; Koh, F.H.-X.; Chong, C.S.; Foo, F.J. Kono-S Anastomosis for Crohn’s Disease: A Systemic Review, Meta-Analysis, and Meta-Regression. Surg. Today 2021, 51, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Purkayastha, S.; Yamamoto, T.; Strong, S.A.; Darzi, A.W.; Tekkis, P.P. A Meta-Analysis Comparing Conventional End-to-End Anastomosis vs. Other Anastomotic Configurations after Resection in Crohn’s Disease. Dis. Colon Rectum 2007, 50, 1674–1687. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Li, Y.; Zhu, W.; Gong, J.; Li, N.; Li, J. Comparing Outcomes between Side-to-Side Anastomosis and Other Anastomotic Configurations after Intestinal Resection for Patients with Crohn’s Disease: A Meta-Analysis. World J. Surg. 2013, 37, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Kono, T.; Ashida, T.; Ebisawa, Y.; Chisato, N.; Okamoto, K.; Katsuno, H.; Maeda, K.; Fujiya, M.; Kohgo, Y.; Furukawa, H. A New Antimesenteric Functional End-to-End Handsewn Anastomosis: Surgical Prevention of Anastomotic Recurrence in Crohn’s Disease. Dis. Colon Rectum 2011, 54, 586–592. [Google Scholar] [CrossRef]
- Holubar, S.D.; Lipman, J.; Steele, S.R.; Uchino, T.; Lincango, E.P.; Liska, D.; Ban, K.; Rosen, D.; Sommovilla, J.; Gorgun, E.; et al. Safety & Feasibility of Targeted Mesenteric Approaches with Kono-S Anastomosis and Extended Mesenteric Excision in Ileocolic Resection and Anastomosis in Crohn’s Disease. Am. J. Surg. 2023, 230, 16–20. [Google Scholar] [CrossRef]
- Tyrode, G.; Lakkis, Z.; Vernerey, D.; Falcoz, A.; Clairet, V.; Alibert, L.; Koch, S.; Vuitton, L. KONO-S Anastomosis Is Not Superior to Conventional Anastomosis for the Reduction of Postoperative Endoscopic Recurrence in Crohn’s Disease. Inflamm. Bowel Dis. 2023, izad214. [Google Scholar] [CrossRef]
- Kelm, M.; Reibetanz, J.; Kim, M.; Schoettker, K.; Brand, M.; Meining, A.; Germer, C.-T.; Flemming, S. Kono-S Anastomosis in Crohn’s Disease: A Retrospective Study on Postoperative Morbidity and Disease Recurrence in Comparison to the Conventional Side-To-Side Anastomosis. J. Clin. Med. 2022, 11, 6915. [Google Scholar] [CrossRef]
- Alibert, L.; Betton, L.; Falcoz, A.; Manceau, G.; Benoist, S.; Zerbib, P.; Podevin, J.; Maggiori, L.; Brouquet, A.; Tyrode, G.; et al. Does KONO-S Anastomosis Reduce Recurrence in Crohn’s Disease Compared to Conventional Ileocolonic Anastomosis? A Nationwide Propensity Score-Matched Study from GETAID Chirurgie Group (KoCoRICCO Study). J. Crohns Colitis 2023, jjad176. [Google Scholar] [CrossRef]
- Nardone, O.M.; Calabrese, G.; Barberio, B.; Giglio, M.C.; Castiglione, F.; Luglio, G.; Savarino, E.; Ghosh, S.; Iacucci, M. Rates of Endoscopic Recurrence In Postoperative Crohn’s Disease Based on Anastomotic Techniques: A Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2023, izad252. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley-Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2019; ISBN 9781119536628. [Google Scholar]
- Narula, N.; Wong, E.C.L.; Dulai, P.S.; Marshall, J.K.; Jairath, V.; Reinisch, W. The Performance of the Rutgeerts Score, SES-CD, and MM-SES-CD for Prediction of Postoperative Clinical Recurrence in Crohn’s Disease. Inflamm. Bowel Dis. 2023, 29, 716–725. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Cuello, C.; Akl, E.A.; Mustafa, R.A.; Meerpohl, J.J.; Thayer, K.; Morgan, R.L.; Gartlehner, G.; Kunz, R.; Katikireddi, S.V.; et al. GRADE Guidelines: 18. How ROBINS-I and Other Tools to Assess Risk of Bias in Nonrandomized Studies Should Be Used to Rate the Certainty of a Body of Evidence. J. Clin. Epidemiol. 2019, 111, 105–114. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Obi, M.; DeRoss, A.L.; Lipman, J. Use of the Kono-S Anastomosis in Pediatric Crohn’s Disease: A Single-Institution Experience. Pediatr. Surg. Int. 2023, 39, 290. [Google Scholar] [CrossRef]
- Cushing, K.; Higgins, P.D.R. Management of Crohn Disease: A Review. JAMA 2021, 325, 69. [Google Scholar] [CrossRef]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohns Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef] [PubMed]
- Adamina, M.; Bonovas, S.; Raine, T.; Spinelli, A.; Warusavitarne, J.; Armuzzi, A.; Bachmann, O.; Bager, P.; Biancone, L.; Bokemeyer, B.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. J. Crohns Colitis 2020, 14, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Ponsioen, C.Y.; de Groof, E.J.; Eshuis, E.J.; Gardenbroek, T.J.; Bossuyt, P.M.M.; Hart, A.; Warusavitarne, J.; Buskens, C.J.; van Bodegraven, A.A.; Brink, M.A.; et al. Laparoscopic Ileocaecal Resection versus Infliximab for Terminal Ileitis in Crohn’s Disease: A Randomised Controlled, Open-Label, Multicentre Trial. Lancet Gastroenterol. Hepatol. 2017, 2, 785–792. [Google Scholar] [CrossRef]
- McLeod, R.S.; Wolff, B.G.; Ross, S.; Parkes, R.; McKenzie, M. Recurrence of Crohn’s Disease after Ileocolic Resection Is Not Affected by Anastomotic Type: Results of a Multicenter, Randomized, Controlled Trial. Dis. Colon Rectum 2009, 52, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Zurbuchen, U.; Kroesen, A.J.; Knebel, P.; Betzler, M.H.; Becker, H.; Bruch, H.P.; Senninger, N.; Post, S.; Buhr, H.J.; Ritz, J.P. Complications after End-to-End vs. Side-to-Side Anastomosis in Ileocecal Crohn’s Disease—Early Postoperative Results from a Randomized Controlled Multi-Center Trial (ISRCTN-45665492). Langenbecks Arch. Surg. 2013, 398, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.S.; Li, J.Y.; Yang, Z.; Chen, X.Y.; Mo, J.J.; Li, S.H. Stapled Side-to-Side Anastomosis Might Be Benefit in Intestinal Resection for Crohn’s Disease: A Systematic Review and Network Meta-Analysis. Medicine 2018, 97, e0315. [Google Scholar] [CrossRef] [PubMed]
- Alshantti, A.; Hind, D.; Hancock, L.; Brown, S.R. The Role of Kono-S Anastomosis and Mesenteric Resection in Reducing Recurrence after Surgery for Crohn’s Disease: A Systematic Review. Color. Dis. 2021, 23, 7–17. [Google Scholar] [CrossRef]
- Grażyńska, A.; Kufel, J.; Dudek, A.; Cebula, M. Shear Wave and Strain Elastography in Crohn’s Disease—A Systematic Review. Diagnostics 2021, 11, 1609. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Country | Study Type | Center | Year | Study Period | Group | Sample | Gender (M) | Age | BMI | Follow Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alibert et al. [19] | France | prospective | multi | 2023 | 2020–2022 | KONO-S | 61 | 26 | 37 (4.75) | 21.9 (1.17) | 6.7 (0.41) |
| CONV | 122 | 55 | 34 (3) | 20.9 (0.90) | |||||||
| Holubar et al. [16] | USA | retrospective | single | 2023 | 2015–2022 | KONO-S | 74 | 36 | 38.2 (16.3) | 25.1 (5.6) | n/a |
| CONV | 66 | 33 | 37.9 (15.5) | 25.4 (5.6) | |||||||
| Obi et al. [27] | USA | retrospective | single | 2023 | 2019–2022 | KONO-S | 9 | 4 | 15.4 | 21.6 | 6.55 |
| CONV | 9 | 3 | 16.2 | 20 | 7.57 | ||||||
| Tyrode et al. [17] | France | retrospective | single | 2023 | 2020–2022 | KONO-S | 30 | 13 | 32.2 (13.4) | 22.3 (3.92) | 12 |
| CONV | 55 | 24 | 36.1 (15.6) | 23.5 (6) | |||||||
| Kelm et al. [18] | Germany | retrospective | single | 2022 | 2019–2021 | KONO-S | 22 | 14 | 37.4 (10.5) | 24.3 | 8.8 (2.5) |
| CONV | 29 | 14 | 36.8 (13.7) | 22.8 | |||||||
| Luglio et al. [5] | Italy | RCT | single | 2020 | 2015–2017 | KONO-S | 36 | 18 | 34 (6.25) | n/a | 24 |
| CONV | 43 | 22 | 43 (8.25) | ||||||||
| Shimada et al. [6] | Japan | retrospective | single | 2019 | 2006–2016 | KONO-S | 117 | 84 | 39 (11.8) | 18.9 (2.51) | 38 (23.7) |
| CONV | 98 | 74 | 34 (11.1) | 18.6 (2.44) | 89 (34) | ||||||
| Kono et al. [15] | Japan | retrospective | multi | 2011 | 2003–2009 | KONO-S | 69 | 57 | 31 (10.7) | n/a | 42 (18.7) |
| CONV | 73 | 58 | 28 (12) | 52 (29.7) |
| Outcome | Studies | Participants | Statistical Method | Effect Estimate 95%CI | p | I2 | Heterogeneity p |
|---|---|---|---|---|---|---|---|
| Overall Complications | 8 | 913 | Random Effects | 0.69 [0.42, 1.15] | 0.16 | 46% | 0.08 |
| CD ≥ III | 4 | 459 | Fixed Effects | 0.54 [0.22, 1.32] | 0.18 | 14% | 0.32 |
| Intrabdominal Abscess | 6 | 624 | Fixed Effects | 0.62 [0.31, 1.25] | 0.18 | 0% | 0.68 |
| SSI | 7 | 730 | Fixed Effects | 1.85 [1.02, 3.35] | 0.04 | 0% | 0.71 |
| Ileus | 6 | 645 | Fixed Effects | 0.95 [0.55, 1.66] | 0.87 | 0% | 0.88 |
| Bleeding | 4 | 446 | Fixed Effects | 0.34 [0.09, 1.25] | 0.1 | 0% | 0.82 |
| Leakage | 7 | 828 | Fixed Effects | 0.34 [0.16, 0.71] | 0.004 | 0% | 0.66 |
| Readmission | 4 | 453 | Fixed Effects | 0.59 [0.26, 1.35] | 0.21 | 5% | 0.37 |
| Reoperation | 4 | 515 | Fixed Effects | 0.12 [0.05, 0.27] | <0.001 | 0% | 0.66 |
| >i2 | 5 | 540 | Random Effects | 0.66 [0.33, 1.29] | 0.22 | 68% | 0.01 |
| Clinical Recurrence | 4 | 562 | Random Effects | 0.42 [0.14, 1.24] | 0.12 | 75% | 0.007 |
| Operation Duration [minutes] | 5 | 702 | Random Effects | 5.71 [−4.93, 16.36] | 0.29 | 83% | <0.001 |
| LOS [days] | 4 | 487 | Fixed Effects | −0.54 [−0.73, −0.34] | <0.001 | 0% | 0.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baloyiannis, I.; Perivoliotis, K.; Sarakatsianou, C.; Chatzinikolaou, C.; Tzovaras, G. The Reduction of Anastomosis-Related Morbidity Using the Kono-S Anastomosis in Patients with Crohn’s Disease: A Meta-Analysis. J. Clin. Med. 2024, 13, 2461. https://doi.org/10.3390/jcm13092461
Baloyiannis I, Perivoliotis K, Sarakatsianou C, Chatzinikolaou C, Tzovaras G. The Reduction of Anastomosis-Related Morbidity Using the Kono-S Anastomosis in Patients with Crohn’s Disease: A Meta-Analysis. Journal of Clinical Medicine. 2024; 13(9):2461. https://doi.org/10.3390/jcm13092461
Chicago/Turabian StyleBaloyiannis, Ioannis, Konstantinos Perivoliotis, Chamaidi Sarakatsianou, Charito Chatzinikolaou, and George Tzovaras. 2024. "The Reduction of Anastomosis-Related Morbidity Using the Kono-S Anastomosis in Patients with Crohn’s Disease: A Meta-Analysis" Journal of Clinical Medicine 13, no. 9: 2461. https://doi.org/10.3390/jcm13092461