
Visual Acuity and Retinal Thickness and Sensitivity after Intravitreal Ranibizumab Injection for Macular Edema in Branch Retinal Vein Occlusion
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. OCT
2.3. Functional Mapping by Microperimetry
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
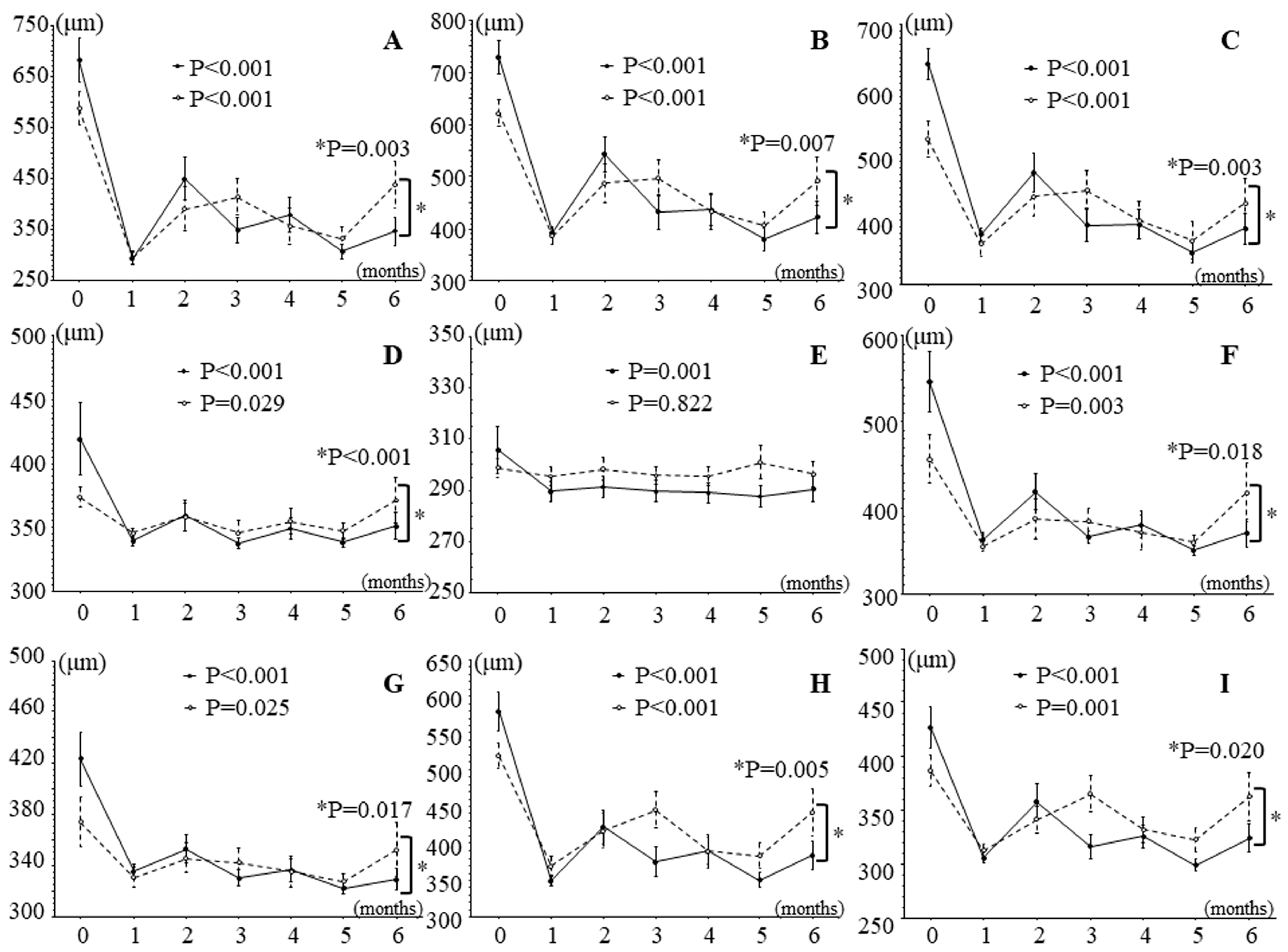
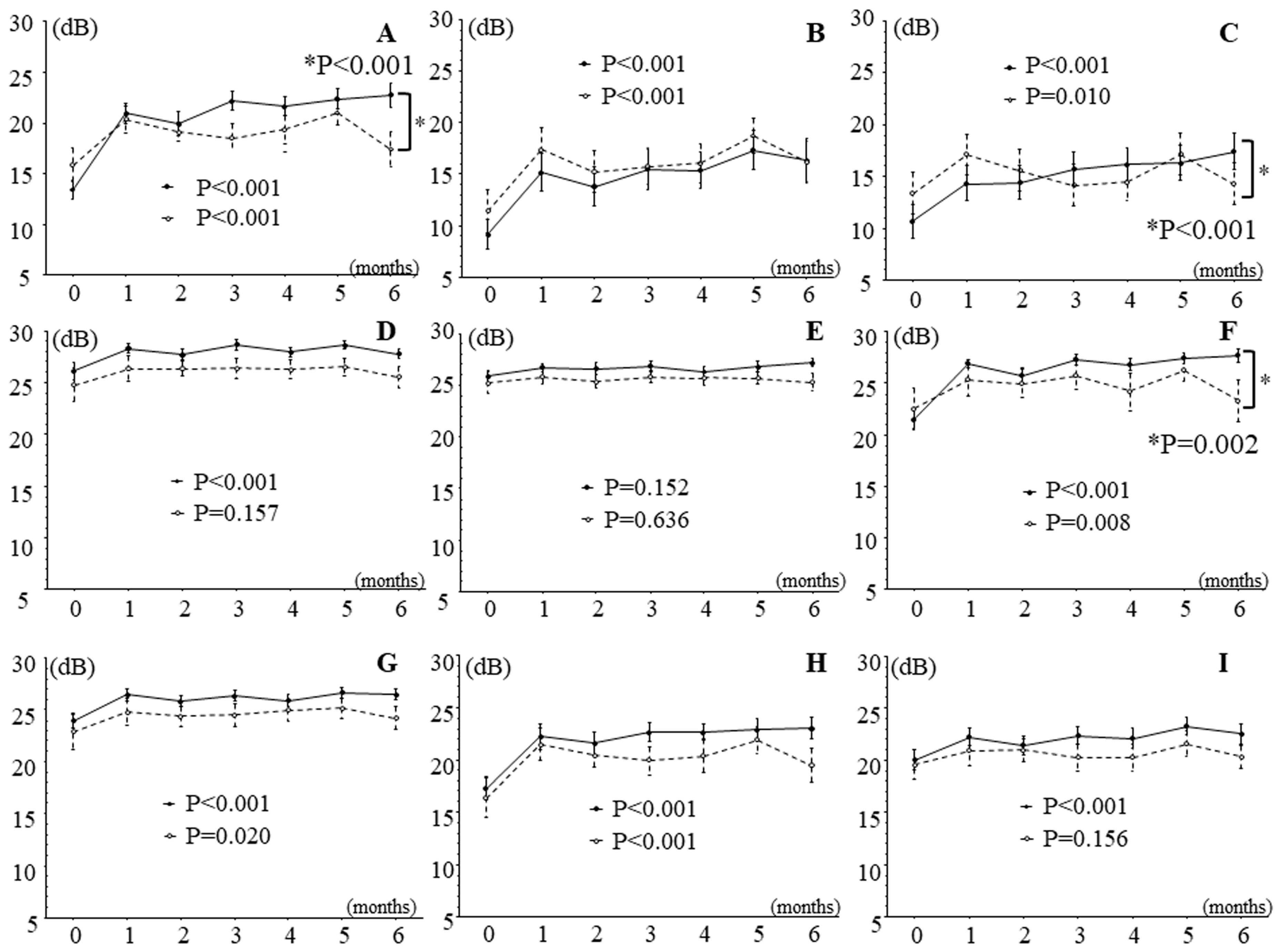
3.2. Effects of IRI on Retinal Thickness and Sensitivity in Patients with Branch Retinal Vein Occlusion and Macular Edema
3.3. Effects of Intravitreal Ranibizumab Injection on Retinal Thickness and Sensitivity in Patients with Branch Retinal Vein Occlusion and Macular Edema Subdivided into Two Groups According to Improvement in Best Corrected Visual Acuity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, T.Y.; Scott, I.U. Clinical practice. Retinal-vein occlusion. N. Engl. J. Med. 2010, 363, 2135–2144. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e311. [Google Scholar] [CrossRef]
- McIntosh, R.L.; Mohamed, Q.; Saw, S.M.; Wong, T.Y. Interventions for branch retinal vein occlusion: An evidence-based systematic review. Ophthalmology 2007, 114, 835–854. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Hafiz, G.; Shah, S.M.; Nguyen, Q.D.; Ying, H.; Do, D.V.; Quinlan, E.; Zimmer-Galler, I.; Haller, J.A.; Solomon, S.D.; et al. Ranibizumab for macular edema due to retinal vein occlusions: Implication of VEGF as a critical stimulator. Mol. Ther. 2008, 16, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Heier, J.S.; Feiner, L.; Gray, S.; Saroj, N.; Rundle, A.C.; Murahashi, W.Y.; Rubio, R.G. Ranibizumab for macular edema following branch retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology 2010, 117, 1102–1112.e1101. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.L.; McIntosh, R.L.; Lim, L.; Mitchell, P.; Cheung, N.; Kowalski, J.W.; Nguyen, H.P.; Wang, J.J.; Wong, T.Y. Natural history of branch retinal vein occlusion: An evidence-based systematic review. Ophthalmology 2010, 117, 1094–1101. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Yasuda, K.; Shimura, M. Cytokines and the Pathogenesis of Macular Edema in Branch Retinal Vein Occlusion. J. Ophthalmol. 2019, 2, 5185128. [Google Scholar] [CrossRef]
- Noma, H.; Funatsu, H.; Mimura, T.; Eguchi, S.; Hori, S. Soluble vascular endothelial growth factor receptor-2 and inflammatory factors in macular edema with branch retinal vein occlusion. Am. J. Ophthalmol. 2011, 152, 669–677.e661. [Google Scholar] [CrossRef] [PubMed]
- Manabe, K.; Tsujikawa, A.; Osaka, R.; Nakano, Y.; Fujita, T.; Shiragami, C.; Hirooka, K.; Uji, A.; Muraoka, Y. Metamorphopsia Associated with Branch Retinal Vein Occlusion. PLoS ONE 2016, 11, e0153817. [Google Scholar] [CrossRef]
- Sugiura, Y.; Okamoto, F.; Morikawa, S.; Okamoto, Y.; Hiraoka, T.; Oshika, T. Time Course of Changes in Metamorphopsia Following Intravitreal Ranibizumab Injection for Branch Retinal Vein Occlusion. Retina 2018, 38, 1581–1587. [Google Scholar] [CrossRef]
- Suñer, I.J.; Bressler, N.M.; Varma, R.; Lee, P.; Dolan, C.M.; Ward, J.; Colman, S.; Rubio, R.G. Reading speed improvements in retinal vein occlusion after ranibizumab treatment. JAMA Ophthalmol. 2013, 131, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, Y.; Okamoto, F.; Murakami, T.; Morikawa, S.; Hiraoka, T.; Oshika, T. Time course of changes in contrast sensitivity following intravitreal ranibizumab injection for branch retinal vein occlusion. Jpn. J. Ophthalmol. 2020, 64, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Awdeh, R.M.; Elsing, S.H.; Deramo, V.A.; Stinnett, S.; Lee, P.P.; Fekrat, S. Vision-related quality of life in persons with unilateral branch retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Br. J. Ophthalmol. 2010, 94, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Wrzesińska, D.; Nowomiejska, K.; Nowakowska, D.; Brzozowska, A.; Avitabile, T.; Reibaldi, M.; Rejdak, R.; Toro, M. Vertical and Horizontal M-Charts and Microperimetry for Assessment of the Visual Function in Patients after Vitrectomy with ILM Peeling due to Stage 4 Macular Hole. J. Ophthalmol. 2019, 6, 4975973. [Google Scholar] [CrossRef] [PubMed]
- Yamaike, N.; Tsujikawa, A.; Sakamoto, A.; Ota, M.; Kotera, Y.; Miyamoto, K.; Kita, M.; Yoshimura, N. Retinal sensitivity after intravitreal injection of bevacizumab for the treatment of macular edema secondary to retinal vein occlusion. Retina 2009, 29, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Barbazetto, I.A.; Schmidt-Erfurth, U.M. Evaluation of functional defects in branch retinal vein occlusion before and after laser treatment with scanning laser perimetry. Ophthalmology 2000, 107, 1089–1098. [Google Scholar] [CrossRef]
- Ota, M.; Tsujikawa, A.; Murakami, T.; Yamaike, N.; Sakamoto, A.; Kotera, Y.; Miyamoto, K.; Kita, M.; Yoshimura, N. Foveal photoreceptor layer in eyes with persistent cystoid macular edema associated with branch retinal vein occlusion. Am. J. Ophthalmol. 2008, 145, 273–280. [Google Scholar] [CrossRef]
- Wu, Z.; Ayton, L.N.; Luu, C.D.; Guymer, R.H. Longitudinal changes in microperimetry and low luminance visual acuity in age-related macular degeneration. JAMA Ophthalmol. 2015, 133, 442–448. [Google Scholar] [CrossRef]
- Michalska-Małecka, K.; Kałużny, J.; Nowak, M.; Gościniewicz, P.; Matysik-Woźniak, A.; Nowomiejska, K.; Karpe, J.; Rejdak, R. Evaluation of retinal function improvement in neovascular age-related macular degeneration after intravitreal aflibercept injections with the use of the assessment of retinal sensitivity: The use of the assessment of retinal sensitivity in anti-VEGF treatment—A STROBE-compliant observational study. Medicine 2019, 98, e17599. [Google Scholar]
- Noda, H.; Kimura, S.; Hosokawa, M.M.; Shiode, Y.; Doi, S.; Takahashi, K.; Matoba, R.; Kanzaki, Y.; Fujiwara, A.; Morizane, Y. Effect of rhegmatogenous retinal detachment on preoperative and postoperative retinal sensitivities. Sci. Rep. 2020, 10, 21497. [Google Scholar] [CrossRef]
- Zabel, P.; Zabel, K.; Kazmierczak, K.; Stankiewicz, M.; Jaworski, D.; Suwala, K.; Buszko, K.; Stafiej, J.; Malukiewicz, G.; Kaluzny, J.J. Vascular density and macular sensitivity in eyes after scleral buckling surgery for macula-on rhegmatogenous retinal detachment. PLoS ONE 2023, 18, e0279683. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Wakamatsu, Y.; Miyata, R.; Kato, K.; Matsubara, H.; Kondo, M. Effectiveness of microperimetry in evaluating anti-vascular endothelial growth factor therapy for diabetic macular edema patients with relatively good vision: A retrospective observational study. Medicine 2021, 100, e2840. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Wang, Y.; Li, X.X. Morphologic and functional evaluation before and after successful macular hole surgery using spectral-domain optical coherence tomography combined with microperimetry. Retina 2012, 32, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Kaluzny, J.J.; Zabel, P.; Kaluzna, M.; Lamkowski, A.; Jaworski, D.; Woznicki, K.; Zabel, K. Macular Sensitivity in the Area of Internal Limiting Membrane Peeling in Eyes after Pars Plana Vitrectomy with the Temporal Inverted Internal Limiting Membrane Flap Technique for a Full-Thickness Macular Hole. Retina 2021, 41, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Tadayoni, R.; Svorenova, I.; Erginay, A.; Gaudric, A.; Massin, P. Decreased retinal sensitivity after internal limiting membrane peeling for macular hole surgery. Br. J. Ophthalmol. 2012, 96, 1513–1516. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Mao, J.; Lao, J.; Deng, X.; Liu, C.; Xu, J.; Wu, S.; Chen, Y.; Shen, L. Macular Retinal Sensitivity and Microvasculature Changes before and after Vitrectomy in Idiopathic Macular Epiretinal Membrane with Classification. Ophthalmologica 2021, 244, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Winterhalter, S.; Vom Brocke, G.A.; Klamann, M.K.; Müller, B.; Joussen, A.M. Monthly microperimetry (MP1) measurement of macular sensitivity after dexamethasone implantation (Ozurdex) in retinal vein occlusions. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1873–1882. [Google Scholar] [CrossRef]
- Kriechbaum, K.; Prager, F.; Geitzenauer, W.; Benesch, T.; Schutze, C.; Simader, C.; Schmidt-Erfurth, U. Association of retinal sensitivity and morphology during antiangiogenic treatment of retinal vein occlusion over one year. Ophthalmology 2009, 116, 2415–2421. [Google Scholar] [CrossRef]
- Winterhalter, S.; Lux, A.; Maier, A.K.; Scholz, C.; Heussen, F.M.; Huber, K.K.; Joussen, A.M. Microperimetry as a routine diagnostic test in the follow-up of retinal vein occlusion? Graefes Arch Clin. Exp. Ophthalmol. 2012, 250, 175–183. [Google Scholar] [CrossRef]
- Rezar, S.; Eibenberger, K.; Bühl, W.; Georgopoulos, M.; Schmidt-Erfurth, U.; Sacu, S. Anti-VEGF treatment in branch retinal vein occlusion: A real-world experience over 4 years. Acta Ophthalmol. 2015, 93, 719–725. [Google Scholar] [CrossRef]
- Kadomoto, S.; Muraoka, Y.; Ooto, S.; Miwa, Y.; Iida, Y.; Suzuma, K.; Murakami, T.; Ghashut, R.; Tsujikawa, A.; Yoshimura, N. Evaluation of Macular Ischemia in Eyes with Branch Retinal Vein Occlusion: An Optical Coherence Tomography Angiography Study. Retina 2018, 38, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Fujino, R.; Asaoka, R.; Aoki, S.; Sugiura, A.; Kusakabe, M.; Asano-Shimizu, K.; Nomura, Y.; Aoki, A.; Hashimoto, Y.; Azuma, K.; et al. The usefulness of the retinal sensitivity measurement with a microperimetry for predicting the visual prognosis of branch retinal vein occlusion with macular edema. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Rachima, S.; Hirabayashi, K.; Imai, A.; Iesato, Y.; Murata, T. Prediction of post-treatment retinal sensitivity by baseline retinal perfusion density measurements in eyes with branch retinal vein occlusion. Sci. Rep. 2020, 10, 9614. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, K.H.; Vestergaard, J.P.; Pedersen, F.N.; Vergmann, A.S.; Sørensen, T.L.; Laugesen, C.S.; Kawasaki, R.; Peto, T.; Grauslund, J. Navigated laser and aflibercept versus aflibercept monotherapy in treatment-naïve branch retinal vein occlusion: A 12-month randomized trial. Acta Ophthalmol. 2022, 100, e1503–e1509. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Funatsu, H.; Mimura, T.; Harino, S.; Shimada, K. Functional-morphologic correlates in patients with branch retinal vein occlusion and macular edema. Retina 2011, 31, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Funatsu, H.; Mimura, T.; Tatsugawa, M.; Shimada, K.; Eguchi, S. Vitreous inflammatory factors and serous macular detachment in branch retinal vein occlusion. Retina 2012, 32, 86–91. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Uji, A.; Lei, J.; Velaga, S.; Nittala, M.; Sadda, S. Interdevice comparison of retinal sensitivity assessments in a healthy population: The CenterVue MAIA and the Nidek MP-3 microperimeters. Br. J. Ophthalmol. 2018, 102, 109–113. [Google Scholar] [CrossRef]
- Otawa, T.; Noma, H.; Yasuda, K.; Narimatsu, A.; Asakage, M.; Tanaka, A.; Goto, H.; Shimura, M. Intravitreal ranibizumab improves macular sensitivity in patients with central retinal vein occlusion and macula edema. BMC Ophthalmol. 2022, 22, 247. [Google Scholar] [CrossRef]
- Eiidome, E.; Noma, H.; Yasuda, K.; Yanagida, K.; Narimatsu, A.; Asakage, M.; Watarai, S.; Goto, H.; Shimura, M. Macular Sensitivity after Intravitreal Ranibizumab Injection for Macular Edema in Central Retinal Vein Occlusion: One versus Three Initial Monthly Injections. J. Vasc. Dis. 2022, 1, 43–52. [Google Scholar] [CrossRef]
- Pavlidis, M.; Stupp, T.; Hummeke, M.; Thanos, S. Morphometric examination of human and monkey retinal ganglion cells within the papillomacular area. Retina 2006, 26, 445–453. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | BRVO (n = 34) |
|---|---|
| Age, years | 61.9 ± 9.7 ‡ |
| Sex, female/male | 18/16 |
| Duration of macular edema, days | 37.0 ± 29.0 ‡ |
| Hypertension | 27 (79.4%) |
| Systolic blood pressure, mmHg | 149 ± 19 |
| Diastolic blood pressure, mmHg | 94 ± 14 |
| Hyperlipidemia | 16 (47.1%) |
| Baseline BCVA logMAR, Snellen | 0.51 ± 0.36 ‡ |
| Baseline CMT, μm | 638 ± 166 ‡ |
| Presence of SRD | 17 (50.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nonaka, R.; Noma, H.; Yasuda, K.; Sasaki, S.; Goto, H.; Shimura, M. Visual Acuity and Retinal Thickness and Sensitivity after Intravitreal Ranibizumab Injection for Macular Edema in Branch Retinal Vein Occlusion. J. Clin. Med. 2024, 13, 2490. https://doi.org/10.3390/jcm13092490
Nonaka R, Noma H, Yasuda K, Sasaki S, Goto H, Shimura M. Visual Acuity and Retinal Thickness and Sensitivity after Intravitreal Ranibizumab Injection for Macular Edema in Branch Retinal Vein Occlusion. Journal of Clinical Medicine. 2024; 13(9):2490. https://doi.org/10.3390/jcm13092490
Chicago/Turabian StyleNonaka, Ryota, Hidetaka Noma, Kanako Yasuda, Shotaro Sasaki, Hiroshi Goto, and Masahiko Shimura. 2024. "Visual Acuity and Retinal Thickness and Sensitivity after Intravitreal Ranibizumab Injection for Macular Edema in Branch Retinal Vein Occlusion" Journal of Clinical Medicine 13, no. 9: 2490. https://doi.org/10.3390/jcm13092490